Embed Size (px)
Citation preview
Karin Amrein, MD, MSc Assoziierte Professorin Medical University of Graz, Austria Division of Endocrinology and Metabolism
VITAMIN D Hilft es dem Intensivpatienten?

CONFLICTS OF INTEREST
• BBraun
• Fresenius Kabi
• MSD
• Novartis
• Novo Nordisk
• Nycomed
• Aguettant
• Sinapharm

VDR KNOCKOUT (KO) MAUS
Bouillon R et al. Endocrine Reviews 2008; 29:726-776
Keisala et al. Premature aging in vitamin D receptor mutant mice. J Steroid Biochem Mol Biol. 2009 Jul;115(3-5):91-7

HD
NICHT KLASSISCHE WIRKUNG
KLASSISCHE WIRKUNG
BASICS VITAMIN D
• VITAMIN D IST EIN STEROIDHORMON (VDR!)
• VITAMIN D REGULIERT ~ 200 GENE •CALCITRIOL (AKTIVES VITAMIN D) WIRD NICHT NUR IN DER NIERE PRODUZIERT • VITAMIN D HAT NEBEN DER KALZIUMHOMÖOSTASE VIELE ANDERE FUNKTIONEN
BASICS VITAMIN D BEI KRITISCH KRANKEN
(ERWACHSENE UND KINDER)
• EIN VITAMIN D MANGEL
• IST HÄUFIG
• MIT SCHLECHTEM OUTCOME ASSOZIIERT
(MORTALITÄT, NIERENVERSAGEN, SEPSIS…)
• FRAGE:
IST VITAMIN D NUR EIN MARKER ODER MEHR?
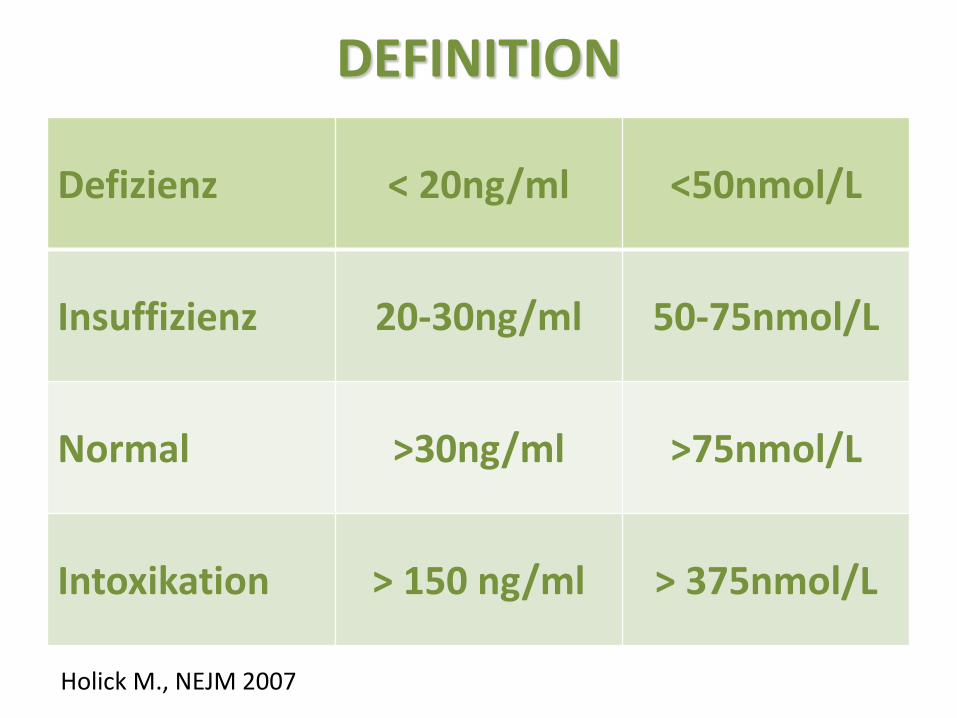
DEFINITION
Defizienz < 20ng/ml <50nmol/L
Insuffizienz 20-30ng/ml 50-75nmol/L
Normal >30ng/ml >75nmol/L
Intoxikation > 150 ng/ml > 375nmol/L
Holick M., NEJM 2007

Herz
Lunge/Muskel
Infektionen
Allgemein- Bevölkerung
Atemwegsinfekte, Tuberkulose
COPD, Myopathie,
Myalgia
Herzinfarkt, Herzinsuffizienz,
Sudden Cardiac Death
Kritisch Kranke
Nosokomiale Infekte Sepsis, SIRS
Lungenversagen Prolong. Weaning,
Critical Illness Myopathy
Kardiogener Schock, Arrhythmie
Adaptiert von: Lee P. et al., Intensive Care Med. 2009 Dec;35(12):2028-32
MECHANISMEN VON VITAMIN D - ICU

