Embed Size (px)
Citation preview

Medications used in the treatment of Spondyloarthropathies
David S. Hallegua MD
Assistant Professor of Medicine
Cedars-Sinai Medical Center/UCLA school of Medicine
Board Member, Spondylitis Association of America

Definition
• The spondyloarthropathies are a group of diseases that share clinical manifestations, genetic predisposition and disease complications
• They share unique disease causing mechanisms that can be treated with specific drugs that target these pathways in the body
• The severity of illness varies widely among affected individuals and treatment can be tailored to disease severity

Ankylosing
Spondylitis
AcuteAnteriorUveitis
Psoriatic Arthritis
Reactive arthritis
Undifferentiated Spondyloarthritis
ArthritisAssociated with Inflammatory
Bowel
JuvenileSpondyloarthritis
Ankylosing Spondylitis and related spondyloarthritis

Disease Mechanisms in AS and related illnesses
• Considerable body of evidence pointing to inflammation as a cause for symptoms
• Inflammation leads to excessive activation of bone remodeling cells causing bone erosions and osteoporosis
• New bone formation can lead to fusion of joints and calcification of ligaments in the spine. The Dkk protein and Wnt pathways have been implicated in AS

FoxP3
Treg cell
Self Ag + TGF
IL-10
TGFPROTECTION
IL-17
IL-22
MMP
INFLAMMATIONSelf Ag + TGF + IL-6
IL-23 (survival)
IL-23R
CTLA-4
TGFGITR
Naive T-cell
RORt
Th17 cell
CTLA4 = cytotoxic T lymphocyte-associated antigen 4; GITR = glucocorticoid-induced TNF receptor-related protein; MMP = matrix metalloproteinase; TGF = transforming growth factor.Tesmer L, et al. Presented at: American College of Rheumatology; November 10-15, 2006; Washington, D.C. Abstract 297; Furuzawa-Carballeda J, et al. Autoimmun Rev. 2007;6:169–175; Bettelli E, et al. Nature. 2006;441:235–238; Ivanov II, et al. Cell. 2006;26:1121; Bacchetta R, et al. J Allergy Clin Immunol. 2007;120:227–235.
Dichotomy of Th17 and Treg Subsets

Activated Osteoclasts
Osteoclast Precursors
RANKRANK
C
ytokines
TNF
ActivatedT cells
Activated Synoviocytes
ActivatedMacrophages
TNF TNF
BONEBONE
RANKRANK
RANK LRANK L
TNFTNF
TNF
RANK = receptor activator of nuclear factor-κB; RANKL = RANK ligand.Gravallese EM, et al. Arthritis Res. 2001;3:6–12; Zwerina J, et al. Arthritis Rheum. 2004;50:277–290.
RA
NK
LR
AN
K L
Synovitis Promotes Bone Erosion and osteoporosis via RANKL and TNF

Organ Involvement in Spondyloarthropathies
• Peripheral arthritis
• Spinal involvement
• Skin and mucous membranes
• Gastrointestinal involvement
• Cardiovascular involvement
• Pulmonary manifestations

Assessment Tools in AS• BASDAI (Bath AS Disease Activity Index)
– 4 Questions on fatigue, pain in neck, back, and hip, pain in other joints, and discomfort in areas tender to touch or pressure
– 2 Questions on duration and severity of morning stiffness (scores are averaged)
• BASMI (Bath AS Metrology Index)
– Used to define clinically significant changes in spinal movement
• ASAS (Assessment in AS) 20, 40,* 50, 70
– Improvement of ≥ 20%, 40%, 50%, or 70% and absolute improvement of ≥ 10 units in ≥ 3 domains:
• Patient global assessment, back pain, inflammation (mean of both BASDAI stiffness scores), and function (BASFI)
– No deterioration: ≥ 20% worsening or worsening of ≥ 10 units (scale of 0-100) in any domain
• ASAS 5/6 (Assessment in AS 5/6)
– ASAS-20 plus 2 additional criteria:
• Spinal mobility (BASMI)
• C-reactive protein (CRP)
– ≥ 20% Improvement in 5 of 6 domains
– No deterioration in any domain
*ASAS-40 is the recommended criteria for evaluating potential disease-modifying agents.

Axial symptoms and signs of AS

Axial symptoms and signs of AS
X-ray showing characteristic squaring of vertebra and syndesmophytes

Dactylitis

Enthesitis

Treatment for SpondyloarthritisPeripheral Spondyloarthritis(± axial disease; ± psoriasis)
NSAIDs ± IA corticosteroids
Early DMARDs if synovitis, joint damage
MonitorGR
2 DMARDs individually or in combinationSSZ, LEF, MTX, cyclosporine
MonitorGR
NR/PR
Active joint disease?(≥ 3 TJC & ≥ 3 SJC)
If YES
TNF antagonistsACR-50 response?PASI-75 response?
GRMonitor
NR/PR
Alternative TNF antagonists followed by other biologics if continued failure
IA = intra-articular; LEF = leflunomide; GR = good response; NR/PR = no response or poor response; PASI-75 = Psoriasis Area and Severity Index (75% response); PsA = psoriatic arthritis; PsARC = Psoriatic Arthritis Response Criteria; SJC = swollen joint count; SSZ = sulfasalazine; TJC = tender joint count. Adapted with permission from Kyle S, et al. Rheumatology. 2005;44:390–397. By permission of Oxford University Press.
NR/PR

