Embed Size (px)
Citation preview

WORKSHOP 7,13.30-15.15 : 7,12 ,JULY 2019
MEDICATION SAFETY IN EMERGENCY
DEPARTMENT
10-12 JULY 2019INTERNATIONAL CONVENTION CENTRE
NUSA DUA –BALI,INDONESIA
Yahaya Hassan, Pharm.D, Professor,Department of Clinical Pharmacy ,
School of Pharmacy, Management & Science University ,University Drive, Off Persiaran Olahraga, Section 13,40100, Shah Alam, Selangor Darul Ehsan, Malaysia,
MEDICATION SAFETYOne of the important missions of the healthcare providers is to ensure patient safety.
Unfortunately medication errors do occur and often go undetected.
Some medication errors may result in serious patient morbidity and mortality
Why Medication Safety is Important
ADEs are a serious public health problem.
more than 1 million emergency departmentvisits.
280,000 hospitalizations each year.
$3.5 billion is spent on medical costs of ADEsannually.
more than 40% of costs related to ambulatory ADEs are preventable
MEDICATION SAFETY
Enhanced awareness on medication
safety:
New and potent medicine
More drugs available
Ensuring patient safety at all levels and
various systems and processes
involved in the entire medicines
management cycle.
MEDICATION SAFETYThe proposed mechanism is a ‘Medication Error Reporting System’ through which medication errors will be monitored and preventive measures can be defined.
This system requires a collective effort from various parties and a change in the way we manage medication errors.
We need to be able to discuss errors openly, encourage reporting of errors and maintain a culture that is non-punitive and blamelessness.
With this, healthcare providers will be able to learn from the errors.
EMERGENCY PHARMACY
DEPARTMENT
MEDICATION SAFETY IN
THE ED
ED INTRODUCTION
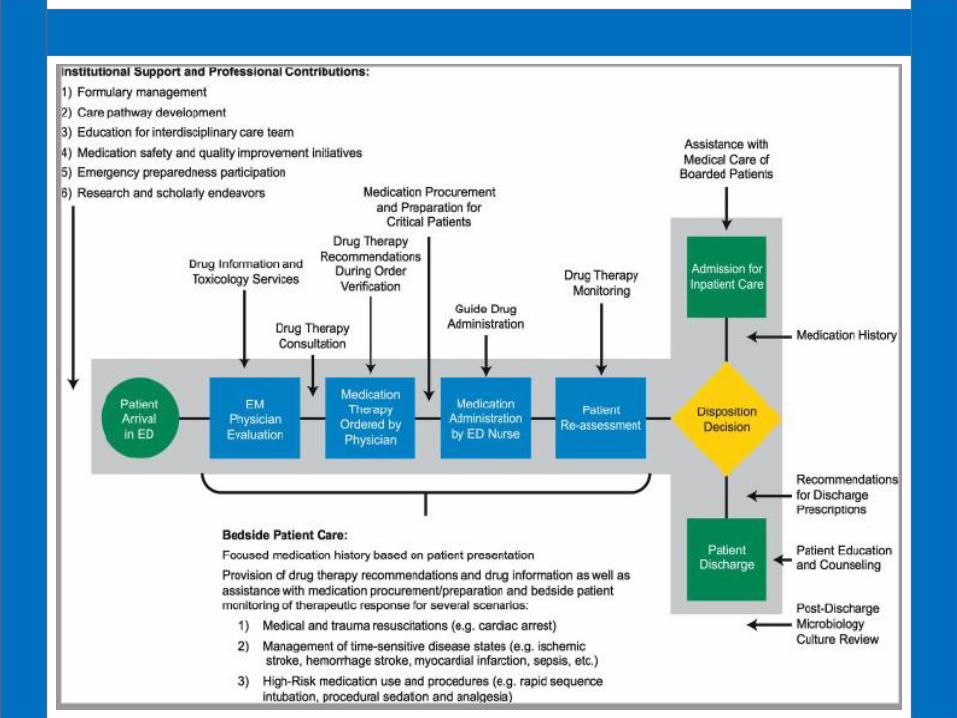
1. ED environment is often overcrowded, fast-paced patient care and high-acuity disease state management.2. Inherent medication safety risks exist because of the complexity of this practice environment.3. Emergency medication use process (e.g., medication selection, ordering, verifying, and dispensing; education; and administration) may be contained in the ED without a pharmacist’s oversight.4. Medications may be administered according to verbal order, and these medications may be readily available on override in automated dispensing cabinets or floor stock to the emergency medicine (EM) team.
ED INTRODUCTION
5. Therefore, the process from prescribing to administration may be done without a pharmacist’s involvement, because legally, it is not required that pharmacists verify medications that are needed emergently.
6. More recently the American College of Emergency Physicians created a policy statement that supports clinical pharmacy services in the ED and collaboration among EM providers in order to promote safe, effective, and evidence-based medication practices; encourage interdisciplinary EM-related clinical research; and foster an environment supporting EM pharmacy residency training.
Overview of
Emergency
Department
Unique practice setting
Serves as point of entry, transition and exit
Intended for treatment and management of emergent or acutely ill
patients
May contain urgent care or fast track section
Workflow
Fast paced
Chaotic
Staff
Primarily health techs, nurses, physician
Expanding to other services for improved access
Patient
Various acuity levels
Boarders
Highest number of preventable adverse drug events of any hospital setting

MEDICATION SAFETY IN
THE ED
Medication errors (MEs)
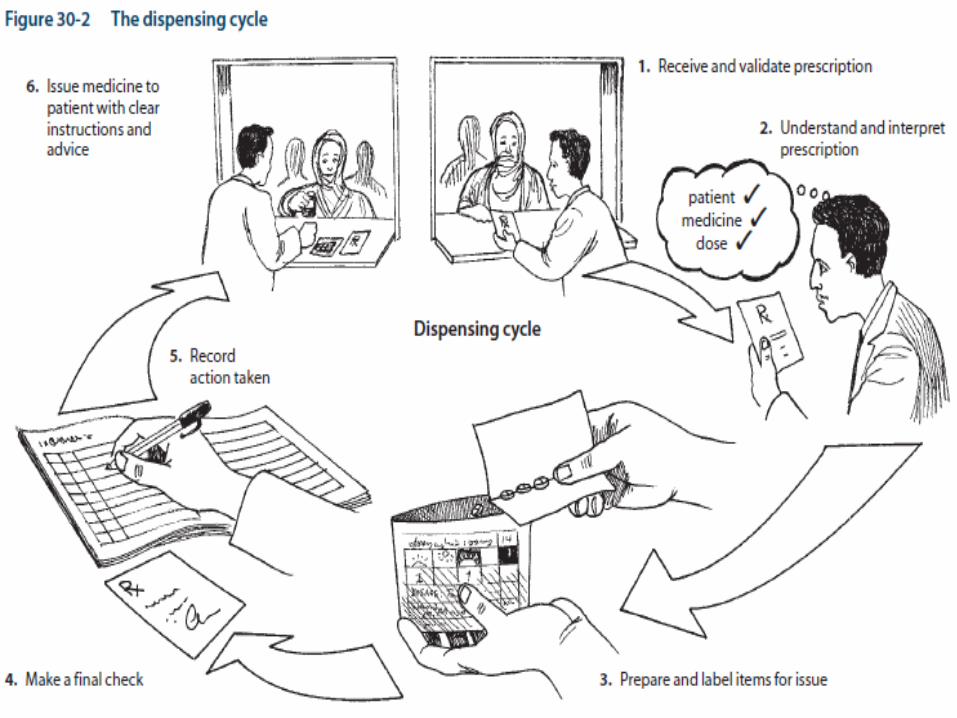
Medication errors (MEs) are defined as any mistake at any stage of the medication use process
•selection and procurement,
• storage,
• ordering and transcribing,
• preparing and dispensing,
• administration, or
• monitoring.
