Embed Size (px)
Citation preview

1
Medicine Review Course 2016 Hypertension
- Insights from Recent Trials
Dr. Kwek Jia Liang
Associate Consultant
Department of Renal Medicine
Singapore General Hospital
24 July 2016

2
Disclosure
• None.

3
Content
• Timeline in Hypertension
• Factors to consider in Hypertension management
• Landmark trials in Hypertension
• JNC 8
• SPRINT
• HOPE-3
• PATHWAY-2
• Conclusion

4
Timeline in Hypertension
http://www.history.com/news/memo-from-1944-warned-that-fdr-would-likely-die-in-office
President Franklin Delano Roosevelt 1882-1945

5
10-Year Risk for Coronary Heart Disease
Framingham Risk Score
(Age, Total Cholesterol, HDL, Smoking, SBP)
www.nhlbi.nih.gov

6
10-Year Risk for Coronary Heart Disease
Singapore MOH CPG (Adapted version, 2011)
MOH CPG Screening for CVD and Risk Factors 2011

7
Factors to consider in Hypertension
• Treatment initiation
• Blood pressure goals
• Dietary Intervention
• Comparison of antihypertensive agents
• Special populations
– Diabetes mellitus
– Elderly
– Chronic kidney disease

8
Outcome Measures in Hypertension Trials • Major cardiac adverse events (MACE) – not standardized
• All-cause mortality, cardiac death, non cardiac death
• Myocardial infarction – fatal, non fatal
• Angina, revascularization, heart failure, hospitalization for
heart failure
• Stroke – fatal, non fatal
• End stage renal failure, doubling of serum creatinine
• Adverse effects to therapy

9
J Curve… or not?
Messerli et al. J Am Coll Cardiol 2009;54:1827-34 Hansson et al. Lancet 1998;352(9118):1755-62

10
Landmark Trials in Hypertension
Saklayen et al. Front Cardiovas Med 2016 Feb 23;3:3

11
Factors to consider in Hypertension • Treatment initiation - VA, MRFIT
• Blood pressure goals - HDFP, HOT, SPRINT
• Dietary Intervention - MRFIT, DASH, MRC, PREDIMED
• Comparison of antihypertensive agents - TOMHS, ALLHAT,
ANBP II, ASCOT, ACCOMPLISH
• Special populations
– Diabetes mellitus - UKPDS, ACCORD
– Elderly - EWHPE, SHEP, HYVET
– Chronic kidney disease - (MDRD), AASK

12
Definition of hypertension
Definition Systolic BP (mmHg) Diastolic BP (mmHg)
Normal BP
<120 <80
Prehypertension
120-139 80-89
Stage 1 Hypertension
140-159 90-99
Stage 2 Hypertension
≥160 ≥100
Based on average of 2 or more properly measured readings at each of 2 or more office visits after an initial screening
Chobanian et al. JNC 7.JAMA 2003;289:2560

13
Definition of hypertension
Mancia et al. 2013 ESH/ESC.Eur Heart J 2013;34:2159-219

14
JNC 8 (2014) - Focus 1. In adults with hypertension, does initiating antihypertensive
pharmacologic therapy at specific blood pressure thresholds
improve health outcomes?
2. In adults with hypertension, does treatment with
antihypertensive pharmacologic therapy to a specified blood
pressure goal lead to improvements in health outcomes?
3. In adults with hypertension, do various antihypertensive
drugs or drug classes differ in comparative benefits and
harms on specific health outcomes?
Bauchner et al. JAMA 2014;311(5):477-8

15
JNC 8 (2014) • *General population ≥60 years old, to treat to a goal of BP
<150/90 (Strong recommendation)
• General population <60 years old, to treat to BP <140/90
(Strong recommendation for DBP target 30 to 59 years old,
expert opinion for SBP target)
• CKD, to treat to BP <140/90 (Expert opinion), should include
ACEi or ARB to improve renal outcome (Moderate
recommendation)
• Diabetic, to treat to BP <140/90 (Expert opinion) James et al. JNC 8. JAMA 2014;311:507

16
Controversy around JNC 8 • JNC 8 members were commissioned by the National Heart,
Lung, and Blood Institute (NHLBI) in 2008
• In 2013, NHLBI announced that it would no longer develop
guidelines
• JNC 8 group declined partnership with AHA/ACC
• In December 2013, JNC 8 group published independently in
JAMA
• In 2015, AHA/ACC/ASH issued its scientific guideline for
hypertension

17
Controversy around JNC 8

18
Other Guidelines on BP Targets
Guidelines General Diabetic CKD Elderly
JNC 8 (2014)
<140/90 <140/90 <140/90 <150/90
ESH/ESC (2013)
<140/90 <140/85 <140/90 (<130/90)*
<150/90 (<140/90)*
ASH/ISH (2013)
<140/90 <140/90 <140/90 (<130/80)*
<150/90
NICE (2011)
<140/90 <150/90 (<140/90)*
ADA (2016)
<140/90 (<130/80)*
NOT <130/70
KDIGO (2012)
<140/90 (<130/80)*

