Embed Size (px)
Citation preview

www.medicaltribune.com
May 2012
Dramatic blood sugar control with gastric surgery
FORUM
Biobanks: Research dream or ethical nightmare?
TREATMENT FOCUS
HRT in menopause: Are the benefits worth the risks?
MARKET WATCH
Pfizer launches pneumococcal vaccine for adults
NEWS
Bergamot orange a natural supplement
2 May 2012
Radha Chitale
Gastric surgery controlled blood sugar better than intensive medical therapy
among obese type 2 diabetics, according to the STAMPEDE trial, the results of which were presented at the 61st Annual Scientific Sessions of the American College of Cardiol-ogy meeting in Chicago, Illinois, US.
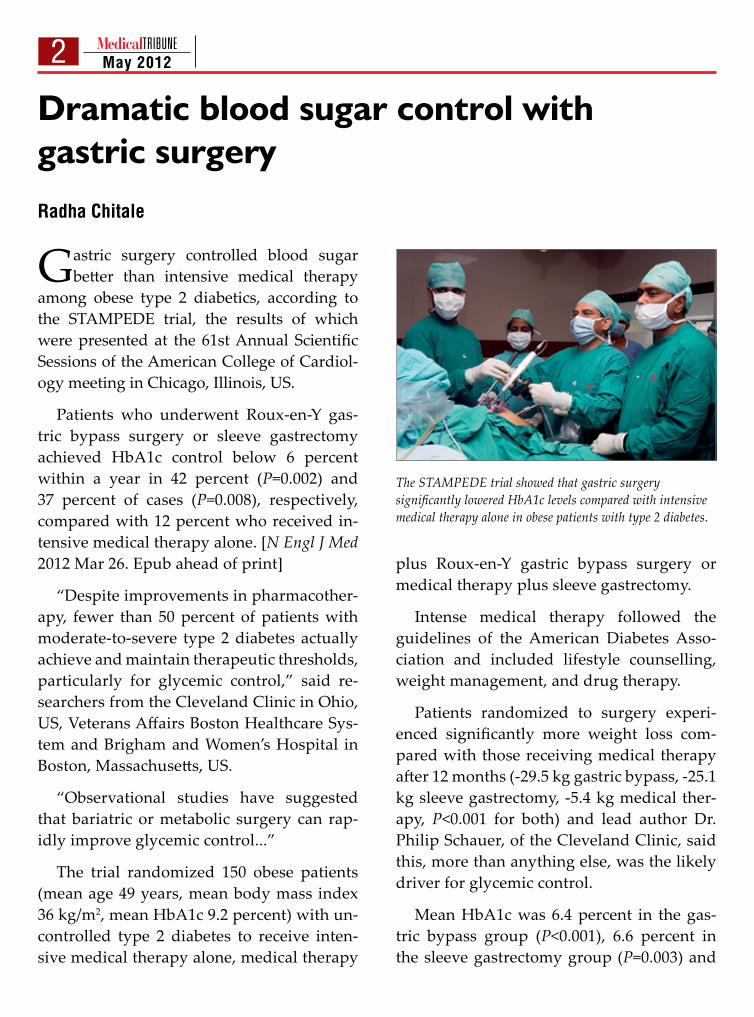
Patients who underwent Roux-en-Y gas-tric bypass surgery or sleeve gastrectomy achieved HbA1c control below 6 percent within a year in 42 percent (P=0.002) and 37 percent of cases (P=0.008), respectively, compared with 12 percent who received in-tensive medical therapy alone. [N Engl J Med 2012 Mar 26. Epub ahead of print]
“Despite improvements in pharmacother-apy, fewer than 50 percent of patients with moderate-to-severe type 2 diabetes actually achieve and maintain therapeutic thresholds, particularly for glycemic control,” said re-searchers from the Cleveland Clinic in Ohio, US, Veterans Affairs Boston Healthcare Sys-tem and Brigham and Women’s Hospital in Boston, Massachusetts, US.
“Observational studies have suggested that bariatric or metabolic surgery can rap-idly improve glycemic control...”
The trial randomized 150 obese patients (mean age 49 years, mean body mass index 36 kg/m2, mean HbA1c 9.2 percent) with un-controlled type 2 diabetes to receive inten-sive medical therapy alone, medical therapy
plus Roux-en-Y gastric bypass surgery or medical therapy plus sleeve gastrectomy.
Intense medical therapy followed the guidelines of the American Diabetes Asso-ciation and included lifestyle counselling, weight management, and drug therapy.
Patients randomized to surgery experi-enced significantly more weight loss com-pared with those receiving medical therapy after 12 months (-29.5 kg gastric bypass, -25.1 kg sleeve gastrectomy, -5.4 kg medical ther-apy, P<0.001 for both) and lead author Dr. Philip Schauer, of the Cleveland Clinic, said this, more than anything else, was the likely driver for glycemic control.
Mean HbA1c was 6.4 percent in the gas-tric bypass group (P<0.001), 6.6 percent in the sleeve gastrectomy group (P=0.003) and
Dramatic blood sugar control with gastric surgery
The STAMPEDE trial showed that gastric surgery significantly lowered HbA1c levels compared with intensive medical therapy alone in obese patients with type 2 diabetes.
3 May 2012
7.5 percent among patients receiving medi-cal therapy.
Patients who underwent surgery also sig-nificantly reduced or halted use of glucose control and cardiovascular medications.
“Reductions in the use of diabetes medica-tions occurred before achievement of maxi-mal weight loss, which supports the concept that the mechanisms of improvement in dia-betes involve physiologic effects in addition to weight loss...” the researchers said.
No deaths or life threatening complications occurred although four patients required a second surgery for complications.
In an accompanying comment, Dr. Paul Zimmet, Baker IDI Heart and Diabetes Insti-
tute, Melbourne, VIC, Australia, and Dr. K. George M. M. Alberti, Kings College Hospi-tal, London, England, said surgery would not be the “universal panacea” for obese patients with type 2 diabetes and pointed out that the study duration was only 1 year and that sur-gery has inherent hazards. [N Engl J Med 2012 Mar 26. Epub ahead of print]
“There is also the problem of ‘remission’ versus ‘cure,’” they said. “Type 2 diabetes is often progressive, and worsening of glycemic control over time is likely in many patients. However, some years of improved glycemia may well result in less microvascular disease.”
Both the researchers and commenters called for further studies on the long-term clinical effects of gastric surgery.
4 May 2012
Electronic skin patches for health monitoring Radha Chitale
Ultra thin ‘electronic skin’ patches that wirelessly relay health information
could free patients who need to be monitored from inpatient care.
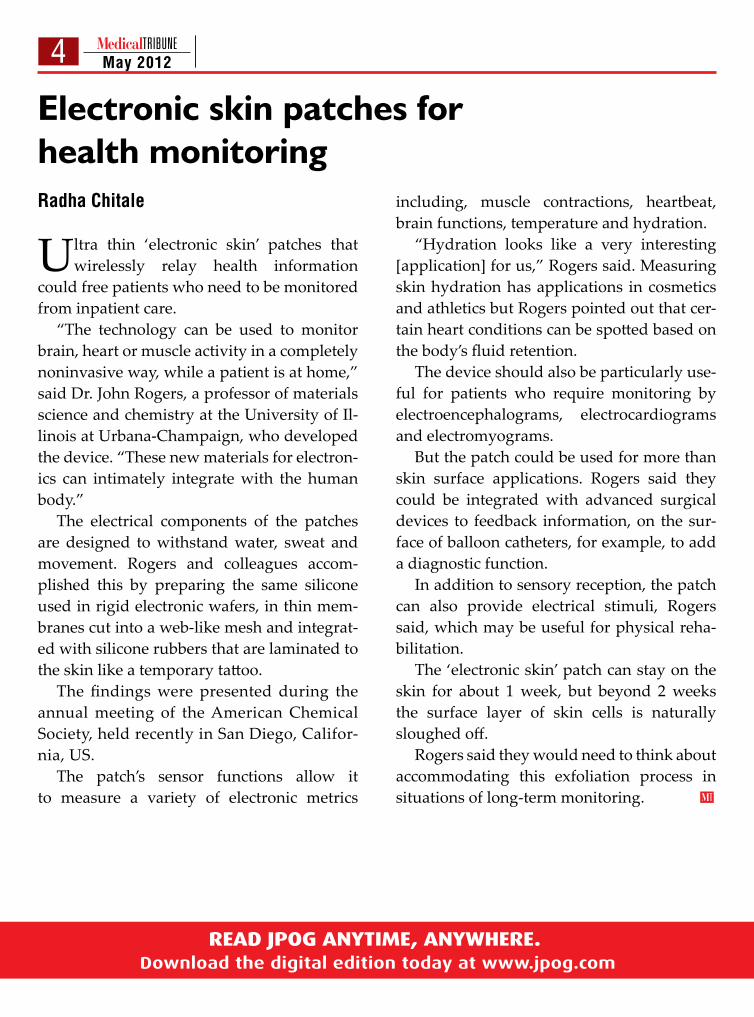
“The technology can be used to monitor brain, heart or muscle activity in a completely noninvasive way, while a patient is at home,” said Dr. John Rogers, a professor of materials science and chemistry at the University of Il-linois at Urbana-Champaign, who developed the device. “These new materials for electron-ics can intimately integrate with the human body.”
The electrical components of the patches are designed to withstand water, sweat and movement. Rogers and colleagues accom-plished this by preparing the same silicone used in rigid electronic wafers, in thin mem-branes cut into a web-like mesh and integrat-ed with silicone rubbers that are laminated to the skin like a temporary tattoo.
The findings were presented during the annual meeting of the American Chemical Society, held recently in San Diego, Califor-nia, US.
The patch’s sensor functions allow it to measure a variety of electronic metrics
including, muscle contractions, heartbeat, brain functions, temperature and hydration.
“Hydration looks like a very interesting [application] for us,” Rogers said. Measuring skin hydration has applications in cosmetics and athletics but Rogers pointed out that cer-tain heart conditions can be spotted based on the body’s fluid retention.
The device should also be particularly use-ful for patients who require monitoring by electroencephalograms, electrocardiograms and electromyograms.
But the patch could be used for more than skin surface applications. Rogers said they could be integrated with advanced surgical devices to feedback information, on the sur-face of balloon catheters, for example, to add a diagnostic function.
In addition to sensory reception, the patch can also provide electrical stimuli, Rogers said, which may be useful for physical reha-bilitation.
The ‘electronic skin’ patch can stay on the skin for about 1 week, but beyond 2 weeks the surface layer of skin cells is naturally sloughed off.
Rogers said they would need to think about accommodating this exfoliation process in situations of long-term monitoring.
5 May 2012 ForumBiobanks: Research dream or ethical nightmare?
Professor Alastair V. Campbell, Director of the Centre for Biomedical Ethics at the National University of Singapore, discussed the research potential of large-scale human health data-bases during the Asia-Pacific Research Ethics Conference, held recently in Singapore.
Biobanks, large epidemiological cohorts, including past and present populations,
that are associated with extensive samples of DNA and other biological materials, linked to health data, offer a rich source of informa-tion for public health research. Data capture health episodes affecting participants as they occur and are often followed up for decades. However, the possibility of information abuse or use for commercial gain is high. Creating and maintaining biobanks raises a number of major ethical questions that should be dealt with as we strive to define and defend the bio-commons.
Opportunities for research
Biobanks warrant unusual consideration. The data they contain offer a broad range of possible research opportunities, mined from a broad range of future health information that will be captured. This is large-scale data, with many participants, making it somewhat impersonal. In addition, a range of research-ers will have access to the data for a very long time.
The major features that make a biobank enterprise different from a piece of research are the need for general consent, appropriate stewardship, and justified trust.
Therefore, special measures are required for biobanks, rather than holding them to the
same standards of research protocol as other data sets.
The UK Biobank is the world’s largest re-source of genetic health and lifestyle data. It includes over 500,000 participants aged 40-69 and has the unique advantage of gaining data from the comprehensive British National Health Service.
This biobank took about 10 years of lead time in order to clarify the governance and ethical framework, in addition to public con-sultations. People would get a letter inviting them for an assessment at a clinic. A major part of the visit was spent explaining what they were giving consent to.
Participants in the UK Biobank consented to access to medical records for the remainder of their lives and after their death, without feedback on the results of their testing, other