MEDICATION ERRORA medication error is any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the healthcare professional, patient or consumer.
Such an event may be related to professional practices, healthcare products, procedures and systems including prescribing, order communication, product labelling, packaging and nomenclature, compounding, dispensing, distribution, administration, education, monitoring and use.
Medication errors may be committed by both inexperienced and experienced personnel like doctors, pharmacists, dentists and other healthcare providers, patients, manufacturers, caregivers and others.
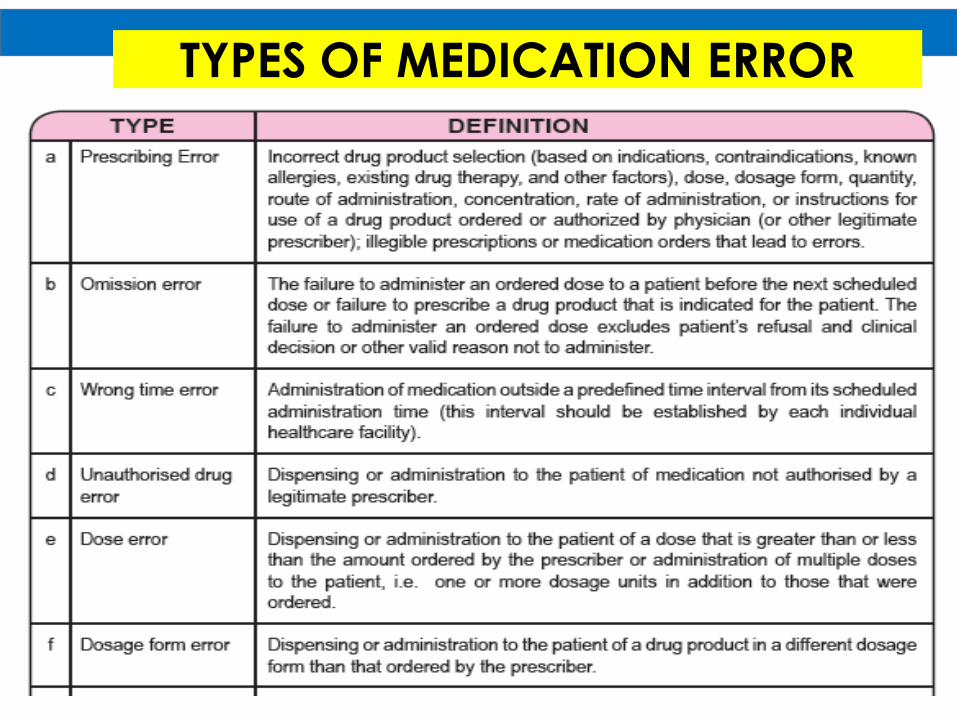
TYPES OF MEDICATION ERRORGeneral
ACEIs can be useful to prevent HF in patients at high risk for developing HF who have a history of atherosclerotic vascular disease, diabetes mellitus, or hypertension
Coronary Artery Disease
A b-Blockers are indicated in all patients without a history of MI who have a reduced left ventricular systolic dysfunction and no HF symptoms
Aspirin should be started at 75–162 mg/day and continued indefinitely in all patients unless contraindicated. Doses should not exceed 100 mg/day when used in combination with ticagrelor.
Clopidogrel 75 mg/day should be considered and continued indefinitely when aspirin is an absolute contraindication
Clopidogrel 75 mg/day or prasugrel 10 mg/day should be given in combination with aspirin after PCI for at least 12 mo after implantation of a either a bare metal stent or a drug-eluting stent
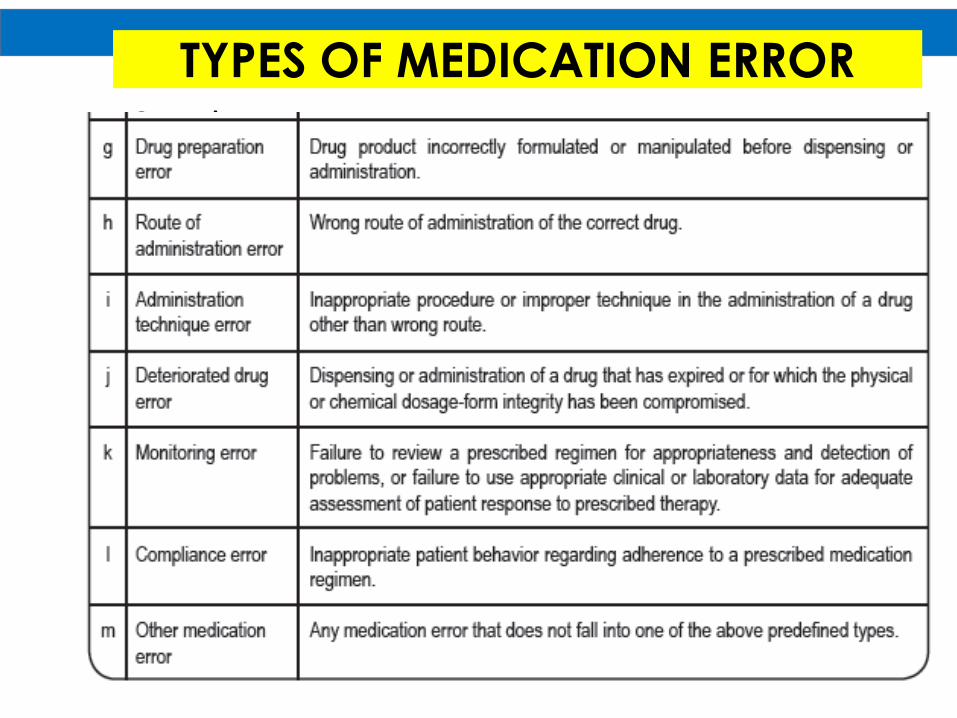
TYPES OF MEDICATION ERRORGeneral
ACEIs can be useful to prevent HF in patients at high risk for developing HF who have a history of atherosclerotic vascular disease, diabetes mellitus, or hypertension
Coronary Artery Disease
A b-Blockers are indicated in all patients without a history of MI who have a reduced left ventricular systolic dysfunction and no HF symptoms
Aspirin should be started at 75–162 mg/day and continued indefinitely in all patients unless contraindicated. Doses should not exceed 100 mg/day when used in combination with ticagrelor.
