Embed Size (px)
DESCRIPTION
MEDICATIONS OF CONTROVERSY Challenges, Risks and Strategies. Alan Lembitz M.D. COPIC. I have no relevant financial relationships to disclose. Disclosure. Risks. Today we are going to talk about:. Overview. Scope of Problem. Safe prescribing practices. - PowerPoint PPT Presentation
Citation preview

© 2006 Wotkyns Creative
MEDICATIONS OF CONTROVERSYChallenges, Risks and Strategies
Alan Lembitz M.D.COPIC

Disclosure
I have no relevant financial relationships to disclose

Risks

OverviewToday we are going to talk about:
Safe prescribing practices
Scope of Problem
Tools- PDMP, Agreements, Consents,
Screening Tools, Diagnostic Tools,
Documentation

PART 1
OPIOIDS
5

6
Being a medical caregiver means putting your self in suffering’s way
Rita Charon M.D.

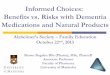
CDC declares painkillers at epidemic levels
Opioids, Anxiolytics and Sedatives

Rates of prescription painkiller sales, deaths and substance abuse treatment admissions (1999-2010)
SOURCES: National Vital Statistics System, 1999-2008; Automation of Reports and Consolidated Orders System (ARCOS) of the Drug Enforcement Administration (DEA), 1999-2010; Treatment Episode Data Set, 1999-2009

Distribution of Opioid Users
Controlledchronic pain
“All the rest”uncontrolled painpseudo-addiction
Addictionabuse

10
Overview
Top Reasons for paid claims in Primary Care:
1
2 Improper treatment of known medical condition
Delay or failure to diagnose (65+%)
3 Medication Errors

Risk by diagnosis
Heads Hearts Bellies Bugs- Severe Infectious
Diseases Failure to DX CA Underappreciated
severity of trauma
COPIC data

OxyContin in increasing doses beginning at ½ tabTID (20 mg) and increasing to 80mg tabs 6 per dayin 4 doses – These are the complete notes

Opiates
Opiates from poppies
Sumerians isolated opium from 3000 B.C.
Given with hemlock to put people to death
China 800 AD Europe 1300
13

Opiates
In 1806 Serturner isolated the morphine alkaloid and named it after the god of dreams, Morpheus
Heroin detailed for cough medicine in 1898
Works thru at least 4 receptors throughout the body
Profound effect is the mu receptor CNS
Controlled Substances Act in 1970 DEA enforces
14

Be sure of the DX
Pain out of proportion to findings
? FX
? Necrotizing fasciitis
Vascular, inc. mesenteric
Compartment syndrome
Don’t miss the CA

Pain diagrams
Accuracy of diagnosis Symptom magnification Objective pre-
procedure, or pre-treatment functionality
Objective post-procedure or post-treatment assessment of functionality
16

Addiction vs. tolerance vs. dependence
Addiction
Compulsive use causing personal harm
Psychological dependence
Rare in terminally ill or pain management
Usually preexisting abuse
Physical dependence
Abstinence syndrome think French connection
Not psychologic addiction
Decrease dose 50% Q 3 days
Tolerance
Decreased effectiveness
over time
Actually rare - if more needs there may be a
reason
Don’t label a tolerant patient
addicted

Addiction
A maladaptive pattern of substance use leading to impairment or distress, but has not met the criteria for Substance Dependence, having ≥ 1 of the following:
Recurrent substance use resulting in failure to fulfill major role obligations at work, home, school
Recurrent substance use in situations in which it is physically hazardous
Recurrent substance-related legal problems Continued substance use despite having
persistent or recurrent problems caused by the substance use
18

Opioid addiction risk factors
Biggest risk factor is a personal or family history of drug/ETOH abuse
Journal of pain v109 pg 113-130 2009
Psych problems
Poor coping skills
Sexual abuse
19

Faces of addiction

Genetics
Pathogenesis
Precipitants
Environmental determinants
Gender specifics
Complications
Relapse-Remission
Criteria of chronic illness

Key to identifying alcohol abuse
ASK
• CAGE: cut back, annoying, guilt, eye opener
• Drinks per week: 7 or 14?• Binge per year: 5 (4)?

