Embed Size (px)
Citation preview
DOI: 10.1542/peds.2013-1451; originally published online September 2, 2013; 2013;132;730Pediatrics
Meghan E. McGrady and Kevin A. HommelA Systematic Review
Medication Adherence and Health Care Utilization in Pediatric Chronic Illness:
http://pediatrics.aappublications.org/content/132/4/730.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2013-1451; originally published online September 2, 2013; 2013;132;730Pediatrics
Meghan E. McGrady and Kevin A. HommelA Systematic Review
Medication Adherence and Health Care Utilization in Pediatric Chronic Illness:
ServicesUpdated Information &
mlhttp://pediatrics.aappublications.org/content/132/4/730.full.htincluding high resolution figures, can be found at:
Supplementary Material
8/peds.2013-1451.DCSupplemental.htmlhttp://pediatrics.aappublications.org/content/suppl/2013/08/2Supplementary material can be found at:
References
ml#ref-list-1http://pediatrics.aappublications.org/content/132/4/730.full.htat:This article cites 40 articles, 13 of which can be accessed free
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by Gerri Mattson on October 1, 2013pediatrics.aappublications.orgDownloaded from

Medication Adherence and Health Care Utilization inPediatric Chronic Illness: A Systematic Review
abstractBACKGROUND AND OBJECTIVE: Advanced understanding of modifiablepredictors of health care use in pediatric chronic illness is critical toreducing health care costs. We examined the relationship betweenmedication non-adherence and health care use in children andadolescents who have a chronic medical condition.
METHODS: A systematic review of articles by using PubMed, PsycINFO,and CINAHL was conducted. Additional studies were identified bysearching reference sections of relevant manuscripts. Studies thattested the relationship between medication non-adherence andhealth care use (ie, hospitalizations, emergency department visits,outpatient visits) or cost in children and adolescents (mean age #18years) who have a chronic medical condition were included. Extraction ofarticles was completed by using predefined data fields.
RESULTS: Ten studies met our inclusion criteria. Nine of the 10 studiesreviewed (90%) demonstrated a relationship between medication non-adherence and increased health care use. The directionality of thisrelationship varied depending on the outcome variable of interest.
CONCLUSIONS: Medication non-adherence is related to increasedhealth care use in children and adolescents who have a chronicmedical condition and should be addressed in clinical care. Futurestudies should include randomized controlled trials examining theimpact of adherence promotion efforts on health care use andcosts. Pediatrics 2013;132:730–740
AUTHORS: Meghan E. McGrady, PhD and Kevin A. Hommel,PhD
Division of Behavioral Medicine and Clinical Psychology, Centerfor Adherence and Self-Management, Cincinnati Children’sHospital Medical Center, Cincinnati, Ohio
KEY WORDSmedication adherence, health care costs, health care quality,access, and evaluation, chronic disease
ABBREVIATIONSED—emergency departmentMPR—medication possession ratio
Dr McGrady contributed to the manuscript by aiding inconception and design, acquisition of data, analysis andinterpretation of data, drafting of manuscript, and statisticalanalysis; Dr Hommel contributed to the manuscript by aiding inconception and design, analysis and interpretation of data,critical revision of the manuscript for important intellectualcontent, and supervision; and both authors approved the finalmanuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-1451
doi:10.1542/peds.2013-1451
Accepted for publication Jul 23, 2013
Address correspondence to Meghan E. McGrady, PhD, Center forAdherence and Self-Management, Cincinnati Children’s HospitalMedical, Center MLC 7039, 3333 Burnet Ave, Cincinnati, OH 45229-3026. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: The design and conduct of the study; collection,management, analysis, and interpretation of the data; andpreparation of the manuscript were supported in part by grantT32HD068223 for Dr McGrady. Dr Hommel is funded in part byR01HD067174. Funded by the National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential conflicts of interest to disclose.
730 McGRADY and HOMMEL

In 2010, the United States spent $2.6trillion on health care, an increase of3.9% from 2009, and 17.9% of its grossdomestic product.1 Hospital care andphysician and clinical services (ie,emergency department [ED] visits,hospitalizations, and office visits, here-after defined as “health care use”) arethe 2 largest components of health carespending,2,3 and accounted for over 50%of the growth in health care spendingfrom 2009 to 2010.1 Continued risinghealth care costs despite the recession,the increasing US national deficit, andthe increasing percentage of US healthspending financed by the government($1.2 trillion, 45% of all US healthspending) have prompted investigationof modifiable factors to reduce healthcare use and associated costs.4 Al-though there is no single strategy foreffectively controlling costs, research-ers have begun to focus on the 83% ofhealth care resources consumed byindividuals who have a chronic medicalcondition.4,5
The number of children and adoles-cents diagnosedwith a chronicmedicalcondition has been steadily increasingover the past 20 years,6 driven in partby increases in the prevalence of obe-sity7 and asthma8 as well as advancesin medical care that increase survival(eg, cystic fibrosis, kidney transplant).9,10
Increases in the prevalence of chronicmedical conditions have only increasedthe already disproportionate healthcare expenses accounted for by childrenand adolescents who have a chronicillness.5,11,12 In 2000, children andadolescents with a special health careneed made up 16% of youth butaccounted for 53% of hospital days.13
Consequently, targeting factors thatinfluence health care use in this pop-ulation may provide 1 of the greatestopportunities to reduce pediatrichealth care spending.
