Embed Size (px)
Citation preview
Medical Update for Audiologists
H. Alexander Arts, MD
Professor of Otolaryngology
Adult & Pediatric Otology & Neurotology
Medical Director, Cochlear Implant Program
Email: [email protected]
Conflict of Interest Disclosure
• I have no current conflicts of interest, financial or otherwise.
• I have in the past served as a paid consultant for Med-El Medical Electronics
• I am the Principal Investigator on two clinical trials sponsored by Cochlear Corp. and receive some salary support for my effort on these studies.
Overview
• Medical diagnoses relevant to audiologists– Disorders causing conductive hearing loss
• Chronic otitis media & Cholesteatoma• Otosclerosis
– Disorders causing sensorineural hearing loss• Acoustic neuroma• Neurofibromatosis Type 2• Meniere’s disease• Sudden hearing loss• Congenital hearing loss• Inner ear malformations• Superior semicircular canal dehiscence syndrome
Overview
• Medical & Surgical Treatment of Hearing Loss– Cochlear implants– Implantable bone conduction devices– Stapedectomy– Surgery for superior semicircular canal dehiscence– Management of single sided deafness
Otitis Media
Time course– Acute vs. chronic
Pathology– Serous or secretory
Chronic otitis media with effusion (COME)
– Suppurative– Mucoid– Adhesive
Acute Suppurative Otitis Media
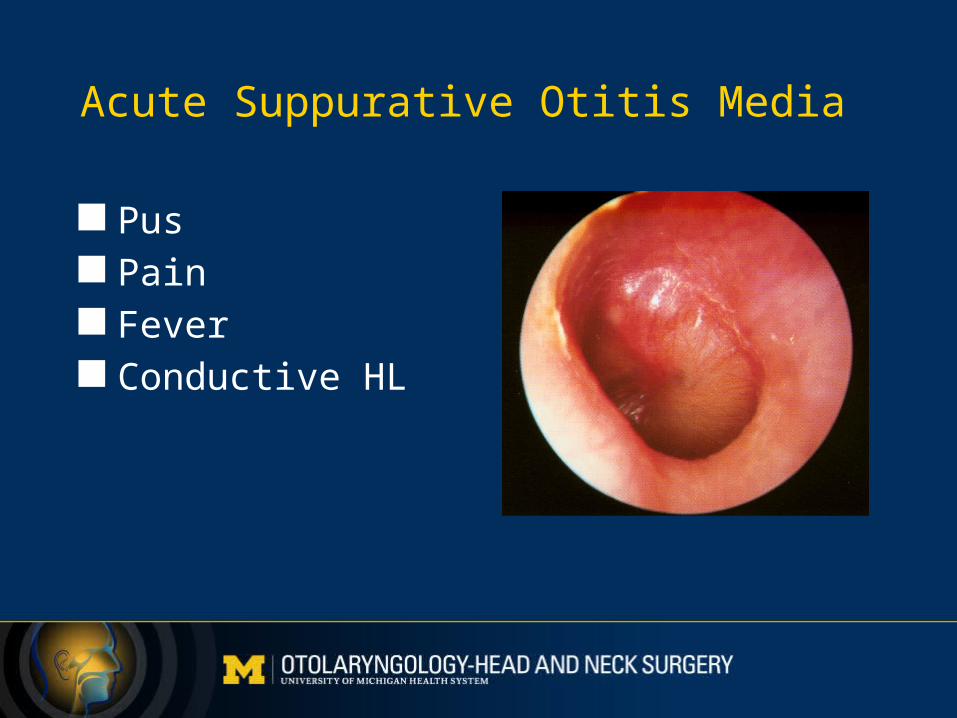
Pus Pain Fever Conductive HL
Chronic Otitis Media
Confusing nomenclature encompassing a wide range of disease processes:– Chronic middle ear effusion– Any persistent tympanic membrane perforation– Cholesteatoma– Atelectatic disease
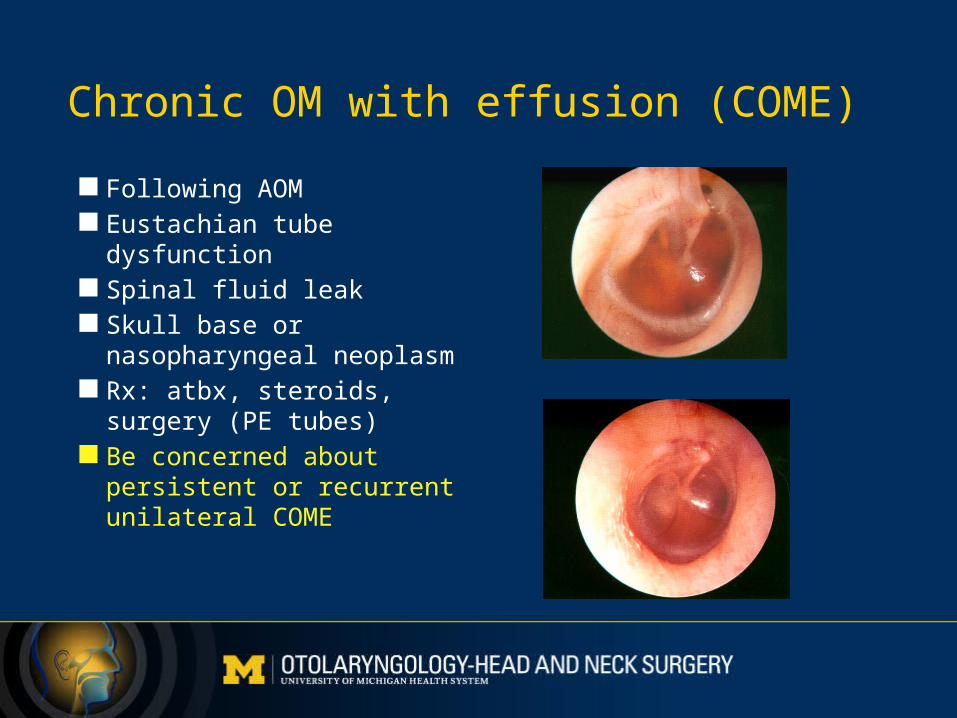
Chronic OM with effusion (COME)
Following AOM Eustachian tube
dysfunction Spinal fluid leak Skull base or
nasopharyngeal neoplasm Rx: atbx, steroids, surgery
(PE tubes) Be concerned about
persistent or recurrent unilateral COME
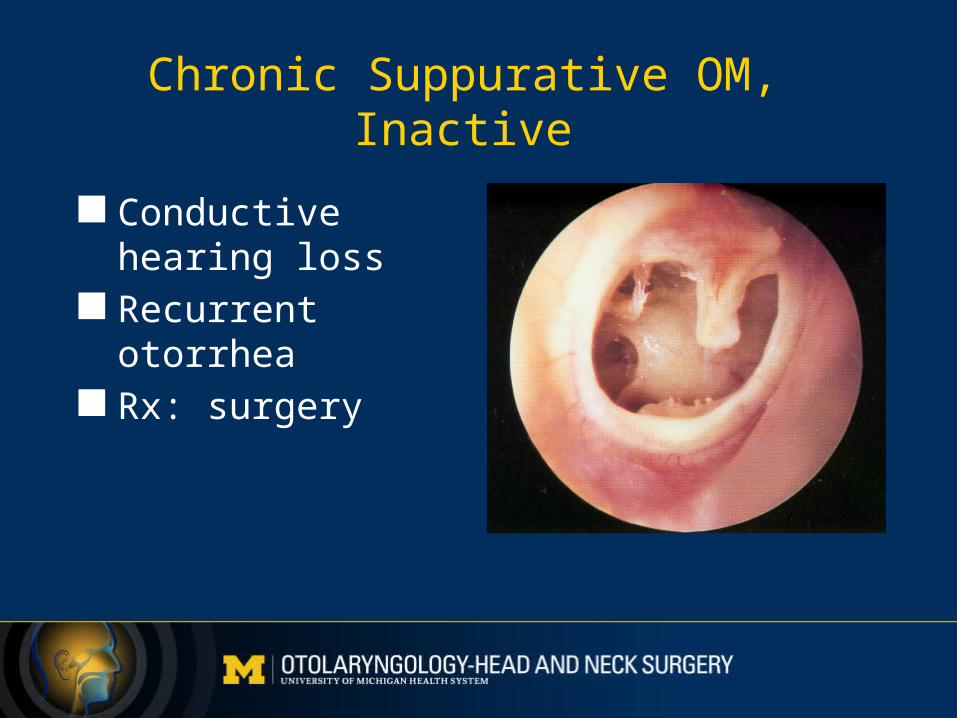
Chronic Suppurative OM, Inactive
Conductive hearing loss
Recurrent otorrhea Rx: surgery
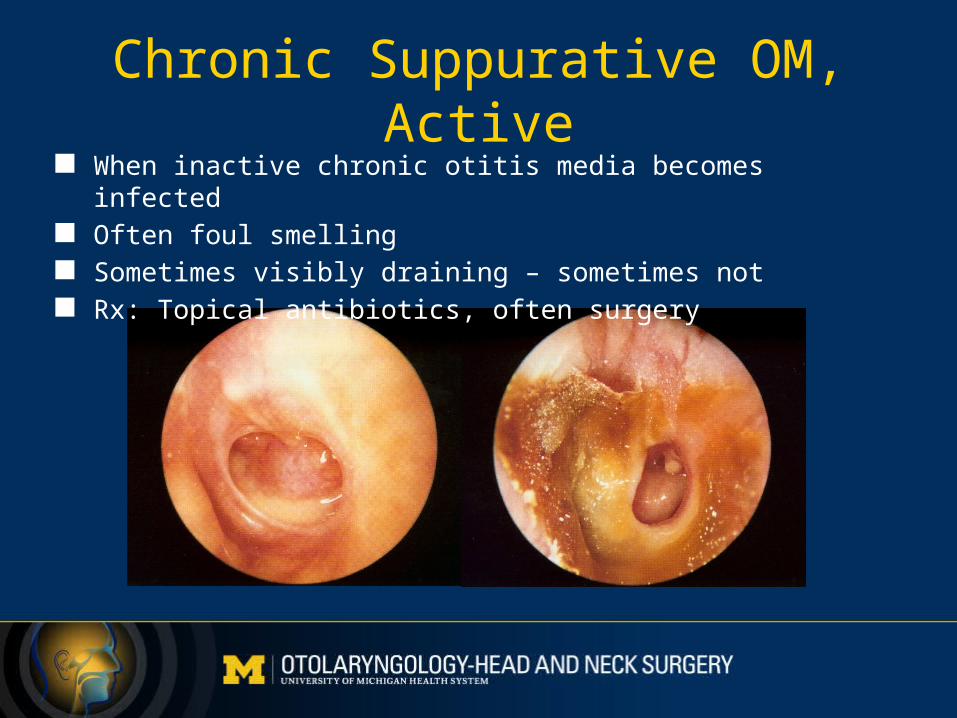
