Embed Size (px)
Citation preview

Brian Hurley, M.D., M.B.A., DFASAM Medical Director of Substance Use Related Care Integration
Los Angeles County Health Agency - Department of Health Services - Department of Mental Health
Medications for Addiction Treatment in the Mental Health
and Physical Health Sectors
Brian Hurley, M.D., M.B.A., DFASAM
No disclosures
Los Angeles County •Population prevalence of SUD is estimated to be 8% (= 864,500)
•10 to 12% of Medi-Cal beneficiairies have a SUD
•13.6% new Medi-Cal beneficiaries (since expansion) have a SUD. ⇒ ~300,000 to 400,000 Medi-Cal beneficiaries in Los Angeles County with SUD
Mark, T. L., Wier, L. M., Malone, K., Penne, M., & Cowell, A. J. (2015). National estimates of behavioral health conditions and their treatment among adults newly insured under the ACA. Psychiatric Services, 66(4), 426-429. California Mental Health and Substance Use System Needs Assessment. 2012. Technical Assistance Collaborative. Available at: http://www.dhcs.ca.gov/provgovpart/Documents/1115%20Waiver%20Behavioral%20Health%20Services%20Needs%20Assessment%203%201%2012.pdf
Los Angeles County
•~43,000 annually receive publicly funded specialty SUD treatment: •~17,000 with heroin use disorder •~10,000 with methamphetamine use disorder
•~6,000 alcohol use disorder •~3,000 with Rx opioid use disorder (up from 1,000 in 2006)
http://www.publichealth.lacounty.gov/sapc/MDU/mdr.htm
“Scaling up the use of MAT will require engaging clinicians who prescribe in all areas of the health sector”
-Dr. Tsai
Los Angeles County
LA County Health Agency
DHS DMH DPH SAPC
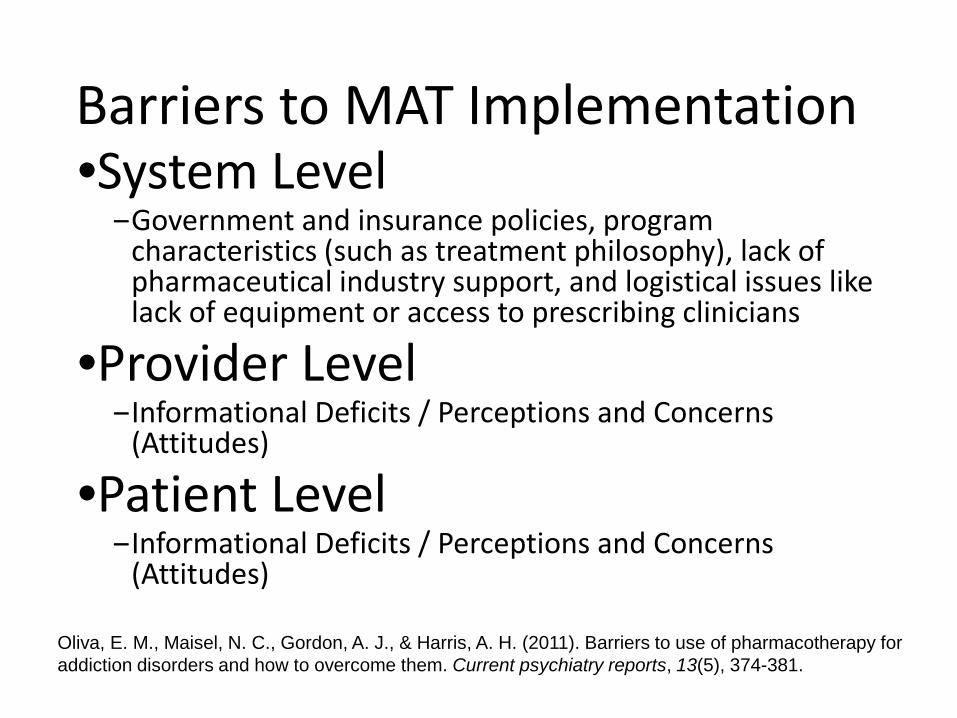
Barriers to MAT Implementation •System Level
‒Government and insurance policies, program characteristics (such as treatment philosophy), lack of pharmaceutical industry support, and logistical issues like lack of equipment or access to prescribing clinicians
•Provider Level ‒Informational Deficits / Perceptions and Concerns
(Attitudes)
•Patient Level ‒Informational Deficits / Perceptions and Concerns
(Attitudes)
Oliva, E. M., Maisel, N. C., Gordon, A. J., & Harris, A. H. (2011). Barriers to use of pharmacotherapy for addiction disorders and how to overcome them. Current psychiatry reports, 13(5), 374-381.
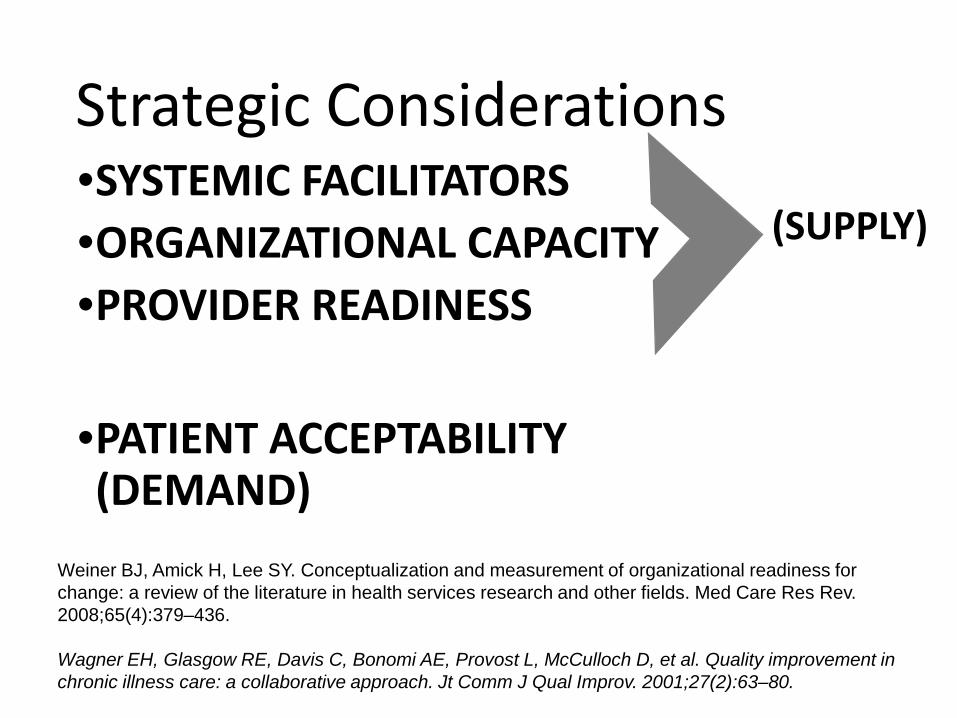
Strategic Considerations •SYSTEMIC FACILITATORS •ORGANIZATIONAL CAPACITY •PROVIDER READINESS
•PATIENT ACCEPTABILITY (DEMAND)
Weiner BJ, Amick H, Lee SY. Conceptualization and measurement of organizational readiness for change: a review of the literature in health services research and other fields. Med Care Res Rev. 2008;65(4):379–436. Wagner EH, Glasgow RE, Davis C, Bonomi AE, Provost L, McCulloch D, et al. Quality improvement in chronic illness care: a collaborative approach. Jt Comm J Qual Improv. 2001;27(2):63–80.
