Embed Size (px)
Citation preview

Medication Safety Technology The Good, the Bad and the Unintended Consequences
Michelle Mandrack RN, MSNDirector of Consulting Services
Matthew Fricker, RPh, MSProgram Director
1

Objectives
• Consider the effects of medication‐related technology on quality
• Discuss the benefits of a medication safety net• Describe some of the unintended consequences of technology
• Describe some of the general concepts of technology implementation and maintenance
2

Terminology
ADC = automated dispensing cabinetBPOC = barcode point‐of‐careCDS = clinical decision supportCPOE = computerized prescriber order entry
3

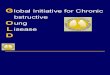
Errors in the Medication Use Process
Prescribing Transcribing Dispensing Administering
39% 12% 11% 38%
Source: Leape, et al. JAMA 1995;274:35-43
Errors
Errors intercepted
Sources of harm 28% 11% 10% 51%
48% 33% 33% 2%
4

General Technology Issues
Does technology improve the quality and safety of the medication use process?
–Yes–No
5

General Technology Issues• Yes IF:‐Well designed ‐ Thoughtfully implemented ‐ Appropriately used
• No IF:‐ Users do not participate in the design phase‐ Layered on dysfunctional, manual systems ‐ Ambiguous content is developed that cannot be utilized by frontline staff
6

General Technology Issues
How much technology is enough?
7

Developing a Medication Safety Net
• No single technology can prevent all medication errors– Establish a medication safety net by using complementary technologies
– Technologies that prevent errors at medication administration will not prevent errors related topreparation in the pharmacy
8

Developing a Medication Safety Net
–Technologies that prevent errors in medication preparation will not identify over‐ and under‐doses
–Technologies that prevent errors in the pharmacy will not prevent errors in drug prescribing
9

General Technology Issues
• What gaps are there in your technology?–Are all patient populations covered?
• Consider what technology may miss:–Wrong patient–Look‐alike/sound‐alike drugs–Overdoses, specifically catastrophic doses
10

General Technology Issues• Limited human resources
– Is there sufficient staff to train, retrain and optimize?
–Order set development for specific populations or disease states (e.g., oncology, pediatrics, neonatology)
–Development and implementation of enhancements or updates
–Database management
11

General Technology Issues• Timelines and milestones for improving utilization
–Measure utilization of BPOC, CPOE, smart pumps
• Implementation and optimization NEVER end–Feedback loop to retrain users –Optimize the technology–Observe for barriers and workarounds
12

General Technology Issues
• Does medication error analysis probe why the technology did not prevent the error?
• Technology does not replace independent double‐checks
13

General Technology Issues
• Reports–What reports are available? –Degree of usefulness/value–Structured review process
14

Clinical Decision Support (CDS)• What CDS is currently functioning?
– Drug interactions, duplicates, dose range checking– Rule based review of renally‐dosed medications – Drug disease interactions
• Order sets are the foundation of CDS – Problematic paper order sets create additional issues when CPOE is implemented
• Alerts– Maximize clinical value– Minimize noise
15

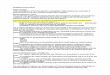
Automated Dispensing Cabinets
16

What Does an ADC Add to Safety?
• Not a primary medication safety strategy – Component of medication distribution models
• Incorporate ISMP core processes to maximize safe use
17

Percent Score for 12 Core ProcessesTotal number of hospitals = 380
%=Mean score/Maximum possible score
18

Overall Lowest Scores (% Not Implemented)
19

Overall Highest Scores (% Fully Implemented)
20

ADC ResourcesInstitute for Safe Medication Practices (ISMP) Guidance on the Interdisciplinary Safe Use of Automated Dispensing Cabinetshttp://www.ismp.org/Tools/guidelines/ADC/default.asp
ISMP Medication Safety Self Assessment ® for Automated Dispensing Cabinets (ADC) http://www.ismp.org/selfassessments/ADC/Login.asp
21

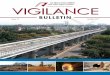
Smart Pump Technology
22

Definition
Smart Pump – infusion device with software that has the ability to alert users to potential medication errors. This software allows an organization to create a library of medications that provides medication dosing guidelines, by establishing concentrations, dose limits and clinical advisories
23

Types of Errors
• Pump misprogramming• IV line errors• Lack of an independent double‐check• Bypassing library• Overriding alerts
24

Programming Errors• IV pump keypad design
– Proximity of the “zero” and “decimal point” keys
• Double Key Bounce– Pump records a number twice although the corresponding key is pressed just once
• Double Keying– Key purposely pressed twice because of delay after the first key is pressed before the number appeared on the screen
– Number or letter key is accidentally pressed twice
25

Programming Errors
• Nurse attempted to program pump for a baby receiving TPN by inputting 13.0 mL/hour–Decimal point key on the pump was somewhat worn and difficult to engage
–Without realizing it, the nurse programmed a rate of 130 mL/hour
26

Other Programming Errors• Wrong drug or concentration selected from library
• Wrong concentration programmed • Wrong dosing units
–mg/hr versus mg/min–mcg/kg/hr versus mcg/kg/min
• Wrong dose related to incorrect patient weight • Wrong channel programmed
27

Limitations – Smart Pumps• Limited number of entries available in the drug library
• Limited in certain patient populations (pediatrics, neonates, oncology)–Sometimes based on availability of pumps or number of line items needed in the drug library for a particular unit
28

Failures in the Double‐Check System
• Double checks not performed independently with one nurse setting the pump, and another nurse independently checking the patient, drug, and settings against the MAR
29