Chronic Suppurative OM, Active When inactive chronic otitis media becomes infected Often foul smelling Sometimes visibly draining – sometimes not Rx: Topical antibiotics, often surgery
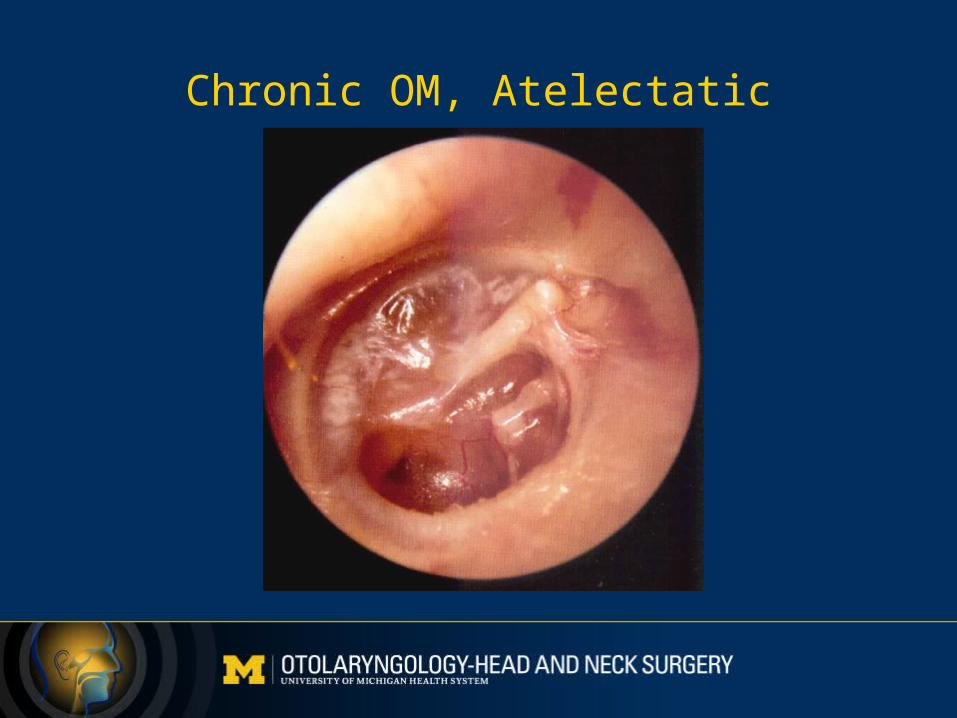
Chronic OM, Atelectatic
Cholesteatoma
Doesn’t have anything to do with cholesterol Is not a tumor Cyst lined with skin Most are acquired, but some are congenital They grow and can be destructive Can cause serious, even life threatening complications
“Safe” vs. “Unsafe” ears. Ears with cholesteatoma are unsafe.
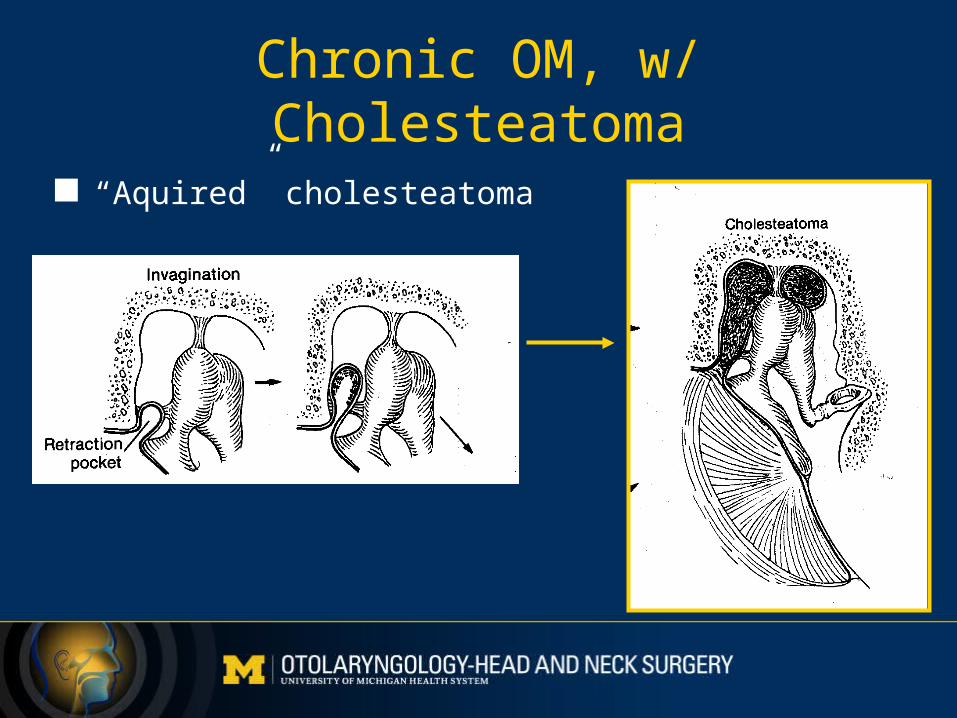
Chronic OM, w/ Cholesteatoma
“Aquired” cholesteatoma
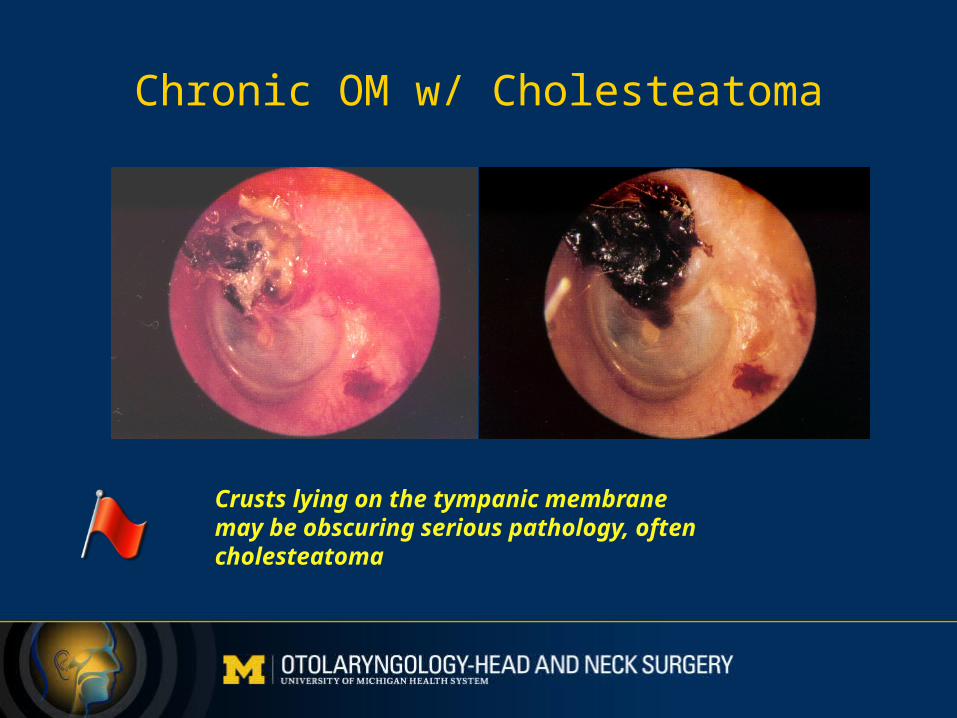
Chronic OM w/ Cholesteatoma
Crusts lying on the tympanic membranemay be obscuring serious pathology, oftencholesteatoma
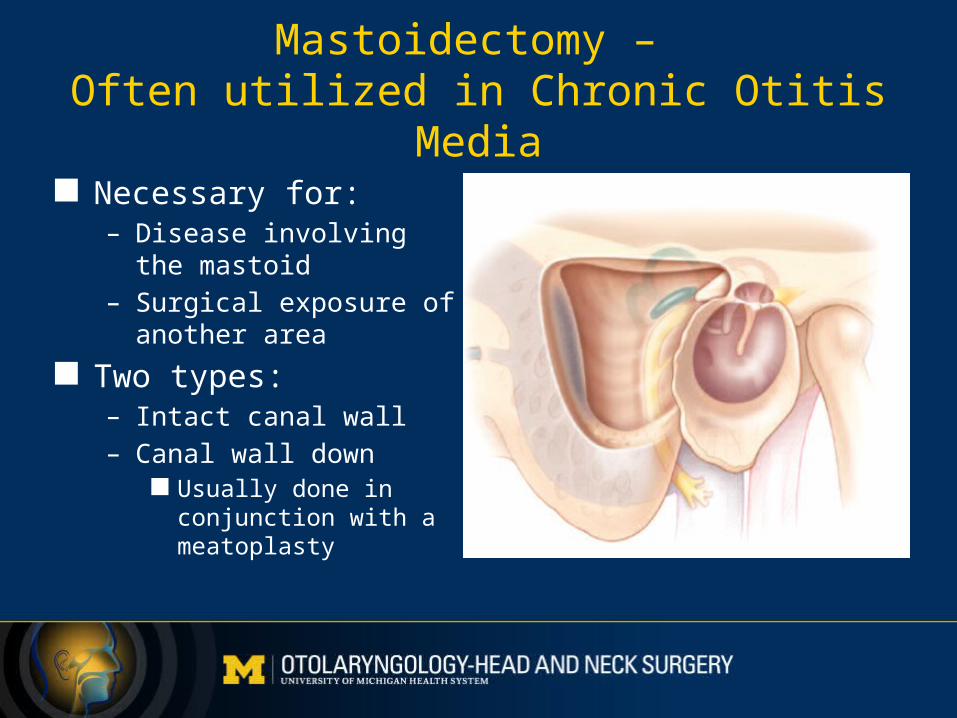
Mastoidectomy – Often utilized in Chronic Otitis Media
Necessary for:– Disease involving the
mastoid– Surgical exposure of
another area
Two types:– Intact canal wall– Canal wall down
Usually done in conjunction with a meatoplasty
Meatoplasty
• Performed with canal wall down mastoidectomy
• Allows aeration and cleaning of the open mastoid cavity