• Vitamin D Council Podcast 03: Vitamin D in hospitalized patients
• Intensive Care Network
http://www.vitamindcouncil.org/blog/vitamin-d-council-podcast-03-vitamin-d-in-hospitalized-patients/#

• randomisiert, doppelblind, placebokontrolliert • 5 ICUs (Neuro, Med, Chirurgie 3x) • 480 Pat. > 48 Std. auf ICU; 25(OH)D ≤ 20 ng/ml
Setting
• 540,000 IU Vitamin D3 vs. Placebo 1x po/NGS • 90,000 IU/ Monat vs. Placebo 5x Intervention
Aufenthaltsdauer im Spital Primärer Endpunkt Sekundäre Endpunkte
Mortalität, Aufenthaltsdauer auf ICU, Labor, 6-Monats-Follow Up…
VITDAL@ICU Correction of Vitamin D Deficiency in Critically Ill Patients
ClinicalTrials: NCT01130181
Amrein BMC Disorders 2012, JAMA 2014
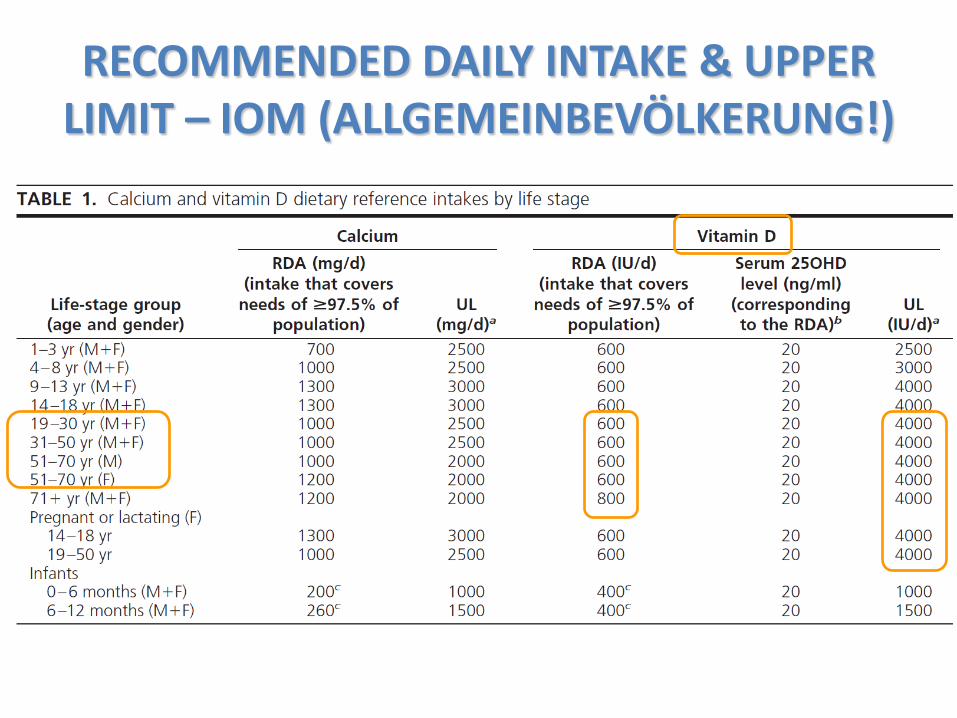
RECOMMENDED DAILY INTAKE & UPPER LIMIT – IOM (ALLGEMEINBEVÖLKERUNG!)

