Embed Size (px)
Citation preview

Medicare-Medicaid Plan DemonstrationsMedicare-Medicaid Plan Demonstrations
Chicago Regional OfficeCenters for Medicare Health Plan Operations
Yolanda Burge-ClarkAugust 19, 2014

• 10 million (aprox) individuals that are
enrolled in both Medicare and
Medicaid (or “dual eligibles”).
• More likely to have mental illness,
have limitations in activities of daily
living, and multiple chronic
conditions.
Who are Medicare-Medicaid Enrollees?
Who are Medicare-Medicaid Enrollees?

Medicare-Medicaid Beneficiaries Account for Disproportionate Shares
of Spending
Medicare-Medicaid Beneficiaries Account for Disproportionate Shares
of Spending
3

Medicare-Medicaid Coordination OfficeMedicare-Medicaid Coordination Office
Section 2602 of the Affordable Care Act
Purpose: Improve quality, reduce costs and improve the
beneficiary experience.
– Ensure Medicare-Medicaid enrollees have full access to the services
to which they are entitled.
– Improve the coordination between the federal government and
states.
– Identify and test innovative care coordination and integration
models.
– Eliminate financial misalignments that lead to poor quality and cost
shifting.
4

Financial Alignment InitiativeFinancial Alignment Initiative
Background: In 2011, CMS announced new models to integrate the
service delivery and financing of both Medicare and Medicaidthrough a Federal-State demonstration to better serve the
population.
Goal: Increase access to quality, seamlessly integrated programs for Medicare-Medicaid enrollees.
Demonstration Models:
– Capitated Model: Three-way contract among State, CMS and health plan to provide comprehensive, coordinated care in a more cost-effective way.
– Managed FFS Model: Agreement between State and CMS under which states would be eligible to benefit from savings resulting from initiatives to reduce costs in both Medicaid and Medicare.
5

Demonstration DetailsDemonstration Details
• 13 total demonstrations
• 10 states have approved capitated demonstrations: Massachusetts, Ohio, Illinois, California, Virginia, New York, South Carolina, Michigan, Texas, and Washington.
• 2 states have Managed fee for Service demonstrations: Washington and Colorado.
• Minnesota approved for alternative model.
• RO V States include IL, OH, MI, and MN.6
1. Letter of Intent; 2. Meet CMS Standards and conditions; 3. State procurement documents released; 4. CMS and State select qualified plans;5. Sign Memorandum of Understanding; 6. CMS and State conduct readiness reviews; 7. Three-way contracts signed; and 8. Implementation, monitoring, and evaluation
Demonstration ProcessDemonstration Process

QualityQuality
• CMS and States jointly conduct a consolidated, comprehensive quality management reporting process
• Core set of CMS measures for all plans in all States– Focus on national, consensus-based measurement sets – Relevant to broader Medicare-Medicaid enrollee
populations
• State-specific measures– Targeted to State-specific demonstration population– Focus on long-term supports and services measures that
are underrepresented in national measures8

• States can request passive enrollment of eligible beneficiaries in their proposals
• Approval of passive enrollment is subject to robust beneficiary protections
• Passive enrollment systems designed to maximize continuity of existing relationships and account for benefits and formularies
• CMS/State may allow for facilitation of enrollment using independent third party
Enrollment ParametersEnrollment Parameters
9

• Individuals not eligible for passive enrollment:– PACE Organization enrollees– Enrollees in employer sponsored insurance or whose
employer/union is paid the Part D Retiree Drug Subsidy
– Enrollees who have opted out of a demonstration plan
– Others as memorialized in the CMS-State Memorandum of Understanding
– For 2014, individuals who were reassigned to a below-benchmark PDP effective January 1, 2014
Enrollment Parameters (cont.)Enrollment Parameters (cont.)
10

• CMS expects States to phase in enrollment over a period of time at program start-up– Examples: By geography or population groups
• CMS/State may limit enrollment for a variety of reasons (e.g., quality, capacity)
• No phase-in to new counties or populations in Years 2 and 3 of the demonstration
Phasing In EnrollmentPhasing In Enrollment
11

• Notification in advance of the enrollment• Ability to opt out at any time• Understandable beneficiary notification• Resources to support beneficiaries– Choice counselors and enrollment brokers– State Health Insurance Programs– Aging and Disability Resource Centers
Enrollment-Related Beneficiary Protections
Enrollment-Related Beneficiary Protections
12

• Milestones based on criteria from the readiness reviews
• Allows CMS and State to monitor demonstration plan as enrollments begin
• System Capacity• Health Risk Assessments• Staffing• Transitions
• May delay future enrollment
Implementation MonitoringImplementation Monitoring
13