Non-steroidal anti-inflammatory drugs
• Most of the NSAID’s have FDA approval for AS• Commonly used non-selective NSAID’s include
diclofenac, ibuprofen, naproxen, indomethacin, enteric coated aspirin, sulindac,
• Appear to help relieve adequate amount of pain and stiffness in 50% of AS patients treated
• Limited by stomach toxicity and loss of efficacy over time


Do NSAIDs Modify Disease Progression?
• 215 patients with AS were randomized to celecoxib 200 mg bid continuous (C) or on demand (OD)
• Structural changes assessed by using the modified Stokes Ankylosing Spondylitis Spine Score (SASSS)
• At 2 years, 76 C patients had complete radiographs compared to 74 OD patients
• Mean +/- SD scores for progression was 0.4 +/- 1.7 in the C group and 1.5 +/- 2.5 in the OD group (p=0.002)
• More studies need to performed before any firm conclusions can be drawn
Wanders A et al. Arthritis Rheum. 2005;52 (6):1756-65

GI Adverse Effects Associated With Conventional NSAIDs
GI Adverse Effects Associated With Conventional NSAIDs
• Upper GI intolerance– Dyspepsia– Nausea– Abdominal pain
• Asymptomatic ulcers
• Symptomatic ulcers
• Ulcer complications– Bleeding – Perforation– Gastric outlet obstruction
• Upper GI intolerance– Dyspepsia– Nausea– Abdominal pain
• Asymptomatic ulcers
• Symptomatic ulcers
• Ulcer complications– Bleeding – Perforation– Gastric outlet obstruction
Upper Gastrointestinal Toxicity From Conventional NSAIDsUpper Gastrointestinal Toxicity From Conventional NSAIDs

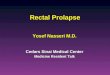
Mortality From NSAID-Induced GI Complications* Versus Other Diseases in United States
Mortality From NSAID-Induced GI Complications* Versus Other Diseases in United States
*Data from 19971. National Center for Health Statistics, 1998; 2. Singh, Triadafilopoulos. J Rheumatol. 1999;26(suppl 56):18–24.
*Data from 19971. National Center for Health Statistics, 1998; 2. Singh, Triadafilopoulos. J Rheumatol. 1999;26(suppl 56):18–24.
20,19720,197
16,68516,685 16,50016,500
10,50310,503
5,3385,338 4,4414,441
1,4371,437
00
5,0005,000
10,00010,000
15,00015,000
20,00020,000
25,00025,000
Leukemia1Leukemia1 HIV1HIV1 NSAIDs GI2
NSAIDs GI2
Multiplemyeloma1
Multiplemyeloma1
Asthma1Asthma1 Cervicalcancer1
Cervicalcancer1
Hodgkin’sdisease1
Hodgkin’sdisease1
Nu
mb
er
of
De
ath
s
Pe
r Y
ea
rN
um
be
r o
f D
eat
hs
P
er
Ye
ar
Cause of DeathCause of Death
Arthritis Care: An Increasing Burden on Healthcare ResourcesArthritis Care: An Increasing Burden on Healthcare Resources

Strategies for Preventing NSAID-Induced GI Injury
Strategies for Preventing NSAID-Induced GI Injury
• Use COX-2 specific inhibitor or non-NSAID analgesic1
• Prescribe lowest effective dose of NSAID
• Administer additional therapy
– Misoprostol2,3
– High-dose H2-receptor antagonist4
– Proton pump inhibitor5,6
• Avoid concomitant anticoagulant or corticosteroid use7,8
• Use COX-2 specific inhibitor or non-NSAID analgesic1
• Prescribe lowest effective dose of NSAID
• Administer additional therapy
– Misoprostol2,3
– High-dose H2-receptor antagonist4
– Proton pump inhibitor5,6
• Avoid concomitant anticoagulant or corticosteroid use7,8
1. Wolfe, et al. N Engl J Med. 1999;340:1888–1899; 2. Graham, et al. Ann Intern Med. 1993;119:257–262; 3. Raskin, et al. Ann Intern Med. 1995;123:344–350; 4. Taha, et al. N Engl J Med. 1998;334:1435–1439; 5. Cullen, et al. Aliment Pharmacol Ther. 1998;12:135–140; 6. Hawkey, et al. N Engl J Med. 1998;338:727–734; 7. Silverstein, et al. Ann Intern Med. 1995;123:241–249; 8. Shorr, et al. Arch Intern Med. 1993;153:1665–1670.
1. Wolfe, et al. N Engl J Med. 1999;340:1888–1899; 2. Graham, et al. Ann Intern Med. 1993;119:257–262; 3. Raskin, et al. Ann Intern Med. 1995;123:344–350; 4. Taha, et al. N Engl J Med. 1998;334:1435–1439; 5. Cullen, et al. Aliment Pharmacol Ther. 1998;12:135–140; 6. Hawkey, et al. N Engl J Med. 1998;338:727–734; 7. Silverstein, et al. Ann Intern Med. 1995;123:241–249; 8. Shorr, et al. Arch Intern Med. 1993;153:1665–1670.
Upper Gastrointestinal Toxicity From Conventional NSAIDsUpper Gastrointestinal Toxicity From Conventional NSAIDs