• randomisiert, doppelblind, placebokontrolliert • 5 ICUs (Neuro, Med, Chirurgie 3x) • 480 Pat. > 48 Std. auf ICU; 25(OH)D ≤ 20 ng/ml
Setting
• 540,000 IU Vitamin D3 vs. Placebo 1x po/NGS • 90,000 IU/ Monat vs. Placebo 5x Intervention
Aufenthaltsdauer im Spital Primärer Endpunkt Sekundäre Endpunkte
Mortalität, Aufenthaltsdauer auf ICU, Labor, 6-Monats-Follow Up…
VITDAL@ICU Correction of Vitamin D Deficiency in Critically Ill Patients
ClinicalTrials: NCT01130181
Amrein BMC Disorders 2012, JAMA 2014
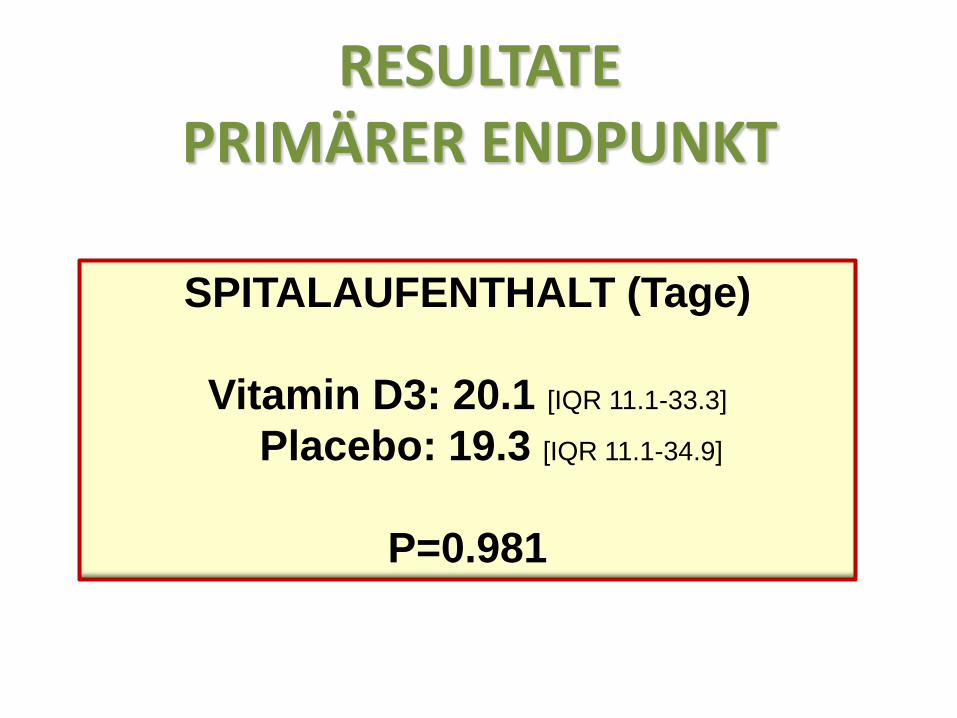
RESULTATE PRIMÄRER ENDPUNKT
SPITALAUFENTHALT (Tage)
Vitamin D3: 20.1 [IQR 11.1-33.3]
Placebo: 19.3 [IQR 11.1-34.9]
P=0.981

RESULTATE SEKUNDÄRER ENDPUNKT
% PATIENTEN MIT >30 NG/ML TAG 7
52% = KORREKTUR DES VITAMIN D - MANGELS

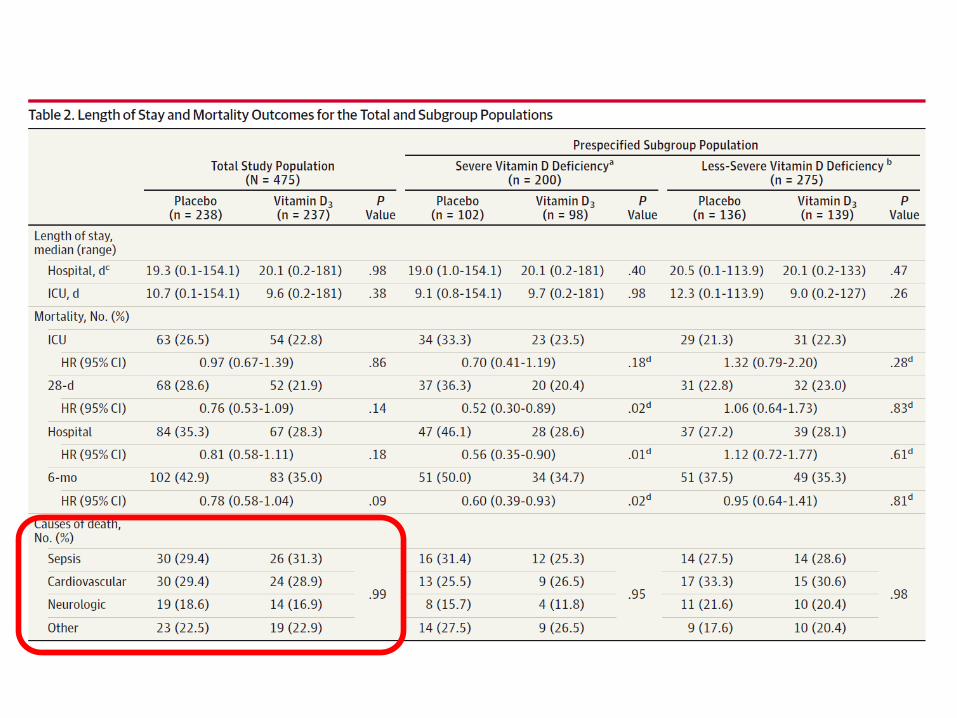
RESULTATE SEKUNDÄRER ENDPUNKT
SUBGRUPPE ≤ 12NG/ML (n=200; 42%)
SPITALSSTERBLICHKEIT
Vitamin D3: 28.6% Placebo: 46.1%
HR 0.56 [95%CI 0.35-0.90]
P=0.01 (log rank), 0.04 (for interaction)