6 May 2012 Forumthan minor initial tests for basic things like blood pressure levels.
Consent for use of participant data is re-scindable but not conditional. That is, you cannot specify what type of research you are willing to allow your tissues to be used for.
The “big brother” scenario
The nightmare scenario would be that “big brother” is watching. How can we be sure such databases won’t be used in ways other than what the participant signed up for? If, for example, stored genetic information could be accessed by court order in a society where au-thorities increasingly want access to citizens? In addition, if the commercial dominates, the whole purpose of the collection is in danger.
This is where ethics in governance comes in. If the ethics governing body believes the participant’s trust was abused, they say so, acting as proxy for the people involved.
The governance of the UK Biobank is in-dependent, and they alone guard the ethics and governance framework. They advise on revisions, monitor the UK Biobank and re-port their findings publicly and provide gen-eral advice.
This kind of data consolidation lends itself to growing into virtual biobanks. Virtual bio-banks are gaining popularity as researchers push to share and use population informa-tion across regions.
The issue of access is important in the face of pressure to link data sets internationally but it is complicated because there is no con-sistency in governance across international biobanks.
Ethicists could discuss whether it is right to trust international entities with biobank data without international consistency.
Security measures are important to have in place to prevent inappropriate access. Stewards must address who has access to the biobank data, to what extent access to other records is controlled and how easy it is to hack into the resource.
Safeguards to prevent abuse
One solution could be for a virtual bio-banks to link registries with safeguards to prevent identification. A person would be as-signed a serial number and the serial number is linked to the health data as a way to store data without compromising the safety of the subject. The link would be stored with an in-dependent trusted third party and without their cooperation, no one can link the health information back to the original subject.
Whatever the problems with broad consent, presumed consent is not sufficient. Biobanks are more than just a collection of tissue or data. Researchers have to see these as public prop-erty for the common good, uninfluenced by commercial or nationalist interests. The pros-pect for large-scale data sharing – for health not profit – could lead to greater information and more justice in healthcare.
Creating and maintaining
biobanks raises a number of
major ethical questions that should
be dealt with as we strive to define
and defend the biocommons
‘‘
Biobanks can be built “from the ground up”, as the UK Biobank was, but they can also be created by linking existing collections of tissue and registry information.
7 May 2012 Philippine Focus
PhilCAT, DOH celebrate World TB Day
Gabriel Angelo Sembrano, RN
Last March 12, 2012, the Philippine Coali-tion Against TB (PhilCAT), along with
the Department of Health (DOH) and other stakeholders, celebrated World TB Day with a strong cry: “Stop Tuberculosis (TB) in my lifetime!”
“Ours is a daunting task and we know that only through continuous cooperation and synchronized actions can we attain our tar-gets and goals. We also engage all stakehold-ers, not only organizations and government agencies, but private individuals as well. The fight versus TB concerns us all,” PhilCAT na-tional chairperson Vincent Balanag Jr. said during the event.
The event stressed that efforts against TB should focus on the often neglected but high-ly vulnerable sector, the children. According to the WHO, around 250,000 children get in-fected and 100,000 of them succumb every year from TB.
Childhood TB is associated with infected parents and other adults who are potential
transmitters that inadvertently pass on the in-fectious agent to children.
Childhood TB significantly contributes to the TB morbidity and mortality in the coun-try. Up to 50% of untreated infants and 15% of older children that has inactive TB will eventually develop to a disease within two years. Health experts suggest that if we con-trol this disease among adults, TB incidence will automatically taper since this is the main hindrance in achieving zero Childhood TB.
DOH’s answer to this is the National Tu-berculosis Program, with Directly Observed Treatment Short-course (DOTS) as one of its strategies. The NTP later on adopted the Public-Private Mix DOTS (PPMD) strategy, designed to increase case detection and to synchronize all TB care providers in manag-ing their TB patients.
Thus, PhilCAT advised that it is high time to “prioritize childhood TB, advocate for ad-dressing the challenges and grasp the oppor-tunities in its prevention and control.”
8 May 2012 Philippine Focus
First Viet Duc-PGH live telecon
Dr. Yves St. James Aquino
The first live, interactive laparoscopic tele-conference between the University of
the Philippines-Philippine General Hospital (UP-PGH) and Viet Duc University Hospital in Hanoi was conducted by the UP-PGH De-partment of Surgery last March 28, 2012. An Internet link was set up between UP-PGH and Viet Duc, which is considered the largest surgical center in Vietnam, along with five of Viet Duc’s satellite hospitals in Bac Ninh, Phu Tho, Son Tay, Thanh Hoa and Benh vien Nhi.
The first hour saw Viet Duc Hospital demonstrate a laparoscopic procedure with single incision port for left adrenalectomy performed on a 34-year-old male patient by a surgical team led by Professor Tran Binh Giang. And in the second half of the confer-ence, UP-PGH demonstrated a laparoscopic common bile duct exploration performed on a 19-year-old female patient by primary sur-geon Dr. Crisostomo Arcilla Jr., assisted by
Dr. Dante Ang and with annotation from Dr. Ramon de Vera.
“The long-term benefit of this would be in terms of teaching, in terms of education. We learn from each other and we save [money] because we don’t travel anymore to see what other surgeons in some parts of Asia are do-ing,” said Dr. Serafin Hilvano, former depart-ment chair and a coordinator with the Asia Pacific Advanced Network (APAN) Medical Working Group.
Hilvano added that the teleconference would be the first in a series of activities being planned with other foreign universities, as part of APAN’s thrust on promoting collaborations among medical institutions across Asia and the Pacific.
Current chair of the surgical department in UP-PGH, Dr. Eduardo Gatchalian, was also in attendance during the teleconference, and he expressed gratitude to the people from both universities for helping make the live telecon-ference a success.
2 15-30 April 2012 Regional
CLINICALCALCULATORS
AT YOUR FINGERTIPS
MIMS Consult offers over 90 must-have clinical calculators And scoring tools for iPhone and iPod Touch.
Time-efficientScoring
Instant Result
Browse ByCategory
Downloadit now!

9 May 2012 Philippine FocusCONFERENCE COVERAGE
Increasing detection of thyroid incidentalomas cause more diagnostic concerns
2012 Philippine Society of Endocrinology and Metabolism Annual Convention, 22-23 March, Manila Philippines
Dr. James Salisi
Technological advances in imaging devices have increased the detection rates of clini-
cally silent nodules such that there has been a sharp increase in the prevalence of thyroid in-cidentalomas, more specifically microscopic papillary cancer, said Dr. Thelma Crisostomo, chief of the Section of Endocrinology and Me-tabolism in Makati Medical Center. However, this has given rise to a clinical management dilemma and controversy since the mortality rate from this type of cancer has been stable and has not varied with the increased detec-tion rate, she added.
The recent clinical practice guidelines on thyroid incidentaloma presented by Crisos-tomo stated the following:
• More malignancies are discovered which are papillary microcarcinoma, but these are indolent, have excellent response to treatment and generally with low mortality;
• Fine needle aspiration biopsy (FNAB) for the high risk group or those patients with worrisome features;
• Non-surgical approach for low risk nod-ules with benign features;
• Thyroid lobectomy alone may be suffi-cient for small (less than 1 cm), low risk unifo-
cal, intrathyroid PTC (parathyroid carcinoma) in the absence of cervical nodal metastasis; and
• RAI (radioactive iodine) is not indicated for patients with unifocal cancer less than 1 cm.
According to Crisostomo, increased diag-nostic scrutiny gives rise to a management dilemma since the detection of these nodules raises the question of cancer. A two-fold in-crease in cancer incidence has been shown to be caused by increased sensitivity of imaging devices like high-definition ultrasonography, MRI, CT and PET scans. Mortality from this type of cancer however has remained stable at 0.5 deaths per 100,000 and this is because majority of incidentalomas have a benign or indolent nature, she added.
Nevertheless small nodule sizes are not a guarantee that the mass is of low risk. Papil-