Non-adherence refers to a lack ofcorrespondence between patient
self-managementbehaviorandmedicalor health advice14 and significantlycontributes to health care use in adultswho have a chronic illness,15–18 ac-counting for an estimated 33% to 69%of adult hospital admissions and $100to $300 billion in annual health carecosts.19,20 Because much of the healthcare use attributable to non-adherenceincludes excess use of urgent care andhospitalizations for preventable com-plications,16 it represents avoidablecosts, an ideal target outcome forinterventions aimed at reducing healthcare spending. As non-adherence ismodifiable with intervention,21 adultadherence promotion efforts have be-gun to focus on both improving healthstatus and reducing health care use,resulting in programs that effectivelydecrease health care costs.15
Efforts to contain pediatric health carecosts could prove to be equally as ef-fective as adult-focused interventions,but have not yet been examined despitethe widespread nature of non-adherencein pediatrics. Approximately 63% ofchildren and adolescents who havea chronic illness are prescribed medi-cation,22 but 50% to 88% of childrenand adolescents are non-adherent totheir prescribed regimens.23–25 As inadult samples, pediatric non-adherencemay be a modifiable predictor of healthcare use and resulting health carecosts. For example, an adolescent whohas asthma may require hospitalizationafter failing to take his controller med-ication for several days and suffering anexacerbation. If his medical care in-cluded regular assessments of his ad-herence and adherence promotionefforts as necessary, this hospitaliza-tion and its associated costs may havebeen avoided.16,26
Understanding the impactof adherencepromotion interventions on health carecosts specific to pediatric populationsis necessary given the numerous de-velopmental factors thatmake pediatric
adherence unique (ie, influence of adultcaregivers and systems on adherence,evolution of illness burden with age,increasing autonomy for disease man-agement) and the variations in healthcare systems and outcomes across thelifespan. For example, health care fi-nancing for over one-third of childrenand adolescents is provided by Med-icaid and Children’s Health InsurancePrograms.27 With inconsistencies inbenefits and reimbursement ratesbetween states, it is difficult to com-pare health care costs across pediat-ric and adult samples. Furthermore,given the more advanced diseasecourse and higher likelihood of com-plications experienced by adults whohave a chronic illness, the benefits inquality of life and cost savings result-ing from pediatric prevention effortsare likely to be less visible in short-term evaluations typically used withthese populations.28
An increased understanding of the re-lationship between non-adherence andhealth careuse inpediatric populationspresents an opportunity to examinea highly prevalent and modifiable(amenable to behavioral intervention)potential contributor to pediatrichealth care costs. Unlike other stablepredictors of health care use (ie,gender, socioeconomic status), non-adherence can be modified with be-havioral intervention, and thus is ofclinical significance. If non-adherencecontributes to pediatric health careuse, there is the potential to have evengreater impact on health care usethan adult efforts, because long-termself-management behaviors are oftendeveloped in childhood and adoles-cence.23 Specifically, promoting adher-ence in pediatric populations may havethe potential to reduce short-termhealth care use as well as long-termhealth care use that may result fromthe increased morbidity associatedwith non-adherence.23
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 4, October 2013 731

Despite the potential significance, toour knowledge no studies have re-viewed the extant literature with a tar-geted examination of the relationshipbetweenmedicationnon-adherenceandhealth care use in children and ado-lescentswho have a chronic illness. Thisissue is timely as health care reformefforts and discussions regarding cov-ered services and service deliverymodels (ie, fee for service versus per-member, per month) move forward.We need to better understand howmodifiable factors contribute to healthcare costs and value to identify relevantand significant priorities of health carereform.Applicationoffindingswithadultpopulations would exclude many of theunique modifiable variables that impactpediatric adherence (ie, family func-tioning, caregiver involvement).14 Thepurpose of this systematic review is toprovide a comprehensive summary ofthe empirical studies examining therelationship between non-adherenceand health care use in childrenand adolescents who have a chronicmedical condition. Recommendationsfor advancing research in this fieldand policy implications are alsodiscussed.
METHODS
The systematic review was conductedin accordance with the publishedguidelines presented in the PreferredReporting Items for Systematic Reviewsand Meta-Analyses Statement.29
Data Search
PubMed, PsycINFO, and CINAHL weresearched in April 2013 for peer-reviewed original research articlespublished in English before April 2013.The search strategy included a combi-nation of Medical Subject Headingsterms (eg, chronic disease, patientcompliance,medicationadherence,healthcare costs, hospitalization, emergencyservice, ambulatory care) and key
words (eg, adherence, non-adherence,self-management, compliance, treat-ment concordance, health care utiliza-tion, outpatient visit, emergencydepartment, hospitalization, healthcare cost, service utilization, serviceuse, health care use, cost, chronic ill-ness, chronic care, chronic) (see Sup-plemental Information). To ensure allrelevant articles were captured, anadditional search was done replacingterms describing “chronic disease”with “diabetes,” “asthma,” or “HIV,” ef-fectively searching some of the mostdeveloped adherence literature basesin pediatrics (see Supplemental In-formation). The search did not includerestrictions on publication date orstudy design.
Study Selection and Screening
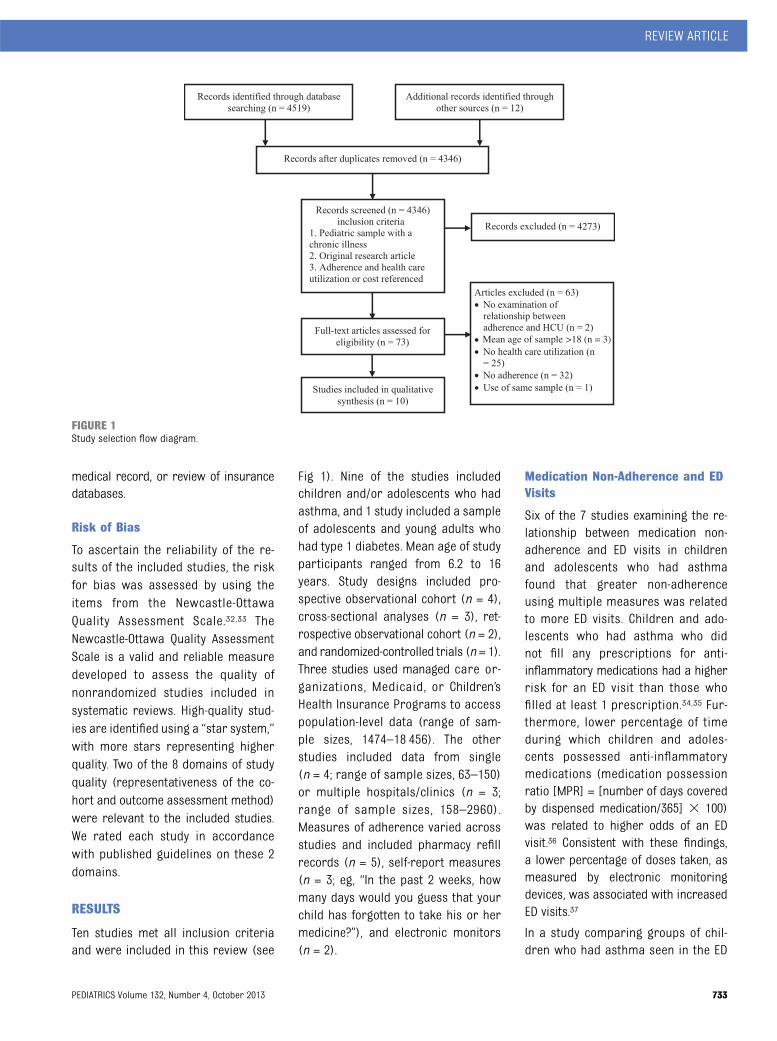
The Preferred Reporting Items forSystematic Reviews and Meta-Analyses4-phase flow diagram detailing studyselection is depicted in Fig 1.29 Theinitial search resulted in 4519 records.After the removal of duplicates, wescreened the abstracts of 4346 manu-scripts. Of these, 73 manuscripts metthe following inclusion criteria: (1)pediatric sample with a chronic illness;(2) original research article; and (3)mention of adherence and health careuse or cost. We then reviewed full-textversions of these 73 manuscripts. Weexcluded studies that did not assessnon-adherence and health care use,did not examine the relationship be-tween these variables, or includedparticipants with a mean age .18years.