RESULTATE SEKUNDÄRER ENDPUNKT
SUBGRUPPE ≤ 12NG/ML (n=200; 42%)
SPITALSSTERBLICHKEIT
Vitamin D3: 28.6% Placebo: 46.1%
HR 0.56 [95%CI 0.35-0.90]
P=0.01 (log rank), 0.04 (for interaction)

6 month mortality rate 42.9 vs. 35.0% P=0.087

6 month mortality rate 37.5 vs. 35.3%

6 month mortality rate 50.0 vs. 34.7%

VITAMIN D & MORTALITÄT

MENDELIAN RANDOMIZATION
Afzal, S.; Brøndum-Jacobsen, P.; Bojesen, S.E.; Nordestgaard, B.G. Genetically low vitamin D concentrations and increased mortality: Mendelian randomisation analysis in three large cohorts. BMJ 2014
96,000 Dänen, Copenhagen
- Primary endpoint: overall mortality, cancer mortality and other mortalities. - genes associated with 25(OH)D levels <8 ng/mL (<20 nmol/L) caused a 30% higher mortality risk and a 40% higher risk of cancer deathsm no correlation with cardiovascular death.
- Genetic variants in DHCR7,CYP2R1!?
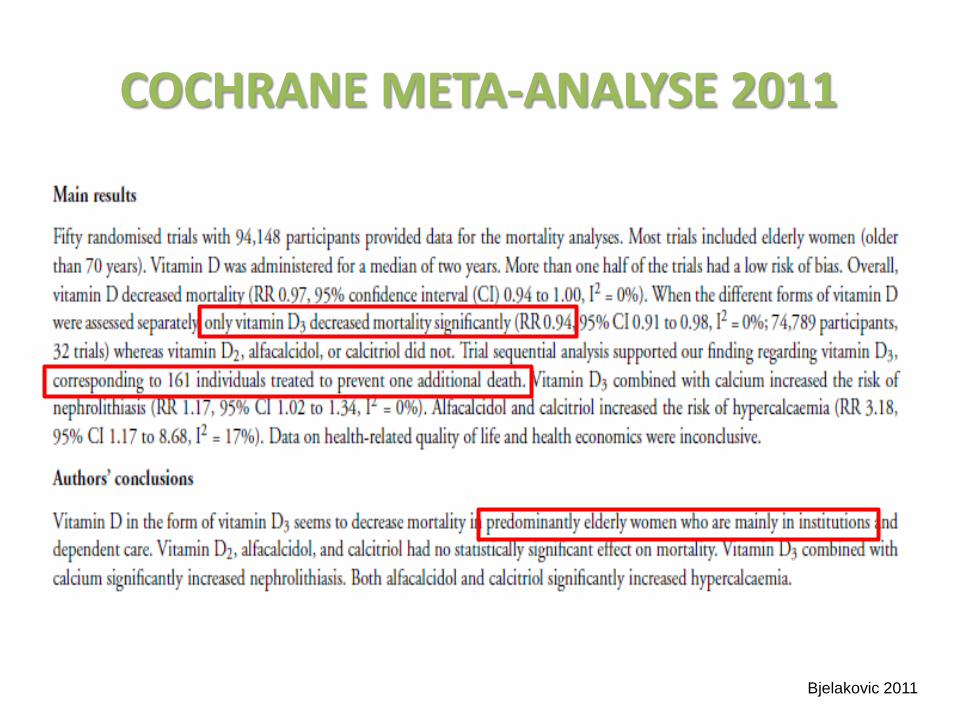
COCHRANE META-ANALYSE 2011
Bjelakovic 2011