Clopidogrel 75 mg/day should be considered and continued indefinitely when aspirin is an absolute contraindication
Clopidogrel 75 mg/day or prasugrel 10 mg/day should be given in combination with aspirin after PCI for at least 12 mo after implantation of a either a bare metal stent or a drug-eluting stent
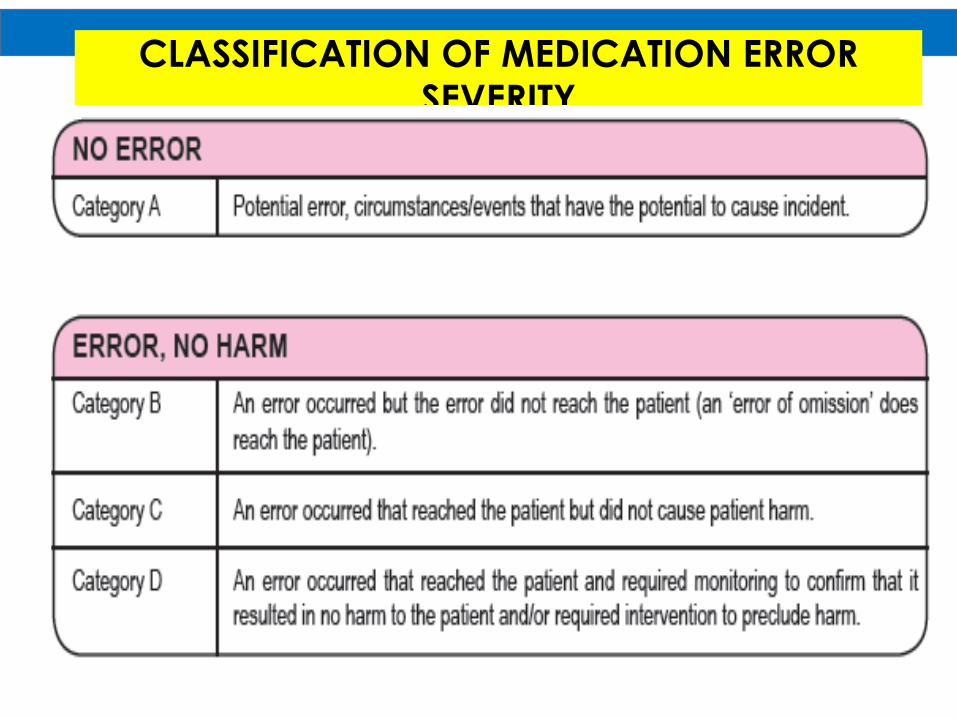
CLASSIFICATION OF MEDICATION ERROR
SEVERITYA medication error is any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the healthcare professional, patient or consumer.
Such an event may be related to professional practices, healthcare products, procedures and systems including prescribing, order communication, product labelling, packaging and nomenclature, compounding, dispensing, distribution, administration, education, monitoring and use.
Medication errors may be committed by both inexperienced and experienced personnel like doctors, pharmacists, dentists and other healthcare providers, patients, manufacturers, caregivers and others.
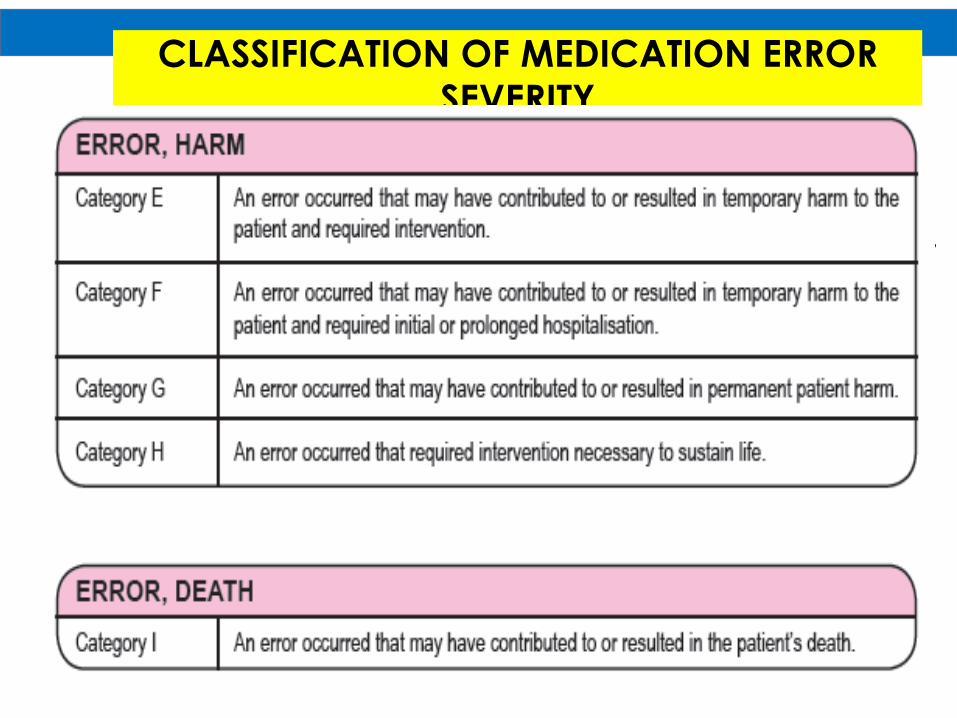
CLASSIFICATION OF MEDICATION ERROR
SEVERITYA medication error is any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the healthcare professional, patient or consumer.
Such an event may be related to professional practices, healthcare products, procedures and systems including prescribing, order communication, product labelling, packaging and nomenclature, compounding, dispensing, distribution, administration, education, monitoring and use.
Medication errors may be committed by both inexperienced and experienced personnel like doctors, pharmacists, dentists and other healthcare providers, patients, manufacturers, caregivers and others.