10 May 2012 Philippine Focuslary cancer is the most common type of thy-roid nodule malignancy. Papillary mircrocar-cinomas however do not manifest as overt disease, some invade the lymph nodes but available research show that mortality range from 0.15 % to 5%. Recurrence is low but some are quite aggressive with 33% of small thy-roid cancers having extra thyroidal invasion. For incidentalomas, 44% had extrathyroidal invasion, 50% had regional node metastasis, with 12% malignancy rate.
According to Crisostomo, investigation of a thyroid incidentaloma should be done in a systematic and cost-effective manner. A bal-ance between curing the ill while not harm-ing those who are not ill must be found. With this in mind, the guidelines advice prudence in subjecting patients with incidentaloma to fine needle aspiration biopsy. Definitely, not all patients presenting with small thyroid nodules found on ultrasonography should undergo biopsy, said Crisostomo.
The gold standard for diagnosing thyroid nodules is gland resection and histopatho-logic examination. But not all patients with thyroid nodules should be subjected to sur-gery or even FNAB. Deciding which lesions should be treated is the key step in managing the disease. Thyroid nodules are commonly seen in women, in areas where diet has low iodine intake and in populations exposed to ionizing radiation.
The prevalence of thyroid incidentalomas by ultrasonography varies, ranging from 30 to 67%. This tool can provide enormous amount of information on deciding what kind of treat-ment a patient should have. Malignancy is suspected once diagnostic features like solid, internal vascularity, microcalcifications, hy-
poechogenicity, irregular margins, or abnor-mal lymph nodes are detected in conjunction with history and physical examination.
The next step would be to biopsy the pa-tient, which is influenced by a combination of patient characteristics and findings on ul-trasonography. Ultrsonographic features that guide decision to biopsy include the size, nature, presence of calcifications and echo-genicity of the nodules.
The strongest indications for a patient to be biopsied are patient with high-risk history, with suspicious sonographic features, and with solid to cystic features of nodules.
The tumor threshold size of a nodule for FNAB is > 1cm with characteristic isoechoic or hypoechoic appearance on ultrasound. FNAB is not indicated for purely cystic nodules.
Microcalcifications are bright foci small-er than 2 mm and are common in papillary cancer. They are calcified psammoma bod-ies and as such are a specific feature for malignancy.
Solid nodules have higher risk of malig-nancy, mixed nodules have less risk for ma-lignancy, cystic are more likely benign.
Many studies find overlap in features of malignant and benign nodules. In the end a single ultrasound feature cannot accurately predict malignancy.
Surgery is reserved for malignant lesions while observation is done for benign le-sions. Low-risk patients are recommended to have periodic ultrasound every 6 months to 12 months then 1 to 3 years to evaluate for growth; low risk and high risk patients with suspicious features are for ultrasound guid-ed FNAB, concluded Crisostomo.
11 May 2012 Philippine Focus
BAVS stimulation in management of adrenal pheochromocytoma
Dr. James Salisi
Bilateral adrenal venous sampling (BAVS) with glucagon stimulation aids in man-
agement of bilateral adrenal pheochromocy-toma, a study conducted by Dr. Chandy Lou Malong et al. at the University of Santo Tomas (UST) Hospital concluded. The investigators reviewed the records of patients who under-went BAVS with glucagon stimulation from 1997 to 2010 at the UST Hospital and tracked the status of their hypertension after removal of the dominant adrenal.
Majority of the patients included in the study suffered headache, paroxysmal hyper-tension and palpitation and 63% of them had right adrenal dominance. Mean age was 33 with highest systolic blood pressure greater than 186 mm Hg and diastolic pressure great-er than 113 mm Hg. The patients had been hypertensive for more than five years and re-quired more than three classes of anti-hyper-tensive drugs when they were seen at the UST Hospital.
Localization and subsequent surgical re-moval of the dominant adrenal resulted in lower blood pressure in patients with the dis-
ease, and fewer antihypertensive medications than pre-surgery.
While venous sampling is reserved for dif-ficult cases of small pheochromocytoma and bilateral adrenal venous sampling has been used in the early detection of disease, the study demonstrated how BAVS can be used to localize the dominant side of the adrenals.
Glucagon stimulation identifies the domi-nant lobe of bilateral adrenal pheochromo-cytoma by comparing the differences in epi-nephrine and norepinephrine post-challenge between the right and left adrenal. Identifica-tion of the dominant adrenal in turn guides the surgical management to relieve hyper-tension and prevent fatal cardiovascular out-comes.
Patients with pheochromocytoma exhibit symptoms such as headache, anxiety, dia-phoresis and palpitations as consequences of catecholamine secretion of the tumor. Pheochromocytoma occurs in 2 to 8 of 1 mil-lion persons per year, and about 0.1% of hy-pertensive patients have it. It is one of the correctable causes of hypertension and its removal can prevent fatal outcomes.
CONFERENCE COVERAGE
2012 Philippine Society of Endocrinology and Metabolism Annual Convention, 22-23 March, Manila Philippines
12 May 2012 Philippine Focus
Pre-IGT state shows other abnormal blood glucose parametersDr. Yves St. James Aquino
Glycosylated hemoglobin (HbA1c) and second hour glucose level after oral glu-
cose tolerance test (OGTT) were significantly increased in individuals in the pre-impaired glucose tolerance (pre-IGT) state versus those with normal OGTT, according to a local study done by Dr. Pilar Torres-Salvador et al., un-der the Section of Endocrinology and Metabo-lism, Department of Medicine, University of Santo Tomas (UST) Hospital.
Shown as a poster presentation, the retro-spective, cross-sectional study reviewed re-cords of patients in the out-patient endocri-nology clinic of UST Hospital who underwent 75 grams OGTT after being suspected of hav-ing type 2 diabetes.
“In the initial stage of diabetes mellitus type 2, the β-cell compensates for the insulin resistance by increasing insulin secretion to maintain normoglycemia, which we termed pre-impaired glucose tolerance state,” wrote the authors. The group demonstrated that in the pre-IGT state, the second-hour glucose is normal (<140 mg/dL) but the insulin levels are increased (>30 uIU/mL) after 75 grams OGTT.
Based on the collected data, the research-ers compared HbA1c of individuals with pre-IGT to those with normal OGTT. In addition, HbA1c was also correlated with the second-hour glucose and insulin levels in both groups.
According to the study, the HbA1c in the two groups were compared using the t-test, while correlation between the second-hour blood glucose level and insulin with the HbA1c was done using the Pearson correla-tion analysis.
Results of the study showed that the sec-ond-hour blood glucose were higher in indi-viduals with pre-IGT at ~118 mg/dL than those with normal OGTT at ~94 mg/dL (p=0.001). The HbA1c levels were also higher, with ~6.09% in the pre-IGT group compared with ~5.15% in the normal OGTT group (p<0.001). Insulin levels were also shown to be higher in the pre-IGT group at ~89.3 uIU/mL, com-pared with normal OGTT group at ~17.4 uIU/mL (p<0.001).
Pearson correlation (r) of the second-hour insulin and HbA1c showed r of 0.437 (p=0.011) in the normal OGTT group, while the pre-IGT group had 0.418 (p=0.017).
Glucose parameters including HbA1c, second-hour blood glucose and second-hour insulin post-OGTT were higher in the pre-IGT group compared with normal OGTT group. In addition, a positive correla-tion was demonstrated between the HbA1c and second-hour glucose levels after OGTT among individuals with pre-IGT state, the study concluded.
CONFERENCE COVERAGE
2012 Philippine Society of Endocrinology and Metabolism Annual Convention, 22-23 March, Manila Philippines

13 May 2012 Philippine FocusCONFERENCE COVERAGE
2012 Philippine Society of Endocrinology and Metabolism Annual Convention, 22-23 March, Manila Philippines
50mCi RAI comparable to 100mCi for thyroid remnant ablation Dr. Yves St. James Aquino
A retrospective cohort study showed lower dose radioactive iodine (RAI) of 50mCi
is as effective as 100mCi for thyroid remnant ablation after total thyroidectomy among 74 patients with low stage differentiated thyroid cancer seen at St. Luke’s Medical Center.
“The administered iodine activity needed to ablate the thyroid remains controversial and there is no consensus as to the recommended specific activity of RAI to ablate residual thyroid especially amongst the low-risk population,” said Dr. Evan Paulo Consencino, one of the study authors.
Consencino and Dr. Reynaldo Rosales with the Section of Endocrinology, Diabetes and Metabolism in St. Luke’s Medical center evaluated 241 patients admitted for RAI from 2006 to 2010. Data was collected from hospi-tal admission records, surgical pathology re-ports and out-patient records. Out of the 241 patients, 74 met the criteria, with 24 patients treated with 50mCi RAI and 50 patients treat-ed with 100mCi.
“Clinical characteristics, tumor characteris-tics and treatment-related data comprise the independent variables,” said Consencino. De-pendent variables included adverse events, efficacy of remnant ablation, need for repeat RAI and duration of stay in the isolation unit,
he added.“Successful remnant ablation is further de-
fined as the absence of clinical evidence, the absence of imaging evidence and the absence of biochemical evidence of persistent thyroid tissue,” clarified Consencino.
After 6 to 12 months of the initial RAI dose, whole-body imaging and checking of serum thyroglobulin of patients were done to evaluate efficacy of remnant ablation. Study data showed 16 patients (66.7%) in the 50mCi group and 38 patients (76%) in the 100mCi group had successful remnant ablation (p=0.526). Computed risk ratio for failure of remnant ablation in the 50mCi group is 1.39 (95% CI, 0.69 to 2.94). The study also noted that there was no statistically significant dif-ference in the need for repeat RAI between the two groups (RR 2.08, 95% CI, 0.31 to 13.91, p=0.440).
Subgroup analysis was performed using criteria such as age, gender, family history of thyroid cancer, focality, lobe involvement, post-operative stage, risk recurrence and lymph node metastasis. In most criteria, fail-ure of remnant ablation was more likely in 50mCi, but the differences were not statisti-cally significant.
Some of the most common acute adverse events noted after RAI administration in-cluded nausea (4.2% in the 50mCi group ver-

14 May 2012 Philippine Focussus 22% in the 100mCi group) and neck pain (4.2% in the 50mCi group versus 16% in the 100mCi group). Overall, reported adverse events were higher in the 100mCi group com-pared with the 50mCi group (36% versus 21%, respectively; 95% CI, 0.24 to 1.37; p=0.187).
Study data also showed duration of hos-pital stay was shorter among those who re-ceived 50mCi (median 2 days) compared with those who received 100mCi (median 2.5 days). According to Consencino, although this is not
statistically significant, patients may find it clinically significant.
“Our results demonstrate that the ad-ministration of 50mCi RAI is as effective as 100mCi for remnant ablation among patients with low-stage, differentiated thyroid cancer treated with total thyroidectomy. Adminis-tration of 50mCi RAI was clinically associ-ated with fewer short-term adverse events and shorter stay in isolation,” concluded Consencino.
Download
it now!
Clinical Calculators At Your Fingertips
MIMS Consult offers over 90 must-have clinical calculators and scoring tools for iPhone and iPod Touch.
15 May 2012 Philippine Focus
Nutrition therapy education on diabetes improves patient attitude
Gabriel Angelo Sembrano, RN
A local study by KP Sanchez et al., included among the poster presentations during the
convention, showed that a medical nutrition ther-apy (MNT) education session could significantly increase the knowledge, skills and attitude (KAP) of diabetic patients.
Coined by the American Diabetes Associa-tion, MNT is described as a nutritional diagnos-tic, therapy, and counseling service furnished by a registered dietitian or nutrition professional for the purpose of disease management.
Through MNT education sessions, diabetic pa-tients are able to understand the different factors that affect their health, helping them manage their condition.
Sanchez et al. conducted a pre-test post-test study to 47 diagnosed diabetes type 2 patients who willingly enrolled in the Diabetic Clinic of the Makati Medical Center. The thrust of the study was to establish the effectiveness of the medical nutrition therapy education session in increasing the knowledge, skills and attitude of diabetic patients. Interventions involved nutrition counseling done by a registered dietician, as well as teaching - imparted through lectures, partici-patory demonstrations and discussions, coupled with visual aids like posters and charts.
When the baseline scores were compared to post-test scores, the study revealed that partici-
pants were able to show significant increase of (p value < 0.05) 27.2%, 60.8% and 44.6% for their level of KAP, respectively.
More particularly, although patients got decent scores in their pre-test, what was remarkable was the increase in the number of patients who got scores of above 80% in all three post-tests.
According to the World Health Organization, uncontrolled hyperglycemia could lead to “seri-ous damage to many of the body’s systems, espe-cially the nerves and blood vessels.” Uncontrolled diabetes could lead to complications, organ fail-ure and eventually death. In 2004, WHO esti-mated that around 3.4 million people died from consequences of high blood sugar and more than 80% of these deaths come from low- and middle-income countries.
Sara F. Morris, RD, MPH, a research assistant in the Department of Nutrition at the Universi-ty of North Carolina in Chapel Hill and Judith Wylie-Rosett, RD, EdD, a professor and head of the Division of Behavioral and Nutritional Re-search in the Department of Epidemiology and Population Health at the Albert Einstein College of Medicine in Bronx, New York said in their pub-lished study entitled Medical Nutrition Therapy: A Key to Diabetes Management and Prevention that “because of the direct correlation between diet and diabetes management, MNT provided by a registered dietitian is a key complement
CONFERENCE COVERAGE
2012 Philippine Society of Endocrinology and Metabolism Annual Convention, 22-23 March, Manila Philippines
16 May 2012 Philippine Focusto traditional medical interventions in diabetes treatment.” In fact, the Standards of Medical Care in Diabetes stress that education encompasses each of the major components of diabetes treat-ment, namely diet, oral hypoglycemic therapy and insulin treatment.
Nutrition is an essential part of diabetes care since blood sugar level responds to different diets. Through MNT, diabetics would know which foods to avoid in order to maintain the right blood sugar level. Hence, complications associated with DM would be likely prevented.