COCHRANE META-ANALYSE 2014
Bjelakovic 2014
Main results We identified 159 trials, 56 randomised trials with 95,286 participants provided usable data on mortality. Most trials included women older than 70 years. The mean proportion of women was 77%. Forty-eight of the trials randomly assigned 94,491 healthy participants. Of these, four trials included healthy volunteers, nine trials included postmenopausal women and 35 trials included older people living on their own or in institutional care. The remaining eight trials randomly assigned 795 participants with neurological, cardiovascular, respiratory or rheumatoid diseases. Vitamin D was administered for a weighted mean of 4.4 years. Forty-five trials (80%) reported the baseline vitamin D status of participants based on serum 25-hydroxyvitamin D levels. Participants in 19 trials had vitamin D adequacy (at or above 20 ng/mL). Participants in the remaining 26 trials had vitamin D insufficiency (less than 20 ng/mL).
.... only vitamin D3 decreased mortality: RR 0.94 (95% CI 0.91 to 0.98); P = 0.002; I2 = 0%; 75,927
participants; 38 trials). Trial sequential analysis supported our finding regarding vitamin D3, with the
cumulative Z-score breaking the trial sequential monitoring boundary for benefit, corresponding to 150 people treated over five years to prevent one additional death. Vitamin D3 statistically significantly decreased cancer mortality (RR 0.88 (95% CI 0.78 to 0.98); P = 0.02; I2 = 0%; 44,492 participants; 4 trials).
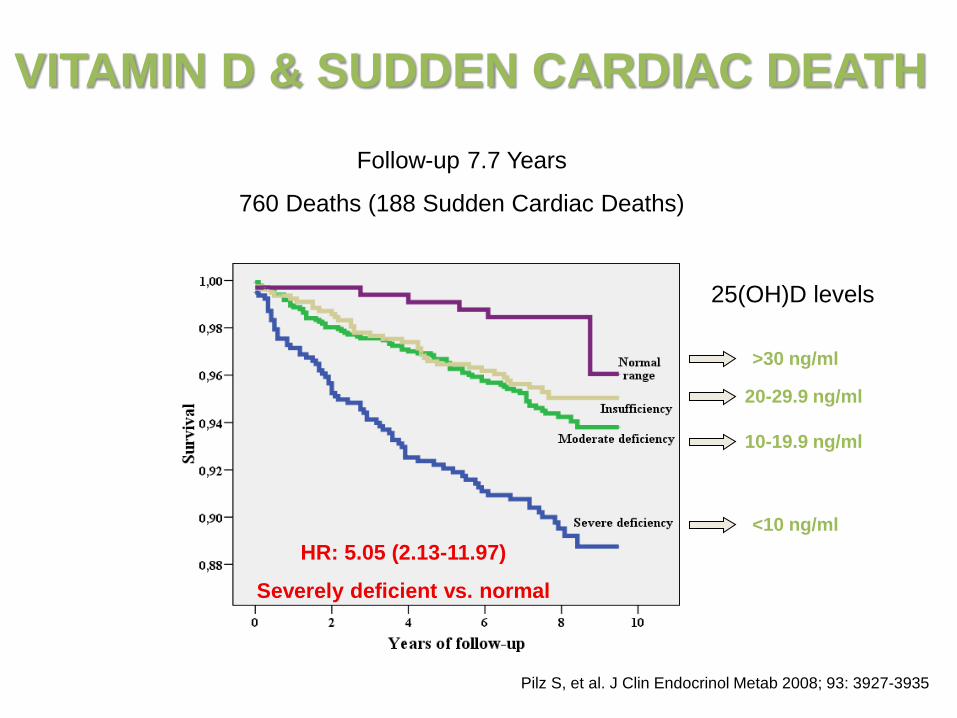
VITAMIN D & SUDDEN CARDIAC DEATH
Pilz S, et al. J Clin Endocrinol Metab 2008; 93: 3927-3935
Follow-up 7.7 Years
760 Deaths (188 Sudden Cardiac Deaths)
25(OH)D levels
>30 ng/ml
20-29.9 ng/ml
10-19.9 ng/ml
<10 ng/ml HR: 5.05 (2.13-11.97)
Severely deficient vs. normal
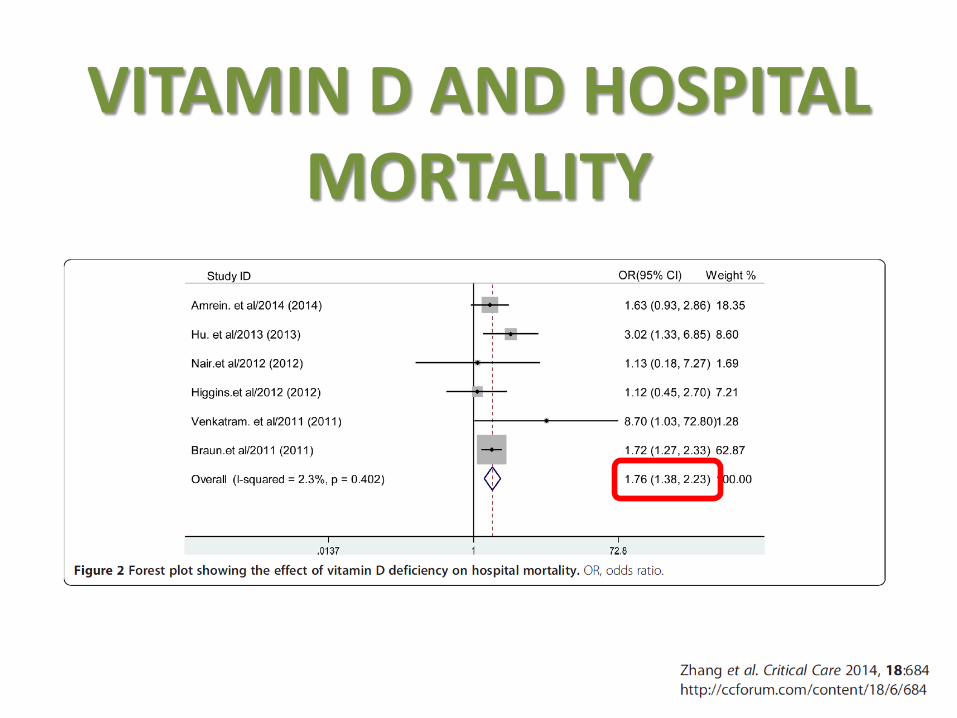
VITAMIN D AND HOSPITAL
MORTALITY
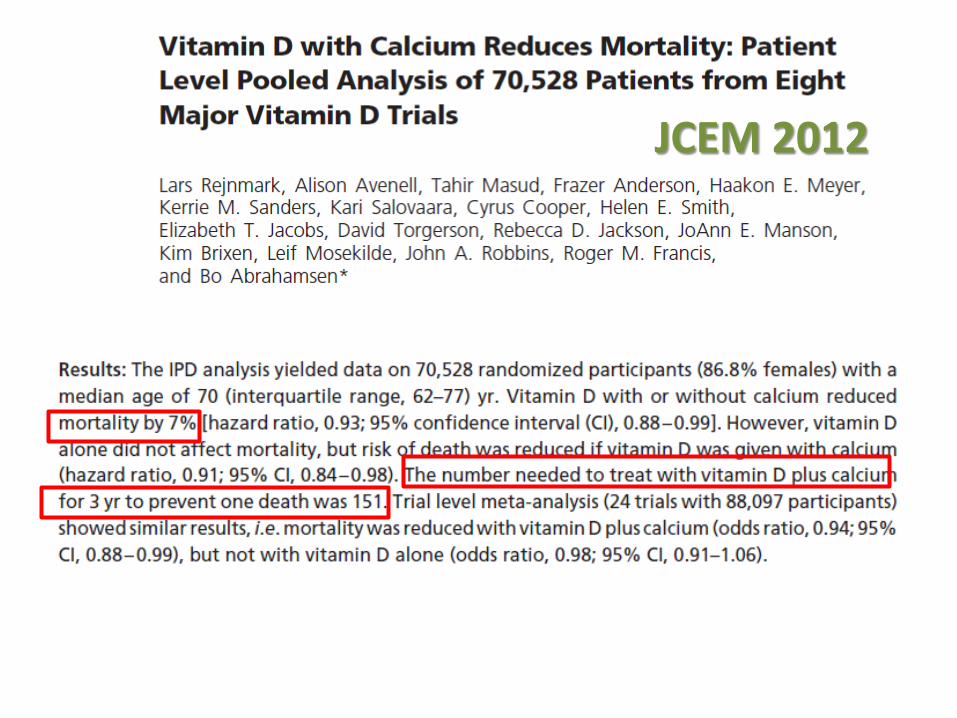
JCEM 2012