• Ongoing Monitoring• Elements based on Readiness Review– Care Coordination– Health Risk Assessments– Provider and Facility Network Capacity
• Part C and Part D data driven monitoring– Call Centers– Part D Appeals and Grievances–Web Sites
• Part C and Part D Reporting Requirements
Ongoing MonitoringOngoing Monitoring
• CMS-State contract management team, emphasis is on efficient coordination between the two entities
• Part D oversight will continue to be a CMS responsibility
• Demo plans will be subject to all existing Part C & D oversight.
Oversight FrameworkOversight Framework

• CMS contracted with independent evaluator (RTI)
• State-specific evaluation plans • Mixed method approach (qualitative and
quantitative)– Site visits– Analysis of focus group data– Analysis of program data– Calculate savings attributable to the demonstration
EvaluationEvaluation
16
• Key issues, include but are not limited to:– Beneficiary health status and outcomes– Quality of care provided across settings and care
delivery models– Beneficiary access to and utilization of care across
settings– Beneficiary satisfaction and experience– Administrative and systems changes and
efficiencies– Overall costs or savings for Medicare and Medicaid
EvaluationEvaluation
17

• MOU signed: February 22, 2013• Contract signed: November 5, 2013• Eligible population:– Age 21 and older– Receiving full Medicaid benefits, and– Enrolled in the Medicaid Aid to the Aged, Blind,
and Disabled (AABD) category of assistance,
IllinoisIllinois

• In the following Medicaid 1915(c) waivers:– Persons who are Elderly; – Persons with Disabilities; – Persons with HIV/AIDS; – Persons with Brain Injury and – Persons residing in Supportive Living Facilities.
• Individuals with End Stage Renal Disease (ESRD) at the time of enrollment.
Illinois (continued)Illinois (continued)

• Excluded from enrollment:– Under the age of 21; – Receiving developmental disability institutional services
or who participate in the HCBS waiver for Adults with Developmental Disabilities;
– Medicaid Spend-down population; – Enrolled in the Illinois Medicaid Breast and Cervical
Cancer program; – Enrolled in partial benefit programs; and – Those having comprehensive Third Party Insurance
Illinois (continued)Illinois (continued)

IllinoisIllinois
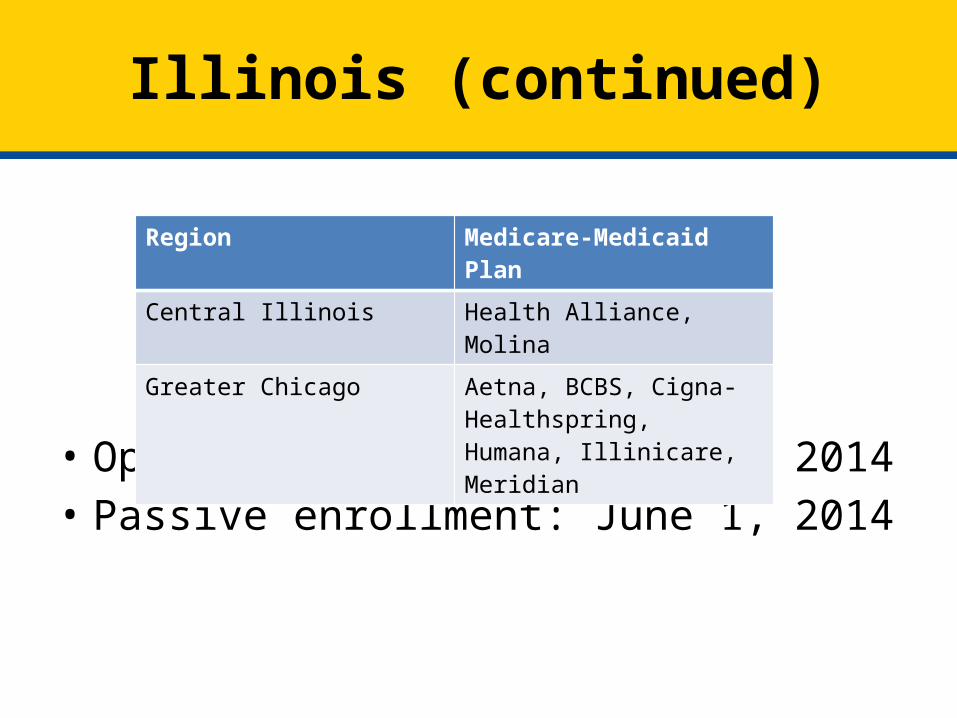
• Opt-in enrollment: March 1, 2014• Passive enrollment: June 1, 2014
Illinois (continued)Illinois (continued)
Region Medicare-Medicaid Plan
Central Illinois Health Alliance, Molina
Greater Chicago Aetna, BCBS, Cigna-Healthspring, Humana, Illinicare, Meridian

