Embed Size (px)
Citation preview

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 1/12
--l:G
=
Czo
-o
c

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 2/12
OVERVIEW
The Innate lmmune System
The innate immune system s rapid acting, nonspecific,and has no memory. It has many components,which
include complement, macrophages,and naturai killerQ.iK) ceils. t is the first line of defenseafter the skin.
The Adaptive lmmune System
The adaptive mmune system s much slower than theimate to get startedbut is very specificand hasmemory.
It consistsof T andB cells,as well as mmuneglobuiins(Igs), and s a second ine ofdefense that is activatedbythe innate immune system.
The adaptive immune system can be divided rntohumoral and cell-mediatedcomponents.
. Humoral: B cells,plasmacel1s, nd mmunogiobulins
. Cell-mediated:T cells, activatedmacrophages, ndactivatedNK ceiis
lnnate vs. Adaptive lmmunity
The innate irnmunesystem s the foundation on whichthe more sophisticatedadaptive mmune system rests.The innate system not only protects the body whilethe adaptive mmune systemgearsup, but it alsohelpsdirect the response.The innate mmune system n gen-eral needsmessageso prevent t from killing, while theadaptive mmune systemneedsmessagesusually fromthe innate immune system) to allow it to ki1l.
The key difference between he 2 systemscanbe foundin thereceptors.
. Innate imrnrlne system receptorsaregeneric ready-
made receptors example:To1l-iike eceptors).Thesereceptorsallow a quick but nonspecific esponse----onethat is very rapid but may not be able o recognizeallpathogens.Think of the innate irnmune system as he"first responders" o anew atlack.
. Adaptive irnmune system eceptorsare custom-madereceptors(T-cel1 eceptors TCRs], B-cell receptors
tBCRsl, and mmunoglobulins[gs]), which arerefined to be as specific aspossible or the pathogen.
This systemhas he ability to recognizea seemingly
infnite vanety of pathogens.Once hesecustom-madereceptorshave served heir purpose, hebody keepsafew of them around in case t needs hem agaur:n thefuture-so it canreact much more ouickly next time(memory).
lnnate and Adaptive Overlap
ft ls important to understand that there is significant
overiap between the innate and adaptive immunesystem. Aa exampie is seen in the macrophages and
THE IMMUNE SYSTEM
NK cells that function aspart of the innatesystem rni-tially, but then they become lr:ther activatedby T cells
and can hen actaspart of the adaptive mmunesystem.Similarly, the "ClassicalPathway" of the complementsystem uses antibody (Ig) to initiate its activrry Thisaniibody involvement n the complementsystem s alsoan example of how the adaptive immune system pro-
videsmemory.Aaother example of overlap is a group of irrnate-likecel1sof the adaptive mmunesystem hat are more rapidactrngand essspecific.
Examplesof imate-like immunecells are:
. y:6 T cellsand naturai kiiler T cells
. B-1 cells (an rnnate-likeversionof B ceils)
CELLSOF THE MMUNE YSTEM
Cells in the immune systemare divided into 2 catego-nes: ll,rnphoid ceilsand myeioid cells.We'li outline thetypeshereand discusshe need-to-knowpoints.
Llmphoid cells:
" Lymphocytes B cells andT cetls)
" B cells:B-1 cells(innate-1ike)
B-2 cells(whatwe typically call "B" ceils). Marginal B cells (innate-like)
" T cells. o.:B ceils:consist f CD4 T cellsandCDST cells.
" Naturai killer T OIKT) ceils (innate-1ike). y:6 T cells(innate-like)
. Naturalkiller cells(difrerent rom the simiiarly namedT ceilsl)
Myeloid cells:
. Granuiocytes. Neutrophils. Eosinophils
" Basophiis. Professionalantigen-presentiagells
. Monocytes/X4acrophages
" Dendritic ceils. Other
. Mast cells
. Erythrocytes
. Platelets
The hrstocompatibility molecuies are the antigensrequired by the body for determination of self vs. non-self material. The genes or the antigens areon chromo-some 6, and this comFlexof genes s cailed the MajorHistocompatibility Complex (lt4lfc). The human MHCis called HLA. There are 3 ciassesof HLA antigens(I,tr, and ltr). The T ceils are able to recognize antigens {
@ 2011 MedStudy

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 3/12
LYMPHOID CELLS
and only i{ they arepresentedby eitherciass or ciass
iI Iil,A antigens.
Class Iil-A antigens }il.,A-A, -B, and-C) areon mostbody tissues---cxcept hey are never found on mafure
RBCs. Liver cells and striated muscle cells may havelittle or none, ulless they become nflamed.Theseclass
antigens resentnon-selfmaterial o the CD8+ T ceils-
aswith h'ansplant ejection, neoplasms, ndviruses.
The class II IILA antigensare on monocytes/macro-phages,Langerhanscells,dendriticcells, andB cells (so
theseqellshave both class and class HLA antigens).These mediate the reaction between macrophages,T cells,and B cells.The CD4+ T ceils recognizemate-rial presentedonly by the class I antigens.Class I hastheHLA-D antigens, ncluding DR2, DR3, andDR4.
Class tr HLA antigensconsistof a few cytokines, ikeTNF and ymphotoxrn, andseveralcomplementcompo-nent structures not discussedmuch in reviews).
LYMPHOCYTES
T Cel ls
Overview
Review: CD stands or "clustersof difflerentiation."CDmarkers are like "name tags" and allow one to "differ-
entiate" one immune cell from another. For example,
T cellsne CD2+ and CD3+. Mafure B cellsareCD19+and CD20+. Natural kiiler cellsareCD16+ and CD56+
FunctionsofT cells:
. Destuoy nkacellular andotherbacteria especiailygram-negative), iruses, ungi, parasites, ndmycobacteria
. Regulateantibodyproduction by B cells
Al1 T ceils have receptors (T-cell receptor = TCR),which are antigen-specific binding sites composedof2 subunits (the majority being alpha and beta and aminority being the innate-likegamma and delta). TheTCR is 5imilar to an immrrnoglobulin,and it is always
foundwith a CD3 complex.Again:All T cellsrecoBnizean antigenonly ifit ispresentedproperly; that is, aiongwith the HLA anhgen of the presentrngcell. This is thekey conceptof MHC resfiction CD8+ T cells recog-
nize antigen only if it is presentedwith a ciass I IILAantigen,whereasCD4+ T cells recosnizeantigenonly ifit is presentedwith a class r I{LA antigen.(A nice wayto remember his: CD8 x MHC I = 8, CD4 x MHC II :
8). On the T ceil, the TC& in associafionwith the CD3protein, recopnizes the IILA antiged-[foreip antigen]complexon the presentingceil (it takes2 to know 2 ).