17 May 2012 Philippine Focus
US Endo Society guidelines on vitamin D updated
Gabriel Angelo Sembrano, RN
The latest US Endocrine Society’s Clinical Guidelines on vitamin D, which was au-
thored by Michael J. Holick, Neil C. Binkley and others, and published last year in the Journal of Clinical Endocrinology and Me-tabolism, was presented by Dr. Aimee An-dag-Silva, assistant professor of De La Salle University (DLSU) College of Medicine and active consultant of DLSU Medical Center and San Juan de Dios Hospital.
Andag-Silva said that based on the new CPG on vitamin D, only those whose serum 25-Hydroxyvitamin D [25(OH)D] blood lev-els of 30 μg/mL and above are getting ade-quate vitamin D. Any level that is lower than that is said to be insufficient, and below 20 μg/mL is considered deficient. But she added that much higher level of vitamin D is better. The minimum level is at 30 μg/mL, and 40 to 60 μg/mL is the recommended range for both children and adults.
According to the Food and Nutrition Re-search Institute-Department of Science and Technology (FNRI-DOST), in the Philippines, the recommended dietary intake of vitamin D is 10 to 15 μg/day or 400 to 600 IU/day.
In order to achieve adequacy, defined as
above 30 μg/mL of 25(OH)D in the blood level, the updated CPG on the vitamin recom-mends that infants, those aged 1 to 18 years old, and lactating or pregnant women who belong to this age group need to have 1,000 IU of vitamin D daily. For those aged 19 years old and above, and pregnant or lactating adults, 1,500 to 2,000 IU of vitamin D daily is needed to raise 25(OH)D to greater than 30 μg/mL.
Andag-Silva mentioned that vitamin D is not produced by the body without the help of the ultraviolet rays from sunlight, and obtaining sufficient vitamin D from natural food sources alone is difficult. She added that although vitamin D can be found in certain foods in small amounts, it is still best to get it through sun exposure because vitamin D acquired from sunlight lasts twice longer in the body and has better bioavailability.
Andag-Silva explained that the best time to get exposed to direct sunlight is between 10AM and 3PM without the use of sun-screen. Some vitamin D researchers suggest having approximately 5 to 30 minutes of sun exposure at least twice a week. Using sun-screen with sun protection factor (SPF) of 30 and above reduces vitamin D-producing UV rays of up to 95%, which conflicts with recom-mended practices to avoid skin cancer.
CONFERENCE COVERAGE
2012 Philippine Society of Endocrinology and Metabolism Annual Convention, 22-23 March, Manila Philippines
18 May 2012 Philippine FocusIn cases where vitamin D deficiency is di-
agnosed, the recommended values for infants and those whose age is between 1 to 18 years old are 2,000 IU/day or 50,000 IU/week for 6 weeks. For those aged 19 years old and above, the correctional dose is 6,000 IU/day or 50,000
IU/week for 8 weeks. The US Endocrine Society underscores the
significance of vitamin D in achieving opti-mum health. It stresses that almost each sin-gle cell in the human body has an interaction with the vitamin.
19 May 2012 Philippine FocusTREATMENT FOCUS: Hormone replacement therapy
HRT in menopause: Are the benefits worth the risks?
Dr. Adrian Paul Rabe
A few months before her 50th birthday, Diana* started experiencing hot flashes. Her husband noted decreased libido, while she complained of vaginal drying and soreness. She also felt tired and depressed despite having no new problems nor strenuous physical activity. After a few weeks of these symptoms, she consulted a gynecologist and was told that she had the classic presentation of menopause.
Menopause results from the reduction and eventual loss of estrogen. It is universal among women in their late 50s, but may oc-cur earlier through spontaneous or iatrogenic mechanisms.
Hormone replacement and its benefits
Hormone replacement therapy (HRT) for menopause seeks to replace lost estrogen. Some forms of replacement also contain pro-gesterone and its derivates, as well as testos-terone. The hormones may be given through multiple routes, such as tablets, patches, vagi-nal rings or injection. Progesterone is given primarily to oppose estrogen, particularly among patients who still have a uterus, while testosterone may be used to treat decreased libido.
The general benefits of HRT include the prevention and reduction of vasomotor symp-toms (hot flashes), vaginal atrophy (includes dryness, soreness, dyspareunia, nocturia),
osteoporosis, joint cartilage loss, colorectal cancer and dementia or cognitive decline.
Despite these multiple benefits, only some women are able to access HRT, according to Dr. Rosiebel Esguerra, a specialist in repro-ductive endocrinology from the University of the Philippines – Philippine General Hospital (UP-PGH).
“Despite the indication for HRT, not every-one is able to afford the treatment. In 2011, a total of 483 women who consulted for meno-pause at [UP-PGH]. There were only 21 pa-tients on the treatment,” said Esguerra
Resolving conflicts of evidence in hormone replacement
Diana was then advised hormone replacement therapy. She was told by her relatives in the United States that hormone replacement could cause a variety of ailments, from ovarian malignancy and

20 May 2012 Philippine Focusbreast cancer to heart attack and stroke. She asks her physician if the benefits of hormone therapy outweigh the risks.
In 2002, a landmark series of studies, the Women’s Health Initiative (WHI), analyzed cardiovascular risk of women, including women in menopause. It found an excess number of cardiovascular deaths among older women receiving hormone replacement. Other trials, such as the Million Women Study in the United Kingdom, have also found increases in stroke, breast cancer, and endometrial bleeding. The progesterone component of HRT has even been linked to an increase in breast cancer. These multiple complications have led many patients and doctors to refrain from utilizing hormone replacement therapy.
In order to address these concerns, a systematic review was performed by Harman and colleagues on the effect of HRT and cardiovascular events. The results were published in the American Journal of Medicine in March 2011. It discovered that the increase in coronary disease risk was “confined to more remotely menopausal or older women.” The average of the population in WHI was 63 years. In the Nurses’ Health Study, where the average age was 51 years, women who started HRT at or near menopause had “significant coronary heart disease protection” compared to those who started later. This set the foundation for the “timing hypothesis.”
Practitioners in the Philippines refer to the Clinical Practice Guidelines on Menopause, published in 2009. However, a decade since the release of the WHI, the International Menopause Society (IMS) has taken into consideration evidence that has come to light.
Individualizing hormonal therapy
After weighing the risks and benefits of HRT, Diana is more amenable to the treatment. She reports that an internet search has revealed many kinds of HRT, and inquires which one is best for her.
Unlike most guidelines, the IMS does not recommend specific types of HRT, nor does it pose a specific dose and regimen. HRT should be customized and individualized when administered. There have been only a few studies that have shown the superiority of one form of HRT over another.
“The most common regimen used is therapy combining estradiol hemihydrate 2mg and drosperinone 1mg. Another common regimen used is conjugated equine estrogen at 0.625mg/tab,” said Esguerra.
Since the main goal of HRT in menopause is to relieve symptoms brought about by estrogen loss, HRT should be given only to symptomatic patients. It should be started early in menopause. Initiating treatment in patients beyond 60 years of age and in patients who have suspected or known cardiovascular disease is not recommended.
The duration of treatment should last as long as the patient experiences symptomatic relief. Annual health checks with a thorough physical examination and focused laboratory work-up serve to assess cardiovascular risk.
There is no clinically proven superior form of HRT. However, progesterone should be added to systemic estrogen in all women with a uterus in order to prevent endometrial hyperplasia and cancer. The exception to the progesterone rule is the use of low-dose vaginal estrogen, where the level of hormone is too low to stimulate the endometrium. Progesterone lowering is also necessary to

21 May 2012 Philippine Focusdecrease the risk for breast cancer. Thus, the patient’s HRT should be titrated so the lowest effective dose is achieved.
The specific route of administration in HRT should be dictated by the patient’s clinical profile and preferences. For instance, in patients with an increased risk of stroke or venous thromboembolism, transdermal estrogen may be utilized in order to avoid the first-pass effect in the liver and decrease these risks.
Androgen insufficiency may also manifest in women with menopause. These women have decreased libido, lowered mood and a diminished sense of well-being. To improve the quality of life, testosterone may also be administered.
Wholistic approach to health during menopause
The IMS recommends that HRT is only part of the wholistic approach to menopausal health. A cardiovascular diet is prescribed, comprised of multiple daily servings of fruits, vegetables, and whole grain fiber. At least 2 servings of fish a week is recommended. Total fat should be low, with the exception of olive oil, which was proven to decrease cardiovascular risk. Weight loss is also crucial in preventing the occurrence of cardiovascular events. Studies have demonstrated that 5 to 10% loss of body weight already results in significant cardiovascular risk reduction.
For menopausal women, exercise should be performed for at least 150 minutes/week. No specific exercise is recommended. The type and intensity should be tailored to the patient’s aerobic fitness, with care to prevent injury.
Smoking cessation and reduced alcohol
consumption (no more than 1 alcohol unit a day) are necessary. These improve cardiovascular health and decrease the risk for cancer.
Hormone replacement and healthy aging
A few months after initiating HRT and making significant lifestyle changes, Diana reports feeling in excellent health. She follows up regularly with her reproductive endocrinologist for adjustment of her hormone therapy. She’s keen on completing a 42-kilometer marathon with her husband, and is currently training for it.
Hormone replacement therapy indeed in-troduces a plethora of benefits to menopausal women that would help increase their quality of life. With a wholistic, individualized ap-proach to the use of HRT, menopause need not be feared, but faced with the dignity and comfort of healthy aging.
*Subject’s last name withheld for privacy
REFERENCESManson JE, Hsia J, Johnson KC, Rossouw JE, Assaf AR, Lasser NL, Trevisan M, Black HR, Heckbert SR, Detrano R, Strickland OL, Wong ND, Crouse JR, Stein E, Cushman M; 2003 Women’s Health Initiative Investigators. Estrogen plus progestin and the risk of coronary heart disease. N Engl J Med 349:523–534.
Beral V, Reeves G, Bull D, Green J; for the Million Women Study Collaborators. Breast cancer risk in relation to the interval between menopause and starting hormone therapy. J Natl Cancer Inst. 2011 Jan 28.
Harman SM, Vittinghoff E, Brinton EA, Budoff MJ, Cedars MI, Lobo RA, Merriam GR, Miller VM, Naftolin F, Pal L, Santoro N, Taylor HS and Black DM. Timing and duration of menopausal hormone treatment may affect cardiovascular outcomes. Am J Med. 2011 March; 124(3): 199–205.
Stampfer MJ, Colditz GA, Willett WC, et al. Postmenopausal estrogen therapy and cardiovascular
disease. Ten-year follow-up from the Nurses’ Health Study. N Engl J Med. 1991; 325:756–762.
Sturdee DW and Pines A on behalf of the International Menopause Society Writing Group. Updated IMS recommendations on postmenopausal hormone therapy and preventive strategies for midlife health. Climacteric 2011;14:302–320.