Placebo (n = 340)
Rofecoxib25 mg/d (n = 373)
Rofecoxib50 mg/d(n = 360)
Ibuprofen2,400 mg/d(n = 354)
Placebo (n = 340)
Rofecoxib25 mg/d (n = 373)
Rofecoxib50 mg/d(n = 360)
Ibuprofen2,400 mg/d(n = 354)
*Life-table estimate, intent-to-treat populationNo statistically significant difference between rofecoxib and placebo†P < 0.001 vs ibuprofen; **placebo group not assessed at week 24Hawkey, et al. Arthritis Rheum. 2000;43:370–377.
*Life-table estimate, intent-to-treat populationNo statistically significant difference between rofecoxib and placebo†P < 0.001 vs ibuprofen; **placebo group not assessed at week 24Hawkey, et al. Arthritis Rheum. 2000;43:370–377.
Cumulative Gastric/Duodenal Endoscopic Ulcer Incidence With Rofecoxib Treatment*Cumulative Gastric/Duodenal Endoscopic Ulcer Incidence With Rofecoxib Treatment*
7.37.3 †
4.7
†
4.7
†
9.7
†
9.7†
8.1
†
8.1
†
13.5
†
13.5
28.528.5
46.446.4
0055
1010151520202525
303035354040
45455050
Week 12Week 12 Week 24Week 24
Pat
ien
ts W
ith
Ulc
ers
3
mm
(%
)P
atie
nts
Wit
h U
lcer
s
3 m
m (
%)
COX-2 Specific Inhibitors: Reducing the Incidence of Upper GI UlcersCOX-2 Specific Inhibitors: Reducing the Incidence of Upper GI Ulcers
****

Celecoxib Long-term Arthritis Safety StudyCelecoxib Long-term Arthritis Safety Study
Ulcer Complication and Symptomatic Ulcer
Rates- All Patients
Ulcer Complication and Symptomatic Ulcer
Rates- All Patients
Silverstein, et al. JAMA. 2000;284:1247–1255.Silverstein, et al. JAMA. 2000;284:1247–1255.
Celecoxib 400 mg BID
Conventional NSAIDs
Celecoxib 400 mg BID
Conventional NSAIDs
An
nu
aliz
ed I
nci
den
ce (
%)
An
nu
aliz
ed I
nci
den
ce (
%)
00
11
22
33
44
ComplicationsComplications Complications andSymptomatic UlcersComplications and
Symptomatic Ulcers
P = 0.09P = 0.09
P = 0.02P = 0.02
0.760.76
1.451.45
2.082.08
3.543.54

Celecoxib NSAIDsCelecoxib NSAIDs
All Patients
MI 0.30.3
CVA 0.10.3
Non-Aspirin Users
MI < 0.10.1
CVA < 0.10.2
All Patients
MI 0.30.3
CVA 0.10.3
Non-Aspirin Users
MI < 0.10.1
CVA < 0.10.2
Cardiovascular Adverse Events in CLASS TrialCardiovascular Adverse Events in CLASS Trial
Cardiovascular Effects of COX-2 Specific Inhibitors: CLASS TrialCardiovascular Effects of COX-2 Specific Inhibitors: CLASS Trial
Celecoxib vs NSAIDs: P = NS for all comparisonsMI = myocardial infarction; CVA = cerebrovascular accidentSilverstein, et al. JAMA. 2000;284:1247–1255.
Celecoxib vs NSAIDs: P = NS for all comparisonsMI = myocardial infarction; CVA = cerebrovascular accidentSilverstein, et al. JAMA. 2000;284:1247–1255.
% of Patients% of Patients

Mortality and Cardiovascular Events in VIGOR TrialMortality and Cardiovascular Events in VIGOR Trial
*P < 0.05 vs naproxenCV = cardiovascular; MI = myocardial infarction; CVA = cerebrovascular accidentBombardier, et al. N Engl J Med. 2000;343:1520–1528.
*P < 0.05 vs naproxenCV = cardiovascular; MI = myocardial infarction; CVA = cerebrovascular accidentBombardier, et al. N Engl J Med. 2000;343:1520–1528.
Rofecoxib NaproxenDifferenceOutcome (n = 4,047) (n = 4,029)(95% CI)
Death 0.5% 0.4%0.1
(-0.15 to 0.49)
CV death 0.2% 0.2%0.0
(-0.21 to 0.21)
MI 0.4%* 0.1%0.3
(0.07 to 0.57)
Ischemic CVA 0.2% 0.2%0.0
(-0.17 to 0.27)
Rofecoxib NaproxenDifferenceOutcome (n = 4,047) (n = 4,029)(95% CI)
Death 0.5% 0.4%0.1
(-0.15 to 0.49)
CV death 0.2% 0.2%0.0
(-0.21 to 0.21)
MI 0.4%* 0.1%0.3
(0.07 to 0.57)
Ischemic CVA 0.2% 0.2%0.0
(-0.17 to 0.27)
Cardiovascular Effects of COX-2 Specific Inhibitors: VIGOR TrialCardiovascular Effects of COX-2 Specific Inhibitors: VIGOR Trial