All T cells areCD2*, andmost are CD3+. T cells alsousually have either a CD4 or CD8 protein on their sur-face. Vrfually all mature T cells forrn a "rosette" withsheepRBCs because he sheepRBCs bind to the CD2on theT ceils.
CD4+T Cells
CD4+ T ceils are the primary defenseagainst exog-
enous antigens.The CD4+ T celis are roughly dividedinto 2 subsets;THl (whrch induce CD8+ T ceils and
lead o cell-mediated mmunity) and TH2 (which induce=
B cells to produce antibody and humoral immunity).They can be activatedoniy by antigenspresentedalong
with ciass r HLA antigens.
Again: These class I antigensare on the professionalantigen-presenting celis (monocytes/macrophages,
Langerhans ells,dendnticcells, andB cells). For exam-ple, a macrophage :rgestsa foreign particle or micro-organism, hen extrudesantigen (onto the macrophagesurface) rom theparticle,which, along with the class IHLA antigen, s presented o the CD4+ T cell. TheseT cells, afterbeing activated, nduceB cells to convertto plasmacells and producespecificantibodiesagainstthat antigen.HfV targetsall CD4 cells,and, even houghthe CD4+ T cells are a main target,macrophagesimono-cytes/microgliai cells also may express he CD4 and
be a target. By targetingCD4+ cel1s,HfV weakens heimmune system, allowurg opporhrnistic infections to
occur.
Natural killer T cellsare a subtypeof CD4+ T cells.
Qrlamealertl: Thereare also nnate ymphoid cells witha very similar name-natural killer ceils.)
Natural killer T cells are not just MHC restricted; heyare restricted to a particular subgroupof MHC calledCDi, which recognizesprimarily lipids andglycolipids.They are so named becausehey share severbl eatureswith natural killer cells, such as granrqe productionandCDi6 andCD56expression.
CD8+T Cells
The CD8+ cellsare cyiotoxicT cells.They are mportantin the defenseagainstvirusesandneoplasticcells. Theyare activatedby neoplasticantigensand other antigenspresentedn associationwith class IILA antigens. Somostcell types canpresentantigen o CD8+ T celIsl)
T RegulatoryCells
Also called T suppressorceils. This can be a con-fusrng group of cells surce it is made up of severaldifferent types of T cells (usuallyCD4+ but also CD8+
and others). The expressionof the transcriptionfactorFO)G3 controls he developmentand function of T reg-ulatory cells. These cells suppress,or more accurately,regulate the immune response by secreting cytokineslike IL-10, T€F-p, and FN-o.
B Cells
Some B cells, upon stimuiation,becomeplasma cells(aatibody-producingcells). B cells are "surface mem- 14ae immunoglobulin positive (SmIg+)"; i.e., they
O 2011 MedStudy-Please Report Copyright Infringements to [email protected]
-€

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 4/12
. Explain he difference etween nnaievs.
adaptivemmunity.
. What are class l HLAantigens, nd wherear e
lhorr lncaiad?
. What mmunogiobulinsre present n mature
B cells?
have IgM and IgD on their surfaces,which distinguish
tlem from T cells, B-cel1precursors,andplasma ceils.
B celis canbe stimulatedto convert to plasma cells by
either antigen alone or activated CD4+ T ceiis. The
specific antibody produced coats the microorganism.
This coating either identiies it as edible to the macro-
phages(opsomzation)or imtiatesthe complementcas-
cade complementactivation),which doesnothing more
than build a mechanism o driil a hole in the cell wail.
Specrficantibodies can also neutraUzebacterial toxinsandviruses(neutralization).
Agaia, remember hat even houghall B cells are SmIg+,
the B-cell precursorsandplasma cells may be SmIg-.
B ce1ls. ike monocy'tes/macrophages,ave the class I*:- - l..srocompaLibiliry LA) antigenson their sur-
faces,so they also can presentforeign antigens o the
CD4+ @eiper)T ceils. The activatedT cells thenhduce
otherB cel1s o convert o piasmaceils andproduce anti-
body. B cel1sare the most specific,antigen-presenting
ceils. Mature B cells are CD19+andCD20+,
NATURALKILLER CELLSThere are also lyrnphoid celis cailednatural killer cells.(Name alert :There are nnate-likeCD4+ T cells with a
very similarname,natural kiiler T cells.)
Naturalkiller Q.IK)cellsplay a major role in the mmrure
system response o tumors and viruses. They express
CD16 and CD56 but not TCR or its associated D3
moiecules (an important differencebetweenthem and
naturalkiiler T cells).
They are ca11ed atural killers because hey are always
in kill mode, and the cellsthey encountermust present
themseivesappropriately :r order to not be lalled. For
example, all cells (exceptmature RBCs) must present
class HLA antigens n order o not be killed by naturalkiller cells.
Natural killer cells are an important component of the
irnmune system because some vjruses reduce class I
HLA expression,protecting them from recognitionand
destruction by T cells. With natural killer cells, it is
precisely this absence or reduction of ciass I I{LA
expression that causes he natural killer cell to kiil (usu-
aliy by inducing apoptosis)the infected cell.
MYELOID CELLS
ft1 ssmparison, natural killer T ceils, iike all other
T cells,requirethe antigen o bepresented n association
with an HLA antigenbefore they canbecomeactivated
to kill.
Granulocytes: White blood ceilswith identifiabiegran-ules in theu cytoplasm.
Neutrophils = polys : PMNs : segs (mature) and
bands (immature).PMNs phagocytizemicroorganisms,especially if coated with antibodies (opsonization;Igcoating "like the shel1 on lzt&Ms@"). If PMNs areabsent,patientsget overwhekningpyogenic nfections.