Data Extraction
One reviewer (Dr McGrady) completeddata extraction from included articlesby using a standardized data collectionform. A second reviewer (Dr Hommel)checked the abstracted data for ac-curacy. Data retrieved from articlesincluded: (1) identification of the
manuscript (authors, year); (2) char-acteristics of participants (child age,child chronic illness, caregiver par-ticipating); (3) study design in accor-dance with published guidelines30
(cohort, cross-sectional, case-control,or randomized clinical trial); (4) mea-sure of non-adherence; (5) measure ofhealth care use; and (6) relationshipbetween non-adherence and healthcare use. In cases in which multiplemeasures of non-adherence or out-comes were used, all variables wereincluded. Questions regarding in-clusion or relevant data were resolvedvia discussion between authors.
Definitions of Variables
Measures of MedicationNon-Adherence
Medication non-adherence was as-sessed using measures of varyingvalidity and reliability,31 including self-report questionnaires, self-reportstructured interviews, electronic mon-itoring devices, prescription refill his-tories, and biochemical assays (seeTable 1). The time period during whichnon-adherence was assessed rangedfrom 24 hours to 365 days. Of note,somemeasures included non-adherencethreshold measurements with cut-points. As these cut-points differedacross studies, definitions of “good,”“high,” or “optimal” adherence pre-sented in this manuscript are thoseprovided by the authors of reviewedstudies.
Measures of Health Care Use
To facilitate comparison across stud-ies, we classified health care use dataas ED visits, outpatient visits, hospi-talizations, or “other” measures (eg,combined number of ED visits, out-patient visits, and hospitalizations) ofhealth care use. Measures of healthcare use were obtained via caregiverself-report, review of the electronic
732 McGRADY and HOMMEL
medical record, or review of insurancedatabases.
Risk of Bias
To ascertain the reliability of the re-sults of the included studies, the riskfor bias was assessed by using theitems from the Newcastle-OttawaQuality Assessment Scale.32,33 TheNewcastle-Ottawa Quality AssessmentScale is a valid and reliable measuredeveloped to assess the quality ofnonrandomized studies included insystematic reviews. High-quality stud-ies are identified using a “star system,”with more stars representing higherquality. Two of the 8 domains of studyquality (representativeness of the co-hort and outcome assessment method)were relevant to the included studies.We rated each study in accordancewith published guidelines on these 2domains.
RESULTS
Ten studies met all inclusion criteriaand were included in this review (see
Fig 1). Nine of the studies includedchildren and/or adolescents who hadasthma, and 1 study included a sampleof adolescents and young adults whohad type 1 diabetes. Mean age of studyparticipants ranged from 6.2 to 16years. Study designs included pro-spective observational cohort (n = 4),cross-sectional analyses (n = 3), ret-rospective observational cohort (n = 2),and randomized-controlled trials (n = 1).Three studies used managed care or-ganizations, Medicaid, or Children’sHealth Insurance Programs to accesspopulation-level data (range of sam-ple sizes, 1474–18 456). The otherstudies included data from single(n = 4; range of sample sizes, 63–150)or multiple hospitals/clinics (n = 3;range of sample sizes, 158–2960).Measures of adherence varied acrossstudies and included pharmacy refillrecords (n = 5), self-report measures(n = 3; eg, “In the past 2 weeks, howmany days would you guess that yourchild has forgotten to take his or hermedicine?”), and electronic monitors(n = 2).
Medication Non-Adherence and EDVisits
Six of the 7 studies examining the re-lationship between medication non-adherence and ED visits in childrenand adolescents who had asthmafound that greater non-adherenceusing multiple measures was relatedto more ED visits. Children and ado-lescents who had asthma who didnot fill any prescriptions for anti-inflammatory medications had a higherrisk for an ED visit than those whofilled at least 1 prescription.34,35 Fur-thermore, lower percentage of timeduring which children and adoles-cents possessed anti-inflammatorymedications (medication possessionratio [MPR] = [number of days coveredby dispensed medication/365] 3 100)was related to higher odds of an EDvisit.36 Consistent with these findings,a lower percentage of doses taken, asmeasured by electronic monitoringdevices, was associated with increasedED visits.37
In a study comparing groups of chil-dren who had asthma seen in the ED
FIGURE 1Study selection flow diagram.
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 4, October 2013 733
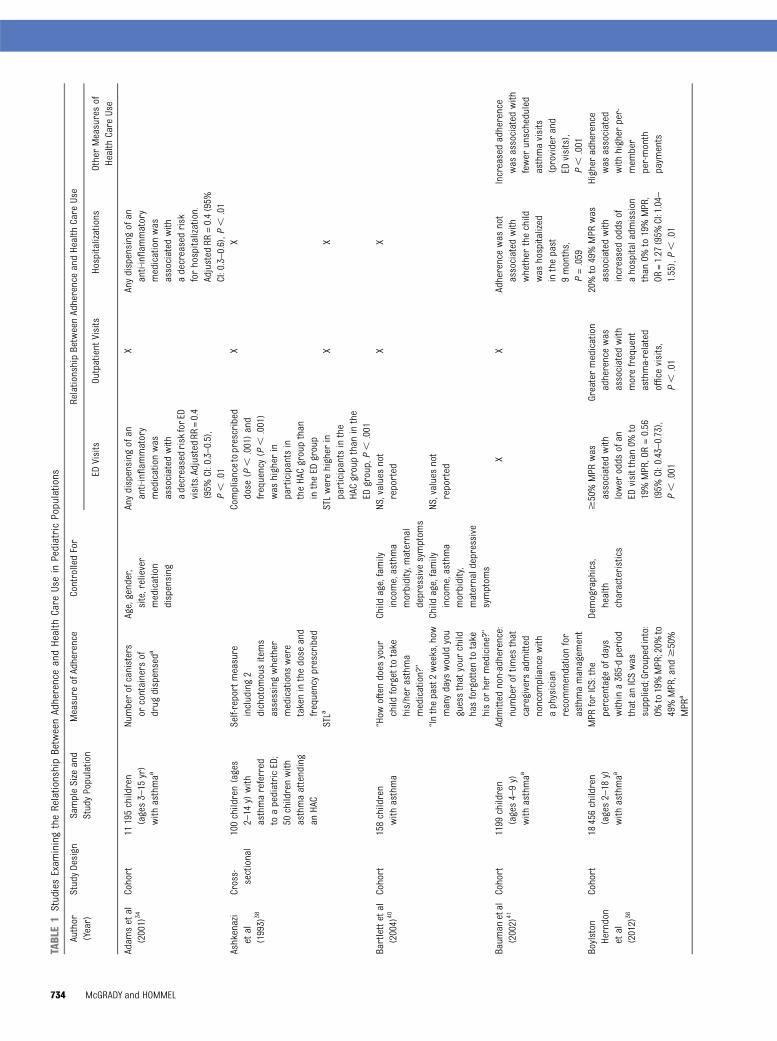
TABLE1
StudiesExam
iningtheRelationshipBetweenAdherenceandHealth
Care
Usein
PediatricPopulations
Author
(Year)
StudyDesign
SampleSize
and
StudyPopulation
Measure
ofAdherence
ControlledFor
RelationshipBetweenAdherenceandHealth
Care
Use
EDVisits
Outpatient
Visits
Hospitalizations
OtherMeasuresof
Health
Care
Use
Adam
setal
(2001)
34Cohort
11195children
(ages3–15
yr)
with
asthmaa
Numberofcanisters
orcontainers
ofdrug
dispenseda
Age,gender,
site,reliever
medication
dispensing
Anydispensing
ofan
anti-inflam
matory
medicationwas
associated
with
adecreasedrisk
forED
visits.AdjustedRR
=0.4
(95%
CI:0.3–0.5),
P,
.01
XAnydispensing
ofan
anti-inflam
matory
medicationwas
associated
with
adecreasedrisk
forhospitalization.