ACE = angiotensin converting enzyme1. Pope, et al. Arch Intern Med. 1993;153:477–484.2. Johnson, et al. Ann Intern Med. 1994;121:289–300.
ACE = angiotensin converting enzyme1. Pope, et al. Arch Intern Med. 1993;153:477–484.2. Johnson, et al. Ann Intern Med. 1994;121:289–300.
Conventional NSAIDs: Effects in Hypertension
Findings From Two Meta-analyses1,2
Conventional NSAIDs: Effects in Hypertension
Findings From Two Meta-analyses1,2
• Conventional NSAID-induced blood pressure elevations occur in treated hypertensive patients (4–6 mm Hg)1,2
• Normotensive patients are minimally influenced
• Greatest effects seen in patients taking:
– ACE inhibitors
– Beta blockers, vasodilators
• Conventional NSAID-induced blood pressure elevations occur in treated hypertensive patients (4–6 mm Hg)1,2
• Normotensive patients are minimally influenced
• Greatest effects seen in patients taking:
– ACE inhibitors
– Beta blockers, vasodilators
Renal and Related Cardiovascular Effects of Conventional NSAIDsRenal and Related Cardiovascular Effects of Conventional NSAIDs

Incidence of Edema*Incidence of Edema*
Renal and Related Cardiovascular Effects of COX-2 Specific InhibitorsRenal and Related Cardiovascular Effects of COX-2 Specific Inhibitors
*Assessed by clinical criteriaWhelton, et al. Am J Ther. 2001;8:85–95.*Assessed by clinical criteriaWhelton, et al. Am J Ther. 2001;8:85–95.
P = 0.014P = 0.014
9.59.5
00
22
44
66
88
1010
Celecoxib 200 mg QD
(n = 411)
Celecoxib 200 mg QD
(n = 411)
Rofecoxib 25 mg QD(n = 399)
Rofecoxib 25 mg QD(n = 399)
% o
f P
atie
nts
% o
f P
atie
nts
4.94.9
6-Week Trial in Treated Hypertensive Patients With OA
6-Week Trial in Treated Hypertensive Patients With OA

Renal and Related Cardiovascular Effects of COX-2 Specific InhibitorsRenal and Related Cardiovascular Effects of COX-2 Specific Inhibitors
*P = 0.014; †P = 0.006; ‡P = 0.007Adapted from Whelton, et al. Am J Ther. 2001;8:85–95.*P = 0.014; †P = 0.006; ‡P = 0.007Adapted from Whelton, et al. Am J Ther. 2001;8:85–95.
Mean Systolic Blood Pressure (SBP)Mean Systolic Blood Pressure (SBP)
Rofecoxib 25 mg QD
Celecoxib 200 mg QD
Rofecoxib 25 mg QD
Celecoxib 200 mg QD
-1-1
00
11
22
33
11 22 33 44 55 66WeekWeek
Me
an
SB
P C
ha
ng
es
Fro
mB
as
elin
e (m
m H
g)
Me
an
SB
P C
ha
ng
es
Fro
mB
as
elin
e (m
m H
g)
*2.11*
2.11
†
2.58
†
2.58
‡
2.61
‡
2.61
-0.32
-0.32
-0.15
-0.15
-0.47
-0.47
6-Week Trial in Treated Hypertensive Patients With OA
6-Week Trial in Treated Hypertensive Patients With OA

Risks for Poor Renal and Related Cardiovascular Outcomes in Users of Conventional
NSAIDs or COX-2 Specific Inhibitors
Renal and Related Cardiovascular Effects of COX-2 Specific InhibitorsRenal and Related Cardiovascular Effects of COX-2 Specific Inhibitors
• Caution and appropriate monitoring when used in:– Heart disease– Pre-existing renal impairment– Liver disease– Advanced age
• Avoid use when serum creatinine 2.5 mg/dL (220 mol/L)
• In elderly hypertensive patients, monitor and treat new onset of edema and/or destabilization of BP control
• In “at risk” individuals (eg, elderly, patients with heart disease), monitor for onset of CHF and treat appropriately
• Caution and appropriate monitoring when used in:– Heart disease– Pre-existing renal impairment– Liver disease– Advanced age
• Avoid use when serum creatinine 2.5 mg/dL (220 mol/L)
• In elderly hypertensive patients, monitor and treat new onset of edema and/or destabilization of BP control
• In “at risk” individuals (eg, elderly, patients with heart disease), monitor for onset of CHF and treat appropriately

Other therapies for AS
• Corticosteroid injections help temporarily with peripheral arthritis, enthesitis
• White willow bark• Yarrow extracts• Acupuncture, massage therapy, spa therapy• Physical therapy, Tai Chi, stretching exercises• Opiates such as a fentanyl patch provides relief of
pain

Other oral disease controlling therapy in SpA
1.Sulfasalazine Effective in doses > 2 gm/day in controlling peripheral arthritis. Rashes, liver inflammation, sperm count, diarrhea
2. Methotrexate Effective in doses of > 7.5mg/week in controlling peripheral arthritis. Low blood counts, liver inflammation, hair loss
3.Thalidomide Effective at doses of 200 mg/day in reducing symptoms of AS. Nerve damage, blood clots, fetal deformities
4. Leflunomide Preliminary evidence of efficacy in peripheral arthritis at 20 mg/day. Liver inflammation, diarrhea, nerve damage
1.Clegg DO et al Arthritis Rheum. 1999;42(11):2325-9. 2.Gonzalez-Lopez L J Rheum.2004;31(8):1568-74
3. Wei JC J Rheum. 2003 Dec;30(12):2627-31 4..Haibel H et al. Ann Rheum Dis. 2005;64(1):124-6