Eosinophils: Involved in the pathology of ailergicreactionsbut also rn the immunoiogic defenseagainstparasrtes.
Basophils are discussed under Immediate Hlper-sensitivity Reactions page9-6).
Professional antigen-presenting cells:Ceils expressingN{FICI and MHCIL This is an exc.lusivegroup of cellsconsrsting f 3 cell types:
1) B celIs.
2) MonocytesAvfacrophageseat opsonized microor-ganisms,processand presentantigens, and secreternterleukil-l (IL-1), which stimulatesT cells.
3) Dendritic ceils are scavengershat,when they ingesta pathogen,changeconforrnation, ravel to a lymphnode,aad activale ymphocytes.
Other:
. Mast Celis are discussed nderknmediateHypersensitivity Reactions page9-6).
. Erythrocytesarecovered n the Hematologysection.
. Megakaryocytes/Platelets rediscussedn theHematoiogysection.
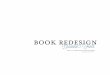
A11antibodies(immunoglobulins)have the same basicstructure(Figwe 9-1). Each monomer is composedof
2 heatry and 2 light chains that are heid together bydisulfide bonds. There are 5 immunoglobulin isotypes:
G, A, M, E, and D. These sotypesare deterrriaedby
differences n the structureofthe constant egions oftheheary chains.All antibodieshave 1 of 2 types of light
chains,kappaor lambda.
Remember he following;
IgG is the main antibody in serum, and it is the majorantibody in the immune response. t readiiy crossesheplacenta. It has 4 subclasses IgGl, IgG2, IgG3, andIgGa). IgG canactivatecomplement.
@2011Medstudy

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 5/12
COMPLEMENT CASCADE
THEANTIBODY
Fab
Hinge egion
Fc
Z Variaote
\regton
L Constant
regionComplement
binding egion
Fn ranonlnr
binding egion
IgA is the main Ig in secretionsand is usually a dimer(2 immunoglobulins)wrth the J chain and a secretorycomponent,which is actually ust apieceof the epitheli-ai or iiver ceil receptorattachedo locally produced gA.It is the main Ig secretedn breast milk. IgA doesnot
acfivatecompiement.
IgM is the first Ig subtypeproduced n an rrfection. It isa monomer on the cell surfacebut js secretedas a pen-tamer (5 immunoglobulins), n which each monomer sconaected y a J chain. gM is useful i:r diagnosisof therecent onsetof iilnessesand can help distinguishacuteversus chronic infection.Because gM is a pentamer, tis thebest antibody or complementactivation.
IgE is the Ig with the lowest concenftation n normalserurnbut is a major factor in many allerglc conditions,including asthma,allergic rhinitis, atopic dermatitis,andfood allergies.
IgD is found in traceamountson adult B cells, and itsfunction is asyet undefined.
The vanability in the speciicities of the anhbodies sdue to the rearrangement f several egions of the anti-body genes, uchas he constantand variable egions.
Immunoglobulins(antibodies)bind specific antigens nthe Fab region and then activateeithercells or comple-ment (discussednext), by means of the Fc region, todestoy tle antigen-bearingmateriai.
OVERVIEWThe 3 Complement Pathways
First a brief review of the compiement system. SeeFigure9-2.
The complementsystem s a core component of boththe irurate and adaptive immune responses. It is nowknown to have ] main pathways: classical, Iectin,
and alternative. Although they ali start with difier-ent mechanisms, hey all end up performing the seme
I Alternative
C1;Cab+C2a-.I a--
Factor
t t l' t ' f t . r - .n
Membraneattack omplex
function--opsonizing target cells with C3b and thenforming the "membraneattackcompiex."
Classical Pathway
The immunoglobuiins (usually IgG and IgM) activatethe ciassicalpathway:C1 complex (with q, r, and s sub-units) nitiates his responsewhena C1q subunitattaches
to antibody a an antigen-antibodycomplex.C1q bindsto theFc portion of at least2 IgGs (or 1 IgM pentamer),or it binds to the surfaceof the pathogen tself. Bindingchanges he conforrnationof the Clq. This activatedClwiil cleavemany C2 andC4, subcomponents f which(C2a andC4b) combine and form C4b2a ("C3 conver-tase"),which in turn activatesmany C3.
Again: 1 IgM pentamercan initiate the classicalpath-way, but it usuailytakesat least2 igGs.
Lectin (or Mannose-Binding) Pathway
Lectins (mannose-binding ectin [MBL]; also calledmannose-or maman-binding proteins) bind mannose
on the surface ofpathogens.Then associated roteasescleave C2 and C4, and fi.rther steps are similar to theclassical pathway. These MBLs are produced by anacute-phaseesponse nd are airly nonspecific.
Alternative Pathway
C3 also is activated by the altemative pathway. C3combines with a factor "8." This complex thenactivatesmore C3 aad actorB, causinga cascade, hichis normally kept under contol by *re inhibitory regula-tory proteins"H" and "I." Both grarn-positiveandgram-negative celi walls directly activate the altemativepathwayby spontaneous ieavageofC3.
A crculatmg bacterium coatedby C3b wiil be recog-nized, removed, and destoyed by Kupffer cells in theliver.
Gommon Terminal Pathway-
Membrane Attack Complex
C3, when combined with either C4b2aor factorB, willactivateC5, which causes heformationof a C5-6-7-8-9membrane attack compiex QaAC). The MAC canpokeholes i:r bacterial ceil membranes.
O 2011 Medstudy-Please Report Copyright Infringementsto [email protected]

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 6/12
. ls hereditary ngioedema n autosomal
dominant r autosomalecessive isorder?
. Whatcauseshereditary'angjioedema,nd how
does i present?
. Terminal omplement eflciency an lead o
increased nfeciionwithwhich organism?
. Whatdoes he CHSO ssaymeasure, nd when
is i] used?
HEREDITARY OMPLEMENT
DEFICIENCIES
Hereditaryngioedema
Hereditary angioedema HAE) is an autosomaldomi-
nant disorder.It is causedby a decreasen Cl inhibi-
tor(Cl-D.{H) function with a secondarilydecreasedC4
(becauseof ongoing consumption).Patientscan have
eithera decreasedC1 inhibitor enryme(85%,Tlpe I) or
a non-fu:rctioningCi inhibitor enzyme 15%' Tlpe II).