Adjusted
RR=0.4(95%
CI:0.3–0.6),P
,.01
Ashkenazi
etal
(1993)
38
Cross-
sectional
100children(ages
2–14
y)with
asthmareferred
toapediatricED;
50childrenwith
asthmaattending
anHAC
Self-reportmeasure
including2
dichotom
ousitems
assessingwhether
medications
were
takeninthedose
and
frequencyprescribed
Compliancetoprescribed
dose
(P,
.001)and
frequency(P
,.001)
was
higher
inparticipantsin
theHACgroupthan
intheED
group
XX
STLa
STLwerehigher
inparticipantsinthe
HACgroupthan
inthe
EDgroup,P,
.001
XX
Bartlettetal
(2004)
40Cohort
158children
with
asthma
“How
oftendoes
your
child
forgettotake
his/herasthma
medication?”
Child
age,family
income,asthma
morbidity,m
aternal
depressive
symptom
s
NS,valuesnot
reported
XX
“Inthepast2weeks,how
manydays
wouldyou
guessthatyour
child
hasforgottentotake
hisor
hermedicine?”
Child
age,family
income,asthma
morbidity,
maternaldepressive
symptom
s
NS,valuesnot
reported
Baum
anetal
(2002)
41Cohort
1199
children
(ages4–9y)
with
asthmaa
Admitted
non-adherence:
numberoftim
esthat
caregivers
admitted
noncom
pliancewith
aphysician
recommendationfor
asthmamanagem
ent
XX
Adherencewas
not
associated
with
whether
thechild
was
hospitalized
inthepast
9months,
P=.059
Increasedadherence
was
associated
with
fewer
unscheduled
asthmavisits
(providerand
EDvisits),
P,
.001
Boylston
Herndon
etal
(2012)
36
Cohort
18456children
(ages2–18
y)with
asthmaa
MPR
forICS:the
percentage
ofdays
withina365-dperiod
thatan
ICSwas
supplied;Groupedinto:
0%to19%MPR;20%
to49%MPR,and
$50%
MPR
a
Demographics,
health
characteristics
$50%MPR
was
associated
with
lower
odds
ofan
EDvisitthan0%
to19%MPR,OR=0.56
(95%
CI:0.43–0.73),
P,
.001
Greatermedication
adherencewas
associated
with
morefrequent
asthma-related
office
visits,
P,
.01
20%to49%MPR
was
associated
with
increasedodds
ofahospitaladm
ission
than
0%to19%MPR,
OR=1.27
(95%
CI:1.04–
1.55),P,
.01
Higher
adherence
was
associated
with
higher
per-
mem
ber
per-month
paym
ents
734 McGRADY and HOMMEL
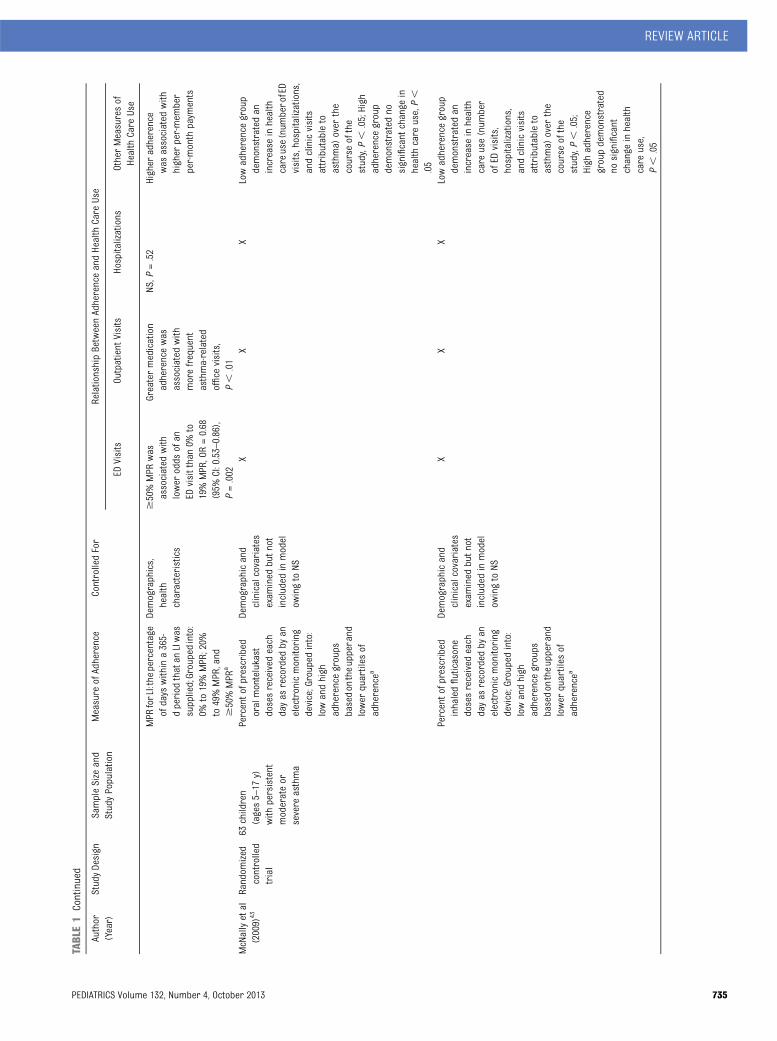
TABLE1
Continued
Author
(Year)
StudyDesign
SampleSize
and
StudyPopulation
Measure
ofAdherence
ControlledFor
RelationshipBetweenAdherenceandHealth
Care
Use
EDVisits
Outpatient
Visits
Hospitalizations
OtherMeasuresof
Health
Care
Use
MPR
forLI:the
percentage
ofdays
withina365-
dperiod
thatan
LIwas
supplied;Groupedinto:
0%to19%MPR;20%
to49%MPR,and
$50%MPR
a
Demographics,
health
characteristics
$50%MPR
was
associated
with
lower
odds
ofan
EDvisitthan0%
to19%MPR,OR=0.68
(95%
CI:0.53–0.86),
P=.002
Greatermedication
adherencewas
associated
with
morefrequent
asthma-related
office
visits,
P,
.01
NS,P
=.52
Higher
adherence
was
associated
with
higher
per-mem
ber
per-month
paym
ents
McNallyetal
(2009)
43Random
ized
controlled
trial
63children
(ages5–17
y)with
persistent
moderateor
severe
asthma
Percentofprescribed
oralmontelukast
dosesreceived
each
dayas
recorded
byan
electronicmonitoring
device;Grouped
into:
lowandhigh
adherencegroups
basedon
theupperand
lower
quartiles
ofadherencea
Demographicand
clinicalcovariates
exam
ined
butn
otincluded
inmodel
owingto
NS
XX
XLowadherencegroup
demonstratedan
increase
inhealth
careuse(num
berofED
visits,hospitalizations,
andclinicvisits
attributableto