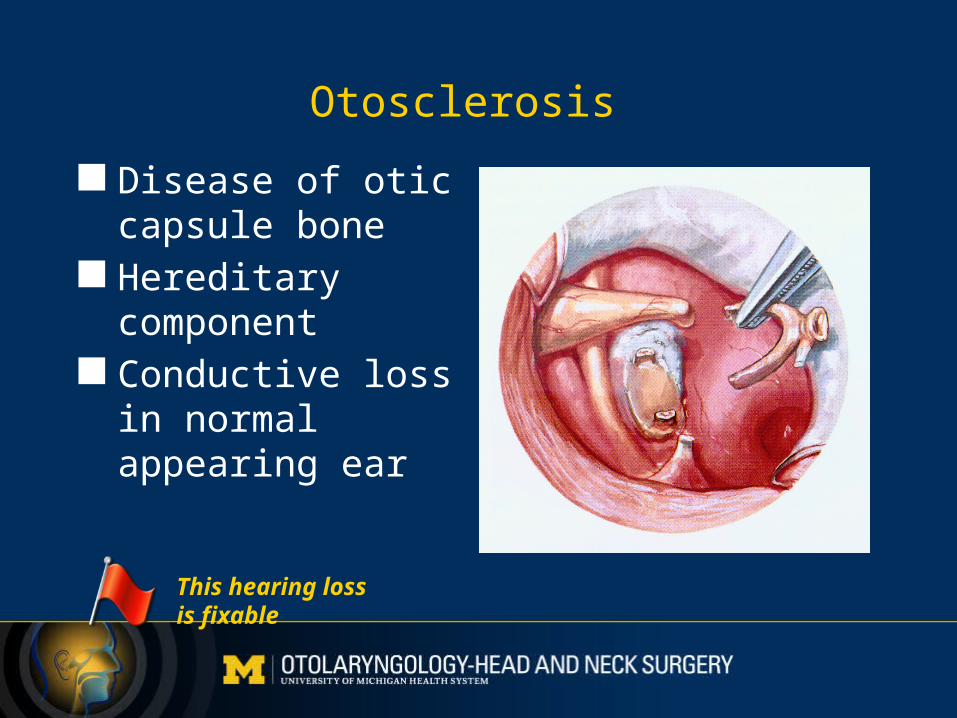
Otosclerosis
Disease of otic capsule bone
Hereditary component
Conductive loss in normal appearing ear
This hearing lossis fixable
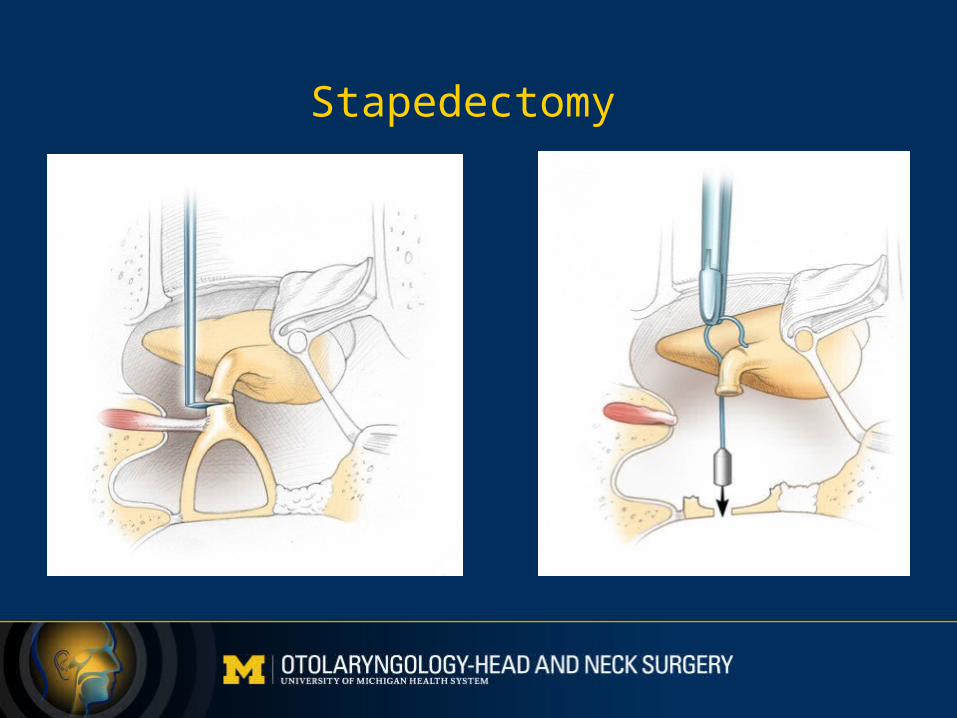
Stapedectomy
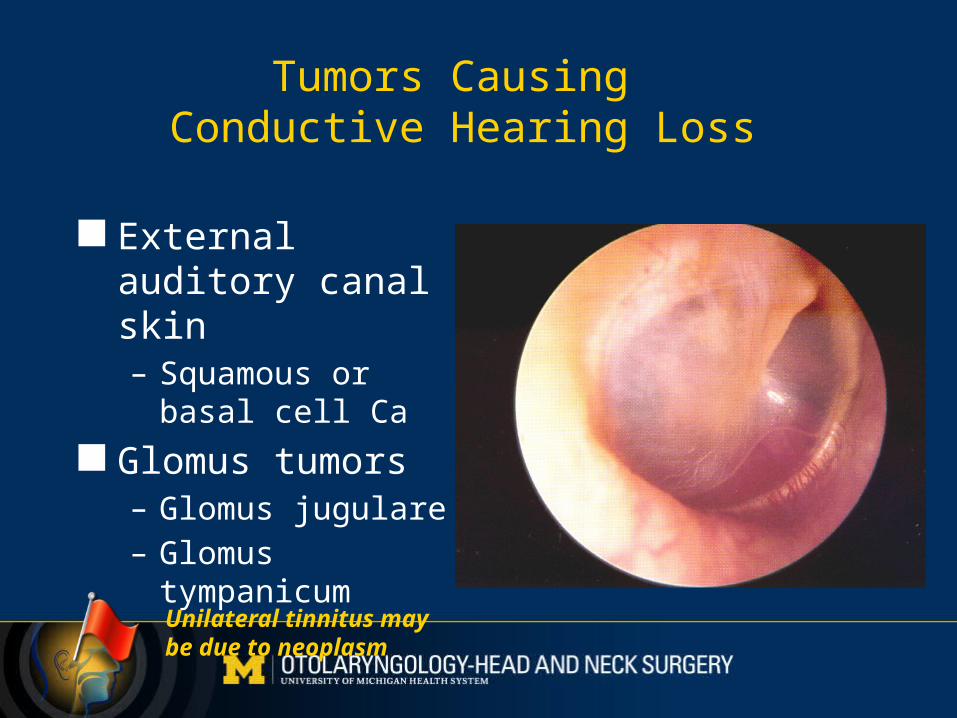
Tumors Causing Conductive Hearing Loss
External auditory canal skin– Squamous or basal
cell Ca
Glomus tumors– Glomus jugulare– Glomus tympanicum
Unilateral tinnitus may be due to neoplasm
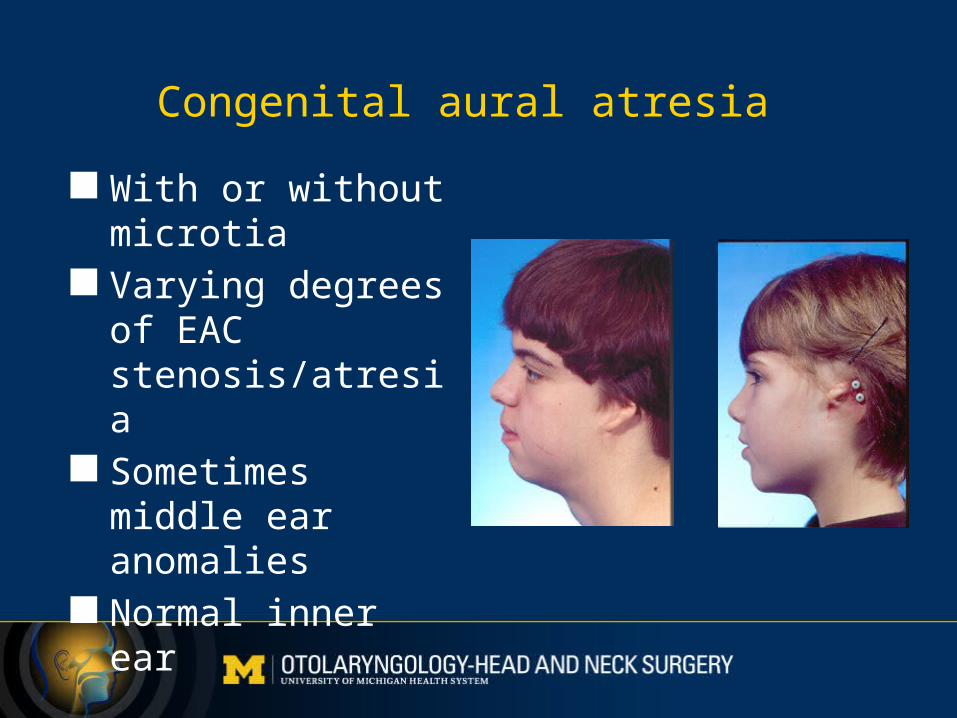
Congenital aural atresia
With or without microtia
Varying degrees of EAC stenosis/atresia
Sometimes middle ear anomalies
Normal inner ear
Etiologies of Sensorineural Hearing Loss
Noise Presbycusis Ototoxicity Meniere’s disease Infection Autoimmune
Congenital Hereditary Developmental Tumors Central nervous system pathology
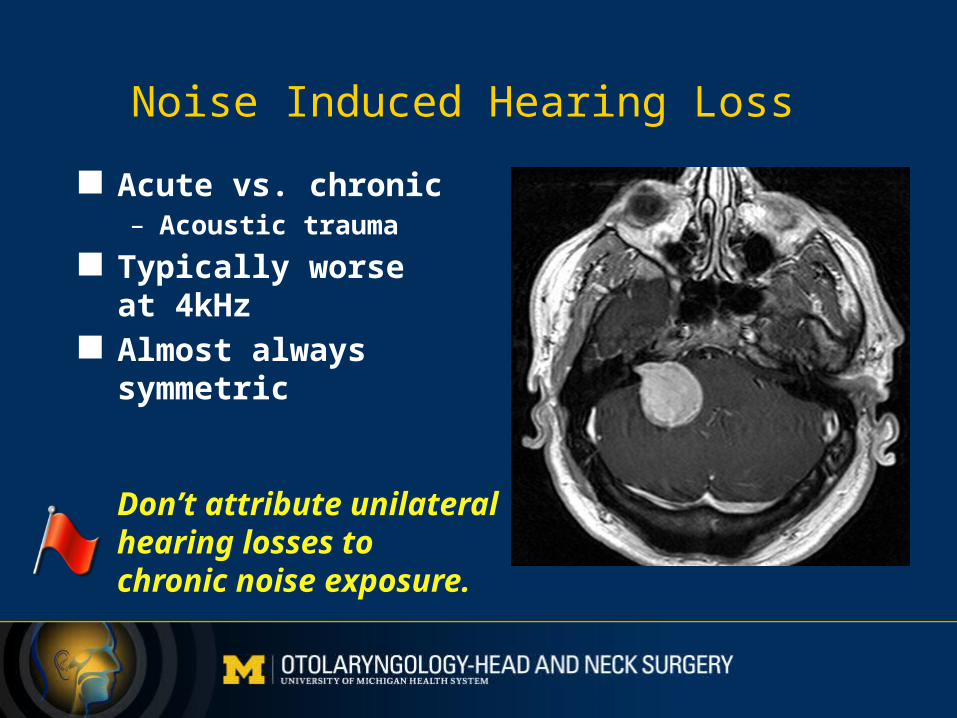
Noise Induced Hearing Loss
Acute vs. chronic– Acoustic trauma
Typically worse at 4kHz
Almost always symmetric
Don’t attribute unilateralhearing losses to chronic noise exposure.