MORTALITY
Autier 2013
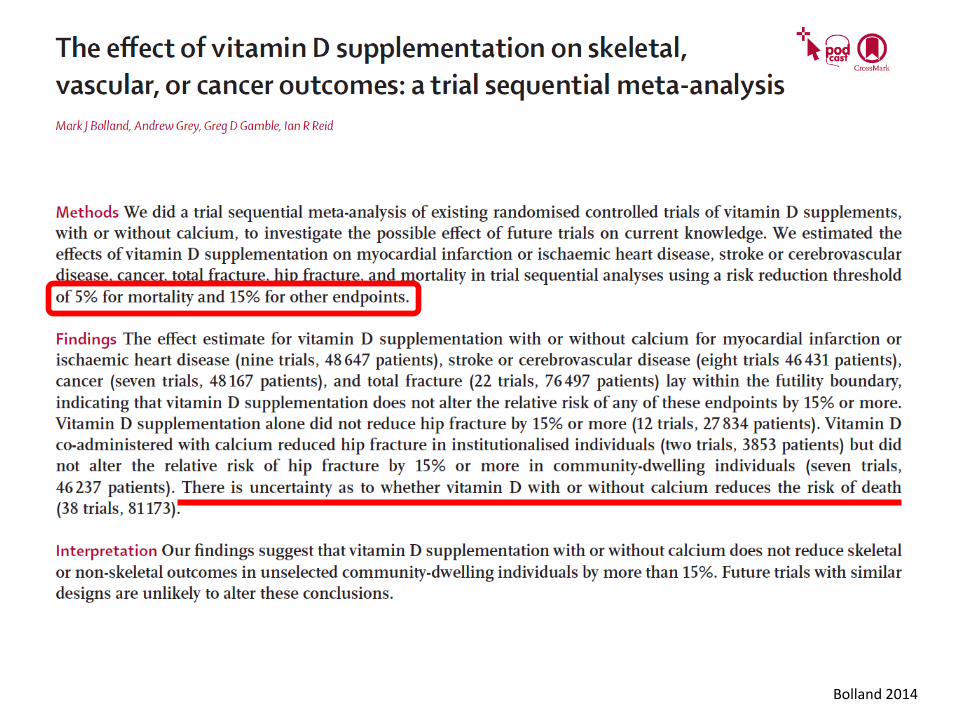
Bolland 2014

Heaney 2013

WELCHE INTERVENTIONEN HABEN JEMALS IM MULTICENTER DESIGN DIE MORTALITÄT REDUZIERT?
Mortality in Multicenter Critical Care Trials: An Analysis of Interventions With a Significant Effect*. Landoni, Giovanni et al. , Critical Care Medicine. 43(8):1559-1568, August 2015.