EMERGENCY
DEPARTMENT AS HIGH
RISK SITUATIONS
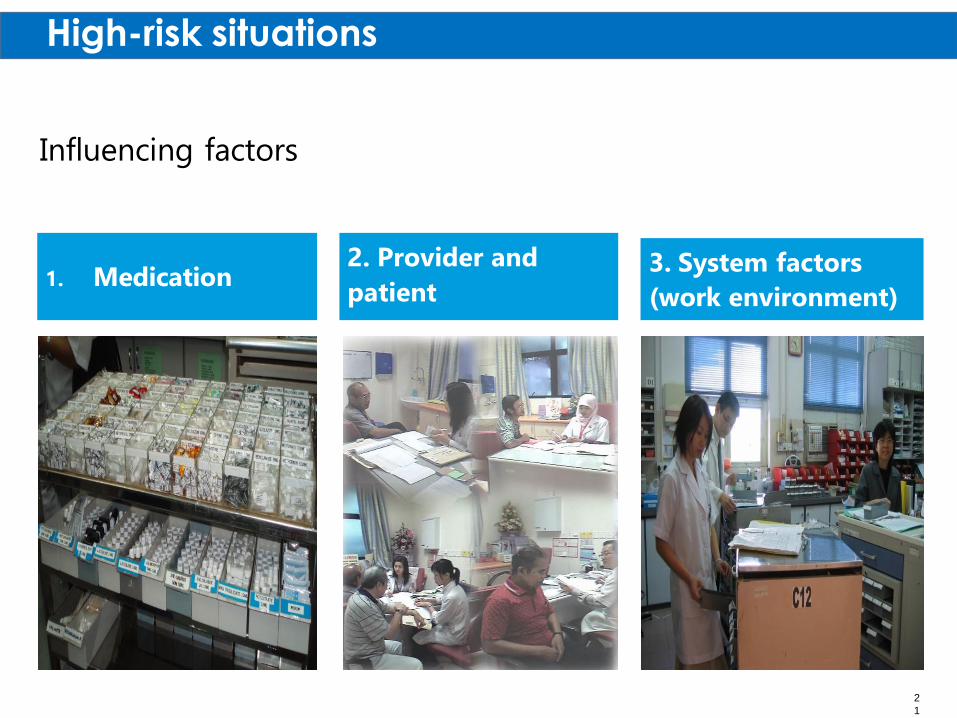
High-risk situations
1. Medication2. Provider and
patient3. System factors
(work environment)
Influencing factors
2
1
MEDICATION SAFETY IN
THE ED
MEDICATION FACTORS
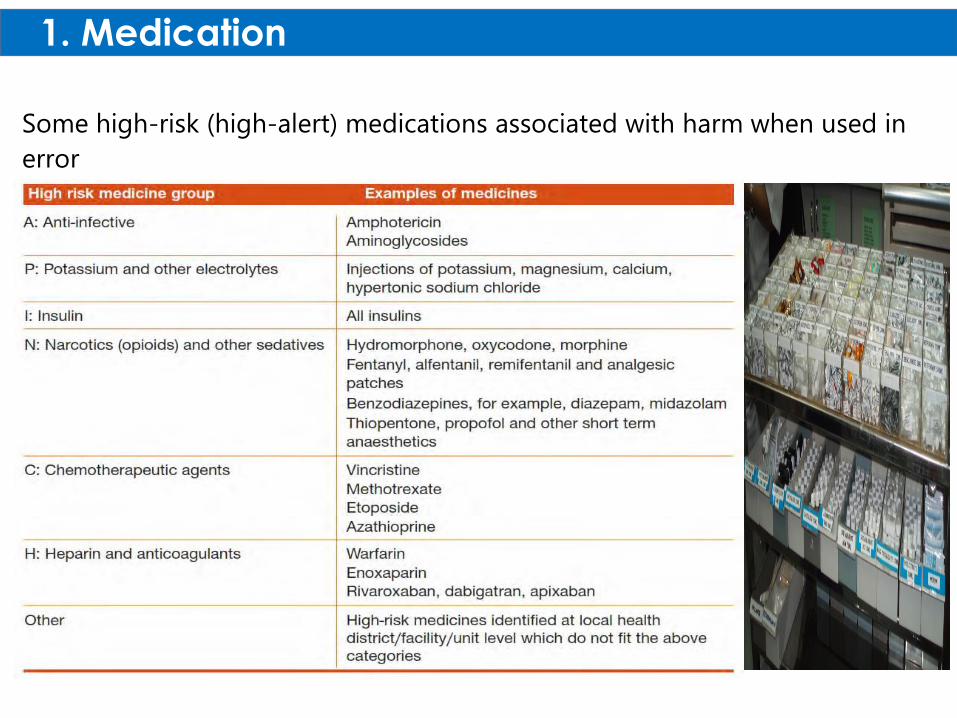
Some high-risk (high-alert) medications associated with harm when used in
error
1. Medication
factors
High Alert Medication
• Could cause an immediate life threatening condition for the patient if an error in administration occurs.
• Labeled with a red dot.
• Inj. Adrenaline• Inj. Digoxin• Tab. Warfarin• Inj. Potassium chloride 15%• Insulin
High Risk Medication
• Risk of causing significant patient harm when they are used in error.
• They are labeled with a yellow dot.