SOAPP
Biggest risk factor is a personal or family history of drug/ETOH abuse
Journal of pain v109 pg 113-130 2009
23

Overdose- accidental vs. intentional
It’s about the documentation
Evaluate for coexisting psych problem
Tip of the iceberg potential
ACTIONS MUST MATCH THE DOCUMENTATION

DEA
Responsible prescribing
Regulation increasing
Stings
Documentation
Pharmacist is the trigger work with them

Street value
Drug Estimated Street Cost
Oxycodone $5-10/ pill
Oxycodone ER $1/mg
Vicodin 5/500 $3-5/ pill
Percocet $5-10/ pill
Methadone $25
Xanax $3-5/ pill
Fentanyl $1/ mcg
26

Dilaudid 4mg #240
Street value of this Rx: $7,000plus
No addressNo datePmNo legitimatepurpose

28
Prescription Drug Monitoring Program
Powerful tool
Use it don’t lose it
Password sacred
Notification

Which of the following is NOT appropriate for a pain agreement?
A) No diversion allowed
B) May request a tox screen at any time
C) Notify us by Thursday if scripts are lost or destroyed
D) Can only go to 1 pharmacy
29

Opioid agreements
An Agreement not a Contract
May specify one pharmacy
Treaters may discuss DX and RX
No diversion Danger of abrupt
withdrawal Pregnancy
Urine or Serum tox screens may be a condition of the agreement.
Lost, wet, left, stolen not acceptable excuses
Compliance with scheduled appointments and referrals
Breach may result in termination, cessation of therapy or referral to addiction specialist


Long-term consent
Indications
Risks
Prohibition of activity if impaired
Withdrawal
Addiction definition and potential
Physical Dependence
Tolerance and Possible Increases in dosages or reduction in effect
32

Align your partners
Clear discussion of philosophy
Pain agreements help guide your partners
A covering prescriber on a routine script- little risk

CMB – red flags
Chronic narcotics without cause
No formal relationship
No physical exam
Suggest different pharmacies
Prescribe for sex or sharing
Prescribe to family

Example of the office visit notes

OxyContin 40mg 2-bidDilaudid 8mg qidSoma 1 qid

DEA examplesNew patient:Prescribed Dilaudid4 mg #240 plusXanax
Do you believe this doctordid an exam of the head,
heart and lungs?

Hassle factors
HIPAA
Records release
Labeling addict can be an issue
Weekend and night calls

Always
Contact the previous physician
Ask the patient about previous alcohol and drug use, or psychiatric or drug related hospitalizations.
Document a thorough and thoughtful exam
Consider a drug screen

PART 2
MEDICAL MARIJUANA
RECREATIONAL MARIJUANA
41

SCOPE OF MMJ
Numbers of registrants
Characteristics of registrants Age Primary Dx
The Dispensaries

MAJOR QUESTIONS TO CONSIDER
Do I certify for MMJ? Informed ConsentScreen for contraindicationsKnow and review the scienceFollowing CMB regulations
Bona fide physician patient relationship Diagnosis established by history and examination Documentation Recommendation for follow-up
Practical Logistics- forms and registry

MAJOR QUESTIONS TO CONSIDER
My patient is on MMJ registry and actively using, does this change my practice and prescribing for them?

MAJOR QUESTIONS TO CONSIDER
What if my patient was inappropriately certified for the registry?CMB unprofessional conduct- license and duty to reportSpecific clinical examples
Minors Psychiatric contraindications Occupations involving public safety

MAJOR QUESTIONS TO CONSIDER
Do I have vicarious liability if I certify, or if I know my patient is using MMJ, or if they are taking opioids, etc?Chart documentation of discussion Informed consent is a process, but a form may be required if
significant risk and non-compliance with recommendations

DRIVING UNDER INFLUENCE
Law Enforcement considerations
Available testing and reliability

SPECIAL SITUATIONS
Physicians who personally are on the registry CPHP CMB COPIC

SUMMARY
Certifying my own patients- how to do this in compliance and consistent with sound medical practice
What to do about your patient who someone else certified for the registry
What about other physicians who certify out of compliance with sound practice
Vicarious liabilityDUI is not just alcohol

Boundaries- Are your issue
Boundary discussions are often about your own conflict
Can be you or the patient with the problem
Discuss what your concern is

Boundaries—Providers role
Clarify boundaries
And negotiate
I don’t give unlimited narcotics but I want to help you. What can we work out….
My role is to help people not just give out narcs…
Can we come up with a short term plan today and then work on something long term?

Do you accept the challenge?
Do you choose to work with this patient?
It is OK to say no
Send a letter 30 days
Taper schedule
Withdrawal and ? refer

53
The good news
Most lawsuits result in defense judgments or verdicts.
Most patient complaints to plaintiffs’ attorneys do not result in lawsuits
Most CMB complaints do not result in discipline
Pain assessments, agreements, consents, documentation and consults help greatly

Our challenge
"....in the sufferer, let me see only the human being” –
Maimonides, 13th Century

55
I appreciate your feedback.
Alan Lembitz M.D.VP, COPIC
Patient Safety and Risk Management
Thank you
Any questions?