Patients have recurrent non-pitting edema with each
episode, lasting 1-3 days. Unlike angioedema and
urticana caused by immediate hlpersensitivity reac-
tions,hereditaryangioedema oesnot causeurticaria or
itching.
Even minor traumacanprecipitateattacks Attacks may
i:rclude la4mgeal obskuction and very often affect the
GI fuact, causilg severe abdominai parn. It does not
respondto epinephrine.Fresbfrozen plasma is protec-
tive when given before tauma, such as dental surgery.
Androgens ncreaseC1-INH levels and decrease well-
ing episodes This was the only available preventive
medication until recently. New therapies approved
inciude piasma-derivedCI-NH for fV use and a kal-
1ilc'ein inhibitor for SQ r:rjection for acute attaci<s.A
bradykinin receptor antagonist is avaiiabie in Europe
andmay soon beavailable n theU.S.
Screen by checking C4 levels. Diagnoseby decreased
CI-INH fi:nctionai assay. f the CI-INH level is aiso
low, then it is Type I HAE. If the C1-I|{H levei is
normal, it is due to anon-functioningCl-I}'{H enz}Tne,
and it is Type Ii HAE.
C1, C2, and C4 DeficiencieS'
CL, C2, or C4 deficiency causesdecreasedactivation
of complementvia the ciassicaipathway. Most of the
complem€ntproteins are inherited as autosomalreces-
sive genes.Although the alternative pathway wiil take
up some of ttre slaclg thesepatients still have recur-
rent sinopubnonary infections (and ear infections when
young) with encapsulated bacteria. In patients with
1 abnorrnal gene, complement blood levels are about
7/2 rormal. In these patients, there is an increased
IMMUNE COMPLEXES
incidence of rheumatoid diseases----€speciailyLEI
C2 deficiency s the most common deflciency n Nonh
American Caucasians;hus, consider t rn pahentswith
eariy-onsetSLE. This is becauseeither heseare mpor-
tant in removing immune complexes,or their genesare
somehowphysically associatedwith genes hat control
immune responsiveness.
C3 Deficiency
C3 deficiency (complete absence) results in severe
pyogemc tacterial) infections.
Cs-C9 Deficiency
C5-C9 MAC deficiency is also called terminal com-
plement deficiency. It results in increased {eisseria
meningococcaVgonococcainfections (especialiymen-
ingitis or septicemia).Screen or terminal complement
deficiencywith CH50 (seebelow). Specificdiagnosis s
madeby assayof thesecomplementcomponents,
cH50
The CH50 assa.ymeasuresh,e otal eomplement
hemoll4ic actrvity of the classicalpathway.A norrnal
test shows hat ail factors(C1{9) arepresent.Krrow
that a CH50 assaysti11 an be normal even f C3 or C4
are significantly lower than normai becausenormal
levels of C3 and C4 are far higher than required.
CH50, C3,andC4 aresometimes sed o foliow
disease ctivityof SLE. The CH50 is a goodscreen
for compiementdeficiencies. f the CH50 is very loq
check individual complementcomponents C1 through
C9 ievels) or specifc deficiencies.
Immune compiexes (ICs) (i.e., antigen-antibody
complexes) fonn during normal, day-to-day immune
surveillance,and then are removed from the serum.As
they forrn, complement s usually activated and a C3
component C3b)wiil attach o the complex.
This C3b-IC entity will be recognizedby, and attach o,
the complement eceptor.The main complement ecep-
tor is CRl. whrch is found in abundanceon RBCs.
The immune compiexesare scrubbedoff the RBCs by
the Kupffer celis in the liver (remember Kupffer cel1s
also remove and destroy C3-coatedgram-positiveandgram-negativebacteria-see above). If there are any
defects in this elimination process, he immune com-
plexesmay build up.
Hepatic vein tlrombosis @udd-Chiari slmdrome)and
cirrhosis resuit in decreased clearance; paroxysmal
nocturnal hemoglobinuria @NIf results in decreased
binding; and SLE results n a decreased mountof CR1
on the RBCs. So each of these will causeincreased
immune complexes n the serum.
O 2011 Medstudy

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 7/12
-$ HYPERSENSITIVITY REACTIONS
irnmune complexes activatecomplement o form C3b,
wluch attaches o theFc portion of the IgG. This main-tains the solubiiity of the compiexes n the serum andprevents hem from cross-connecting nd precipitating.
IgA doesnot activate he classicalcomplementpathway,so thereforemay be more susceptible o precipitation;
this causesmmune complex deposition manifestations
when high levels build up. More in Type III hypersensi-tivity below
OVERVIEW
A11 hypersensitivity reactions are immune-mediatedtissue njury resulting in a variefy of diseases: llergies,autoimmunedisease,and a variety of other inffamma-tory diseases.
There are 4 typesof hypersensitivity eactions per Geiland Coombs):
Type I: IgE mediated. mmediate(anaphylactic,atopic)
Type II; IgG or IgM mediated.Cytotoxic
Tlpe II I: knmune complex(antibody-antigen)mediated.
Type fV: Cell-mediated.Delayed ype
TYPE : IMMEDIATE YPERSENSITIVITYREACTION
Allergies
The "ciassic" ailerg:es are Type I hypersensitivity
reactions. Examples: Hives/urticariE allergrc rhinitis,allergic asthma, eaction to insect stiags, drugs@CN,etc.), and oods.(peanuts, ggs,shelli0sh, tc.).
Type l: Acute Response
The acute phaseof immediate hlpersensitivity reactionsoccurs within t hour after exposure-usually withinmilutes. Mast cell degranulation especiallyproducinghistamine) s the causeof the symptoms.This reaction sIgE-mediated.These gE antibodiesare antigen-specificand occur only in response o previous exposure o thesameallergen.
The base Fc portion) oflgE antibodiesbinds o arecep-tor on mast cells.This receptor s not specific,so there
are many IgEs (each with its own antigen specificity)bound o amast cell. No reactionoccurswhenIsE bindsto themast cell.