asthma)
over
the
course
ofthe
study,P,
.05;High
adherencegroup
demonstratedno
significant
change
inhealth
care
use,P,
.05
Percentofprescribed
inhaledfluticasone
dosesreceived
each
dayas
recorded
byan
electronicmonitoring
device;Grouped
into:
lowandhigh
adherencegroups
basedon
theupperand
lower
quartiles
ofadherencea
Demographicand
clinicalcovariates
exam
ined
butn
otincluded
inmodel
owingto
NS
XX
XLowadherencegroup
demonstratedan
increase
inhealth
care
use(num
ber
ofED
visits,
hospitalizations,
andclinicvisits
attributableto
asthma)
over
the
course
ofthe
study,P,
.05;
High
adherence
groupdemonstrated
nosignificant
change
inhealth
care
use,
P,
.05
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 4, October 2013 735
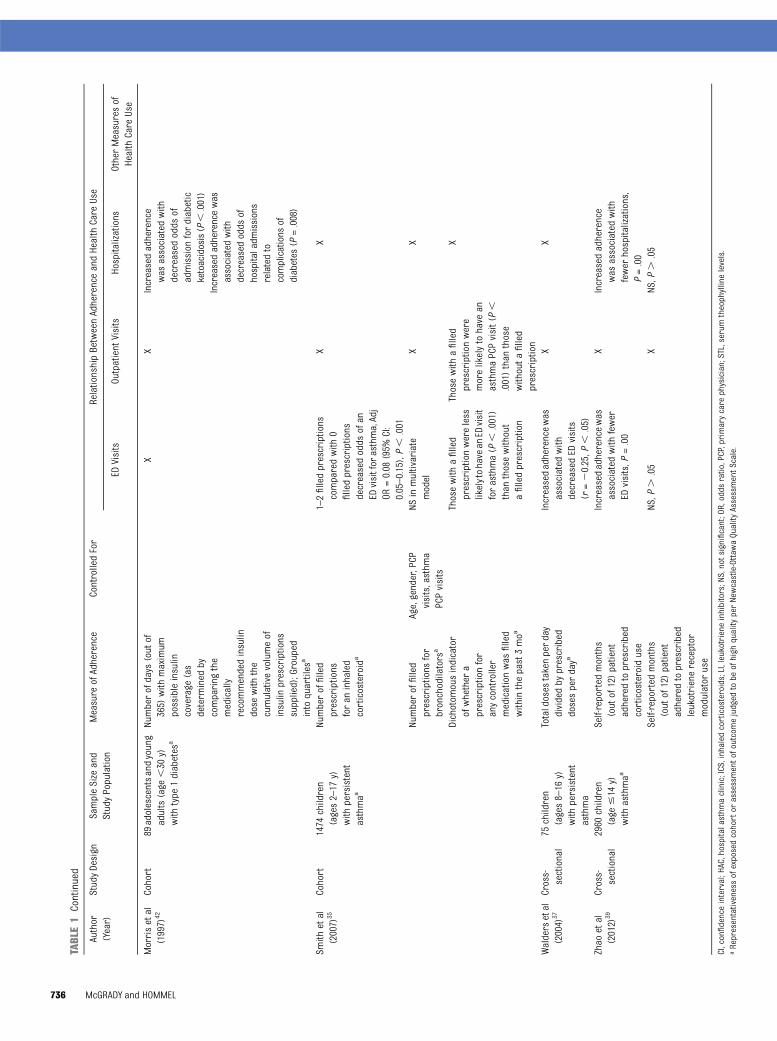
TABLE1
Continued
Author
(Year)
StudyDesign
SampleSize
and
StudyPopulation
Measure
ofAdherence
ControlledFor
RelationshipBetweenAdherenceandHealth
Care
Use
EDVisits
Outpatient
Visits
Hospitalizations
OtherMeasuresof
Health
Care
Use
Morrisetal
(1997)
42Cohort
89adolescentsandyoung
adults(age
,30
y)with
type
1diabetes
a
Numberofdays
(out
of365)
with
maximum
possibleinsulin
coverage
(as
determ
ined
bycomparing
the
medically
recommendedinsulin
dose
with
the
cumulativevolumeof
insulin
prescriptions
supplied);Grouped
intoquartiles
a
XX
Increasedadherence
was
associated
with
decreasedodds
ofadmission
fordiabetic
ketoacidosis(P,.001)
Increasedadherencewas
associated
with
decreasedodds
ofhospitaladm
issions
relatedto
complications
ofdiabetes
(P=.008)
Smith
etal
(2007)
35Cohort
1474
children
(ages2–17
y)with
persistent
asthmaa
Numberoffilled
prescriptions
foran
inhaled
corticosteroida
1–2filledprescriptions
comparedwith
0filledprescriptions
decreasedodds
ofan
EDvisitfor
asthma,Adj
OR=0.08
(95%
CI:
0.05–0.15),P,
.001
XX
Numberoffilled
prescriptions
for
bronchodilators
a
Age,gender,PCP
visits,asthm
aPCPvisits
NSinmultivariate
model
XX
Dichotom
ousindicator
ofwhether
aprescriptionfor
anycontroller
medicationwas
filled
withinthepast3moa
Thosewith
afilled
prescriptionwereless
likelytohavean
EDvisit
forasthma(P
,.001)
than
thosewithout
afilledprescription
Thosewith
afilled
prescriptionwere
morelikelytohave
anasthmaPCPvisit(P,
.001)than
those
withouta
filled
prescription
X
Waldersetal
(2004)
37Cross-
sectional
75children
(ages8–16
y)with
persistent
asthma
Totaldoses
takenperday
dividedby
prescribed
dosesperdaya
Increasedadherencewas
associated
with
decreasedED
visits
(r=20.25,P
,.05)
XX
Zhao
etal
(2012)
39Cross-
sectional
2960
children
(age
#14
y)with
asthmaa
Self-reported
months
(out
of12)patient
adheredtoprescribed
corticosteroiduse
Increasedadherencewas
associated
with
fewer
EDvisits,P
=.00
XIncreasedadherence
was
associated
with
fewer
hospitalizations,
P=.00
Self-reported
months
(out
of12)patient
adheredtoprescribed
leukotrienereceptor
modulator
use
NS,P
..05
XNS,P
..05
CI,confidenceinterval;HAC,hospitalasthm
aclinic;ICS,inhaled
corticosteroids;LI,leukotriene
inhibitors;NS,notsignificant;OR,odds
ratio,PCP,primarycare
physician;STL,serumtheophyllinelevels.
aRepresentativenessofexposedcohortor
assessmentofoutcom
ejudged
tobe
ofhigh
quality
perNewcastle-Ottaw
aQuality
AssessmentScale.