22 May 2012 Philippine Focus
The physician as a landscape artist and a hotelier
Dr. James Salisi
Sarangani Highlands Hotel sits on a hill overlooking Sarangani bay. Co-owned
and managed by Dr. Tranquilino Ruiz, the hotel started out as a garden that evolved into a restaurant with a spectacular view of the largest bay in the Philippines; and later on it expanded into a 21-room hotel with function rooms.
In 2007, Ruiz, in partnership with Dr. Ana-bel Abella and a business partner from Manila, acquired a piece of land in General Santos, 300 feet above sea level. They started design-ing landscapes and people started coming in; eventually, these frequent visitors asked them to put up a restaurant. When business picked up, they expanded and put up a hotel now called Sarangani Highlands.
“It is named after the bay, Sarangani Bay, Sarang ani which is an Indonesian phrase for ‘this is our territory,’” said Ruiz. As operations manager, he spends most of his time running the business, taking care of the restaurant and the hotel as well as the maintenance of the landscape of the resort.
What started out as a hobby evolved into a business. Ruiz would do landscaping on the side and even attended workshops to know more. He did Manny Pacquiao’s house, com-mercial spaces like hotel and sports center, and other doctor’s houses in General Santos. He also acted as a consultant in the design of Plaza General in General Santos as well as for
the General Santos City Airport.Because people know that he is a doctor
(he introduces himself as one), the perception about their place is improved especially with regard to cleanliness. “Being a doctor is an advantage when you go into business. Loans from banks are easier to get,” he said.
Ruiz is a direct descendant of the first colo-ny supervisor of Agricultural Colony Number 9, Don Tranquilino Ruiz, who was appointed by Governor Francis Burton Harrison. Ruiz has a degree in Commerce and secretly took science courses in preparation for medicine, not law, which his father wanted him to take.
After obtaining his medical degree from Southwestern University Matias H. Aznar College of Medicine, he worked as resident physician in Bohol for 10 years. He went back to Glan and established a clinic.
Since he comes from a political family, he started engaging with the community in the
BEYOND THE CLINIC

23 May 2012 Philippine Focusearly 90s by promoting tourism in Glan. He converted their ancestral house into a gallery of memorabilia from the early days of Glan. Open to the public for viewing, his art col-lection and family heirlooms told the history of the Ruiz family and the history of Glan.
He eventually ran for public office in the last elections and won a seat in the town coun-cil. Because of his experience as a doctor and as part of the hospitality industry, he has been selected to head the committees on tourism, health and social services.
His work in the tourism industry started in 1994 when he spearheaded activities related to it. For example, he inspired the indigenous people like the B’laan to engage the younger generations of their tribe to continue their weaving tradition and basketry.
Ruiz is keen on promoting tourism because he believes that it creates jobs for the people especially in Glan, Sarangani, which has pris-tine white-sand beaches and an expansive view of Sarangani bay that regularly attract tourists from neighboring General Santos City and the rest of southern Mindanao.
“We should always provide people with jobs. Kapag may trabaho ang tao, they will not … ask for dole out from the politicians,” he said.
His eye for landscape design has helped him create a unique environment for Saran-gani Highlands Hotel. Well-tended flower gardens and trees that surround the hotel provide a romantic backdrop for weddings while the bonsai trees from his fellow physi-cians, wooded pathways, and fountains lend a tranquil vibe that easily relaxes the mind.
But more than the spectacular view and the privilege of shaping an aesthe-tically pleasing space for visitors in General Santos City, what he likes about the Sarangani Highlands is that he gets to meet a lot of people. The hotel and its gardens are his sanctuary from the stresses of being a physician-on-call and a public ser-vant.
We should alwaysprovide people with jobs.
Kapag may trabaho ang tao, they will not ask for dole out
from the politicians
‘‘2 15-30 April 2012 Regional
CLINICALCALCULATORS
AT YOUR FINGERTIPS
MIMS Consult offers over 90 must-have clinical calculators And scoring tools for iPhone and iPod Touch.
Time-efficientScoring
Instant Result
Browse ByCategory
Downloadit now!
24 May 2012 Philippine FocusNOTES ON LEADERSHIP
The Medical Tribune’s Dr. Yves Saint James Aquino talks to presidents of specialty societies to discuss their roles in promoting their respective fields
Leading the way for the educated patient
A fulfilling aspect in leading one of the old-est specialty societies in the Philippines
was being able to recommend changes to im-prove medical training and practices, said Dr. Gabriel Jasul, immediate past president of the Philippine Society of Endocrinology and Me-tabolism (PSEM).
“One of the thrusts of PSEM ... is a strong emphasis on training of future endocrinolo-gists,” explained Jasul, who holds his clinic at St. Luke’s Medical Center in Quezon City.
“We try to really watch how we start our trainees from their training years up to their
early practice years, because we feel that, real-ly, the future of the specialty of endocrinology is based on these young trainees. They are the lifeline of the society.”
To further strengthen the training of the fellows, PSEM has collaborated with local and international societies, especially in do-ing more research, Jasul shared.
“The Philippines is slowly gaining its lead-ership role in the region. Even for research, many drug trials, new drugs that are not yet in the market, are being tested in the Philip-pines. So, there are many endocrinologists as well as other specialists who are now involved in drug trials. That’s a positive development because it means we’re able to participate in international undertakings,” he explained.
According to Jasul, these kinds of research would help improve the way specialists man-age their patients. However, he emphasized that the real challenge is increasing patients’ awareness of the fact that most of the non-communicable diseases handled by the spe-cialty (eg, diabetes, obesity), are actually pre-ventable.
“Many of our projects right now are really focused on disease prevention,” Jasul said. These diseases are not only problems in en-docrinology, but are considered public health concerns as well. “We need to have concrete and multi-disciplinary approach to the prob-
Dr. Gabriel JasulImmediate Past PresidentPhilippine Society of Endocrinologyand Metabolism
Phot
o co
urte
sy o
f NG
P In
tegr
ated
Mar
ketin
g C
omm
unic
atio
ns

25 May 2012 Philippine Focuslem. Otherwise the problem will be worse 50 years from now.”
A number of advocacy programs by PSEM are geared towards awareness campaigns, which are done through training of health workers, distribution of educational materi-als and lay workshops. These programs are usually done in partnership with government agencies, non-governmental organizations, private companies and other specialty societ-ies.
PSEM initiated the Hawak Kamay Laban sa Diabetes Train-the-Trainors workshops to train barangay health workers (BHW), which help these health volunteers understand dia-betes, even improving their skills on how to prevent it and how to screen patients. Train-the-Trainors courses were held in Manila and Laoag, involving hundreds of BHWs.
The Hawak Kamay Diabetes Academy on Air, in collaboration with DZMM Teleradyo, ABS-CBN Foundation and Merck Sharp and Dohme (MSD), is a weekly 15-minute radio program with the same objective of diabetes awareness and prevention as the Train-the-
Trainors workshops. Various topics on diabe-tes are discussed by PSEM volunteers, with a short question and answer portion to extend diabetes education to more patients.
PSEM has also prepared e-modules, or dig-ital aids containing educational information on diabetes, through the National Telehealth Center of the University of the Philippines-Manila, to reach health workers in far-flung areas.
Lay fora on other conditions such as thy-roid diseases, cholesterol problems, osteopo-rosis and obesity are regularly conducted by PSEM in different parts of the country. Ac-cording to Jasul, whenever they hold week-end courses for medical professionals and health volunteers, they do simultaneous lay fora for the patients and their families. In a year, at least four weekend courses are con-ducted by the society, with each course cover-ing one of the four major topics that include general endocrinology, diabetes, lipid imbal-ances and thyroid problems.
Being active with the advocacy program is the kind of mark that Jasul wanted to leave during his term, and one of the thrusts that PSEM is hoping to continue.
“I think the best patient really is the edu-cated patient,” he said.
“Compliance is always a big problem in many chronic diseases, and we are dealing with not only diabetes, but also thyroid dis-ease, obesity. So, to be able to get the patient to cooperate and to comply, you really need to make sure that they are well-educated about their disease,” Jasul concluded.
We need to have concrete and multi-
disciplinary approach to the problem. Otherwise the
problem will be worse 50 years from now.
‘‘