• Passive enrollment phased in over 6 month period.– No more that 5,000 per month in Chicago region– No more than 3,000 per month in Central IL region
• Eligible members will receive notification of passive enrollment by the State at 60 days and 30 days prior to being enrolled.
• Members can opt out at any time.
Illinois (continued)Illinois (continued)

• March Enrollment: 160• July Enrollment: 37,000• Goal of 135,000 enrollees• Transition period for medical, behavioral, and
LTSS is 180 days• Medicare Part D transition period unchanged.
Illinois ( continued)Illinois ( continued)

• Funding to support Options Counseling:– $394,932 (August, 2013)
• Funding to support Ombudsman Program:– $267. 556 (December 2013)
• Enrollment Broker Contact Information: – 1-877-912-8880 (TTY: 1-866-565-8576), – Monday to Friday from 8 a.m. to 7 p.m. and
Saturday from 9 a.m. to 3 p.m.
Illinois (continued)Illinois (continued)

• MOU signed: December 11, 2012• Contract signed: February 11, 2014• Eligible population includes – Full-benefit Medicare-Medicaid Enrollees only. – Individuals with serious and persistent mental illness– Intellectual Disabilities (ID) and other
Developmental Disabilities (DD) who are not served through an IDD 1915(c) HCBS waiver or an ICF-IDD may opt into the ICDS program.
OhioOhio
• Excluded Individuals:– Only eligible for Medicare Savings Program
benefits (QMB-only, SLMB-only, and QI-1) – ID and other DD who are served through an IDD
1915(c)HCBS waiver or an ICF-IDD– enrolled in PACE– have other third party insurance– under age of 8– on a delayed Medicaid spend down
Ohio (continued)Ohio (continued)

OhioOhio

Region Medicare-Medicaid Plans Enrollment Start
Northeast Buckeye, Caresource, United
May 1st
Northwest Aetna, Buckeye June 1st
Northeast Central Caresource, United June 1st
Southwest Aetna, Molina June 1st
East-Central Caresource, United July 1st
West Central Buckeye, Molina July 1st
Central Aetna, Molina July 1st
Ohio (continued)Ohio (continued)

• Medicare Opt-in enrollment and Medicaid passive enrollment: May 1, 2014
• Medicare passive enrollment: January 1, 2015• May Enrollment: 5,000• July Enrollment: 14,000• Provider transition period of 90 days for
enrollees identified for high risk care and 365 days for all others
• Transition period for all drugs follows Part D rules
Ohio (continued)Ohio (continued)

• Funding to support Ombudsman Program: $272, 354 (March, 2014)
• Enrollment Broker Contact Information: – 1-800-324-8680– Monday through Friday from 7:00 am to 8:00 pm
and Saturday from 8:00 am to 5:00 pm – TTY users should call Ohio Relay Service at 7-1-1
Ohio (continued)Ohio (continued)

• MOU signed April 3, 2014• Estimate 100,000 eligible beneficiaries• 8 Medicare-Medicaid Plans• 4 PIHPs are responsible for all behavioral
health services • Eligible population– Over 21– Full Medicaid benefits
MichiganMichigan

• Individuals excluded from demonstration– Under 21– Previously disenrolled due to special disenrollment from
Medicaid managed care defined in 42 CFR 438.56 – Additional Low Income Medicare Beneficiary/Qualified
Individuals (ALMB/QI)– Medicaid spend downs or deductibles– Medicaid who reside in a State psychiatric hospital– Commercial HMO coverage– Elected Hospice Services
Michigan (continued)Michigan (continued)
Michigan (continued)Michigan (continued)