Pamidronate in AS
• 84 AS patients randomized to 60 mg or 10 mg monthly for 6 months
• Primary outcome variable – 50% decrease in BASDAI
• 40% of the 60 mg group achieved the primary outcome variable
• No change in ESR/CRP seen and no major side-effects were noted. Occasional bone pain
• MRI of lumbar spine showed decrease in edema
Maksymowych WP et al. Arthritis Rheum 2002. 46:766-773

TNF Antagonists in Psoriatic ArthritisACR and PASI Results at Week 24
ACR = American College of Rheumatology response; BIW = twice weekly; EOW = every other week.1. Mease PJ, et al. Arthritis Rheum. 2005;52:3279–3289; 2. Mease PJ, et al. Arthritis Rheum. 2004;50:2264–2272;3. Enbrel® (etanercept) package insert. Immunex Corporation; Thousand Oaks, CA; 2006; 4. Antoni C, et al. Ann Rheum Dis. 2005;64:1150–1157.
40 mg EOW(N = 151)
Adalimumab1
25 mg BIW(N = 101)
Etanercept2,3 Infliximab4
5 mg/kg(N = 100)
Pat
ien
ts,
%
40 mg EOW(N = 69)
Adalimumab1
25 mg BIW(N = 66)
Etanercept2,3 Infliximab4
5 mg/kg(N = 83)
75
47
75
59
23
60
42
6
39
0
20
40
60
80
100
PASI-50 PASI-75 PASI-90
5750 54
39 37 41
23
9
27
0
20
40
60
80
100ACR-20 ACR-50 ACR-70

1.2
0.8
0.4
0
–0.8
–0.4
1.2
0.8
0.4
0
–0.8
–0.4
1.2
0.8
0.4
0
–0.8
–0.4
Mea
n C
han
ge
Fro
m B
asel
ine
Time From Randomization, Months
5 15 250 10 20 5 15 250 10 20 5 150 10 20
Total Sharp Score Erosion Score JSN Score
ETN = etanercept; JSN = Joint Space Narrowing; OL = open label; PsA = psoriatic arthritis.Adapted with permission from Mease PJ, et al. J Rheumatol. 2006;33:712–721.
Etanercept → Etanercept (n = 71)Placebo → Etanercept (n = 70)
ETN OL ETN OL ETN OL
Radiographic Progression in Patients With PsA Receiving Etanercept for 2 Years

Week 12 Week 24
Adalimumab (n = 205) (baseline mean = 6.4)
Placebo (n = 106)(baseline mean = 6.7)
Mea
n C
han
ge
in M
AS
ES
‡
-1.3-1.6
-2.7
* -3.2†
-4
-3
-2
-1
0
*P = 0.018 vs placebo; †P = 0.005 vs placebo.‡Mean change from baseline.MASES = Maastricht AS Enthesitis Score.van der Heijde D, et al. Arthritis Rheum. 2006;54;2136–2146.
ATLAS
Score range: 0–13 for pain
Adalimumab: Enthesitis Scores (MASES)

Etanercept: Sustained Efficacy for up to 72 Weeks
Res
po
nd
ers,
%
n = 139 n = 129 n = 105
0
25
50
75
100
0 12 24 36 48 60 72 84 96Week
ASAS-20ASAS-40ASAS 5/6
Double-BlindEtanercept 25 mg BIW
Open-Label Etanercept 25 mg BIW
ASAS = Assessments in Ankylosing Spondylitis group; BIW = twice weekly.Davis JC, et al. Ann Rheum Dis. 2005;64:1557–1562. Adapted with permission from BMJ Publishing Group.


Certolizumab Pegol Plus MethotrexateACR Response Rates at Week 24
Placebo(n = 130)
Certolizumab Pegol200 mg q 2 wk
(n = 252)
Certolizumab Pegol400 mg q 2 wk
(n = 252)*P < 0.001 vs placebo; †P ≤ 0.006 vs placebo. Smolen J, et al. Ann Rheum Dis. 2007;66(suppl 1):187. Abstract THU0202.
119
57 57
31
32 33
16
*
*
*
*
††
RAPID 2
0
10
20
30
40
50
60
70
Pat
ien
ts,
%
ACR-20
ACR-50
ACR-70

Golimumab in Ankylosing SpondylitisASAS Response Rates at Week 14
Placebo(n = 78)
Golimumab50 mg q 4 wk
(n = 138)
Golimumab100 mg q 4 wk
(n = 140)P < 0.001 vs placebo. Inman R, et al. Arthritis Rheum. 2008 Nov;58(11):3402-12.
21.8
59.460.3
15.4
43.5
54.3
ASAS 20 ASAS 40
0
10
20
30
40
50
60
70
80
90
Pat
ien
ts,
%

Efficacy of TNF Antagonists in AS: BASDAI-50 Response Rates
Better Response if Treated Early
Rudwaleit M, et al. Ann Rheum Dis. 2004;63:665–670. Used with permission from BMJ Publishing Group.
73
58
31
0
20
40
60
80
< 10 years 11–20 years > 20 years
Pat
ien
ts,
%
(n = 37) (n = 33) (n = 29)