• Amiodarone
• Infusion. Dextrose 50%
• Inj. Metoprolol
• Inj. Phenytoin
• Tab. Glibenclamide
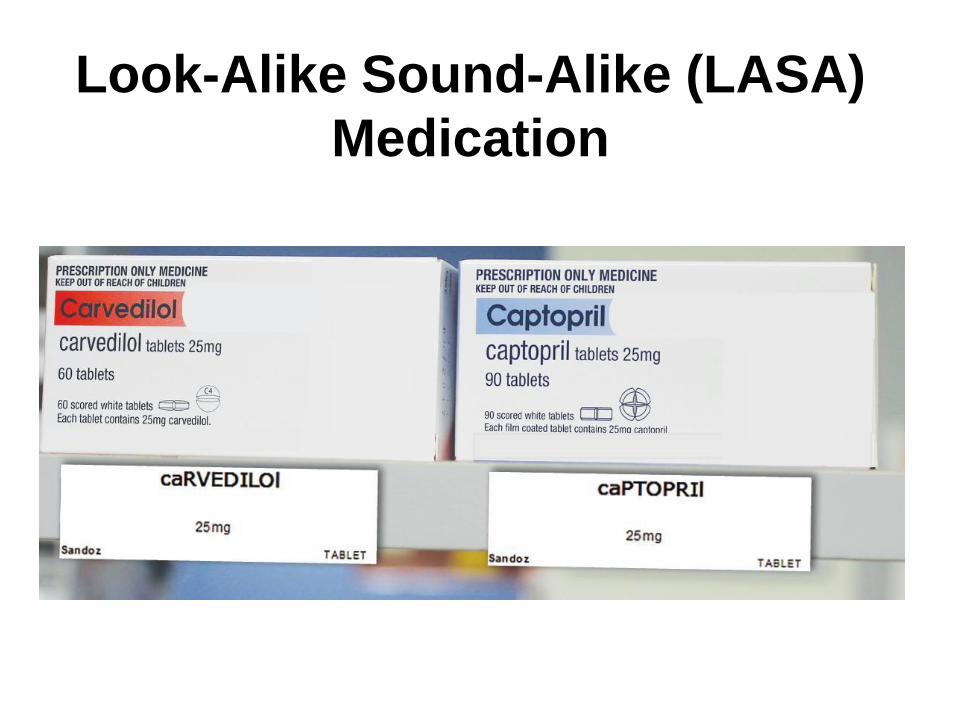
Look-Alike Sound-Alike (LASA)
Medication
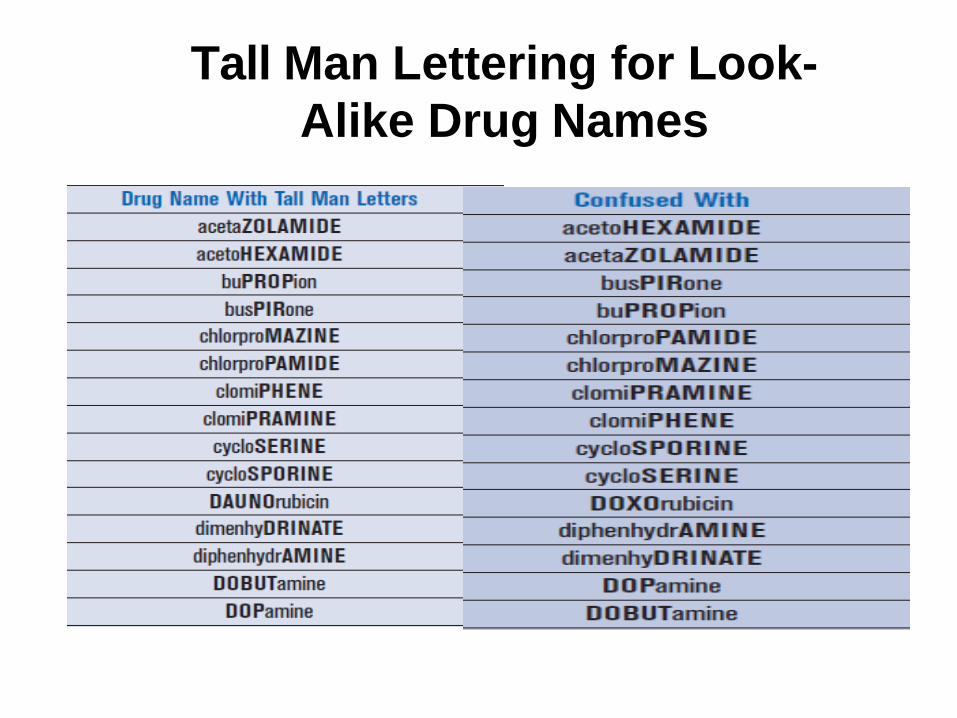
Tall Man Lettering for Look-
Alike Drug Names

Summaryensure the 5 Rs
Prescribing
Dispensing
Administering
RIGHT
1. Drug
2. Dose
3. Route
4. Time
5. Patient
MEDICATION SAFETY IN
THE ED
PROVIDER AND PATIENT
FACTORS
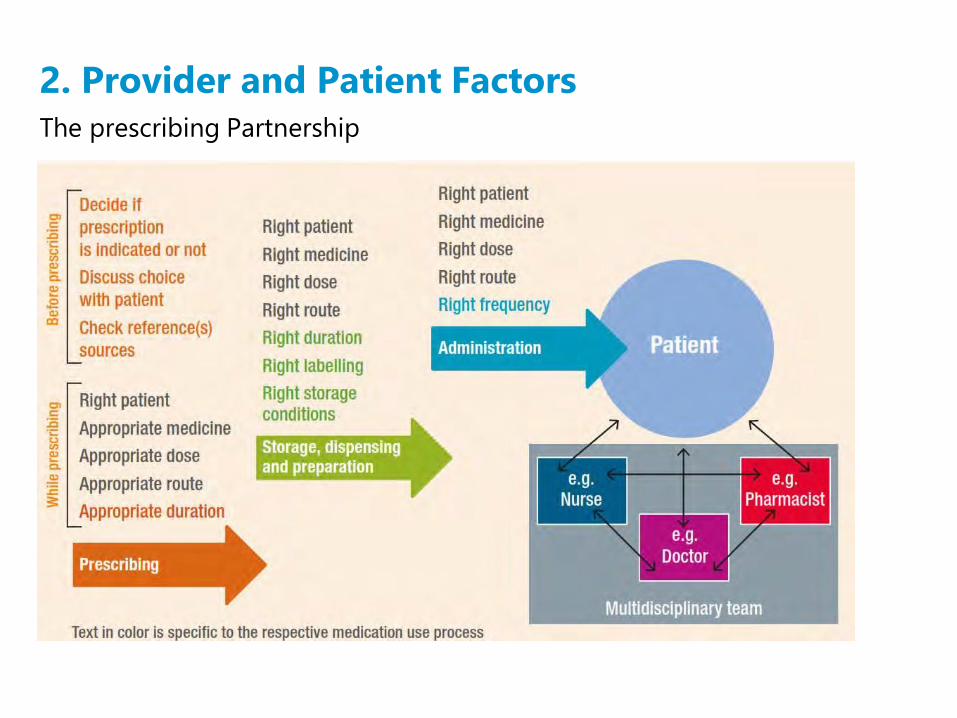
The prescribing Partnership
2. Provider and Patient Factors
Key
Points
ED pharmacy team could comprise of any or all
of the following:
Clinical Pharmacist
Pharmacist
Technician
Role of the ED pharmacist consist of clinical, administrative and
technical duties
Role of the ED technician is to support ED pharmacy team
Optimization involves ongoing evaluation of current practice
ED technician role could be further optimized through utilization
in medication reconciliation process
Limitations to implementation varies from one facility to another
Medication Histories
An accurate medication history is important to prevent medication errors and ADEs in the hospital and during transitions of care.