19
Is the picture going to get any clearer?

20
Recent important hypertension trials
• SPRINT (NEJM 2015)
• HOPE-3 (NEJM 2016)
• PATHWAY-2 (Lancet 2015)

21
SPRINT
Study Design
Multicenter, open label, randomized controlled trial Target SBP<120mmHg versus SBP<140mmHg Outcome – Primary composite outcome of myocardial infarction, other acute coronary syndromes, stroke, heart failure, or death from cardiovascular causes.
Population N= 9361 Non diabetic, SBP 130-180mmHg, ≥50 years old, increased risk of CV events (10-year CV risk ≥15%, clinical or subclinical CVD, eGFR 20-60 ml/min/1.73m2, >75 years old)
Duration of Follow-up
3.26 years – due to early termination of trial (planned for max 6 years)
SPRINT Research Group et al. N Engl J Med 2015;373(22):2103:16

22
SPRINT
SPRINT Research Group et al. N Engl J Med 2015;373(22):2103:16
>60% started with SBP>145
121
136

23
SPRINT
SPRINT Research Group et al. N Engl J Med 2015;373(22):2103:16

24
SPRINT
SPRINT Research Group et al. N Engl J Med 2015;373(22):2103:16

25
SPRINT
Conclusion For non DM patients with high risk of CV event, SBP<120 resulted in lower rates of fatal and nonfatal major CV events and death from any cause
SPRINT Research Group et al. N Engl J Med 2015;373(22):2103:16

26
SPRINT on kidneys
The CKD patients in the intensive group had
• No reduction in CVD event rate or related mortality
• No impact on CKD progression
• Increased incidence of CKD
• Increased incidence of AKI
SPRINT Research Group et al. N Engl J Med 2015;373(22):2103:16

27
SPRINT versus ACCORD
SPRINT ACCORD
Non DM with high CV risk DM with high CV risk
N = 9361 N = 4733
Mean age 68 Mean age 62
Included CKD Excluded CKD (Cr>132.6μmol/L)
1 intervention 2x2 factorial design
Composite outcome 25% lower in intensive compared to
standard
Composite outcome 12% lower in intensive compared to standard but not stat sig

28
HOPE-3
Study Design
2x2 factorial, multicenter, international, double-blind, randomized, placebo-controlled trial Rosuvastatin (10mg) versus Candesartan (16mg) + HCTZ(12.5mg) versus Combi versus Placebo Outcome - composite of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke
Population N= 12,705 in 21 countries Men ≥ 55years old, women ≥ 65 years old No CVS disease, intermediate risk
Duration of Follow-up
5.6 years
Lonn et al. N Engl J Med 2016;374:2009-20

29
HOPE-3
Lonn et al. N Engl J Med 2016;374:2009-20

30
HOPE-3
Lonn et al. N Engl J Med 2016;374:2009-20
Baseline BP 138.1/81.9
Active has greater decrease (6/3mmHg) than placebo

31
HOPE-3
Lonn et al. N Engl J Med 2016;374:2009-20

32
HOPE-3
Conclusion Therapy with candesartan + HCTZ was not associated with a lower rate of major CV events
Lonn et al. N Engl J Med 2016;374:2009-20

33
HOPE-3
Cushman et al. N Engl J Med 2016;374:2085-7

34
HOPE-3 versus SPRINT
Cushman et al. N Engl J Med 2016;374:2085-7
HOPE-3 SPRINT
Intermediate CVS risk High CVS Risk
Greater BP decrease by 6/3mmHg
Greater SBP decrease by 14.8mmHg
Fixed low doses used Intensive regimen with specific BP target

35
PATHWAY-2 Study Design
Multicenter, double-blind, randomized, placebo-controlled, crossover trial Spironolactone versus doxazosin/bisoprolol/mean of both/placebo in resistant hypertension Outcome – Difference in average home BP between spironolactone and placebo, average of other 2 drugs, each of other 2 drugs respectively
Population N= 314, UK (predominant white Caucasian) Age 18 – 79, clinic SBP≥140 (≥135 for DM), or home SBP≥130 At least 3 months of maximally tolerated doses of ACEi/ARB, CCB and Diuretic
Duration of Follow-up
1 year, including placebo run-in and 12 weeks for each medication
Williams et al. Lancet 2015;386:2059-68

36
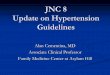
PATHWAY-2
Williams et al. Lancet 2015;386:2059-68
- 8.7mmHg - 4.03mmHg - 4.48 mmHg

37
PATHWAY-2
Williams et al. Lancet 2015;386:2059-68

38
PATHWAY-2
Williams et al. Lancet 2015;386:2059-68

39
PATHWAY-2
Conclusion Spironolactone was the most effective add-on drug for the treatment of resistant hypertension
Williams et al. Lancet 2015;386:2059-68

40
PATHWAY-2
Williams et al. Lancet 2015;386:2059-68

41
PATHWAY-2 – Interesting points
Williams et al. Lancet 2015;386:2059-68

42
Conclusion
• Consideration for BP target should include the CVS risk
• Target BP <140/90 in hypertensive with low CVS risk
• Consider BP <130/80 (even <120/80 if able to tolerate) for
those with high CVS risk
• Sensible assessment of benefits and risks, especially in the
elderly and CKD groups
• Close monitoring for adverse effect including renal function
• In resistant hypertension, spironolactone can be the 4th line

43
Thank You