Switching to Adalimumab From Etanerceptor Infliximab
ASAS Response Rates at Week 12
0
20
40
60
80
100
ASAS-20 ASAS-40 ASAS 5/6
Pat
ien
ts,
%
No Prior ETN or IFX (n = 877)
Prior ETN or IFX (n = 309)
RHAPSODY
ASAS = Assessments in Ankylosing Spondylitis group; ETN = etanercept; IFX = infliximab.Burmester G, et al. Presented at: American College of Rheumatology annual meeting; November 6-11, 2007; Boston, Massachusetts, USA. Abstract 945.
80
6067
46
63
43

Do TNF blockers modify progression of spinal bone fusion?
• All TNF blockers decrease bone marrow edema on Gad or fat suppressed MRI
• 41 patients with AS (Group 1) with complete x-ray sets from an extension trial of infliximab 5 mg/kg for 2 years compared to 41 patients from GESPIC (Group 2)
• Group 1 patients were older, had a longer disease duration and more radiographic damage at baseline.
• Mean mSASSS change was 0.4 (+/-2.7) (Group 1) and 0.7 (+/-3.4) (Group 2) (p=n.s.).
Baraliakos X et al Ann Rheum Dis. 2005 Mar 18

Uveitis

n
Flares/100
Patient-years
P
Before Anti-TNF
With Anti-TNF
All anti-TNF 46 51.8 21.4 0.03
Etanercept 13 54.6 58.5 0.92
Monoclonals 33 50.6 6.8 0.001
Infliximab 25 47.4 9.0 0.008
Adalimumab 8 60.5 0.0 0.04
Monoclonal TNF Antagonists May Be More Effective Than Etanercept in Preventing Uveitis Flares in AS
Guignard S, et al. Ann Rheum Dis. 2006;65:1631–1634.Images used from the collection of JT Rosenbaum, MD.

Psoriasis rash, skin and nail changes

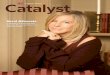
PASI Scoring and PASI Response Levels
PASI = Psoriasis Area and Severity Index.Fredricksson T, et al. Dermatologica. 1978;157:238–244.
Baseline PASI-50 PASI-75 PASI-90
Total PASI scoreis the sum of involvement andseverity scores for each body region
Region Area Involvement Severity
0.4
0.2
0.3
0.1 Multiply eacharea factor
byinvolvementscore (0–6)
Multiply eacharea factor
bysum of severity
scores (0–4) for redness, scale,
and thickness
PASI Response
PASI Score

Psoriasis: Response to TNF Antagonists at Weeks 24 to 26
0
20
40
60
80
100
Pat
ien
ts,
%
PASI-75 PASI-90 PGA "Clear or Almost Clear"
ADA1
40 mg EOW(N = 814)
ETN2
25 mg BIW(N = 162)
ETN2
50 mg BIW(N = 164)
IFX3
3 mg/kg q 8 wk
(N = 149)
IFX3
5 mg/kg q 8 wk
(N = 150)
70
49
60
44
20
39
59
30
55
65
33
64
78
56
79
ADA = adalimumab; ETN = etanercept; IFX = infliximab; EOW = every other week; BIW = twice weekly; PGA = Physician’s Global Assessment. 1, Menter A, et al. J Am Acad Dermatol. 2008;58:106–115. Epub 2007 Oct 23; 2. Leonardi CL, et al. N Engl J Med ,2003;349:2014–2022; 3. Menter A, et al. J Am Acad Dermatol. 2007;56:31.e1–e15.

Health-Related Economic Consequences of not Treating Severe RA With a TNF Antagonist
• Analysis of RA patients from a single UK district
• All met BSR/NICE guidelines for TNF antagonist eligibility
• Some patients did not receive TNF antagonists due to budget shortfalls
• Healthcare utilization: cost/1000 patient-months On TNF Antagonist (n = 56)
Not on TNF Antagonist
(n = 36)
Outpatient visits
$737 $50,440
Nurse Calls $338 $586ER visits $1052 $3206Hospitalisations $27,720 $290,070Total costs $29,848 $344,302Conclusion: failure to treat active RA results in additional costs
Beevor C, et al. Ann Rheum Dis. 2007;66(suppl II):163. Abstract THU0128.

Greenberg
SolomonSuissa
Dixon
0.0
0.5
1.0
1.5
2.0
2.5
MichaudJacobsson
Carmona
0.0
0.5
1.0
1.5
2.0
2.5
Cardiovascular Events All-Cause Mortality
Use of TNF Antagonists and the Risk for Cardiovascular Events and Death
Data expressed as standardized mortality ratios, hazard ratios, and incidence rate ratios.Dixon W, et al. Arthritis Rheum. 2006;54(9 suppl). Abstract 681; Suissa S, et al. Arthritis Rheum. 2006;55:531–536; Greenberg J, et al. Arthritis Rheum. 2006;54(9 suppl). Abstract 917; Solomon DH, et al. Arthritis Rheum. 2006;54:3790–3798; Michaud K, Wolfe F. Ann Rheum Dis. 2005;64(suppl III):87; Jacobsson L, et al. Arthritis Rheum. 2006;54(9 suppl). Abstract 729; Carmona L, et al. Ann Rheum Dis. 2007;66:880–885.
Rat
io
Rat
io