HELFEN ANTIBIOTIKA INTENSIVPATIENTEN?
JA!?!!! ABER NUR WENN EINE INFEKTION VORLIEGT

LARGE ONGOING RCT‘s
• VITAL Study:
• 25,000 pat > 50/55 yrs, US, 2010 – 2016
• FIND Study
• 18,000 pat, Finland
• Vida Study:
• > 5,000 elderly pat., NZ
• DO HEALTH Study:
• 2152 pat. > 70; 7 europ. Centers

LEITLINIEN
• ZIEL 25(OH)D > 20ng/ml
• IOM (ALLGEMEINBEVÖLKERUNG)
• 600-800 IU/d, max. 4000 IU/d
• ENDOCRINE SOCIETY (RISIKOPAT.)
• 1500 – 2000 IU PRO TAG!!!
• SICHERES LIMIT 10,000 IU/d Ross 2011 Holick 2011
CONCLUSIO
• ZIELSPIEGEL > 20 ng/ml (zumindest Knochen)
• ERFORDERLICHE DOSIS oft 2000 IU/d oder mehr
• LINK VITAMIN D UND ICU - Outcome
• VITdAL-ICU: Signifikant niedrigere Spitalssterblichkeit bei
prädefinierter Subgruppe mit schwerem Vitamin D
Mangel (NNT 6; absolute Differenz 17.5%, relative 44%)
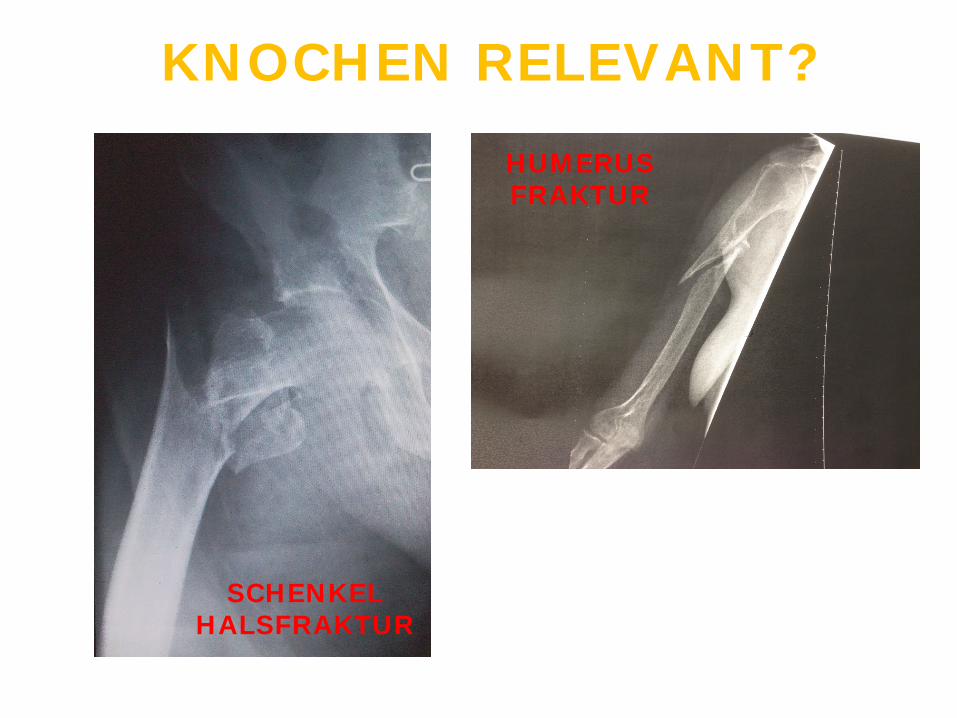
KNOCHEN RELEVANT?
SCHENKEL HALSFRAKTUR
HUMERUS FRAKTUR
FRAGILITY FRACTURES (fx)
• Fragility fx are associated with – increased morbidity – Increased mortality
• One year after hip fx – Institutionalization and death is a major
problem (up to 50%!)
Pasco 2005, Edwards 2009, Papaioannou 2010
FRACTURES AFTER ICU?
• MEN: 2.41 fx per 100 patient years • WOMEN: 3.84 fx per 100 patient years
• 65% increased risk compared with age-
matched random population sample • (HR 1.65, 95% 1.08-2.52, p=0.02, elderly
women) Orford CCM 2011