A multicenter evaluation of ED pharmacist–completed medicationhistories completed in a multicenter, double-blind, randomized fashionfound that discrepancies were reduced by 33% (OR 0.1055; 95% CI,0.05–0.24) compared with physician conducted medication histories(Becerra-Camargo 2013).
Pharmacists can obtain an accurate medication history (Patanwala2014). A program using ED pharmacists to address errors andinconsistencies in ED admission and discharge medicationreconciliations found that that admission medication histories obtainedby pharmacists were accurate more often than when obtained by anurse (90.2% vs. 66.7%, p < 0.05) (Nana 2012).
Transitions of Care
Recent initiatives have focused on providing effectiveand safe care during patient transitions.
In the ED, patients are either discharged or admitted.
The pharmacist or pharmacist- extender has manyopportunities to optimize medication management atthese transitions.
Boarding Patients
ED overcrowding causes a derangement in the usual workflow and throughput, leading EDs and institutionsto modify normal operating procedures for increased patient volume (Jellinek 2010).
Patients may “board” in the ED, even though they are admitted to the hospital. This causes problemsbecause inpatient provider teams are managing care, but EM nurses are still providing bedside care toboarding patients and new ED patients presenting.
This is not optimal and can lead to overall delays in new and routine medication therapies. One institutionchanged the nursing workflow to assign nurses to either ED patients or boarding patients, to prevent mixingboth designations.
An EM clinical pharmacist was also designated to follow up on boarding patients 1 hour after the scheduledmedication administration time to identify delays or issues. Two hundred sixty-six medicationadministration opportunities in 79 patients were evaluated.
The EM clinical pharmacist intervened by clarifying orders with the physician, expediting medication fromthe pharmacy, directly dispensing to the nurse, providing nurse education, or procuring medication a totalof 52 times (19.5%) (Jellinek 2010).
Cardiovascular, antimicrobial, respiratory, GI, and anticoagulant agents were the most common medicationsnot administered on time and requiring pharmacist intervention.
Medication Order Review and ConsultativeActivities
Over 6 months with 24-hour pharmacy services to the
ED, 3482 medications were prospectively reviewed by
EM clinical pharmacists for adult and pediatric patients,
and 642 (18.4%) clinical interventions were made (Sin
2015).Interventions described were nursing drug information
(27.7%),
Dose or frequency adjustment (21.1%),
Physician drug information (18.2%),
Antibiotic recommendations (15.1%),
Titration of intravenous drug therapy (9.3%),
Initiation/change drug therapy (5.1%), and
Duplication (3.2%).
Medication Order Review and ConsultativeActivities
A separate, multicenter, prospective study collected medication errorsintercepted over 1000 hours of EM clinical pharmacist time and focusedon the activities that led to these medication error interceptions. Thesites were geographically diverse and represented both academic andcommunity sites (Patanwala 2012a).Of the 364 confirmed medication error interceptions for 16,446patients, involvement in consultative activities resulted in the mosterrors intercepted (51.4%), followed by review of medication orders(34.9%). Most medication orders resulting in medication errors werewritten or computerized (54.4%); however, 32.7% were verbal.
These data show the importance of clinicalpharmacists physically in the ED and participating indirect patient care at the bedside.
Medication Event Reporting
A review of medication-error reports over 3.5 years at one
academic medical center found that dedicated EM clinical
pharmacists reported 94.5% of medication errors compared
with other health care professionals (5.7%, p < 0.001)(Weant
2010b).
Moreover, adding two dedicated EM clinical pharmacists was
associated with 14.8 times the number of medication error
reports completed by pharmacy personnel compared with
when there were no dedicated ED pharmacy services.
These are important results because error reporting is
crucial for systems improvement and safeguarding
implementation.
PHARMACIST INTEGRATION INTO THE EM TEAM
The ED can be a difficult patient care setting.
ED has high volume, high patient acuity, wide range of
disease state management.
The evening and early overnight hours are the busiest
times, with a constant influx of patients, packed waiting
rooms, and many patients in hallway beds or chairs
because the ED or hospital is at maximum capacity at
many institutions.
In this environment, sustainability of staff is difficult, and
high turnover is evident.
PHARMACIST INTEGRATION INTO THE EM TEAM
. Electronic prescribing can be enhanced for:
• Disease state–specific medication order sets or order
panels
• Creation of ED-specific medication preference lists
Drive prescribing practices to formulary medications
Aid in correct formula/concentration selection and
administration of medications with alternative routes of
administration
■■ Intranasal administration of midazolam for minimal
sedation or tranexamic acid–soaked packing for
epistaxis
○○ Inclusion of medications available in the automatic dispensing
cabinets
■■ Improve time to medication administration and ED
throughput
Education
Several opportunities exist for educating ED staff. Together with bedside education during pharmacotherapy consults for clinicians and nurses, other teaching opportunities are often offered.
Providing formal didactic education or whiteboard teaching for attendings and EM medical resident, facilitating simulation activities for EM clinicians and nurses,and providing nursing in-services and hands-on sessions (for medication preparation or electronic smart pumps) fornurses working with high-risk medications are examples.
It is important that EM clinical pharmacists volunteer for these education opportunities, not only to continue improving relationships with the interdisciplinary team but also to demonstrate expertise, which will ultimately improve the frequency at which providers reach out for pharmacotherapy consults.