TB = tuberculosis; TST = tuberculin skin test.Hochberg MC, et al. Semin Arthritis Rheum. 2005;34:819–836; Keystone E, et al. J Rheumatol. 2005;32:8–12; Schiff MH, et al. Ann Rheum Dis. 2006;65:889–894; Scott DL, Kingsley GH. N Engl J Med. 2006;355:704–712.
Safety Considerations With TNF Antagonists
• Serious infections
– Do not initiate in patients with active infections
– Patients with RA are at higher risk than the general population
– Monitor closely and consider discontinuing if a serious infection develops
• Opportunistic infections and TB
– Include histoplasmosis, listeriosis, pulmonary aspergillosis, Pneumocystis carinii pneumonia
– Patients should be screened for latent TB with a TST prior to use and re-evaluated on a yearly basis
• Lymphoma
– Patients with RA are at higher risk for lymphoma than the general population, AS patients may be similar to RA
– Risk for lymphoma may be increased in children receiving TNF antagonists

CHF = congestive heart failure; MMR = measles/mumps/rubella; MS = multiple sclerosis; NYHA = New York Heart Association; SLE = systemic lupus erythematosus.Hochberg MC, et al. Semin Arthritis Rheum. 2005;34:819–836; Keystone E, et al. J Rheumatol. 2005;32:8–12; Schiff MH, et al. Ann Rheum Dis. 2006;65:889–894; Scott DL, Kingsley GH. N Engl J Med. 2006;355:704–712.
Safety Considerations With TNF Antagonists• Administration reactions• Live vaccines are contraindicated
– Including MMR, varicella, Herpes zoster, yellow fever, and intranasal influenza mist vaccines
• Demyelinating disorders– Rare; includes exacerbation of MS, optic neuritis, Guillain-Barré syndrome
• Hematologic abnormalities– Rare; includes cytopenia and pancytopenia (including aplastic anemia)
• CHF– Rare with adalimumab and etanercept– Infliximab is contraindicated in patients with NYHA class III & IV CHF
• Autoantibodies, SLE, lupus-like syndrome and new onset psoriasis– Rare; symptoms include cutaneous lesions, photosensitivity, and
pleural/pericardial serositis, new onset psoriasis

Significant Risk Factors Associated With Infections in Patients With RA
• 5596 Patients with RA (6817 PY)
• 3012 Receiving TNF antagonists (54%; 2722 PY)
• ADA: 12%; ETN: 40%; IFX: 48%
Variable Adjusted RR (95% CI)
TNF blocker 1.16 (1.06, 1.28)ACR functional class > 2 1.32 (1.19, 1.48)Erosion 1.16 (1.04, 1.28)Diabetes 1.27 (1.08, 1.50)Lung disease 1.37 (1.18, 1.58)Smoking 1.63 (1.46, 1.83)
ADA = adalimumab; CI = confidence interval; ETN = etanercept; IFX = infliximab; PY = patient-years; RR = relative risk. Maury E, et al. Arthritis Rheum. 2005;52:S547. Abstract 1453.
CORRONA

TNF Antagonists Increase the Risk of Hospitalization for Bacterial Infections in Patients With RA
• Health organization database cohort of RA patients:
– TNF antagonist: N = 2393 (3894 PY)
– MTX: N = 2933 (4846 PY)
• Claims review of all patients with a history of RA who were hospitalized for infection: 1998–2003; 187 charts
• Chart review of all bacterial infection diagnoses by nurses and 2 blinded infectious disease specialists
Conclusions:
• RR for infection: 1.9 (1.3–2.8) for anti-TNF agent vs MTX
– Number to treat: 143 patients had to receive anti-TNF agents for 1 increased infection
– Pneumonia: 1/3 of cases
• RR for infection: 4.2 (2.0–8.8) within the first 6 months of therapy
RR = relative risk; PY = patient-years.Curtis JR, et al. Arthritis Rheum. 2007;56:1125–1133.

TNF Antagonist Treatment and the Risk of Hospitalization for Infection
• Swedish RA database – 6410 Biologic-treated patients
• 1998–2006• IFX 64%, ETN 40%, ADA 13%
– 46,937 Hospitalized patients• 1964–2004
• 434 Hospitalizations for infection– 5.3 per PY with TNF antagonists
RR Adjusted for Age, Sex, Propensity
All Infections
1.31 (1.18–1.46)
Respiratory 1.20 (1.02–1.46)
Sepsis 1.11 (0.85–1.45)
Articular 1.63 (1.15–2.31)
GI 0.81 (0.57–1.16)
Cutaneous 0.88 (0.61–1.28)
ARTIS
Conclusions:• Increase of 30% in hospitalization in
patients receiving TNF antagonists• No increase in mortality• Risk decreases with duration of
treatment (RR = 0.82 after 2 years)
ADA = adalimumab; ETN = etanercept; IFX = infliximab; PY = patient-years; RR = relative risk.Adapted from Askling J, et al. Ann Rheum Dis, 2007;66:1339–1344 .

TNF Antagonists and the Risk of Serious Postoperative Infections
On/Off at Time of Surgery
On/Off for 28 d Before Surgery
On Off On 28 d Off 28 d
SPOI 49 (3.0%) 15 (3.5%) 59 (3.4%) 5 (1.4%)
AOR(CI)
1.00(Ref)
1.15 (0.62–2.12)
1.00(Ref)
0.38 (0.38–0.93)
• Treatment with TNF antagonists or DMARDs resulted in the same risk for SPOI (OR not significant)
• Patients on or off TNF antagonists had same low risk of SPOI• Patients off TNF antagonists > 28 days had a 60% reduction in SPOI• Data support discontinuation of TNF antagonists ≥ 4 weeks before surgery
BSRBR
AOR = adjusted odds ratio; OR = odds ratio; Ref = referent; SPOI = serious postoperative infections.Dixon W, et al. Ann Rheum Dis. 2007;66(suppl II):118. Abstract OP0215; Dixon W, et al. Data presented at: European League Against Rheumatism Annual Meeting; Barcelona, Spain; June 13-16, 2007.