736 McGRADY and HOMMEL

to those seen in asthma clinic, self-reported non-adherence was higherin those seen in the ED.38 Similarly,caregiver report of more non-adherencewas associated with more ED visits forchildren who had asthma.39 In con-trast, a third study using a self-reportmeasure of adherence found no re-lationship between non-adherenceand ED visits when included in a multi-variate model.40
Medication Non-Adherence andOutpatient Visits
Both of the studies examining medica-tion non-adherence and outpatientvisits found that non-adherence wasassociated with fewer asthma-relatedoffice visits. In a sample of childrenwho had asthma, the fewer daysa child possessed inhaled cortico-steroids or leukotriene inhibitors, theless often asthma-related office visitsoccurred.36 Similarly, children who hadnot filled a prescription for a controllermedication in the past 3 months wereless likely than children who had filleda prescription to have an asthma pri-mary care physician visit.35
Medication Non-Adherence andHospitalizations
Findings of the 5 studies examiningmedication non-adherence and hospi-talizations were mixed and variedbased on method of adherence mea-surement. Four of these studies in-cluded children who had asthma and1 included adolescents and youngadults who had type 1 diabetes. Forchildren who had asthma, failing tofillanyprescriptionsforanti-inflammatorymedication was associated with anincreased risk for hospitalization.34
However, when MPRs for inhaled cor-ticosteroids were calculated andgrouped, those with 20% to 49% MPRhad increased odds of a hospital ad-mission as compared with those withan MPR of 0% to 19%.36 MPRs for
leukotriene inhibitors were not asso-ciated with hospitalizations.36
Caregiver self-reports of non-adherenceto corticosteroids were associatedwith more hospitalizations in a sampleof children who had asthma.39 In an-other sample, however, a compositescore comprised of asking caregiversyes/no questions related to their ad-herence to filling prescriptions, givingmore/less medication than prescribed,and obtaining recommended devicesyielded no relation to whether the childwas hospitalized in the past 9 months.41
In a sample of adolescents and youngadults who had type 1 diabetes, non-adherence was associated with in-creased odds for admission for diabeticketoacidosis and other diabetes-relatedcomplications.42
Medication Non-Adherence andOther Measures of Health Care Use
Similar to the aforementioned resultslinking non-adherence with more fre-quent ED visits, caregivers of childrenwith higher levels of self-reportednon-adherence also reported morefrequent unscheduled asthma visits(defined as provider and ED visits).41
Results of growth curve modelinganalyses suggest that medication non-adherence may be associated not onlywith rates of health care use, but alsochanges in health care use patterns.43
In a sample of African American chil-dren who had asthma, non-adherencewas associated with greater increasesin health care use over time than thosedemonstrated by groups of partic-ipants with better adherence.43
The only study to directly examinecosts related to non-adherence in-dicated that non-adherence wasassociated with lower per-member,per-month public insurance paymentsin a sample of children who hadasthma.36 As adherence to medicationrequires payment for prescriptions,Boylston Herndon et al found that
non-adherent children had lower drug-related costs than children with higheradherence levels. In this study, thecosts saved by not filling prescriptionswere more than the increased costs ofvisiting the ED or being hospitalizedincurred by these participants.
Risk for Bias
Risk for bias as identified by the itemsfrom the Newcastle-Ottawa QualityAssessment Scale and the inclusion ofconfounding variables is presented inTable 1. Three of the 10 studies (33%)included a cohort likely representa-tive of the relevant pediatric pop-ulation. Over three-quarters of studies(n = 8, 80%) used objective outcomemeasures.
DISCUSSION
Nine of the 10 studies reviewed (90%)demonstrated a relationship betweenmedication non-adherence and increa-ses in at least 1 health care use vari-able. Of note, the directionality of therelationship between medication non-adherence and health care use depen-ded on the outcome of interest. Themajority of studies examined reportedthat medication non-adherence wasassociated with more ED visits andhospitalizations.
The relationship between medicationnon-adherence and ED visits and hos-pitalizations is consistent with findingsin adult samples18,44,45 and suggeststhat there is potential to reduce the$1800 per child spent on hospital carein 2010.46 Children and adolescentswho were non-adherent suffered frommore exacerbations and complicationsrequiring medication attention andthus required more ED visits or hospi-talizations.
Although non-adherence was linkedwith more ED visits and hospital-izations, it was also related to feweroutpatient visits.35,36 These studies did
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 4, October 2013 737

not differentiate between recom-mended outpatient visits (eg, regularlyscheduled planned clinic visits) andexcessive outpatient visits (eg, sickvisits that may have been preventedwith optimal adherence), and are likelyillustrating the relationship betweenmultiple aspects of treatment adher-ence. Specifically, patients who arenon-adherent to 1 aspect of theirmedical regimen (taking medication)are also more likely to be non-adherentto other parts of their medical regimen(attending regular clinic appoint-ments). Thus, this relationship mayrepresent non-adherence to recom-mended necessary treatment (bothmedications and clinic attendance) asopposed to less excessive health careuse.
In all, thefindings of this review suggestthatmedication non-adherence is likelyan important contributor to health careuse in pediatric chronic illness pop-ulations. Clinically, these results sug-gest that interventionefforts to improveadherencemayresult in reducedhealthcare use and ultimately reduced healthcarecosts.Currentlyavailablepediatricadherence interventions can effec-tively improve adherence and healthoutcomes.21,47 To our knowledge, nostudies have examined the cost-effectiveness of adherence inter-ventions with pediatric populations.Emerging adult literature, however,suggests that the reduced healthcare and indirect (eg, productivityloss, absenteeism) costs significantlyoutweigh the costs of implementing
behavioral adherence-promoting inter-ventions.48–51
Several limitations and resultingimplications for future research exist.First, the relatively small number ofstudies that met inclusion criteria andthe varied risk for bias across studiesindicate that this is a nascent area ofresearch that requires further in-vestigation. To broaden the literaturebase in this important field, future re-search examining adherence shouldinclude health care use and cost anal-yses and be conducted with additionalillness populations. Including addi-tional illness populations is of partic-ular importance, as it will allow for animproved understanding of how ad-herence relates to health care costsacross a variety of illnesses with vary-ing medical regimens and health careusepatterns. Second, the observationalstudy design of the reviewed manu-scripts negates the possibilities of de-termining the implicationsof improvingadherenceonhealthcareuseandcosts.Future research should examine thisquestion in the context of randomizedcontrolled trials using longitudinaldata. Third, as the method of assessingadherence varied significantly betweenstudies, it is not possible to directlycompare results. Given the significantimplications of this research, futureefforts should use evidence-basedmethods of adherence assessment.31
Fourth, currently available methodscan result in misleading findings, suchas cost-savings associated with lowerdrug-related costs attributable to
non-adherence. Researchers usingrelatively brief follow-up periods cap-ture only the short-term drug costsavings realized from non-adherenceand not the long-term, more costlyconsequences (eg, more frequenthospitalizations) of non-adherence.Thus, future research should addressthis methodologic issue by longitudinaldesigns that account for expectedcosts (eg, medication refills) versusunexpected costs (eg, ED visits) andfollow participants for periods of timethat allow for long-term consequencesof non-adherence to be realized. Fifth,the generalizability of our findings tonon-Western populations may be lim-ited by our exclusion of non-Englishmanuscripts. As the prevalence ofnon-adherence is a global concern,15
more inclusive reviews should be con-sidered.