DANKE!
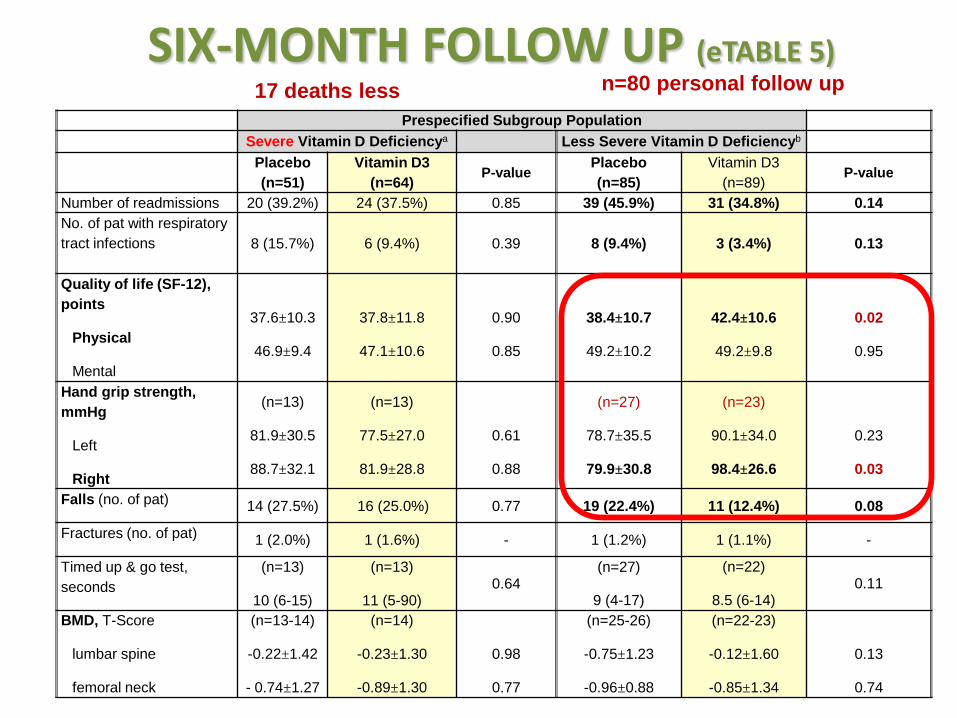
SIX-MONTH FOLLOW UP (eTABLE 5)
Prespecified Subgroup Population Severe Vitamin D Deficiencya Less Severe Vitamin D Deficiencyb
Placebo (n=51)
Vitamin D3 (n=64) P-value
Placebo (n=85)
Vitamin D3 (n=89)
P-value
Number of readmissions 20 (39.2%) 24 (37.5%) 0.85 39 (45.9%) 31 (34.8%) 0.14 No. of pat with respiratory tract infections 8 (15.7%) 6 (9.4%) 0.39 8 (9.4%) 3 (3.4%) 0.13
Quality of life (SF-12), points
Physical
Mental
37.6±10.3
46.9±9.4
37.8±11.8
47.1±10.6
0.90
0.85
38.4±10.7
49.2±10.2
42.4±10.6
49.2±9.8
0.02
0.95
Hand grip strength, mmHg
Left
Right
(n=13)
81.9±30.5
88.7±32.1
(n=13)
77.5±27.0
81.9±28.8
0.61
0.88
(n=27)
78.7±35.5
79.9±30.8
(n=23)
90.1±34.0
98.4±26.6
0.23
0.03
Falls (no. of pat) 14 (27.5%) 16 (25.0%) 0.77 19 (22.4%) 11 (12.4%) 0.08
Fractures (no. of pat) 1 (2.0%) 1 (1.6%) - 1 (1.2%) 1 (1.1%) -
Timed up & go test, seconds
(n=13)
10 (6-15)
(n=13)
11 (5-90) 0.64
(n=27)
9 (4-17)
(n=22)
8.5 (6-14) 0.11
BMD, T-Score
lumbar spine
femoral neck
(n=13-14)
-0.22±1.42
- 0.74±1.27
(n=14)
-0.23±1.30
-0.89±1.30
0.98
0.77
(n=25-26)
-0.75±1.23
-0.96±0.88
(n=22-23)
-0.12±1.60
-0.85±1.34
0.13
0.74
17 deaths less n=80 personal follow up






![arXiv:1610.06491v1 [astro-ph.EP] 20 Oct 2016 · Schmiedlstraˇe 6, 8042 Graz, Austria. (stefan.reimond@oeaw.ac.at) 1Space Research Institute, Austrian Academy of Sciences, Graz, Austria](https://img.pdfslide.us/doc/110x75/5e3306b2710be5743022ddc8/arxiv161006491v1-astro-phep-20-oct-2016-schmiedlstrae-6-8042-graz-austria.jpg)





