MEDICATION SAFETY IN
THE ED
PRACTICE POINTS
STRAEGIES
ED
Pharmacist
Roles
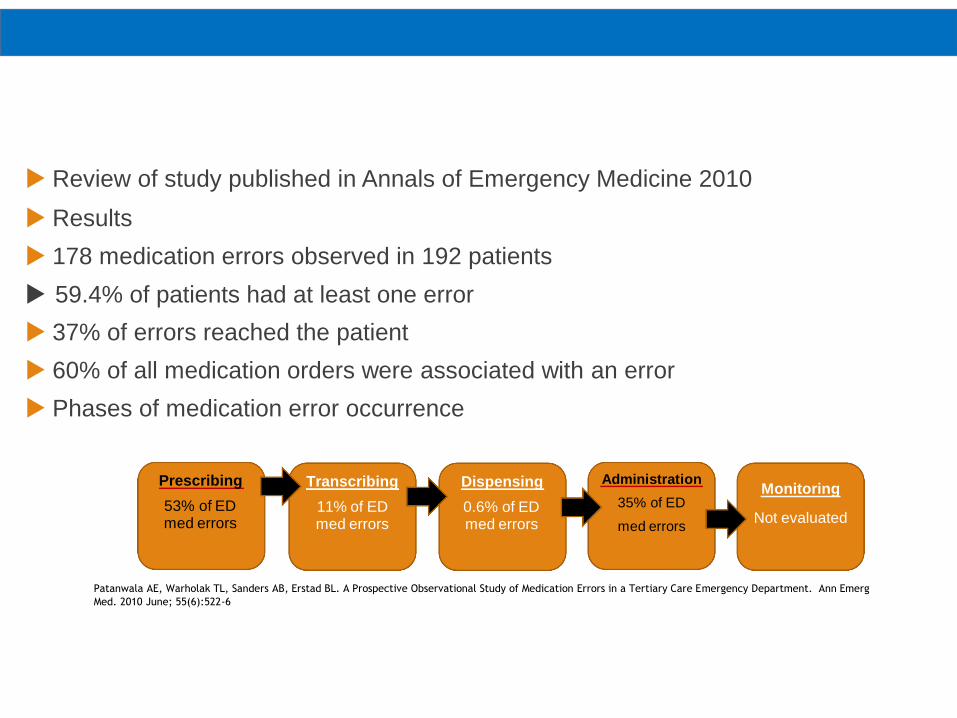
Review of study published in Annals of Emergency Medicine 2010
Results
178 medication errors observed in 192 patients
59.4% of patients had at least one error
37% of errors reached the patient
60% of all medication orders were associated with an error
Phases of medication error occurrence
Patanwala AE, Warholak TL, Sanders AB, Erstad BL. A Prospective Observational Study of Medication Errors in a Tertiary Care Emergency Department. Ann Emerg
Med. 2010 June; 55(6):522-6
Prescribing
53% of EDmed errors
Transcribing
11% of EDmed errors
Dispensing
0.6% of EDmed errors
Administration
35% of ED
med errors
Monitoring
Not evaluated
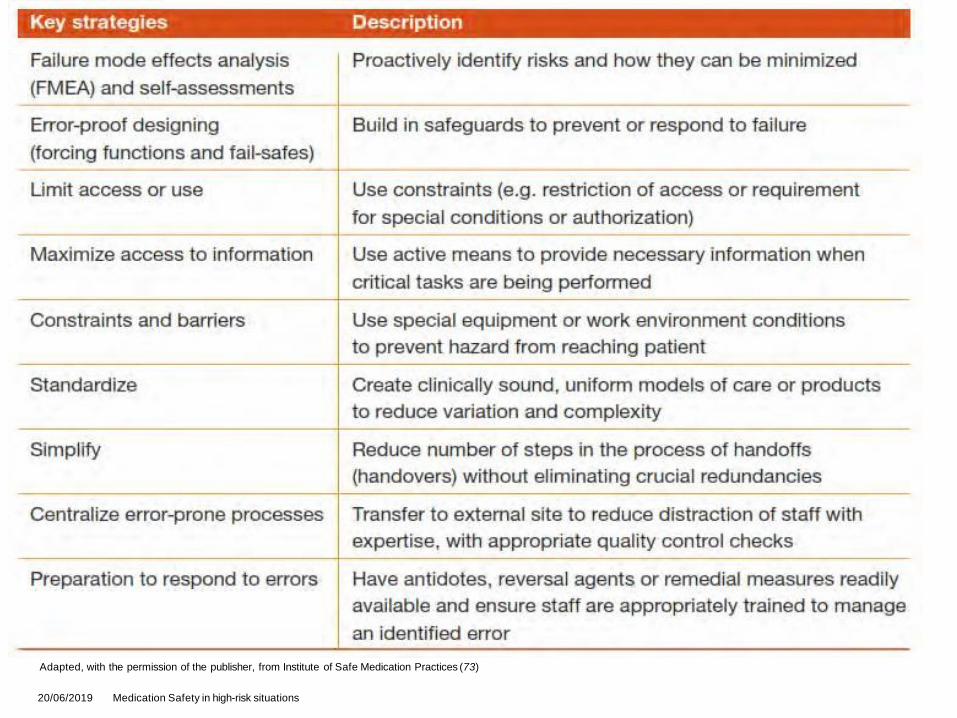
Adapted, with the permission of the publisher, from Institute of Safe Medication Practices (73)
Key Strategies for medication
safety
20/06/2019 Medication Safety in high-risk situations

Practice Points
Key points for pharmacists involved in patient care in
the ED include the following:
• EM clinical pharmacists must be well versed in both
ambulatory and critical care disease states because most
patients are discharged from the ED.
• Clinical activities involving direct patient care should
account for the most pharmacist time in the ED.
• Time-dependent emergency response should be a priority
because these patients have a high likelihood of
decompensation, medication errors, and use of high-risk
medications.
Practice Points
• ASPs in the ED focus on appropriate drug selection, dose,
and duration; rapid initiation of antibiotics; and prevention
of patient re-presentation to the ED and hospital
readmissions.
• Pharmacists improve medication safety and prevent ADEs
in the ED.
• Most medication errors are captured through consultative
activities compared with medication order review, showing
that pharmacists must be physically present in the ED.
Practice Points
• Cost avoidance estimated from ADE prevention and
through pharmacist intervention is one way to justify
pharmacist services in the ED.
• Pharmacist-extenders and not EM clinical pharmacists
should complete medication histories.
• The ED provides a unique setting for pharmacists to focus
on transitions of care because patients are both being
admitted and being discharged.
• Many pathways for training and resources are available forEM clinical pharmacists.