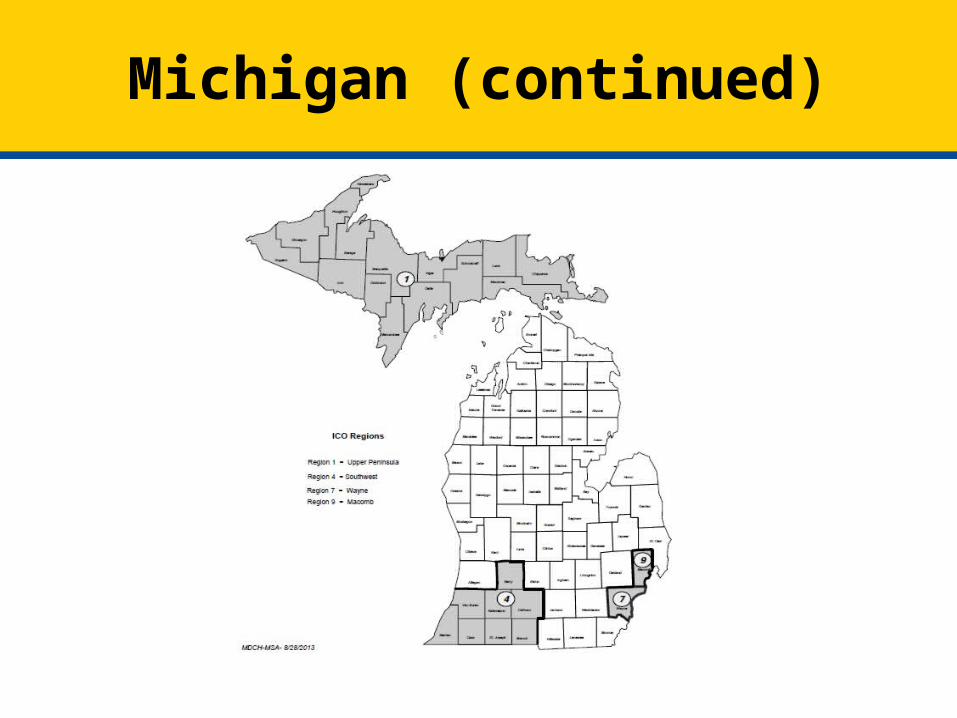
• Four regions– Region 1- Upper Peninsula– Region 4- Southwest Michigan- Barry, Berrien,
Branch, Calhoun, Cass, Kalamazoo, St. Joseph, and Van Buren counties
– Region 7- Wayne County– Region 9- Macomb County
Michigan (continued)Michigan (continued)
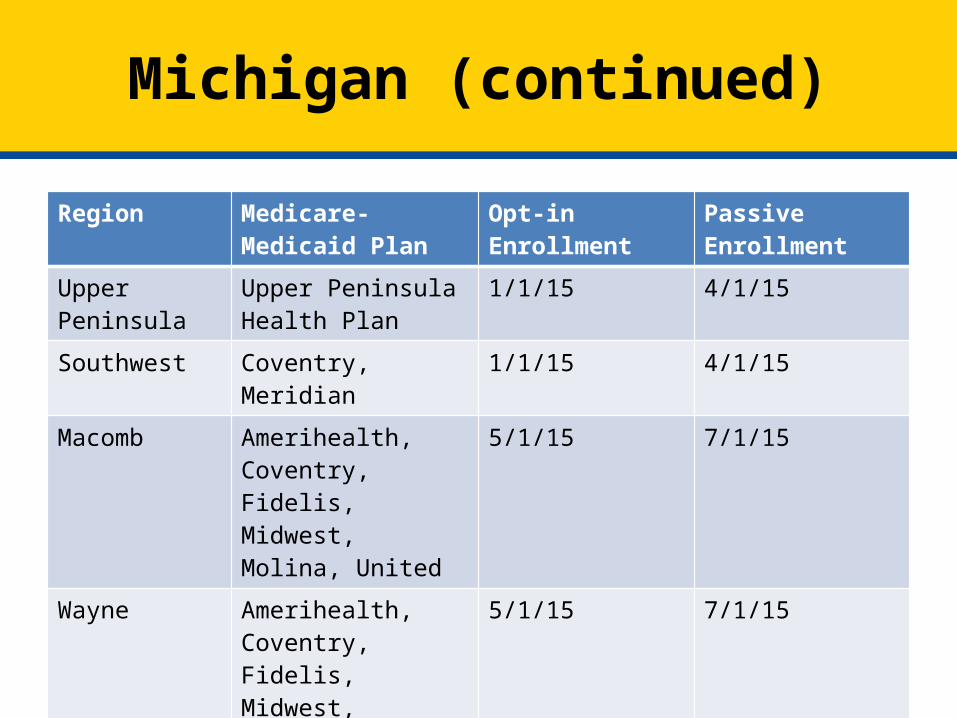
Region Medicare-Medicaid Plan
Opt-in Enrollment Passive Enrollment
Upper Peninsula Upper Peninsula Health Plan
1/1/15 4/1/15
Southwest Coventry, Meridian 1/1/15 4/1/15
Macomb Amerihealth, Coventry, Fidelis, Midwest, Molina, United
5/1/15 7/1/15
Wayne Amerihealth, Coventry, Fidelis, Midwest, Molina, United
5/1/15 7/1/15
Michigan (continued)Michigan (continued)

• MOU signed September 12, 2013• Implemented in 2013• Alternative design to Financial Alignment
Initiative• Using current MSHO DSNP plans• Demonstration focused on:– Administrative efficiencies, – marketing, – quality
MinnesotaMinnesota

• Medicare-Medicaid Coordination Office http://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-MedicaidCoordination.html – Financial Alignment Initiative
• Integrated Care Resource Center http://www.integratedcareresourcecenter.com/
Additional ResourcesAdditional Resources





