A certain allergen interacts with the allergen-specificreceptoron the Fab portion of IgE, and, whenthe sameantigen reacts with more than 1 IgE-thereby interlink-ing the 2-the mast cell is stimulated to degranulateand reiease histamine and also begin syntbesizing andsecrctng other mediators Qeukotiene Ca, PGD2, andcytokines). Histamine is responsible for most of theacute s)mptoms.
Mastcellsalso elease therproductshathavechemo-tacticeffects, ndsomeof themareenzymesch1r:rase^- l
k*+^^^\4r1u uJPL45rr.
Review: Histami:re interacts with 3 receptors: H,, H",hnd H3.Activation of H; receptorcauses he wheal andflare, bronchoconstriction, and pruritus. H7 receptoractivation results in, of course, ncreasedgastric acidsecretion. H3 activation causes decreasedhistaminesynthesisand release negative eedback).
Type l: Late-Phase Response
Late-phase esponse: to 12 hous after the immediatereaction s a late-phase esponse LPR).This lastshoursto days and usuaily causesan eosi:rophiiic nflamma-tory nfltate. Typically, thereis an induration that haserythema, burning, and is occasionally pruntic.The LPR is one of the causesof nonspecific airwayhypersensitivity.
The LPR is a resultof the rutial, immediate gE reactionstimulating he synthesis f cytokines.Basophilsmay bernvoivedwith the late-phaseesponse.
The probabiiify of a LPR increaseswith the seventy ofthe acutereaction.
Type l: Anaphylaxis
Aaaphylaxis s usuaily an extreme gE-mediated orm ofimmediatehypersensitivityreaction,but it can also becaused y the by-productsof activatedC3,4, and5 (ana-phylatoxins), which, like IgE, cause he releaseof thecytoplasmic granulesfrom mast cells (+/- basophils),The released cl4oplasmic granules cause an immedi-
ate hypersensitivity reaction. ASAAISAIDs, physicalstress,and certain chemicais suifites hat causeasthma;opiates) an becauses fnon-IgE-mediatedanaphylaxis.
The most common causesof anaphylaxis are drugs,foods, and insect stings. Personswith asthmaor heartdiseaseare at gteaternsk for fatal anaphylaxis.Bees,wasps,andyellow jacketsare commonculpritsof insectsting anaphylaxis.Arry insect sting can occasionallycausea large iocal reaction.This doesnot increase herisk of anaphylaxis,and further workup is not necessary.Of course,anaphylaxis tself does equire workup-usu-ally skin tests.
Note that ASA-induced anaphyiaxis s a separates1.n-
drome from ASA-induced urticana, and both of theseare separate rom ASA-induced asthma,which is oftenassociated ith rhinosinusitisand polyps.
Type l: Treatment
Notes on H, antihistami:res:Cyproheptadine decreasesgrowth hormone secretion.Avoid most autihistamines npregnantpatients;when needed,usehydroxyzine, diphen-hydramine,chlorpheniramine,and ripelennamine.
@2011 Medstudy-Please Report Copyright lnfringements io [email protected]

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 8/12
HYPERSENSITIVITY REACTIONS
decreased ascularpenneability.The effect of eprneph-rine is bluntedm pahentson beta-blockers, o thesearereiatively contaildicated in patientsat nsk of anaphy-lactic reaction.Glucagon or vasopressinnjectionsmaybe used n patientson beta-blockersduring anaphylaxisif theresponseo epinephnnespoor.
ryPE ll: GYTOTOXICYPERSENSITIVITYType II reactionsoccur when an IgG or IgM antibodybrnds o a fixed tissueantigenor ceil receotor.Theseareautoantibodies,
Binding of the antibody results :r targetcell destructionby variousmeans:
. Compiementactivationmay causecells to be lysedbythemembraneattack complexMAC, discussed npage9-4)
. Compiementactivation may result n opsonizationfrom the productionofC3b. Phagocytes ave areceptoror C3b.
.Phagocytes lsohave a receptor or the Fc portion ofthe antibodiesand hereforemay attackantibody-coatede11s.
Examplesof target ceil receptors:
Targetcell Disease
PlateletsRBCs
WBCs
Thrombocl'topenia
Autoimmunehemoiltic anemta
Leukopenia
Examplesof target .xed tissuea:rtigens:
Tareet4ntigen DiseaseComponentof thebasement Anti-GBM disease
membrane 1<rdtey nd ung)ACh receptoron muscie cells Myastheniagravis
ryPE ll l : IMMUNECOMPLEXHYPERSENSITIVITY
Aaytime you see a vasculitis,think of Tlpe III h1,per-sensitivityreaction.Type II reactionsare alsoseenn Igautoimmunediseases nd reactionso drugs.
lmmune complexes ICs) form when antibodiescombinewith antigen (self or foreign). A hlpersensitivity reactionoccurs when antibody (usually IgG) reacts with a targetantigen to forrn ICs, which precipitateand activate com-plementwith subsequent mall vessel nflammationandnecfosls.
Remember: ustbecause n antibody eactionoccursandICs are ormed, t doesnot necessarilymean herewilt beprecipitation. Significant precipitatron occurs only whenthere s slight antigen excessn relation to antibody.
When the antibody response initiates, there is a hugeexcess f antigens ompared o antibodies Ag:Ab >> 1).The ICs tlat are formed are smail, soluble, and quickiycieared.
a#%uiz. Whatprocess ausesan immediate
hypersensit ivityeaction?
. Whendoes he atephaseof Type
hypersensitivityeactionoccur?Why does toccur?
. Knowhow o treatanaphylaxis-bothmiidan dea\/a re
. Whichanti-hypertensives relatively
contraindicatedn someone t risk oranaphylaxis? hy?
. At whatantigen;antibodyatiodoesmost Cprecipitationccur n a Type ll hypersensit ivityreaction?
Treatrnent for immediate hypersensitivity diseases:
Avoidance of the allergen, and give Antihistamines(occasionally steroids) and AJiergen-specific mmuno-therapy(3 As). The immunotherapy may take6 monthsto show an effect, with maximal effect in 3 years.
Patientsat high risk, such as beekeepers, hould also getar epinephrineauto-ir ection(EpiPen@,win-Ject@)it.Effeciive immunotherapycauses n ncrease n T reguia-tory cell secretionof IL-10 and blocking antibodiesofthe IgG isotype, amongmany other effects.Only reac-tionsthat are gE-mediatedbenefit rom immunotherapyIrealment.