(SUPPLY)
Core Components of Addiction Treatment
•Counseling* •Support* •Medications*
*When appropriate Source: https://www.samhsa.gov/treatment
• Pharmacological therapy • Psychosocial services/interventions • Coordination/integration of substance use
disorder treatment and other medical/psychological needs
• Provider and community education and outreach
Shared Components of MAT in Primary Care
Chou R, Korthuis PT, Weimer M, Bougatsos C, Blazina I, Zakher B, Grusing S, Devine B, McCarty D. Medication-Assisted Treatment Models of Care for Opioid Use Disorder in Primary Care Settings. Technical Brief No. 28. (Prepared by the Pacific Northwest Evidence-based Practice Center under Contract No. 290-2015-00009-I.) AHRQ Publication No. 16(17)-EHC039- EF. Rockville, MD: Agency for Healthcare Research and Quality. December 2016. www.effectivehealthcare.ahrq.gov/reports/final.cfm - Accessed 12/6/2016.
SUMMIT Study
Ober, A. J., Watkins, K. E., Hunter, S. B., Lamp, K., Lind, M., & Setodji, C. M. (2015). An organizational readiness intervention and randomized controlled trial to test strategies for implementing substance use disorder treatment into primary care: SUMMIT study protocol. Implementation Science, 10(1), 1.
https://www.rand.org/content/dam/rand/pubs/tools/TL100/TL148-1/RAND_TL148-1.pdf
https://www.rand.org/content/dam/rand/pubs/tools/TL100/TL147/RAND_TL147.pdf


CHCF Treating Addiction in the Primary Care Safety Net
http://www.tapcprogram.com
CHCF Treating Addiction in the Primary Care Safety Net •Project ECHO for Buprenorphine •Coaching by experts •Monthly CSAM webinars •In-Person Learning Sessions •Bup Waiver Trainings •Site Visits
•Directly operates > 80 programs •Contracts with > 700 providers •>250,000 individuals served / year
•Addiction Medicine in Psychiatric Practice •Availability of naltrexone long acting injection, oral naltrexone, acamprosate, disulfiram, and buprenorphine
•On-site urine toxicology availability •Policies, procedures, and parameters
LAC DHS Programs
•MAT in four ambulatory care clinics
•Dual Diagnosis (COD) Program operated by DMH at a DHS Hospital (Harbor-UCLA)
•Sobering Center
LAC DHS Programs
LAC DHS Programs
DHS DMC-ODS Enrollment
DHS DMC-ODS Enrollment
• Five pilot ambulatory care sites • Co-locating LPHAs, SUD Counselors, and MCWs • Separate medical record system

Vision for Los Angeles County •Expand addiction medicine capacity in primary care and mental health sites:
Willing Patients
Org Capacity
Treatment Ready Clinicians