26 May 2012 Philippine Focus
Dr. Noel LagmanOutgoing PresidentPhilippine College of Emergency Medicine
A young specialty gains more ground
Mention emergency medicine, and one inevitably thinks of a chaotic and al-
most cinematic picture in emergency rooms, much like the American TV series appropri-ately entitled ER.
“Well, when we get trauma patients, stab wounds, gunshot wounds, it’s almost simi-lar. Minus the drama. But we also have our own little drama in (our own) ER,” admitted Dr. Noel Lagman, outgoing president of the Philippine College of Emergency Medicine (PCEM).
Considered as one of the most exhilarat-ing practices, emergency medicine or EM is
a relatively young field in the Philippines that started in the late 1980s. And even much younger is the field’s specialty society, PCEM. Only three years ago, in 2009, that the two separate emergency medicine societies—the Philippine College of Emergency Medicine and Acute Care (PCEMAC) and the Philip-pine Society of Emergency Care Physicians (PSECP)—merged to form a unified college, according to Lagman, who practices at Maka-ti Medical Center.
Within a few years, PCEM was able to standardize its by-laws, establish a board to oversee specialty training and set up annual conventions, while balancing the interest of the two original groups. To further enhance local practice, PCEM intends to become part of regional and international societies for emergency medicine, which would give EM doctors the opportunity to attend larger con-ferences and conventions.
“It would give us more learning. More studies and more understanding on how EM should work, especially in the Philippines. There are lot of new technologies that we don’t have yet,” said Lagman.
As a relatively young field, Lagman admit-ted that the society is facing serious challeng-es. And one of them is dealing with patients.
“The concept of what an emergency is, [this] is not yet really understood by all the
NOTES ON LEADERSHIP
The Medical Tribune’s Dr. Yves Saint James Aquino talks to presidents of specialty societies to discuss their roles in promoting their respective fields
27 May 2012 Philippine Focuspeople. When the Filipino people think that, for example, when they have fever for only a few hours, they think that it’s an emergency and that they really have to go to the ER,” said Lagman.
It is important for Filipinos to understand that EM doctors need to prioritize which pa-tients should be seen first, he added.
But the problem is not just the patients, even colleagues in the profession is a chal-lenge.
training (institutions) in their provinces,” said Lagman.
The exhilarating, fast-paced practice of emergency care is the typical reason why doc-tors enter the specialty, but for Lagman, who originally wanted to become a surgeon like his father, the reason was more personal.
“When my father got sick ... he had a cardio-respiratory arrest at home, and I had to resus-citate him there in the garage and bring him to the hospital,” Lagman shared. With only interns and no resident or consultant meeting them at the ER, he ended up performing CPR on and intubating his own father.
The passion that he discovered 16 years ago still remains, he said, especially when he en-counters challenging cases such as acute MI, gunshot wounds and other types of trauma patients.
“You have to think fast. You have to decide fast when to refer, and when to bring the pa-tient up to the OR. That’s the most exciting thing about emergency medicine,” Lagman shared.
‘‘ The concept of what an
emergency is, [this] is not
yet really understood by
all the people.
“Because it’s fairly new, some other doc-tors, especially the old doctors, really don’t understand what emergency medicine is. They think that we’re trying to get into their practice, but we’re not,” clarified Lagman. He explained that the practice of EM doctors re-main within the confines of the ER. Clinical practice guidelines are being developed in or-der to “know where to end our practice and when to refer to other doctors. ... We will have to refer the patients back to them, of course.”
Besides the older generation of doctors, the society also has to deal with pursuing the younger generation to have more medical graduates enter the specialty. Most of the ac-credited training institutions are in Metro Ma-nila, and PCEM is planning to expand accredi-tation to include hospitals in other provinces.
“We’re training doctors from the provinces and then sending them back to open up those
28 May 2012 Philippine FocusMARKET WATCH
Unilab’s LRI and Therapharma merge
LRI and Therapharma, two of the biggest divisions of United Laboratories, announced their official merging last February 21,
2012, in the presence of luminaries from the medical community. LRI-Therapharma’s combined experience in cardiovascular and
metabolic treatments paved the way to the company’s Triumvirate of Stroke Management, which includes Plogrel (Clopidogrel bisulfate), Trombocil (Cilostazol) and Aspilet (Aspirin).
Plogrel is indicated for the prevention of atherosclerotic events in patients with history of recent myocardial infarction (within a few days until <35 days from occurrence), recent ischemic stroke (from 7 days until <6 months) or established peripheral arterial disease.
Trombocil is indicated for the treatment of ischemic symptoms eg ulcer, pain and coldness of extremities in chronic arterial occlusion. Also for prevention of recurrence of cerebral infarction except car-diogenic cerebral embolism.
Aspilet is indicated for suspected acute MI, and for prophylactic treatment of thromboembolic disorders, MI, transient ischemic at-tacks and stroke.
Pfizer launches pneumococcal vaccine for adults
Representatives from Pfizer during the launch
Pfizer Inc. has officially launched in the Philippines its vaccine
for adults aged 50 years old and above against pneumonia, the lead-ing cause of morbidity and the fifth leading cause of mortality in our country. Filipinos aged 50 years old and above account for 88 percent of deaths due to pneumonia.
“Often, pneumococcal disease attacks individuals with compromised immune systems and these are usually adults who are already suffering from other conditions,” said Dr. Rontgene Solante, president of the Philippine Society of Microbiology and Infectious Diseases.
The pneumococcal vaccine of Pfizer has been available in the country since 2010 for use in children ages 2 to 5 years old and is now approved for adults 50 years old and above in the Philippines since November 2011. The adult indication was approved by the European Medi-cines Agency last October 2011 and the US Food and Drug Administration last December 2011.

29 May 2012 Philippine FocusMARKET WATCH
MSD promotes better diabetes management with breakthrough medicine
Merck Sharp & Dohme (MSD), a global healthcare lead-er that provides medicines, vaccines, biologic therapies
and consumer care products, promoted better management of diabetes by discussing dipeptidyl peptidase-4 inhibitors, one of the latest drugs for diabetes.
One of guest speakers, Dr. Daniel Drucker, senior scientist with Samuel Lunenfeld Research Institute in Mt. Sinai Hospi-tal, Toronto, discussed the science behind DPP-4, as well as its efficacy and safety profile.
Drucker has been involved in studies on incretin-based therapies, to which DPP-4 inhibitors belong, that are now widely used for the treatment of type 2 diabetes.
“For the first time in the management of diabetes, we are able to use medications that do not produce hypoglycemia or a low blood sugar as a side-effect, and do not cause weight-gain,” said Drucker.
Drucker also explained that the new drugs are the easiest drugs to prescribe. “They can be taken once a day, and there are once weekly versions in development,” he said.
Dr. Daniel Drucker
Invida introduces new anti-aging skin care range
Invida recently launched the Kinerase® Skin Care System, which utilizes kine-
tin, a potent bio-growth factor derived from plants. The skin care line was devel-oped by Canada-based Valeant Pharma-ceuticals, a multinational specialty com-pany.
“Our almost three decades of research has shown that kinetin exerts powerful effects in de-laying several signs of skin aging,” said Prof. Suresh Rattan, a noted biogerontologist, during the media launch held last March 2012 in Bonifacia Global City, Taguig.
Rattan, currently the head of the Laboratory of Cellular Aging, Depart-ment of Molecular biology, Aarhus University, Denmark, is considered the “Father of Kinetin” as he holds the sole inventorship for discovering the anti-aging effects of kinetin in human skin cells.
“We are pleased to make the Kinerase® Skin Care System available to Filipino dermatolo-gists and their patients,” said Dr. Maaliddin Biruar, medical and scientific affairs director of Invida Philippines.
30 May 2012 Philippine FocusMARKET WATCH
Aspen, Africa’s largest pharmaceutical manufacturer, opened its local subsidiary in the Philippines, aiming to
make high-quality branded medicines available to Filipino patients at affordable cost.
“We take great pride in formally opening our office in the Philippines. This business initiative forms part of Aspen’s state global expansion strategy into emerging and established markets, and we look forward to working closely with the Philip-pine government and local regulatory bodies in providing quality products to meet the health-care needs of the Filipino people,” said Mr. Stephen Saad, Aspen Group Chief Executive.
Aspen has 18 manufacturing facilities in 13 pharmaceutical manufacturing sites on six con-tinents. Four of the sites are located in Sout Africa, four in Australia, and one each in Kenya, Tanzania, Brazil, Mexico and Germany.
Aspen Philippines commenced operations in January 2012 with only four employees, but after two months, the staff complement has increased to nearly 100 Filipinos.
“We are honored and grateful that Aspen chose to establish its first Asian subsidiary in the Philippines. Our partnership with a global pharmaceutical leader not only makes medicines of superior quality with prices that are within means available to Filipino patients, it also pro-vides employment to local talents,” said Ms. Ace Itchon, President and CEO of Aspen Philip-pines, Inc.
Aspen brings quality, affordable drugs to the Philippines
Eli Lilly and Company and the Philippine Society of
Endocrinology and Metabo-lism (PSEM) awarded insulin medication for life to selected recipients during the society’s annual convention held in EDSA Shangri-La Hotel.
Patients that are eligible for medical support must be Fili-pino citizens, have no private or public prescription cover-age, and must be earning an amount within the program guidelines. Patients must be nominated by a PSEM member.
Insulin vials and syringes will be delivered or dispensed directly to patients by their physi-cians.
“Insulin for Life” awarded during PSEM convention
Photo shows (from left) Dr. Levy Jasul, PSEM immediate past president; Dr. Rosa Allyn Sy, project chair of Insulin for life; recipeint Cecilia Dela Queva; and Dr. Cecille Añonuevo-Cruz.
31 May 2012 News
Bergamot orange a natural supplement for cholesterol control
Rajesh Kumar
An Australian cardiologist has found a natural ally in his fight against metabolic dis-orders – an extract of the bergamot orange, an Italian citrus fruit which has long been be-lieved to possess heart health benefits.
Dr. Ross Walker, who runs a private prac-tice in Sydney, said he has successfully used the extract in about 700 of his registered pa-tients who are overweight with dyslipidemia and elevated blood sugar levels.
Within a few weeks of starting the supple-ment, some of those patients have totally avoided the need for statins while others have reduced their statin dose to control dys-lipidemia. As a bonus outcome, their blood glucose and middle obesity have also signifi-cantly reduced, said Walker.
His findings are consistent with those of an unpublished clinical study conducted in Italy involving more than 200 patients with hyperlipidemia. In the study, 1 month’s sup-plementation with bergamot reduced LDL cholesterol by 39 percent and blood sugar by 22 percent, and raised HDL cholesterol by 41 percent.
“Bergamot contains extremely large amounts of polyphenols, as compared to other citrus species. Two of these, Brutelidin and Metilidin, directly inhibit cholesterol bio-synthesis in a similar way to statins and they are not found in any other citrus derivatives,” said lead study author Dr. Vincenzo Mollace, professor in the faculty of pharmacology at the University of Cantanzaro in Italy.
Bergamot extract blocks the HMG CoA reductase enzyme at a different level than statins. As a result, myalgia and other side ef-fects typically associated with statins can be avoided because bergamot does not block the component that depletes the muscular co-en-zyme q10, said Walker.
“Bergamot extract (BergametTM) also in-hibits cholesterol absorption in the gut, the same way plant sterols do. That’s why I ask my patients to take it 15 minutes before meal twice a day, in the afternoons and evenings, to block cholesterol absorption from food,” he said.
“The unique and most important action of bergamot, due to which cardiologists (like me) are supporting this, is that it affects meta-bolic syndrome as a whole: raising HDL cho-lesterol, lowering LDL and blood sugar and reducing arterial stiffness and middle obesity.”
Could patients be advised to consume ber-gamot juice as part of a healthy diet to prevent metabolic syndrome, rather than taking its extract in a pill form? Walker said it is not that easy since bergamot orange is extremely bit-ter/sour and large amounts of its juice would be needed to get the desired benefit.
“[Bergamot extract] is not a replacement for statins. Patients who have had a heart at-tack or have vascular disease do need to take statins. [But] the extract can be useful in pre-venting metabolic syndrome, correcting it in early stages and as a supplement to reduce statin dose,” he said.