Treatment or anaphylaxis
. With mildto-moderate symptoms i.e.,with urticanabut no severehypotension),give epinephrine1:1,000
0.24.5 ccIM (maxrmumdosage ,5 mg, 0.5 ccof1:1,000: 0.5mg; donotgive V); repeat very15-20miautes asneeded. f thecauses antigenicmaterialinjecied nto an extremity (e.g.,beestrng),placeatoumiquetproximai to t}tesite, nject 0.15-0.3 cc ofeprnephrine1/1,000SQ at the inoculation site, andremoveany stiager without compressing hepoisonsac.Start anfV.
. ParenteralH, andH, antagonistsusuailydiphenhydramiaeand cimetidine,respectively)mayaisobe given. In-ha1ed lbuterolmay be given ifbronchospasm evelops.Steroidsmay helppreventthedelayed late-phase)eacrions.
'For significant
hlpotension,give
epinephrine1 0,0005 cc fV q 5-10 mrn(5 cc of i :10,0000.5mg), anormal saline bolus,and (lastly)dopamineasneeded.
' fV steroidsarenot effective or acutecases ut mayabortor decreasehe delayed esponse.
Personswith anaphylaxis rom iasectstings shouldsub-sequentiy eceive mmunsft s1apy.
Epinephrine causesalpha and beta adrenergic effects,resulti:rg in bronchial relaxation, vasoconstriction, and
@ 2011 Medstudy

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 9/12
OTHER URTICARIA
Within 1-2 weeks, as exceedinglymore antibodiesare
produced,a pourt is reachedwhen there is only slight
antigenexcess, nd the ICs interlaceand becomebiggerand lesssolubie. Theseprecipitateur the small vesseis
and activate compiement,which starts a cascade aus-
ing the releaseof more cytokines and the gathenngofmore nflammatory cells. This processultimateiyresults
in necrosisof the smallvessels.The pathoiogichallmarkskin sign is leukocytoclasticvasculitis (hemorrhagic,
urduratedesions).
As the antigens cleared,here comesapoint when hereis antibody excess. he formedICs are arge andquickly
clearedby crculatrng phagocytes macrophages).
There are 2 animal models or what happens linicaily:
1) Serumsictrqiessa systemic eaction):A largeamountof antigen s injected i:rto a nonimmunizsd animal,and you seea necrotic vasculitis similar to the onejust discussed.
2) Anhus reaction(a locai reaction):The animal s firsthyperimmunized,so there are many circuiatingIgGantibodies,and hen given a small intraderrnal njec-tiorr of the target antigen.All reaction o,',-:urs t th€injection site, where there are many ICs made-
inducing the complementcascade nd nflar-nmation.Within 4-6 hours,a painful indurated esionappearsandmay progress o a sterile abscess.
Here are some examplesof diseases n which Tlpe trIreaciionplays part. .
Autoimmuns diseasesandassociated ntigen/s):
. SLE (nuclearmaterialssuchas ds-DNA, Smithantigen,and many others)
. Hashimoto hyroiditis (thyroglobulin)
. Perniciousanemja inu'insic actor)
. Rheumatoid arthritis (rheumatoid factor)
Extemal antigens:
. Hepatitis-antigen-associatederumsickness
. Tetaausand diphtheria immunization
. Local i:rsuiinreactions
Serum sicicress and Arthus Tlpe itr hypersensihvityreactions are usually self-limited, and patients usuallyrecover ully. Occasionally, orticosteroids regiven.
Treatnrentof autoimmunediseasess covered n othersections, articularlyRheumatology.
Treablent for extemal antigen reaction i.s to stop theexposure o the antigen.
TYPE V: GELL-MEDIATEDHYPERSENSITIVITY
Type V
Freviouslyensitized celis nteractwith an antigen,
causingan inflammatoryreaction.The reactionpeaks n
24--12 hours-hence the common name; delayed-fype
hypersensitivity.
Tuberculia sensitivity and some types of contact
dermatitisare exampiesof delayedhypersensitivity.
Don't get this "delayed-typ"" fV hypersensitivity eac-
tion confrrsedwith the "latephase"of TypeIl
TYPEV:AUTOIMMUNETIMULATORYHYPERSENSITIVITY
The term Type V hypersensitivityreaction is used bysome o indicatewhen the autoimmunegG hasa stimu-latory effecton a receptor asdistrnguishedrom Tlpe II,which is destructive). t is not part of the Gel1-Coombsciassification.Arr example s Graves disease,where anigG stimulates he TSH receptor.
Besides he above ailergen-mediated rticaria,there areseveralother causes furticaria:
. Acquired cold urticaria is usualiymediatedby eithercryoglobulinsor IgE. Shockmay occur f thepatient
is immersed n cold water Testwith a S-minuteskinice-cubechallenge.
. Familial cold urticaria is an autosomaldomi:rant,inherited inflarnmatory diseasecharacterizedbyurticaria,myalgias, ever,and oi:rt pain aftercoidexposure.
. Cholinergic urticaria isprecipitatedby heat(e.g.,hot shower,hot day,exercise).Usuallypresentsas
punctate lesionsthat are very pruritic.. Immediate pressure urticaria is seenwith severederuatographisrn andmay deveiop around thewaistline.
. Delayed pressure urticaria rypically causes weilingandbuming (not itching) of palins andsolesseveraihours after carrying a load for a while or walking longdistances.
. Autoimmune urticaria occurswhen autoantibodiesto the IgE receptoron mastcells ink the receptorsandcausedegranulation.
. Chronic urticaria occurswhen hives ast morethan6 weeks.Most often the underlyurgcause s unlcf,rown.In somepatients, hyroid disease an causechronic
urficaria, so remember o check or thyroid functionand thyroid autoantibodies.
. Urticarial vasculitis can cli:ricallyresemblechronicurticaria.However,patients eport hives asting> 24 hours n a fxed location(in contast to chronicurticaria, which resoives in minutes to hours ormigrates continually). Other red flags includeresidual ecchymcisis, yperpigmentation, rpetechiae.Diagnosewith skin biopsy.