Meniere’s disease
Classic symptoms:– Fluctuating/progressive hearing loss– Tinnitus– Episodic vertigo
Pathology: endolymphatic hydrops ? Endolymphatic hypertension Rx:
– Na+ restriction, diuretics– Vestibular ablation
• Surgical• Intratympanic gentamicin
Sudden SensorineuralHearing Loss (SSNHL)
A syndrome with a host of causes A viral neuritis or cochleitis in most cases
1% will have acoustic neuroma Steroids beneficial
Systemic vs. intratympanic
Antivirals may be beneficial Occasionally a sudden hearing loss can be conductive
1. We treat sudden sensorineural hearing loss as an emergency.2. Do not assume that a sudden loss is due to otitis media with effusion.3. All SSNHL patients should have an MRI.
This is important.
Congenital sensorineural hearing loss
Acquired – intrauterine insult:– Maternal rubella, CMV, syphilis, herpes, toxoplasmosis– Hyperbilirubinemia– Birth injury– Teratogenic drugs
Thalidomide, quinine, Dilantin, isoretinoin, others
Congenital sensorineural hearing loss
Hereditary about 1:4000 live births 90% autosomal recessive
– Non-syndromic– Syndromic
Dominant: Waardenburg’s, Alport’s, Pierre Robin, Crouzon’s, Treacher-Collins, BOR
Recessive: Mucopolysaccharidoses, Jervell-Lange-Nielsen, Pendred’s, Usher’s
Other: Nager, CHARGE, Goldenhar’s
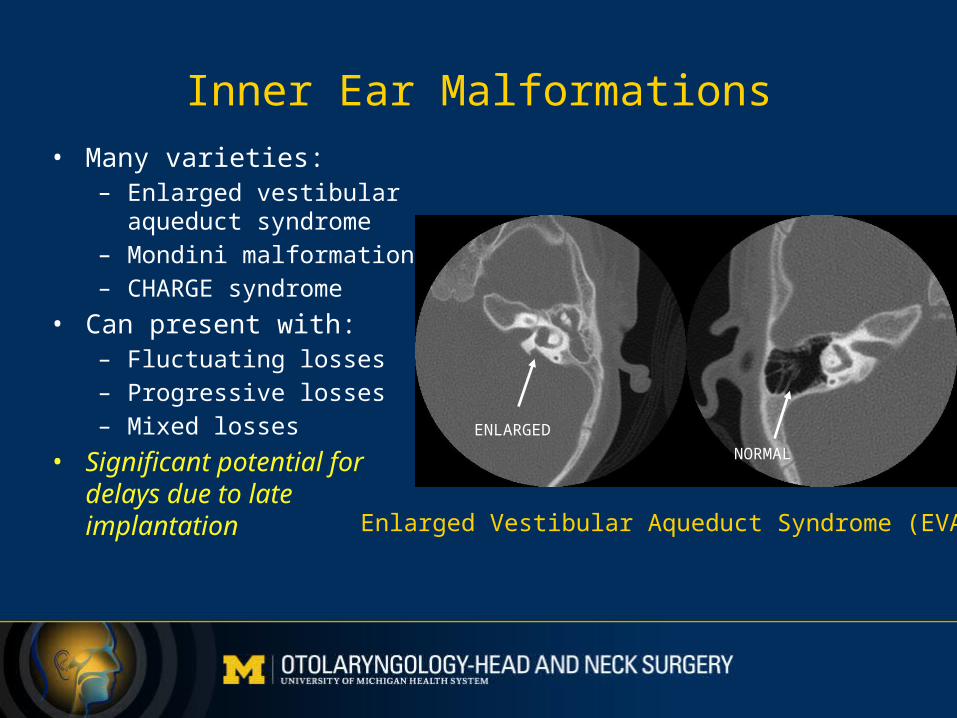
Inner Ear Malformations
• Many varieties:– Enlarged vestibular aqueduct
syndrome– Mondini malformation– CHARGE syndrome
• Can present with:– Fluctuating losses– Progressive losses– Mixed losses
• Significant potential for delays due to late implantation
ENLARGED
NORMAL
Enlarged Vestibular Aqueduct Syndrome (EVAS)
Risk Factors for Newborn Hearing Loss