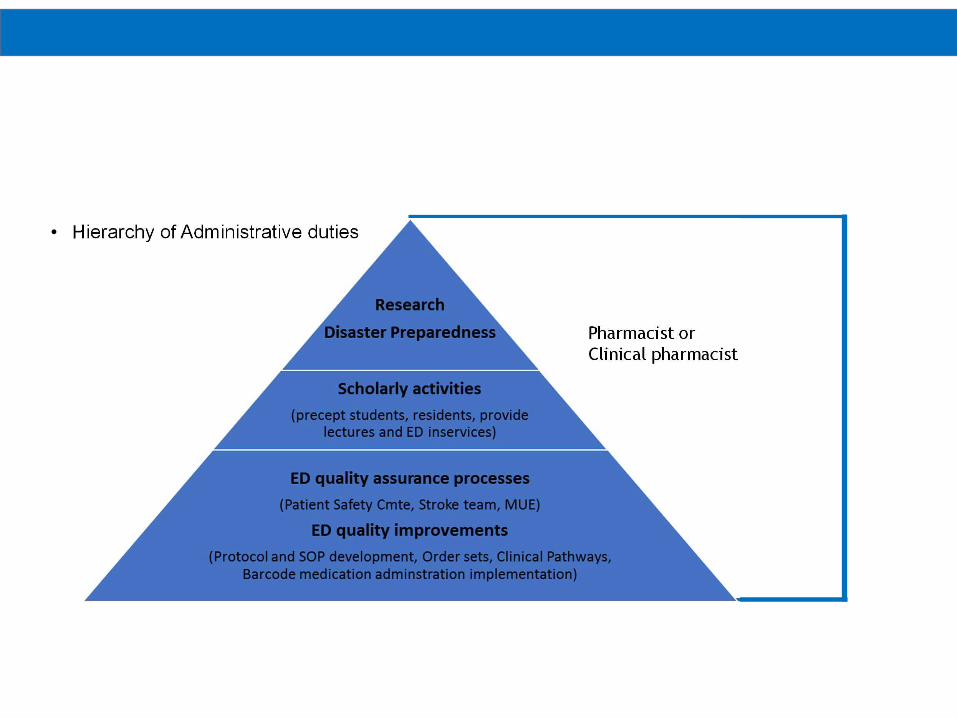
ED Pharmacist Role -
Administrative• Hierarchy of Administrative duties
Pharmacist or
Clinical pharmacist
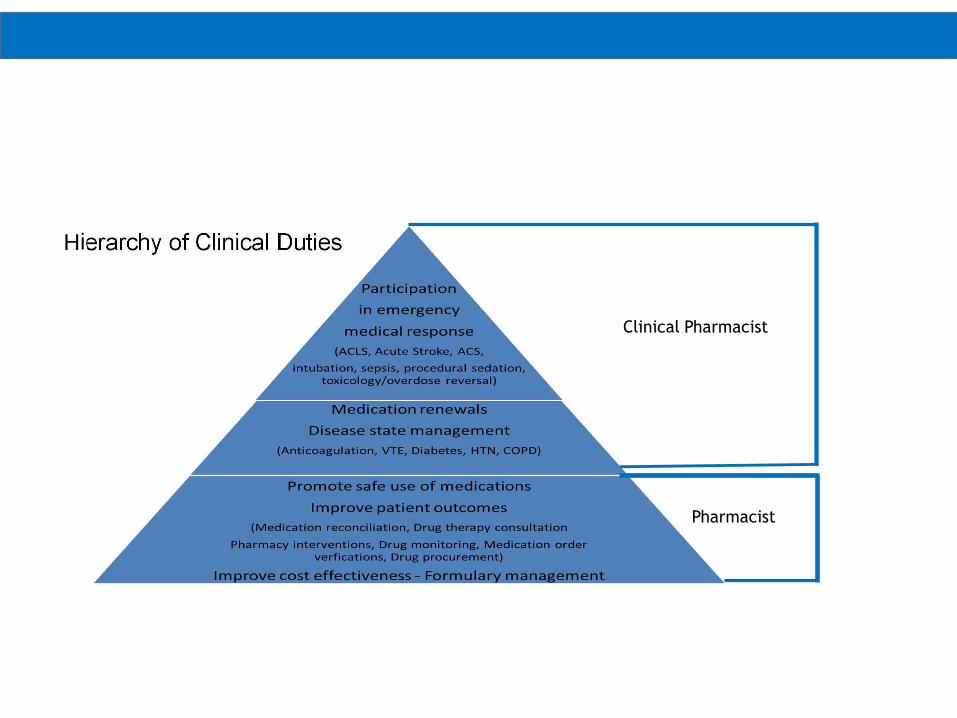
ED Pharmacist
Role - ClinicalHierarchy of Clinical Duties
Clinical Pharmacist
Pharmacist
EM Clinical Pharmacy Practice Guidelines
EM Clinical Pharmacy Practice Guidelines
In 2008, ASHP published a statement on ED pharmacy services
(ASHP 2008). Regardless of institution size or needs, the core roles should include:• Working with EM physicians, nurses, and other members of the EM team to develop and monitor medication use systems that promote safe and effective medication use in the ED• Collaborating with the interdisciplinary team to promote medication use that is aligned with national quality indicators• Participating in the selection, implementation, and monitoring of technology used in the medication use process• Providing direct patient care as part of the EM team• Participating in and leading quality improvement and emergency preparedness efforts• Educating not only patients but also the EM team about safe and effective medication use• Conducting ED-based clinical research and expanding pharmacy education and postgraduate training focused on EM
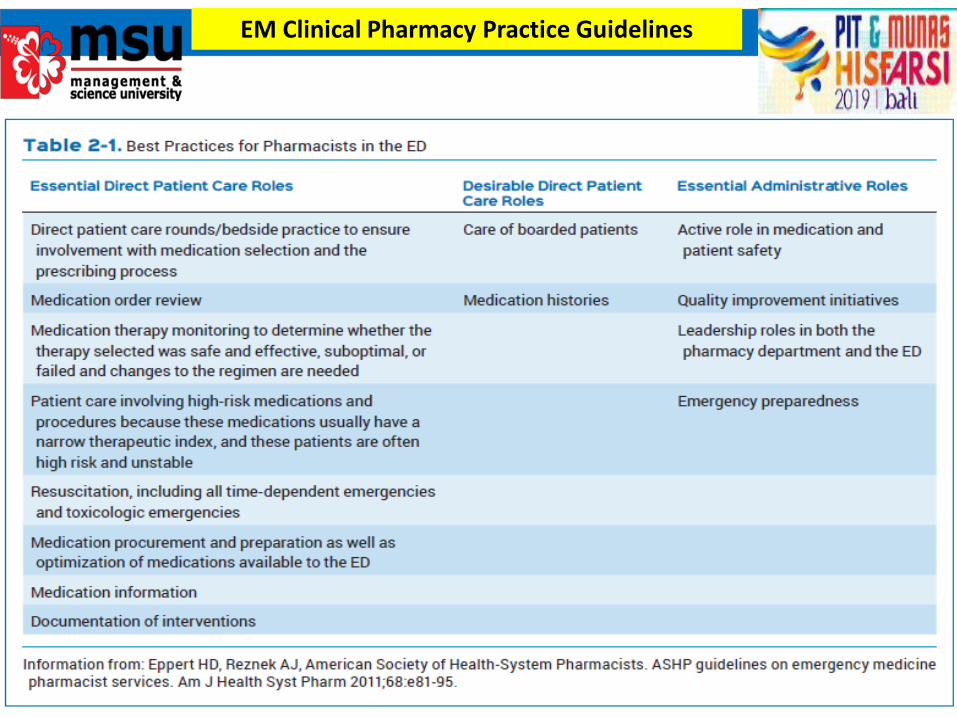
EM Clinical Pharmacy Practice Guidelines
CONCLUSION
Overall, the ED continues to need
direct pharmacy involvement because
EM clinical pharmacists have many
opportunities to affect patient care and
more pharmacists and increased
training opportunities are still needed in
this setting.
THANK YOU