Resources allocated to improving ad-herence are often fairly limited. In thecurrent economic and political cli-mate, however, increasing attentionhas been paid to novel approaches toimproving health outcomes while re-ducing spending. Results of this reviewsuggest that targeting non-adherencein children and adolescents who havea chronic illness may provide a uniqueopportunity to reduce health care usein a continually growing population.Consistent with the call for actionproposed by the World Health Organi-zation,15 multidisciplinary efforts topromote adherence should be a pri-ority for all medical providers andpolicy makers.
REFERENCES
1. Martin AB, Lassman D, Washington B,Catlin A; National Health ExpenditureAccounts Team. Growth in US healthspending remained slow in 2010; healthshare of gross domestic product wasunchanged from 2009. Health Aff (Millwood).2012;31(1):208–219
2. Schoenman J, Chockley N. UnderstandingU.S. Health Care Spending. Washington, DC:NIHCM Data Brief; 2011:1–13
3. Haber S, McCall N, Cromwell G. ChildrenWith High Health Care Utilization and Spe-cial Health Care Needs: Draft Manuscript.Washington, DC: RTI International; 2007
4. Emanuel EJ. Where are the health care costsavings? JAMA. 2012;307(1):39–40
5. Partnership for Solutions. Chronic Conditions:Making the Case for Ongoing Care. Baltimore,MD: The Johns Hopkins University; 2002
6. Van Cleave J, Gortmaker SL, Perrin JM.Dynamics of obesity and chronic health
738 McGRADY and HOMMEL

conditions among children and youth.JAMA. 2010;303(7):623–630
7. Wang G, Dietz WH. Economic burden ofobesity in youths aged 6 to 17 years: 1979-1999. Pediatrics. 2002;109(5). Available at:www.pediatrics.org/cgi/content/full/109/5/e81
8. Weiss KB, Sullivan SD, Lyttle CS. Trends inthe cost of illness for asthma in the UnitedStates, 1985-1994. J Allergy Clin Immunol.2000;106(3):493–499
9. Cystic Fibrosis Foundation. Cystic FibrosisFoundation Patient Registry 2010 AnnualData Report. Bethesda, MD: Cystic FibrosisFoundation; 2010
10. Smith JM, Martz K, Blydt-Hansen TD. Pedi-atric kidney transplant practice patternsand outcome benchmarks, 1987-2010: Areport of the North American PediatricRenal Trials and Collaborative Studies.Pediatr Transplant. 2013;17(2):149–157
11. Berry JG, Hall M, Hall DE, et al. Inpatientgrowth and resource use in 28 children’shospitals: a longitudinal, multi-institutionalstudy. JAMA Pediatr. 2013;167(2):170–177
12. Chevarley FM. Utilization and Expendituresfor Children With Special Health CareNeeds. Rockville, MD: Agency for HealthcareResearch and Quality; 2006
13. Newacheck PW, Kim SE. A national profile ofhealth care utilization and expenditures forchildren with special health care needs.Arch Pediatr Adolesc Med. 2005;159(1):10–17
14. Modi AC, Pai AL, Hommel KA, et al. Pediatricself-management: A framework for research,practice, and policy. Pediatrics. 2012;129(2).Available at: www.pediatrics.org/cgi/con-tent/full/129/2/e473
15. Sabate E. Adherence to Long-term Therapies:Evidence for Action. Geneva, Switzerland:World Health Organization; 2003
16. Bender BG, Rand C. Medication non-adherence and asthma treatment cost.Curr Opin Allergy Clin Immunol. 2004;4(3):191–195
17. Muenchberger H, Kendall E. Predictors ofpreventable hospitalization in chronic dis-ease: priorities for change. J Public HealthPolicy. 2010;31(2):150–163
18. Roebuck MC, Liberman JN, Gemmill-ToyamaM, Brennan TA. Medication adherence leads tolower health care use and costs despite in-creased drug spending. Health Aff (Millwood).2011;30(1):91–99
19. Berg JS, Dischler J, Wagner DJ, Raia JJ,Palmer-Shevlin N. Medication compliance:a healthcare problem. Ann Pharmacother.1993;27(9 suppl):S1–S24
20. DiMatteo MR. Variations in patients’ ad-herence to medical recommendations:
a quantitative review of 50 years of re-search. Med Care. 2004;42(3):200–209
21. Kahana S, Drotar D, Frazier T. Meta-analysisof psychological interventions to promoteadherence to treatment in pediatricchronic health conditions. J Pediatr Psy-chol. 2008;33(6):590–611
22. Newacheck PW, Taylor WR. Childhoodchronic illness: prevalence, severity, andimpact. Am J Public Health. 1992;82(3):364–371
23. Rapoff MA. Adherence to Pediatric MedicalRegimens. New York, NY: Springer; 2010
24. Logan D, Zelikovsky N, Labay L, Spergel J.The Illness Management Survey: identifyingadolescents’ perceptions of barriers toadherence. J Pediatr Psychol. 2003;28(6):383–392
25. Hommel KA, Davis CM, Baldassano RN. Ob-jective versus subjective assessment oforal medication adherence in pediatric in-flammatory bowel disease. Inflamm BowelDis. 2009;15(4):589–593
26. de Brantes F, Rosenthal MB, Painter M.Building a bridge from fragmentation toaccountability—the Prometheus Paymentmodel. N Engl J Med. 2009;361(11):1033–1036
27. Federal Interagency Forum on Child andFamily Statistics. America’s Children inBrief: Key National Indicators of Well-Being,2012. Washington, DC: U.S. GovernmentPrinting Office; 2012
28. Stille C, Turchi RM, Antonelli R, et al; Aca-demic Pediatric Association Task Force onFamily-Centered Medical Home. The family-centered medical home: specific consid-erations for child health research andpolicy. Acad Pediatr. 2010;10(4):211–217
29. Moher D, Liberati A, Tetzlaff J, Altman DG;PRISMA Group. Preferred reporting itemsfor systematic reviews and meta-analyses:the PRISMA statement. BMJ. 2009;339:b2535
30. Vandenbroucke JP, von Elm E, Altman DG,et al; STROBE Initiative. Strengthening thereporting of observational studies in epi-demiology (STROBE): explanation and elab-oration. PLoS Med. 2007;4(10):e297
31. Quittner AL, Modi AC, Lemanek KL, Ievers-Landis CE, Rapoff MA. Evidence-basedassessment of adherence to medicaltreatments in pediatric psychology. J PediatrPsychol. 2008;33(9):916–936, discussion 937–938
32. Wells G, Shea B, O’connell D, et al. TheNewcastle-Ottawa Scale (NOS) for assess-ing the quality of nonrandomised studies inmeta-analyses. Paper presented at 3rdSymposium on Systematic Reviews: Beyondthe Basics; 2000
33. Higgins JPT, Altman DG. Assessing Risk ofBias in Included Studies. Cochrane Hand-book for Systematic Reviews of Inter-ventions. West Sussex, England: John Wiley& Sons, Ltd; 2008:187–241