@ 2011 Medstudy-Please Report Copyright lnfringements to [email protected]

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 10/12
Q-d1%ulEA tubercuiinest s an exampie f which ypeof
hypersensitivityeaction?
What s the difference etweena Type l and aTypeV hypersensitivityeaction?
How s he cholinergic rt icariaeaction
init iated?
. Urticaria pigmentosa is discussed elow under'Mastocytosis."
Allergic rhinitis; May be seasonal, rovokedby season-ally presentpollens, or perennial,usualiy provoked bydustmites,molds,or animaldanders.Once nitiated, hepatient has a nonspeciflchypersensitivify o many irri-
tating strnuli. Eosinophils will appearon nasal smearonJy f the patient is symptomatic.Patientswith peren-
nial (year-round)allergicrhuritis have a lugh eosilophilcount n secretions ear-round
NARES: Patientswith "non-allergicrhinitis with eosin-ophiiia syndrome" have chronic nasal congestion (butnot sneezingor rhinorrhea) and, like perennial allergicrhimtis, eosinophilia.of he nasal secretions.Patientsdonot demonstrate ensitization o allergen,eitherby skinprick test or RAST test (Skin Testrngvs. RAST onpagee- ).
Vasomotor rhinitis: Tlus is an interestingreaction toneurogemc/vagaistimuii. Patients will have sneezing
attacks,followed by nasai congestion on exposwe tocold,sunlight,or various other stimuli.
Rhinitis medicamentosa s rebound congestioncausedby prolongeduseofvasoconstrictingnasal drops (phen-ylephrineor oxlmetazoline).
Other possible causes of chronic nasai congestionincludedeviatedseptum, oreignbody, umors, anddrugreactions especiallywith propranololandalpha-methyl-dopa).Persistentasal ongestionmay accompany reg-nancy(rhinitis of pregnancy).
Treatrnent Hl antihistamines are first-line theraovfor allergrcrhinitis. However, intranasalsteroid spraysare the most effective medicine for allereic rhinitis.Iatranasal steroid sprays are effective in iil types ofrnrnltls;cromolyn only in the allergic 5pe.
RH N TIS
*?Early-generation a6ifol5famines (diphenhydramine,fir'chlorphenirarnine, and hydroxyzine) have the major
. sideeffectof sedation.This is due o the ability of thesegrygs o cross treblood-brainbarrier and nteractwith4opamiae,serotonin,and acetylcholile receptors n the
The interaction with acetylcholine receptors alsoin biuny vision and dry mouth. 2"d generation
antihistamines cetirizine,fexofenadine,oratadine,des-ioratadine)do not cross he blood-brainbarrier as muchand cause ittle to no sedation.
The etiology of exercise-inducedasthmais uncertain.
The earlyresponsemay be due o mastceil degranulationia the airways or excessivecooling. The late response(again:no PGD, is generated"rnhe ateresponse) ausesa dramatic ncrease n inflammatorycells (often eosino-phils) n theairways.Swimmrng s oneofthe leastasthma-inducing exercises.
Sulfitescan exacerbateor precipitates1'rnptomsm sus-ceptiblepatients.Treatrnents coveredur thepulmonary
sectron,but to simpirfy and summarizethe importantpoints bneffy, monitor andfollow controi using the ruleor zs.
In the2007 guidelines, he 2 major componentso assessfor contol are mpainnent (symptoms)and risk (admis-
sions): f patientshavemore than2 asthmas)anpromsaweek during the day or more thaa 2 syrnpt,:rrs (impair-ment) a month during the mght, they are uncontrolledand needto step up ther regimen,accordingto guide-line-specific recommendations. f they have had 2 ormore ER visits/admissions risk) for astlma, they areaiso uncontolied. Patientsshouldbe followed approxl-mateiy every2 months.
The categoriesof control that shouldbe appiied at eachvisit:
1) Conh-olled
2) Not well contolled
3) Very pooriy controlled
Again, if patients are not controlled, they need inten-sification of treatment. This can inciude treatmentofcontributory comorbid conditions ike rhimhs and sas-troesophagealeflux.
Complete nformation is ur thePuL:ronarysection.
Pneumonitis:Hlpersensitivity pneumonitis is immunecomplex-mediatedand cel-mediated(Types tr and .Acute bronchopulrnonaryaspergillosis ABPA) is IgE-mediatedald immune complex-mediated TypesI anditr). Both
respond o glucocorticoids. n neither one ofthesewould you give allergy njections.Why? Answer:
' Hlpersensitivity pnermeliljs is not lgE-mediated.. ABPAmay be worsenedby aliergy njections-they
could.induceproductionof moreAspergilizs-immunecomplexes.
Botl arediscussedn thePulnonary section.

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 11/12
9- l 0 SKIN TESTING VS. RAST
In vitro tests for antigen-specificgE in serum include
radioailergosorbent est EAST) and fluorenzymeim-
munoassay CAP-FEIA). Skin testurg is more specificandsensitive,so useblood testing only if theskin testingcennotbe done,aswhen he patient:
'Has extensiveskin disease. Has dermatographism. Has anaphylactic sensitivrty to the ailergen
' Is on antihistaminesthesedepress he skin test
response),wb-ichcarurotbe withheid for 1-2 weeks
Mastoclosis is a rare disorder characterized y abnor-mal mast cell proiiferation and accumulation n variousorgans.The degreeof involvementdetermines heextentof tle disease.
There are cutaneous, ystemic,and malignant lypes ofmastocytosis:
. Cutaneous mastocytosis esults rom increasedmastcells n the dermrs. t causes rticariapigmentosa,
which is diagnosed y formation of a wheal on gentle
stoking of themacuie@arier sign).. Systemicmastocytosisalso has :rcreasedmast celis
in the tissues so patientsalso haveabdominal
symptoms, atigue,andepisodes hat mimicanaphylaxis,n addition o urticariapigmentosa).
. Malignant mastocytosiscauses everesystemic
symptoms,but oftenno skjn changes.Signs urcludehepatosplenomegaiynd ymphadenopathy.
Treatrnent:Stay away from cold, heat, alcohol,ASA, andopiates.Orai ffomoiyn may help for GI symptoms.Variouschemotherapyegimenshave beenused n the treatnent ofsystemic andmalipant mastocytosis.Unfodunately, che-motherapyhas not beenparticularly successfiil.