Family hx of hearing loss Maternal infection during pregnancy Low birth weight Hyperbilirubinemia Ototoxic medications Mechanical ventilation > 5 days APGAR scores of <5 at 1min or <7 at 5min
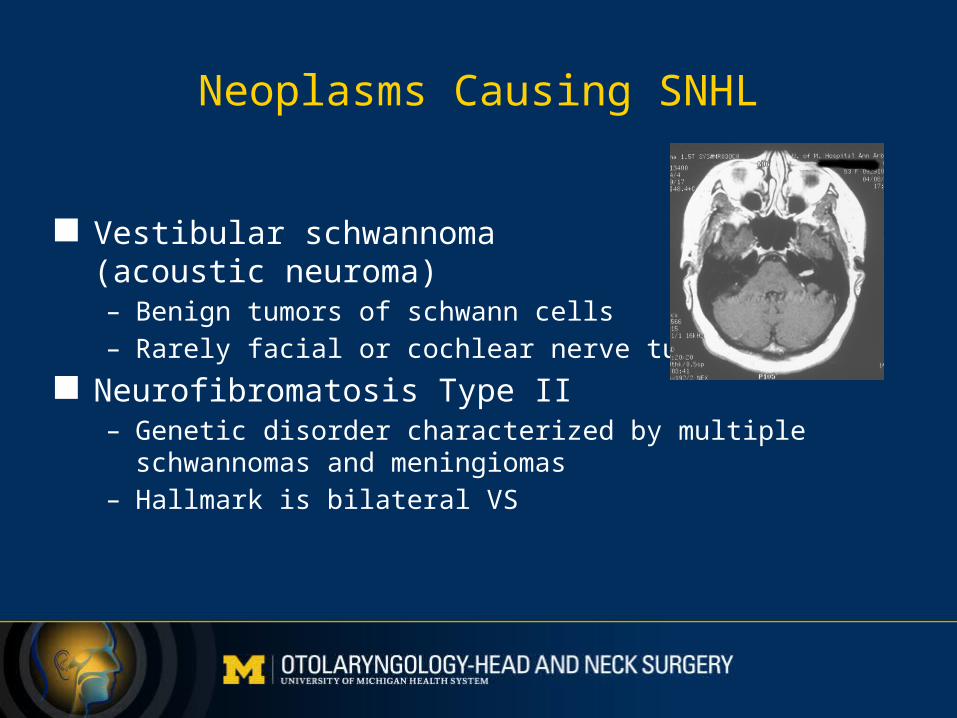
Neoplasms Causing SNHL
Vestibular schwannoma (acoustic neuroma)– Benign tumors of schwann cells– Rarely facial or cochlear nerve tumors
Neurofibromatosis Type II– Genetic disorder characterized by multiple schwannomas and
meningiomas– Hallmark is bilateral VS
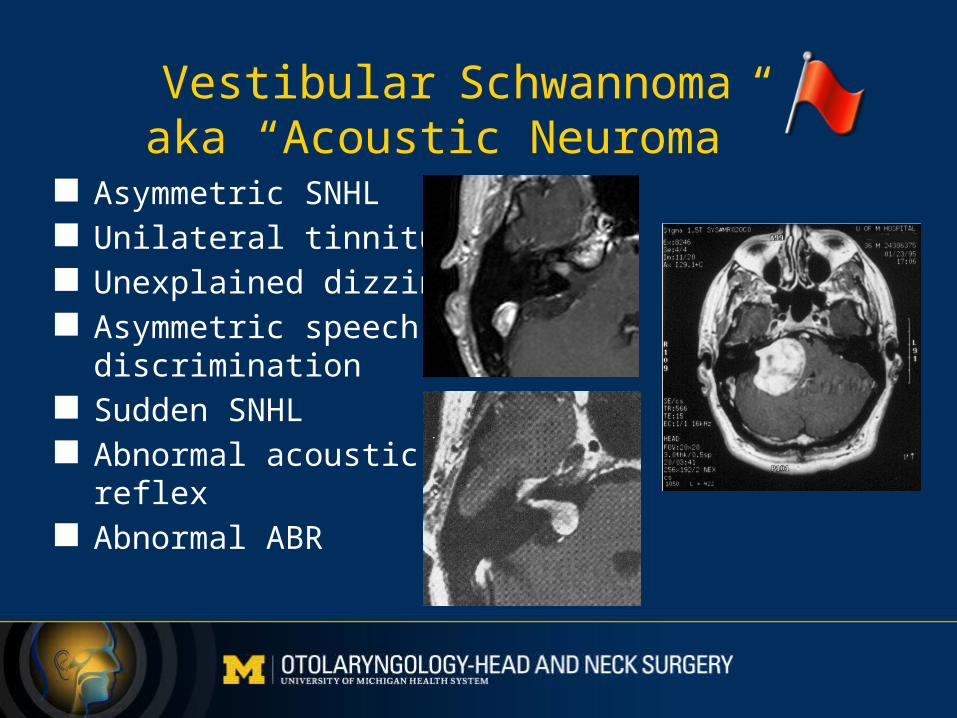
Vestibular Schwannomaaka “Acoustic Neuroma”
Asymmetric SNHL Unilateral tinnitus Unexplained dizziness Asymmetric speech
discrimination Sudden SNHL Abnormal acoustic
reflex Abnormal ABR
Neurofibromatosis Type 2
• Often not detected until adulthood
• Have a high index of suspicion with bilateral asymmetric losses, even in children
Other Neoplasms Causing HL
Meningioma Glomus tumors (paraganglioma) Epidermoids Endolymphatic sac tumors (Von Hippel Lindau disease)
ABR vs. MRI for Diagnosis of Retrocochlear Lesions
• ABR is a sensitive screening tool for vestibular schwannoma > 1cm
• For lesions < 1cm, ABR can have up to a 15% false negative rate
• MRI is essentially 100% sensitive
• I use ABR for screening when missing a < 1cm lesion would not alter our management– Elderly– Multiple other medical morbidities
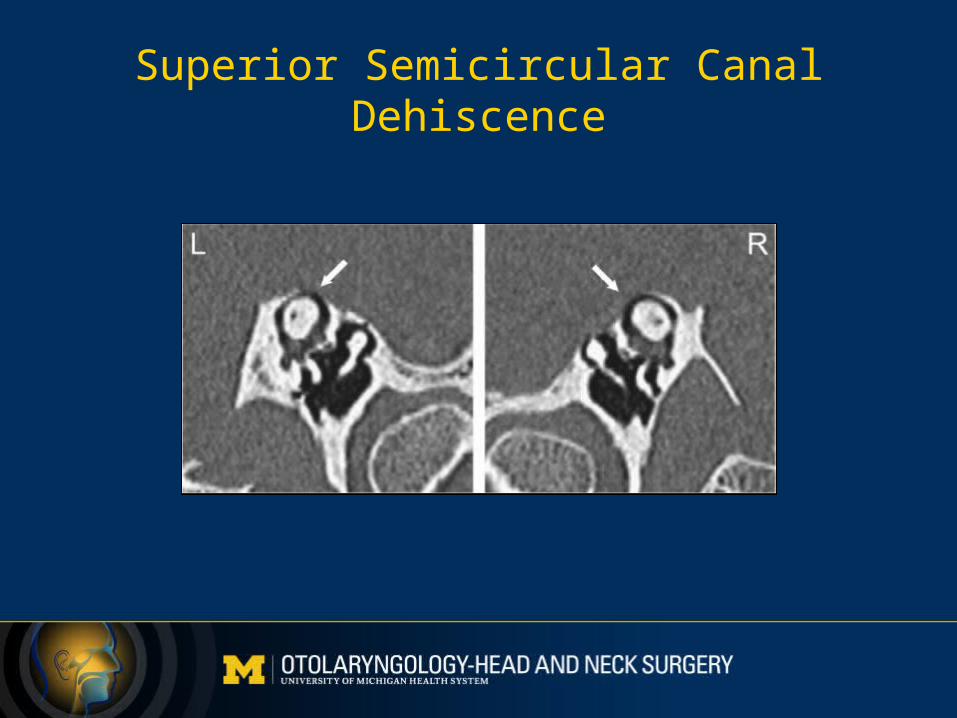
Superior Semicircular Canal Dehiscence
Superior Semicircular Canal Dehiscence
• Symptoms:– Aural fullness– Hearing loss– Pulsatile tinnitus– Autophony– Sound or pressure induced vertigo– Hyperacousis
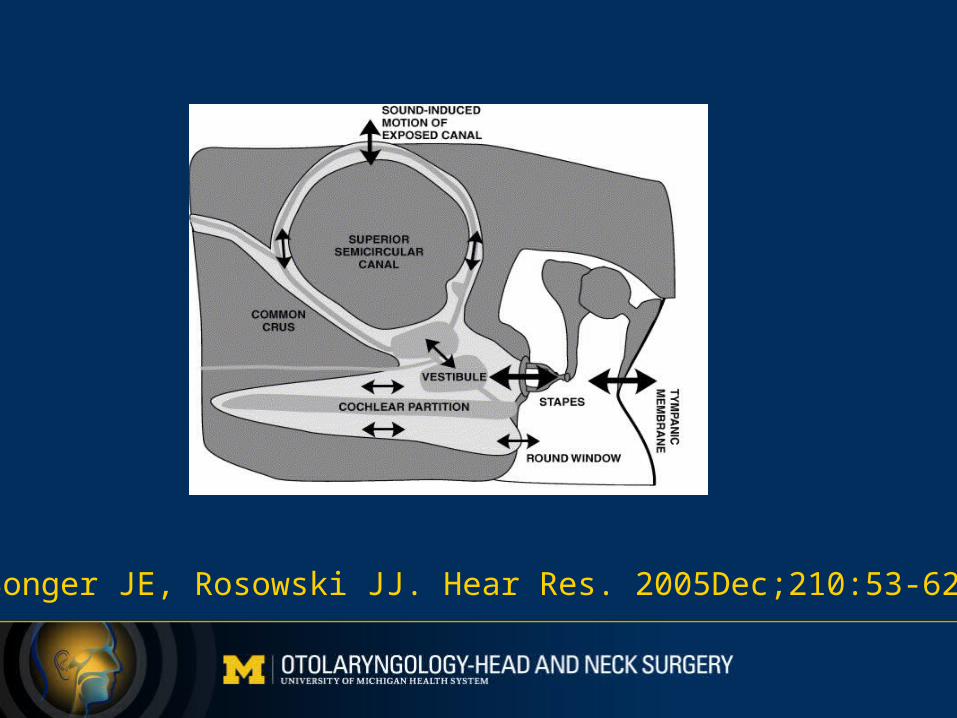
Songer JE, Rosowski JJ. Hear Res. 2005Dec;210:53-62.