32 May 2012 News
Omega-3 fatty acids help slow aging of the brainRajesh Kumar
The status of omega-3 fatty acids as ‘brain food’ is well established. However, re-
search now suggests a diet lacking in these fatty acids may cause brain to age faster and lose some of its memory and thinking abilities.
The finding has prompted a study author to recommend that physicians should remind patients to regularly consume fatty fish or other food sources of omega-3 as part of a bal-anced diet.
“[In the study] people with lower blood levels of omega-3 fatty acids had lower brain volumes that were equivalent to about 2 years of structural brain aging,” said lead research-er Dr. Zaldy Tan of the Easton Center for Al-zheimer’s disease research and the division of geriatrics at the University of California at Los Angeles, California, US.
A total of 1,575 people with an average age of 67 and free of dementia underwent MRI brain scans for the study. They were also giv-en tests that measured mental function, body mass and omega-3 fatty acid (comprising doc-osahexaenoic acid or DHA, and eicosapentae-noic acid, EPA) levels in their red blood cells. [Neurology 2012;78: 658-664].
Fatty acid composition of red blood cells (RBC) reflects dietary fatty acid intake aver-aged over the RBC lifespan of up to 120 days, whereas plasma concentrations reflect intake over only the last few days.
The researchers found that people whose
DHA levels were among the bottom 25 percent of the participants had lower brain volume compared to people who had higher DHA levels. Similarly, participants with levels of all omega-3 fatty acids in the bottom 25 percent also scored lower on tests of visual memory and executive function, such as problem solv-ing and multi-tasking and abstract thinking.
“Lower DHA levels are associated with smaller brain volumes and a ‘vascular’ pat-tern of cognitive impairment, even in persons free of clinical dementia,” concluded the re-searchers.
It may be premature for physicians to advise their patients to consume adequate amounts of food rich in omega-3 specifically for their brain health, without evidence from a large randomized control trial. But Tan said there is already ample evidence supporting the benefits of this fatty acid in cardiovascular and overall health and such an advice could only be beneficial.
The regular consumption of fatty fish or other food sources of omega-3 fatty acids is well known to be part of a balanced diet.
33 May 2012 News
participants’ vestibular function, a measure of how well they kept their balance. They found that people with a 25-decibel hearing loss, clas-sified as mild, were nearly three times more likely to have a history of falling. Every addi-tional 10-decibels of hearing loss increased the chances of falling by 1.4 fold (95% CI, 1.3-1.5).
Even mild hearing loss increases risk of fallingRajesh Kumar
Adults aged 60 and older should be rou-tinely screened for hearing loss and
treated according to best practice guidelines, according to Dr. Frank Lin, assistant professor of otolaryngology at the Johns Hopkins Uni-versity School of Medicine and Bloomberg School of Public Health in Baltimore, Mary-land, US.
The advice follows research findings that link even mild hearing loss to a three-fold risk of falls. Hearing loss among the elderly is al-ready associated with a range of social and cognitive problems, including dementia. But the researchers feel the latest finding could help in the development of new ways to pre-vent falls and resulting injuries that cost bil-lions of dollars in health care.
“We still do not know if treating hearing loss can reduce falls. But hearing loss treat-ment entails no risks and could potentially only lead to benefits for cognitive, social and physical functioning,” said Lin, adding that hearing loss was only one of many potential risk factors for falls.
To determine whether hearing loss and falling are connected, Lin and colleagues used data from the 2001 to 2004 cycles of the US National Health and Nutrition Examination Survey. A total of 2,017 participants aged 40 to 69 had their hearing tested and answered questions about whether they had fallen over the past year. [Arch Intern Med 2012;172:369-371]
They also collected demographic informa-tion, including age, sex and race, and tested
The finding held true even when research-ers accounted for other factors linked with falling, including age, sex, race, cardiovascu-lar disease and vestibular function. Excluding participants with moderate to severe hearing loss from the analysis also didn’t change the results.
Among the possible explanations for the link is that people who can’t hear well might not have good awareness of their overall en-vironment, making tripping and falling more likely, said Lin.
Another reason hearing loss might increase the risk of falls is cognitive load, in which the brain is overwhelmed with demands on its limited resources.
“Gait and balance are things most people take for granted, but they are actually very cognitively demanding. If hearing loss imposes a cognitive load, there may be fewer cognitive resources to help with maintaining balance and gait,” he said.
Gait and balance are ...
actually very cognitively
demanding
‘‘
34 Industry UpdateRole of heart rate, sympathetic activity in CVDCompelling evidence from experimental and clinical studies links elevated heart rate with higher risk of cardiovascular events in patients with coronary artery disease and chronic heart failure. At a recent cardiology symposium sponsored by Merck Serono, three experts discussed the role of heart rate and sympathetic activity in the development of CVD as well as the sympatho-inhibitory and cardioprotective effects of selective beta-blockers, in particular bisoprolol (Concor®).
The cardiovascular continuumThe cardiovascular disease (CVD) continuum
frames CVD as a chain of events initiated by a number of risk factors leading to the end stage of the disease. [Circulation 2006;114:2850-2870]. It continues as a pathophysiologic process last-ing for decades. It is essential that cardioprotec-tion at each stage is provided to the patient.
Hypertension is one of the earliest and most important risk factors in the CV continuum and its effective control is now recognized as a pre-requisite for strategies for the prevention of stroke, coronary events and heart failure.
Adrenergic neural factors may participate in the development and progression of the hyper-tensive state and its complications. This repre-sents the rationale for the use of antihyperten-sive drugs with sympatho-inhibitory effects. [Am J Hypertension 2010; 23:1052-1060]
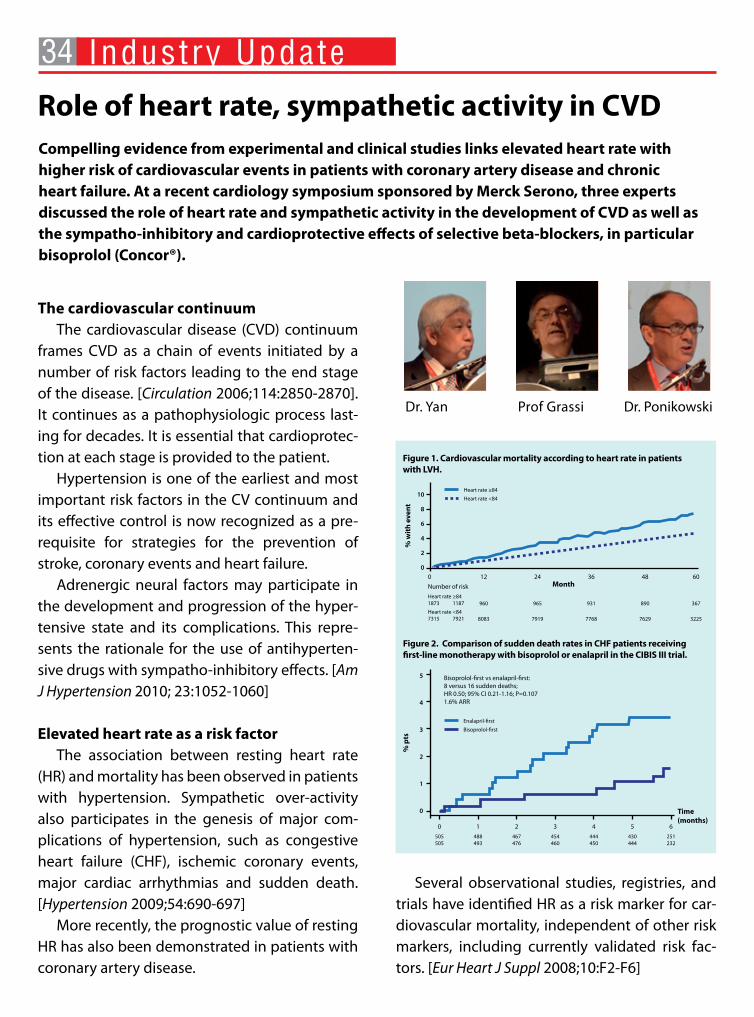
Elevated heart rate as a risk factorThe association between resting heart rate
(HR) and mortality has been observed in patients with hypertension. Sympathetic over-activity also participates in the genesis of major com-plications of hypertension, such as congestive heart failure (CHF), ischemic coronary events, major cardiac arrhythmias and sudden death. [Hypertension 2009;54:690-697]
More recently, the prognostic value of resting HR has also been demonstrated in patients with coronary artery disease.
Several observational studies, registries, and trials have identified HR as a risk marker for car-diovascular mortality, independent of other risk markers, including currently validated risk fac-tors. [Eur Heart J Suppl 2008;10:F2-F6]
Dr. Ponikowski Prof GrassiDr. Yan
10
8
6
4
2
0
Heart rate ≥84
Heart rate <84
% w
ith
eve
nt
0
Number of risk
Heart rate ≥841873 1187
Heart rate <847315 7921
12
960
8083
24
965
7919
36
931
7768
48
890
7629
60
367
3225
Month
Figure 1. Cardiovascular mortality according to heart rate in patients with LVH.
5
4
3
2
1
0 Time (months)
% p
ts
Bisoprolol-first vs enalapril-first:8 versus 16 sudden deaths;HR 0.50; 95% CI 0.21-1.16; P=0.1071.6% ARR
Enalapril-first
Bisoprolol-first
0
505505
1
488493
2
467476
3
454460
4
444450
5
430444
6
251232
Figure 2. Comparison of sudden death rates in CHF patients receiving first-line monotherapy with bisoprolol or enalapril in the CIBIS III trial.

35 Industry UpdateConsequently, HR is included in some risk as-
sessment models for patients after acute coro-nary syndrome or post-myocardial infarction (MI). [Eur Heart J Suppl 2008;10:F11-F16; J Am Coll Cardiol 2009;54:1154-61]
A study by Okin et al. showed that every 10 bpm higher HR on in-treatment ECGs in hyper-tensive patients was associated with a 16 per-cent increase in adjusted risk of CV mortality and with persistence or development of a HR ≥84 was associated with a 55 percent greater risk of CV death. (Figure 1). [Eur Heart J 2010;31:2271-2279] In terms of all-cause mortality, increments of 10 bpm in this sample of patients was associ-ated with a 25 percent greater risk, while HR ≥84 persistence or development was associated with a 79 percent greater adjusted risk.
Sympathetic over-activity represents a hall-mark of the hypertensive state. Pronounced in-fluence of the autonomic imbalance on cardio-vascular morbidity and mortality is not simply a function of hemodynamic effects. Recent stud-ies have revealed that a major determinant of the pathological process results from autonomic dysregulation of the inflammatory/immune sys-tem. [Hypertension 2012;59:755-762]
Role of beta-blockers in CVDThere is strong evidence to support the the-
ory that beta-blockers positively interfere with neuroadrenergic function.
Analyses of randomized clinical trials of be-
ta-blockers suggest that the beneficial effect of these agents in reducing total mortality and sud-den cardiac death after MI is proportionally re-lated to their ability to reduce resting HR.
‘‘ If HR is a risk factor for hypertension, it would follow that reduction in HR would improve clinical outcomes
Dr. Peter Yan Cardiologist at Peter Yan Cardiology Clinic,
Gleneagles Medical Centre, Singapore
‘‘ An ideal CV drug should
possess sympathomodulatory
and cardioprotective propertiesProfessor Guido Grassi
Professor of internal medicine in the department of clinical medicine at
San Gerardo Hospital, Universita Milano Becocca, Milan, Italy
A statistically significant relationship was found between resting HR reduction and reduc-tion in cardiac deaths and nonfatal MI recur-rence. [Eur Heart J 2007;28:3012-3019; Am J Car-diol 2008;101:865-869] Therefore, beta-blockers may play an important role in HR reduction in the CVD continuum.
HR reducing effects of bisoprololCardiac events are the leading cause of late
morbidity and mortality after successful major vascular surgery. After peripheral bypass surgery, for example, 3-year mortality is approximately 30-40 percent.
‘‘ There is no doubt that HR
reduction is closely linked with
improvement in mortalityDr. Piotr Ponikowski
Medical University, Centre for Heart Disease, Clinical Military Hospital, Wroclow, Poland
Peri-operative and long-term post-operative bisoprolol administration produces a 3-fold re-duction in late cardiac death and MI rates among high-risk patients after successful major noncar-diac vascular surgery.