There are many diseasesassociatedwith certainHLAantigens. This makes sense becausethe HLA com-piex is the backbone of immune surveillance.Manyrheumatic disorders are associated with HIA-F.27,espeoiallyanfylosing spondylitis,acuteanterioruveitis,Reiter
syrdrome,psoriatic spondyloarthropathy,
andjuvenile rheumatoid arthritis. But not aduit rheumatoid
arthritis (this is associatedwith the DR4 and DR2 anti-gens-see Rheumatologysection).
IMMUNOGLOBULINDEFICIENCIES
See also Hereditary ComplementDeficienciespage -5 .
Congenital agammaglobulinemia (: "Bruton""X-iinked" = )CLA): Patients have i:rcreased sus-
ceptibility to pyogenic and encapsulated organisms(Staphylococcus, Streptococcus, meningococcus,Haemophilus).Hence, they have recurrent sinopuhno-nary and ear nfections.They usuallyhave normal resis-tance o fungi (i.e.,will not get chronic candidiasisas do
patientswith HIV/AIDS ), most gram-negativeorgan-isms (see T-ceil functron on page 9-2), and viruses.The oniy exception s that )il.,A patientsare susceptibleto enteroviral infections andGiardia.
Prognosis s good if the condition s caught early.Checkail of the patient'sbrothersand the maie cousinson themother'sside.
Diagnosis: g assayshowsvery low IgG and no IgA, M,E, or D. Therearealso no B cells (i.e.,no SmIg*celis).
Treatments directedat replacing mmunogiobulinswrthexogenousWG or SQIG.
Common variable immunodeficiency (CVID):
Deficiency of IgG, IgA, and/or gM. Like XLA, patientshave decreased esistance o encapsulatedorganisms(5. pneumoniae, H. infueraae). They have recurrentsiropulmonary infectionsald bronchiectasis. hey alsotendto get giardiasis.There s an increasedncidenceofautoimmunedisease ndmalipancy.
Diagnosis:Ig assayshows low IgG, igA, andlor IgM.Unlike )CLA, CWD patientshavematureB cellspresent.
Treatment s directedat replacing mmunoglobulinswithexogenousVIG or SQIG.
IgA deficiency: The most common Ig deficiency. ts
incidence s as high as i/600 Most patients are asymp-tomatic. It is associatedwith only a siightly increasedincidence of autoimmunediseases.SomepatientswithIgA deficiency have recurrent sinopubnbnary rnfec-tions, recurrentgiardiasis,and aa associationwith mul-tiple autoimmune diseases, uch as celiac diseaseandHashimoto's.
For these patientswith recurrent infection, teat withprophyiactic antibiotics.This is discussedmore in theInfectiousDiseasesection.
Wiskott-Aldrich syndrome: Low IgM and elevatedIgA and IgE. The triad of findings is eczema,_immuno-deficiency, and
$uombocytopenia.Remembering that it
is X-linked makes or a nice maemonic ("Wisk through, r F iF i l . . \
the HflT"). It can be treated successfirllywith bonemarrowtranspiantation.
CELL.MEDIATED EFICIENCY
DiGeorge syndrome (congenitai thymic hypoplasia) is aT-ceil deficiency due to an early intauterine malfonna-tion of the embryo that can affect severaltissues, nclud-ing the thymus, the parathyroids, the heart and great
@2011MedStudy-PleaseReportCopyrightnfringementso [email protected]

8/13/2019 medstudy book
http://slidepdf.com/reader/full/medstudy-book 12/12
CANCER IMMUNOTHERAPY
e*&uie. What does a RAST estmeasure?
. What are thb 3 different ypesof mastocytosis,and how do they preseni?
. Urticariapigmentosas seen n whichdisorder?
. Which mmune eficiency as no matureB cells?
. Whai s the mostcommon mmunoglobuiindeflciency?What are ts symptoms?
. What s Wiskott-A ldrich yndrome?
vessels, nd he face.These nfants may presentn hlpo-calcemic etanyl There s awide range of symptomsandvariabledecreasen T-ceil function reiated o thevariabledecreasen thymic tissue.Lr manypatients,amicrodele-tion in 22qll canbe demonstated.For the mostseverely
affected nfants (with no thy.rnusor T cellsl), teatrnentwrth thymus tansplantation is under investigation. Anicern:remonic or tlese fi:rdings s "DiGeorgeCATCH-22" (Qardiac, Abnormal facies, lhyreic hypoplasia,Cleft lip, Hypocalcemia,22 cbromosome).
COMBINED EFICIENCIES
Severe, combined irnmunodeficiency: A deficiency innumbers or function of both T and B cells. Either auto-somal ecessiveor X-Iinked. Aiways fatal unless reated.There are several types, and some can be teated withcompatibiebone marrow transplantation.
Ataxia-telangiectasias an autosomal ecessivedisorder
causingboth celluiar and ig deficiency. This results nrecurent silobronchial infections, bronchiectasis,andprogressive elangiectasias. hesepatientsalso have aprogressiveneurologic deterioration of uncertain etiol-ogy, characteized by cerebeilar ataxia and progressivementaldeterioration.
Know the following:
'lnterferons, in general,are cytostatic not 'cidal) andoften cause q4rptoms similar to a severeviralsyndrome.
Alpha-interferon hasbeeneffectivelyused n hairy cell leukemia.
' Tumor necrosis actor isproducedby activatedmacrophages. t athactsPMNs and causesvasodilation.
'Monoclonai antibodiesareused o carry chemothera-py agentsor isotopesto the hrmor.
' Iaterleukin-2 is a lymphokine that activates henaturalkiller T cells; test results arepromising for teatingmeianoma andrenal csll cancer.



















![[Medstudy] MedStudy Internal Medicine Pulmonology,(BookFi.org)](https://img.pdfslide.us/doc/110x75/577cc6c01a28aba7119f0e58/medstudy-medstudy-internal-medicine-pulmonologybookfiorg.jpg)


![Book - Titanic - Book[1]](https://img.pdfslide.us/doc/110x75/563dbaf8550346aa9aa92bb6/book-titanic-book1.jpg)