Superior Semicircular Canal Dehiscence
• Findings– Conductive or mixed hearing loss (mostly low frequency)– Supra-normal bone conduction thresholds– Tullio phenomeon
• Sound induced nystagums
– Electrocochleography• Elevated SP/AP ratio
– VEMP• Reduced thresholds
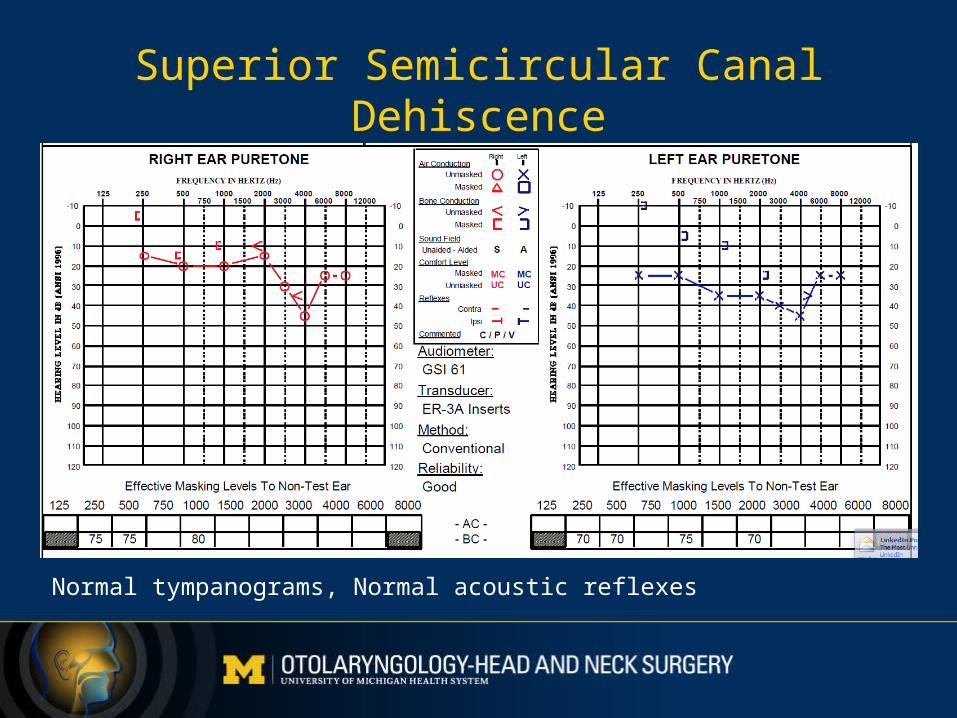
Normal tympanograms, Normal acoustic reflexes
Superior Semicircular Canal Dehiscence
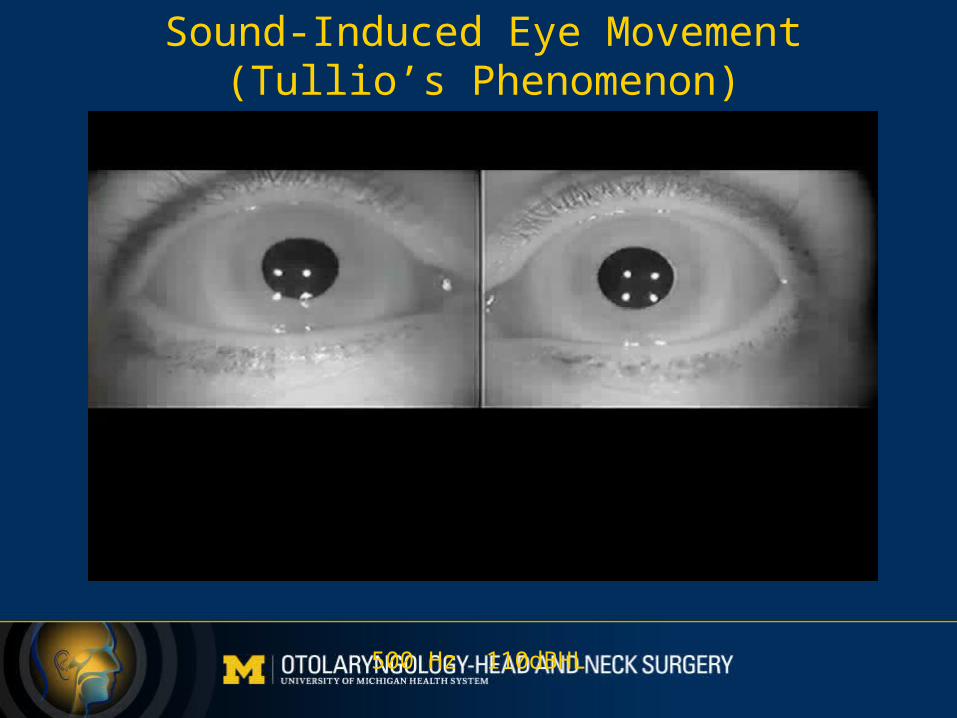
Sound-Induced Eye Movement(Tullio’s Phenomenon)
500 Hz 110dBHL
Superior Semicircular Canal Dehiscence
• Etiology is unknown• Found in 0.7% of temporal bones• Sometimes induced by strain or trauma• Surgical plugging provides excellent control of vertigo
– Often improves hearing
What’s New in Cochlear Implants
• Expanded indications• Electro-acoustic stimulation (Hybrid devices)• MRI compatibility• Use in single sided deafness
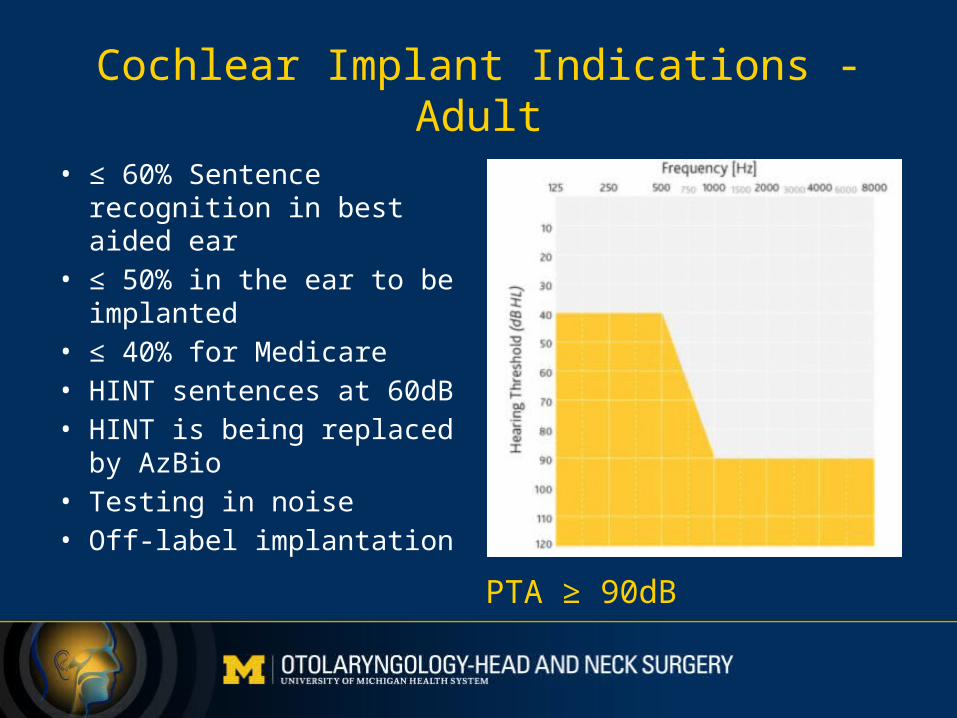
Cochlear Implant Indications - Adult
• ≤ 60% Sentence recognition in best aided ear
• ≤ 50% in the ear to be implanted
• ≤ 40% for Medicare• HINT sentences at 60dB• HINT is being replaced by
AzBio• Testing in noise• Off-label implantation PTA ≥ 90dB
Cochlear Implant Indications - Children
• 12-23 mos: PTA ≥ 90dB• > 23 mos: PTA ≥ 70dB• Failure of improvement of speech and language skills
after proper amplification and aural rehab over 3 months• In older children:
– MLNT or LNT ≤ 30%
• Can also test in noise in borderline candidates
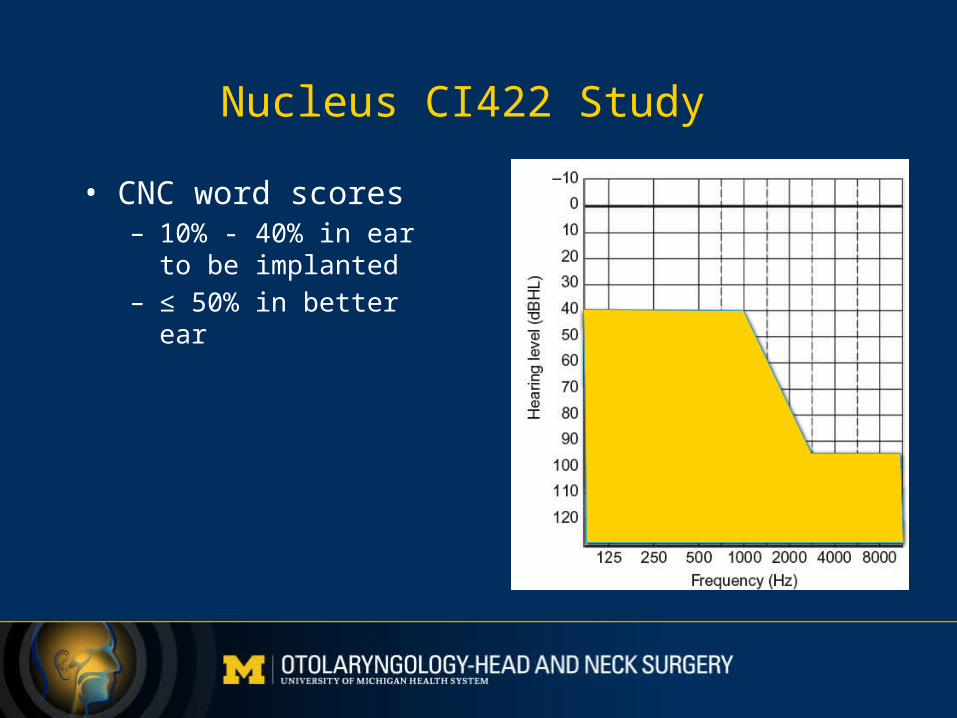
Nucleus CI422 Study
• CNC word scores– 10% - 40% in ear to be
implanted– ≤ 50% in better ear
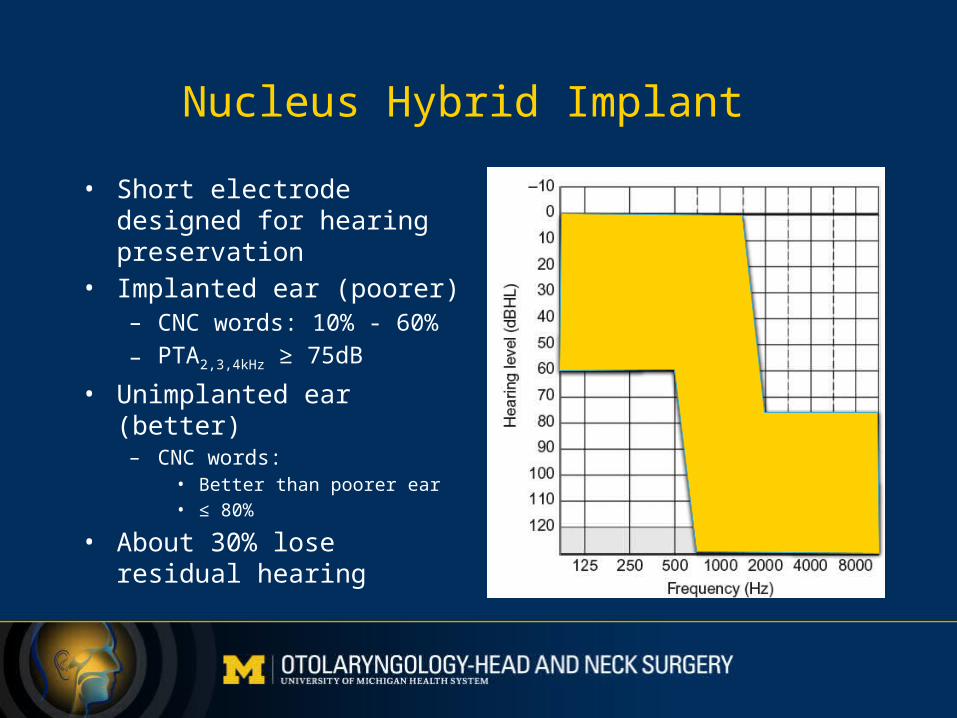
Nucleus Hybrid Implant
• Short electrode designed for hearing preservation
• Implanted ear (poorer)– CNC words: 10% - 60%
– PTA2,3,4kHz ≥ 75dB
• Unimplanted ear (better)– CNC words:
• Better than poorer ear• ≤ 80%
• About 30% lose residual hearing
Cochlear Implants for Single Sided Deafness
Cochlear Implants forSingle Sided Deafness
• Data from bilateral CI patients leaves no doubt that some patients perform substantially better with both CI’s vs. either one individually– Studies have shown benefits from:
• Binaural summation• Binaural squelch• Localization• Alleviation of head shadow effect
• CI experience in patients with one normal hearing ear began with unilateral deafness complicated by severe tinnitus
Cochlear Implants for SSD
• Vermeire (2009)– 20 adult patients with unilateral severe tinnitus and SNHL– Demonstrable speech-in-noise benefit
• Hansen (2013)– 29 adult patients
• Included 10 with CI in combination with labyrinthectomy for Meniere’s disease
– Localization improved in most
• Gartrell (2014)– Single patient carefully studied, clearly showed improved
localization
Cochlear Implants for SSD
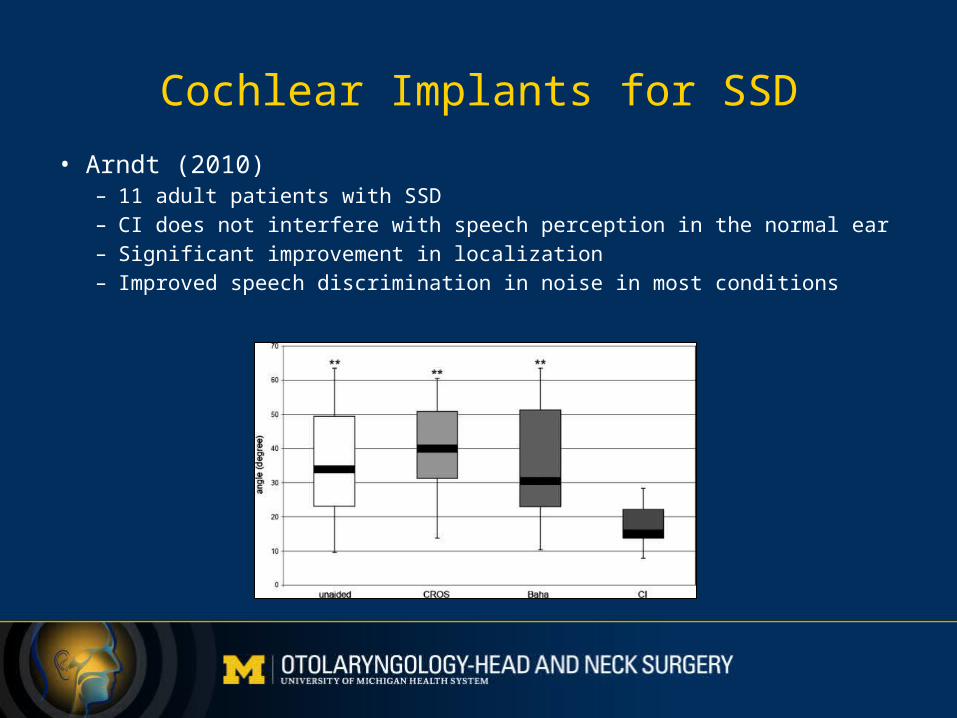
• Arndt (2010)– 11 adult patients with SSD– CI does not interfere with speech perception in the normal ear– Significant improvement in localization– Improved speech discrimination in noise in most conditions
Cochlear Implants in Children with SSD
• Hassepass (2012)– 3 children, 4-10 yo, non-traumatic SSD– Demonstrated improvement in localization and speech-in-noise– All children use device all waking hours at 1 year
• Plontke (2013)– Single case report: 8 yo boy after temporal bone fracture– Speech-in-noise tests improved to almost normal values in all
presentation modes– Improvement in localization was demonstrated
Cochlear Implant Illustrative Cases
• Extremely satisfied users– Complex bilateral otosclerosis patient after complete SNHL
following stapedectomy revision– Rapidly progressive bilateral Autoimmune Inner Ear Disease
(Cogan’s syndrome)
• Extremely unsatisfied user– Adult with congenital unilateral deafness
Cochlear Implants for SSD
• Bottom Line:– CI is a reasonable option for selected patients with SSD– Important considerations include:
• Recency of deafness• Etiology of deafness• Surgical status of ear• Hearing status of contralateral ear• Realistic expectations• Presence of tinnitus
Cochlear Implants and MRI
• The implanted magnet creates problems for patients needing MRI
• Until recently the magnets would have to be temporarily removed for MRI, and then replaced afterwards
• Med-El now has a clever magnet design that can be left in place for MRI’s up to 3T