36 Industry UpdateThe results of the CIBIS (Cardiac Insufficien-
cy Bisoprolol) II trial showed that patients with heart failure in sinus rhythm with the initial low-est HR and the greatest HR reduction with time (2 months) will have the best prognosis. Beta-blockade with bisoprolol further improves sur-vival at any level of basal HR to a similar extent. [Circulation 2001;103:1428-1433]
When bisoprolol, carvedilol and nebivolol were compared directly, HR at exercise was de-creased at 3 hours following intake of the first single dose of each drug by bisoprolol (-24 per-cent), carvedilol (-17 percent) and nebivolol (-15 percent). [Cardiology 2006;106:199-206]
The results of the CIBIS-ELD (in elderly) study showed that the selective β1-adrenoceptor-blocker bisoprolol was associated with a greater reduction in HR than carvedilol. [Eur J Heart Fail 2011;13:670-680]
In comparison with other antihypertensive agents, bisoprolol frequently proved to be more effective or better tolerated. [J Cardiovasc Pharma-col 1986; 8:S122-127]
Bisoprolol in congestive heart failureSudden death is the most prevalent cause of
death in the early course of CHF. When bisoprolol was compared to enalapril (CIBIS III trial) bisopro-lol was found to be non-inferior to enalapril and at least as important as ACE inhibitors in patients with CHF (Figure 2). [Eur Heart J 2006; 8: C43-C50]
A bisoprolol-first strategy reduced mortality by 31 percent, compared with an enalapril-first strat-egy. The results support bisoprolol as a first-line treatment for CHF.
Recently, it was suggested that switching
from carvedilol to bisoprolol may help with con-tinuation of beta-blocker treatment as well as dosage increase in patients with heart failure who suffer adverse symptoms or signs, allowing them to reach the target dose. [J Am Coll Cardiol 2012;59:E885]
Atrial fibrillation (AF) occurs frequently soon after coronary artery bypass grafting (CABG) and often results in increased mortality and morbidity, particularly in patients with heart failure. Bisopro-lol is more effective than carvedilol in decreasing the incidence of post-discharge AF after CABG in patients with decreased left ventricular function. Greater effectiveness of bisoprolol could be relat-ed to its greater β1-receptor selectivity, imparting a greater degree of protection against increases in sympathetic activity. [Am J Cardiol 2011;107:215-219]
The pharmacokinetic properties of bisoprolol provide the prerequisite for a single daily dose and ensure an extremely low inter- and intra-in-dividual variability of the plasma concentration profiles. [J Cardiovasc Pharmacol 1986; 8:S16-20]
ConclusionsIt has been postulated that elevated heart
rate may become a therapeutic target in CV dis-eases, particularly in coronary artery disease and chronic heart failure. Beta-blockers reduce mor-bidity, mortality, and improve functional status in CHF patients, thus remaining a cornerstone of the pharmacological management of CHF. Bisoprolol is a highly cardioselective β-blocker. It is safe, ef-fective, and well tolerated. Due to its high β1 se-lectivity and pharmacokinetic profile, it confers reliable 24-hour efficacy and cardioprotection.

37 May 2012 Calendar
May
5th European Clinam Conference for Clinical Nanomedicine7/5/2012 to 9/5/2012Location: Basel, Switzerland Info: Clinam, European Foundation for Clinical NanomedicineTel: (11) 41 61 695 9395Fax: (11) 41 61 695 9390Email: [email protected] Website: www.clinam.org
19th European Congress on Obesity9/5/2012 to 12/5/2012Location: Lyon, FranceInfo: European Association for the Study of ObesityTel: (44) 20 8783 2256Fax: (44) 20 89796700Email: [email protected] Website: www.eco2012.org
American Thoracic Society International Conference 2012 18/5/2012 to 23/5/2012Location: San Francisco, California, US Tel: (1) 212 315 8652Email: [email protected] Website: www.thoracic.org/go/international-conference
American Society of Hypertension19/5/2012 to 22/5/2012Location: New York, New York, US Info: American Society of HypertensionTel: (1) 212 696 9099Fax: (1) 212 696 0711Email: [email protected] Website: www.ash-us.org/Scientific-Meetings/Future-Meet-ings.aspx
Digestive Diseases Week 201219/5/2012 to 22/5/2012Location: San Diego, California, US Info: American Society of Gastrointestinal EndoscopyTel: (1) 301 272 0022Fax: (1) 301 654 3978Email: nmurphy@gastro .org Website: www.ddw.org
19th WONCA Asia Pacific Regional Conference24/5/2012 to 27/5/2012Location: Jeju, Korea Tel: (82) 2 566 6031Email: [email protected] Website: www.woncaap2012.org
June
2012 American Society of Clinical Oncology Annual Meeting1/6/2012 to 5/6/2012Location: Chicago, Illinois, US Tel: (1) 571 483 1300Email: [email protected] Website: chicago2012.asco.org
10th Royal College of Obstetricians and Gynecologists International Scientific Congress5/6/2012 to 8/6/2012Location: Kuching, Malaysia Tel: (60) 3 6201 1858Email: [email protected] Website: www.rcog2012.com
15th International Congress of Infectious Diseases13/6/2012 to 16/6/2012Location: Bangkok, ThailandTel: (1) 617 277 0551Fax: (1) 617 278 9113Email: [email protected] Website: www.isid.org/icid
15th World Congress of Pain Clinicians27/6/2012 to 30/6/2012Location: Granada, SpainInfo: Kenes InternationalTel: (41) 22 908 0488 Fax: (41) 22 9069140Email: [email protected] Website: www.kenes.com/wspc
38 May 2012 Calendar
Upcoming
17th World Congress on Heart Disease 201227/7/2012 to 30/7/2012Location: Toronto, Ontario, CanadaInfo: International Academy of CardiologyTel: (1) 310 657 8777 Fax: (1) 310 659 4781 E-Mail: [email protected] Website: www.cardiologyonline.com
European Society of Cardiology Congress 201225/8/2012 to 29/8/2012Location: Munich, GermanyInfo: European Society of CardiologyTel: (33) 4 9294 7600 Fax: (33) 4 9294 7601 E-Mail: [email protected] Website: www.escardio.org/congresses/esc-2012
15th Biennial Meeting of the European Society for Immunodeficiencies (ESID 2012)3/10/2012 to 6/10/2012Location: Florence, ItalyTel: (41) 22 908 0488Fax: (41) 22 732 2850Email: [email protected]: www.kenes.com/esid
42nd Annual Meeting of the International Continence Society 15/10/2012 to 19/10/2012Location: Beijing, ChinaTel: (41) 22 908 0488Fax: (41) 22 906 9140Email: [email protected]: www.kenes.com/ics
World Allergy Organization International Scientific Conference (WISC 2012)6/12/2012 to 9/12/2012Location: Hyderabad, IndiaInfo: World Allergy OrganizationTel: (1) 414 276 1791Fax: (1) 414 276 3349E-mail: [email protected]: www.worldallergy.org


Publisher : Ben Yeo
Deputy Managing Editor : Greg Town
Senior Editor : Naomi Rodrig
Contributing Editors : Hardini Arivianti (Indonesia), Christina Lau (Hong Kong), Leonard Yap, Saras Ramiya, Pank Jit Sin, Malvinderjit Kaur Dhillon (Malaysia), Dr. Yves St. James Aquino (Philippines), Radha Chitale, Elvira Manzano, Rajesh Kumar (Singapore)
Publication Manager : Cliford Patrick
Designers : Nur Malathy, Charity Chan, Lisa Low, Donny Bagus, Joseph Nacpil
Production : Edwin Yu, Ho Wai Hung, Jasmine Chay
Circulation Executive : Christine Chok
Accounting Manager : Minty Kwan
Advertising Co-ordinator : Rachael Tan
Published by : UBM Medica Pacific Limited27th Floor, OTB Building, 160 Gloucester Road, Wanchai, Hong Kong Tel: (852) 2559 5888 Fax: (852) 2559 6910 Email: [email protected]
Advertising Enquiries:
China : Yang XuanTel: (8621) 6157 3888 Email: [email protected]
Hong Kong : Kristina Lo-Kurtz, Miranda Wong, Marisa Lam, Jacqueline Cheung Tel: (852) 2559 5888 Email: [email protected]
India : Monica BhatiaTel: (9180) 2349 4644 Email: [email protected]
Indonesia : Ritta Pamolango, Hafta Hasibuan, Sri Damayanti Tel: (6221) 729 2662 Email: [email protected]
Japan : Mamoru TakagiTel: (813) 5562 6961 Email: [email protected]
Korea : Kevin YiTel: (822) 3019 9350 Email: [email protected]
Malaysia : Irene Lee, Lee Pek Lian, Sumitra Pakry, Grace Yeoh Tel: (603) 7954 2910 Email: [email protected]
Philippines : Marian Chua, Julie Mariano, Philip KatipunanTel: (632) 886 0333 Email: [email protected]
Singapore : Jason Bernstein, Carrie Ong, Elijah Lee, Reem Soliman Tel: (65) 6223 3788 Email: [email protected]
Thailand : Wipa SriwijitchokTel: (662) 741 5354 Email: [email protected]
Vietnam : Nguyen Thi Lan Huong, Nguyen Thi My DungTel: (848) 3829 7923 Email: [email protected]
Europe/USA : Kristina Lo-KurtzTel: (852) 2116 4352 Email: [email protected], [email protected]
Medical Tribune is published 12 times a year (23 times in Malaysia) by UBM Medica, a division of United Business Media. Medical Tribune is on controlled circulation publication to medical practitioners in Asia. It is also available on subscription to members of allied professions. The price per annum is US$48 (surface mail) and US$60 (overseas airmail); back issues at US$5 per copy. Editorial matter published herein has been prepared by professional editorial staff. Views expressed are not necessarily those of UBM Medica. Although great effort has been made in compiling and check-ing the information given in this publication to ensure that it is accurate, the authors, the publisher and their servants or agents shall not be responsible or in any way liable for the continued currency of the information or for any errors, omissions or inaccuracies in this publication whether arising from negligence or otherwise howsoever, or for any consequences arising there-from. The inclusion or exclusion of any product does not mean that the publisher advocates or rejects its use either generally or in any particular field or fields. The information contained within should not be relied upon solely for final treatment decisions.
© 2012 UBM Medica. All rights reserved. No part of this publication may be reproduced in any language, stored in or introduced into a retrieval system, or transmitted, in any form or by any means (electronic, mechanical, pho-tocopying, recording or otherwise), without the written consent of the copy-right owner. Permission to reprint must be obtained from the publisher. Ad-vertisements are subject to editorial acceptance and have no influence on editorial content or presentation. UBM Medica does not guarantee, directly or indirectly, the quality or efficacy of any product or service described in the advertisements or other material which is commercial in nature.
Philippine edition: Entered as second class mail at the Makati Central Post Of-fice under Permit No. PS-326-01 NCR, dated 9 Feb 2001. Printed by Fortune Printing International Ltd, 3rd Floor, Chung On Industrial Bldg, 28 Lee Chung Street, Chai Wan, Hong Kong.
ISSN 1608-5086