0.0
0.5
1.0
1.5
2.0
Europe North AmericaEurope
Eve
nts
per
100
PY
Prior to TSTPrescreening
After Introduction of TSTPostscreening
No. of cases 7
534
23 4
7058 4914Exposure (PY)
*Through April 15, 2005. Data from RA clinical trials with adalimumab, including open-label extension studies and phase IV studies.PY = patient years; TB = tuberculosis.Adapted with permission from Schiff MH, et al. Ann Rheum Dis. 2006;65:889–894. Used with permission from BMJ Publishing Group.
0.330.08
1.31
Combined 0.27
TB Rates Prescreening and Postscreening in Clinical Trials With Adalimumab

Adverse Event Reports per 100 PY Pneumocystis carinii pneumonia 0.07Histoplasmosis 0.06Atypical mycobacteria 0.06Listeriosis 0.05CMV infections 0.04Aspergillosis 0.04Systemic candidiasis 0.03Coccidioidomycosis 0.03Cryptococcus 0.02Nocardia 0.02Toxoplasmosis 0.01Blastomycosis 0.00
CMV = cytomegalovirus; PY = patient-years.FDA Periodic Safety Update Report 10; August 2004.
Infliximab and Opportunistic Infections Postmarketing Reports

Risk of Malignancy in Patients
Receiving Biologic DMARDs
Cancer Cases
Odds Ratio(95% Confidence
Interval)
All 537 1.0 (0.8–1.2)
Breast 102 0.9 (0.5–1.3)
Colon 37 0.8 (0.3–1.7)
Lung 112 1.1 (0.7–1.8)
Lymphoma 45 1.0 (0.5–2.0)
Melanoma 32 2.3 (0.9–5.4)*
Skin (nonmelanoma) 623 1.5 (1.2-1.8)†
*P = 0.07; †P < 0.001.Wolfe F, Michaud K. Arthritis Rheum. 2007;56:2886–2895.

Cancer Rates in RA Patients Treated With TNF Antagonists
• Overall, no increased occurrence of cancer in patients receiving TNF antagonists1
• Signals suggestive of an increased risk for certain cancer types1 are consistent with results from other studies– Lung (COPD trial of infliximab)2
– Solid malignancies (Wegener’s granulomatosis etanercept study)3
– Melanoma and nonmelanoma skin cancer4 – Lymphoma and Leukemia in children⁵
Cancer Site
Relative Risk (all Primaries) by Time Since Start of Treatment1
< 1 Year 1–3 Years > 3 Years
All sites 0.98 (0.75–1.27) 0.88 (0.70–1.11) 0.99 (0.76–1.27)
Lung 1.11 (0.56–2.19) 1.15 (0.65–2.03) 1.62 (0.94–2.77)
Breast 0.72 (0.26–1.96) 0.65 (0.28–1.51) 0.50 (0.20–1.24)
NMSC 2.06 (1.00–4.23) 1.57 (0.84–2.92) 1.15 (0.50–2.63)
COPD = chronic obstructive pulmonary disease; NMSC = nonmelanoma skin cancer.1. Askling J, et al. Data presented at: EULAR; June 13–16, 2007; Barcelona, Spain. Abstract OP0013; 2. Rennard SI, et al. Am J Respir Crit Med. 2007;175;926–934; 3. WGET Research Group. N Engl J Med. 2005;352:351–361; 4. Wolfe F, Michaud K. Arthritis Rheum. 2007;56:2886–2895; 5. Watson KD, et al. Ann Rheum Dis. 2006;65(suppl III):512. Abstract SAT0202.
ARTIS

CA = cancer; CI = confidence interval; IRR = incidence risk ratio; PY = patient-years.Watson K, et al. Ann Rheum Dis. 2006;65(suppl III):512. Abstract SAT0202.
IRR
0.1
0.2
1.0
2.0
4.0
DMARD TNF Antagonist
0.4
No PriorCA
PriorCA
No PriorCA
PriorCA
8.0CAStatus N
CA(n)
Rate per1000 PY
DMARD
No prior CA 1819 27 14.1
Prior CA 58 1 18.2
Anti-TNF Agents
No prior CA 9844 158 8.4
Prior CA 154 6 20.5
• The overall risk of cancer was not significantly different between patients receiving DMARDs and patients receiving TNF antagonists (IRR = 0.7; 95% CI: 0.4, 1.2)
• The risk of recurrent cancer was not increased in patients receiving DMARDs (IRR = 1.2, 95% CI: 0.2, 8.9) but was significantly increased with respect to lymphoid malignancies in patients receiving TNF antagonists (IRR = 2.5; 95% CI: 1.2, 5.8)
The Effect of Previous Cancer on the Risk of Recurrent Cancer With TNF Antagonists
10.0

Future Direction of Spondyloarthritis Research
•Improve understanding of risk of infectious and neoplastic risks of treatments
•Increase in the therapeutic arsenal to control the illness
•Prevention of fusion of the spine and the joints