Best Practices Using High‐Leverage Strategies
• Set the standard that all medications, including continuous infusions, intermittent infusions and bolus doses are administered using the smart pump along with the error reduction software
• Incorporate hard stops as well as soft stops, especially for high‐alert medications
30

Best Practices Using High‐Leverage Strategies
• Use wireless communication to update libraries and download quality data
• Establish standard concentrations and dosing units• Maximize use of commercially available products
31

Barcode Point‐of‐Care
32

Workarounds to BPOC System: Their Occurrences, Causes and Threats to Patient Safety
• 15 workarounds observed – Affixing patient ID labels to medication cart, crib– Pre‐scanning medications for several patients
• 31 probable causes– Unreadable barcodes– Medication package does not match patient dose – Battery failures– Travel distance required to obtain refrigerated medications
• Noise obscuring alarms
(JAIMA Vol 15, No 4 July/August 2008)
33

Bar Coded Medication Administration – A Last Line of Defense
• Traditional strategy is nursing vigilance • BPOC has ben successfully implemented in other clinical applications
• More drug administration errors are captured post implementation than thought existed
Cescon and Etchells, JAMA, May 14, 2008 – Vol 299, No 18

Effect of Bar‐Code Technology on the Safety of Medication Administration
• Units without bar‐code eMAR had 776 non‐timing errors in medication administration – Units with bar‐code eMAR had 495 errors
• 51% reduction in potential ADEs from the above errors
• Prevent approximately 95,000 potential ADEs
Poon, Keohane, et al; NEJM 362;18, May 6, 2010

Process Measures• Bedside Scan Rate
– Identify barriers to scanning– Identify staff who have difficulty consistently scanning
• Wrong Patient• Wrong Drug
– Identify and trend which medications are involved, (e.g., insulin)
• Percent of medications barcoded– Identify barriers to barcoding medications
36

Process Measures
• Bad Scans–Are medications scanned when they are received in the pharmacy from the wholesaler or outsourced re‐packager?
– Is there a mechanism for nurses to inform the pharmacy when medications are not able to be scanned?
37


Failure Points with a BPOC SystemWhere Metrics Will Not Help
• Orders that generate multiple tasks for the same drug
–A new antibiotic written “now and then” that generates two tasks on two different shifts
For example – ceftriaxone 1 g daily, now and then q24 hours written at 0630, given by the night shift and then another task is generated for the standard time at 0800
39

Failure Points with a BPOC System Where Metrics Will Not Help
• Medication scans correctly but is administered via the wrong route (oral liquid given IV)
• IV infusion scanned but the pump is not started• Inhaler scanned correctly and given to the patient who then administers the medication incorrectly
40

Limitations – BPOC
• Limited functionality in certain patient populations, e.g., pediatrics, neonates, oncology
• System response time • Limited bandwidth • Connectivity issues
41

What Can CPOE Do?
• Require that all elements are present• Provide clarity of order – no handwritten prescriptions
• Dose checking • Provide access to information from previous encounters
42

What Can CPOE Do?
• Create firewalls to prevent errors• Eliminate the need for shadow charts• Provide access to charts both inside and outside the hospital
• Prevent clarification calls by providing feedback during the ordering process
43

Clinical Decision Support• Dose limits
–Single dose–Dose/24 hours
• Patient information–Allergies, height, weight, comorbidities
• Route of administration–Filters that only allow medications ordered via specific routes, e.g., intravenous vs. intrathecal
44

Clinical Decision Support• Duplicate drug therapy • Contraindicated drugs• Dose modifications based on interaction with lab data• Drug/drug and drug/food interactions• Quality controls • Drug information
45

Who Were the Early Adopters?
• Partners/Brigham and Women’s Hospital• Regenstrief Institute• Latter Day Saints (LDS) Hospital• Vanderbilt University Medical Center
46

What Makes Them Unique?
• Home grown• Not commercially available• Evolved over years• Academic learning centers
47

What Has Changed?
• CPOE is available from commercial vendors• Expansion into community hospitals• Fewer internal resources within hospitals to support CDS
• Publications on increasing errors and CPOE’sability to decrease the potential for errors
48

Unintended Consequences of CPOE • Alert Fatigue
– Using a commercial data base to identify alerts without considering the alerts needed by the organization
– Not realizing the resources needed to build custom alerts
• Assuming CPOE will identify all prescribing errors– What CDS is really functioning? – What has been turned off because of alert fatigue?– What rules have been written (e.g., renally dosed drugs)?
49

Unintended Consequences of CPOE
• Downstream effect of a poorly designed CPOE system– Exploding order set that generates multiple pages of orders
• Numerous orders that will never be needed• Time consuming order review by the pharmacy
50

Unintended Consequences of CPOE
• Duplicate therapy in multiple order sets • Conditional Orders
– “If, then” orders (e.g., “Start patient on beta blocker if ok with Renal”)
• Initial impact on workload which requires seeing fewer patients during training period
51

Unintended Consequences of CPOE
• Impact of a bifurcated workflow (both CPOE and manual orders used within the facility)– Duplicate orders received in pharmacy– Variation in nursing order verification processes
52

Medical Staff Participation
• Communicate the status of the implementation
• Work on the impact of CPOE on user workflow• Facilitate the development of departmental order sets
53

Medical Staff Participation
• Champion the utilization of CPOE in their respective department– Become knowledgeable as a super‐user to assist colleagues during go‐live
– Provide oversight for departmental training
54

CPOE Challenges• Limited use of clinical decision support• Limited resources to support:
– CDS– Training– Enhancements, updates, upgrades– Downtime and connectivity issues
• Limited functionality in certain patient populations
– Pediatrics, neonates, oncology
55

Questions
56