34. Adams RJ, Fuhlbrigge A, Finkelstein JA,et al. Impact of inhaled antiinflammatorytherapy on hospitalization and emergencydepartment visits for children with asthma.Pediatrics. 2001;107(4):706–711
35. Smith SR, Wakefield DB, Cloutier MM. Re-lationship between pediatric primary pro-vider visits and acute asthma ED visits.Pediatr Pulmonol. 2007;42(11):1041–1047
36. Herndon JB, Mattke S, Evans Cuellar A,Hong SY, Shenkman EA. Anti-inflammatorymedication adherence, healthcare utiliza-tion and expenditures among Medicaid andchildren’s health insurance program en-rollees with asthma. Pharmacoeconomics.2012;30(5):397–412
37. Walders N, Kopel SJ, Koinis-Mitchell D,McQuaid EL. Patterns of quick-relief andlong-term controller medication use inpediatric asthma. J Pediatr. 2005;146(2):177–182
38. Ashkenazi S, Amir J, Volovitz B, Varsano I.Why do asthmatic children need referral toan emergency room? Pediatr AllergyImmunol. 1993;4(2):93–96
39. Zhao J, He Q, Zhang G, et al. Status ofasthma control in children and the effect ofparents’ knowledge, attitude, and practice(KAP) in China: a multicenter study. AnnAllergy Asthma Immunol. 2012;109(3):190–194
40. Bartlett SJ, Krishnan JA, Riekert KA, ButzAM, Malveaux FJ, Rand CS. Maternal de-pressive symptoms and adherence totherapy in inner-city children with asthma.Pediatrics. 2004;113(2):229–237
41. Bauman LJ, Wright E, Leickly FE, et al. Re-lationship of adherence to pediatricasthma morbidity among inner-city chil-dren. Pediatrics. 2002;110(1 pt 1). Availableat: www.pediatrics.org/cgi/content/full/110/1/e6
42. Morris AD, Boyle DI, McMahon AD, GreeneSA, MacDonald TM, Newton RW. Adherenceto insulin treatment, glycaemic control, andketoacidosis in insulin-dependent diabetesmellitus. The DARTS/MEMO Collaboration.Diabetes Audit and Research in TaysideScotland. Medicines Monitoring Unit. Lan-cet. 1997;350(9090):1505–1510
43. McNally KA, Rohan J, Schluchter M, et al.Adherence to combined montelukast andfluticasone treatment in economically dis-advantaged African American youth withasthma. J Asthma. 2009;46(9):921–927
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 4, October 2013 739

44. Encinosa WE, Bernard D, Dor A. Does pre-scription drug adherence reduce hospital-izations and costs? The case of diabetes.Adv Health Econ Health Serv Res. 2010;22:151–173
45. Valenti WM. Treatment adherence improvesoutcomes and manages costs. AIDS Read.2001;11(2):77–80
46. Agency for Healthcare Research and Qual-ity. Total health services—mean and me-dian expenses per person with expenseand distribution of expenses by source ofpayment: United States, 2010. Medical Ex-penditure Panel Survey Household Component
Data. Available at: http://meps.ahrq.gov/mepsweb/. Accessed July 8, 2013
47. Graves MM, Roberts MC, Rapoff M, Boyer A.The efficacy of adherence interventions forchronically ill children: a meta-analytic re-view. J Pediatr Psychol. 2010;35(4):368–382
48. Chapman RH, Ferrufino CP, Kowal SL, ClassiP, Roberts CS. The cost and effectiveness ofadherence-improving interventions for an-tihypertensive and lipid-lowering drugs. IntJ Clin Pract. 2010;64(2):169–181
49. Chapman RH, Kowal SL, Cherry SB, Ferru-fino CP, Roberts CS, Chen L. The modeledlifetime cost-effectiveness of published
adherence-improving interventions for an-tihypertensive and lipid-lowering medi-cations. Value Health. 2010;13(6):685–694
50. Desborough JA, Sach T, Bhattacharya D,Holland RC, Wright DJ. A cost-consequencesanalysis of an adherence focused pharmacist-led medication review service. Int J PharmPract. 2012;20(1):41–49
51. Patrick AR, Schousboe JT, Losina E, SolomonDH. The economics of improving medica-tion adherence in osteoporosis: validationand application of a simulation model.J Clin Endocrinol Metab. 2011;96(9):2762–2770
WHAT’S IN A NUMBER: While I have not thought too much about my three sons’ability to father children, researchers are worried about the fertility of thecurrent generation of men between the ages of 18 and 25 years. As reported inThe Wall Street Journal (In the Lab: July 15, 2013), many in the reproductivescience world believe that we are entering a “sperm crisis” due to falling spermcounts. In general, men have approximately 60 million sperm in each milliliter ofsemen. As long as a man has approximately 40 million in each milliliter, he isconsidered fertile. As the number falls beneath this threshold (and particularlybelow 20 million), either the ability to conceive begins to drop or the time toconception increases. Several European studies have demonstrated that menhave much lower sperm counts now than previously. A study of nearly 26,000healthy French men followed at fertility clinics because of partner infertilitydemonstrated a 30% decline in sperm count from 1989 to 2005. Another largestudy showed that sperm counts had declined by almost 50% in the past 50 years.While on average French men still have healthy sperm counts (49 million permilliliter of semen), approximately 1 in 5 northern European men have spermcounts low enough to affect fertility. Why sperm counts have declined is notknown. Possible explanations include in utero such as maternal smoking, earlylife exposures to phthalates, and sedentary jobs, frequent hot baths, fatty foods,and marijuana use. Even central obesity has been implicated. Scientists areworried about the implications beyond fertility as sperm count may be an easyand sensitive measurement of other effects lifestyle may have on other bodyfunctions or processes. Others are not so convinced that a “crisis” is at hand.While the study of French men only included presumably healthy men, manystudies have been in men presenting to clinics because of infertility and thus maynot be representative of the general population. I am not sure how to counsel mysons on this topic. Other than to wait until they are sure they are absolutely readyto start a family, I generally simply recommend a healthy lifestyle and appro-priate protection should fertility be something they find themselves needing toconsider.
Noted by WVR, MD
740 McGRADY and HOMMEL