Embed Size (px)
Citation preview

Medical student attitudes toward the doctor–patientrelationship
Paul Haidet,1,2 Joyce E Dains,3 Debora A Paterniti,4 Laura Hechtel,5 Tai Chang,3 Ellen Tseng3 & John CRogers3
Context Medical educators have emphasized the im-
portance of teaching patient-centred care.
Objectives To describe and quantify the attitudes of
medical students towards patient-centred care and to
examine: (a) the differences in these attitudes between
students in early and later years of medical school; and
(b) factors associated with patient-centred attitudes.
Methods We surveyed 673 students in the first, third,
and fourth years of medical school. Our survey utilized
the Patient–Practitioner Orientation Scale (PPOS), a
validated instrument designed to measure individual
preferences towards various aspects of the doctor–
patient relationship. Total PPOS scores can range from
patient-centred (egalitarian, whole person oriented)
to disease- or doctor-centred (paternalistic, less attuned
to psychosocial issues). Additional demographic data
including gender, age, ethnicity, undergraduate course-
work, family medical background and specialty choice
were collected from the fourth year class.
Results A total of 510 students (76%) completed data
collection. Female gender (P < 0Æ001) and earlier year
of medical school (P ¼ 0Æ03) were significantly
associated with patient-centred attitudes. Among
fourth year students (n ¼ 89), characteristics associ-
ated with more patient-centred attitudes included
female gender, European-American ethnicity, and pri-
mary-care career choice (P < 0Æ05 for each compar-
ison).
Conclusion Despite emphasis on the need for curricula
that foster patient-centred attitudes among medical
students, our data suggest that students in later years of
medical school have attitudes that are more doctor-
centred or paternalistic compared to students in earlier
years. Given the emphasis placed on patient satisfaction
and patient-centred care in the current medical envi-
ronment, our results warrant further research and
dialogue to explore the dynamics in medical education
that may foster or inhibit student attitudes toward
patient-centred care.
Keywords Attitude; curriculum; delivery of health care;
*doctor–patient relations; education, medical,
undergraduates, *methods; patient-centred care;
patient-centred satisfaction.
Medical Education 2002;36:568–574
Introduction
The doctor–patient relationship is central to the deliv-
ery of high quality medical care, and has been shown to
affect patient satisfaction and a variety of other biologi-
cal, psychological, and social outcomes.1 Patient-
centred care is one aspect of the doctor–patient
relationship that takes into account patients’ preferenc-
es, concerns, and emotions; it has been proposed as a
mechanism through which favourable patient outcomes
are achieved.2,3 In recent years, medical educators have
recognized the importance of patient-centred care by
instituting a variety of curricula to teach communica-
tion skills, professional values, and humanistic attitudes
and behaviours to medical students.4 However, a large
body of qualitative and ethnographic data exists to
suggest that the culture of medical education focuses
more on the biomedical mechanisms of disease than on
the issues central to patients’ preferences, concerns,
and emotions.5 Such a dynamic between school curri-
1Houston Veterans Affairs Medical Centre, Houston, Texas, USA,2Department of Medicine, Baylor College of Medicine, Houston,
Texas, USA, 3Department of Family and Community Medicine,
Baylor College of Medicine, Houston, Texas, USA, 4Department of
Medicine, University of California Davis School of Medicine,
Sacramento, California, USA, 5Department of Biology, Augustana
College, Rock Island, Illinois, USA
Correspondence: Paul Haidet MD MPH, Houston Veterans Affairs
Medical Centre, 2002 Holcombe Boulevard (152), Houston, Texas
77030, USA. Tel.: 00 1 713 794 8601; Fax: 00 1 713 748 7359;
E-mail: [email protected]
Learning to care
568 � Blackwell Science Ltd MEDICAL EDUCATION 2002;36:568–574

culum and culture may act as a barrier to educators’
attempts to promote patient-centred care. We conduc-
ted this study to describe and quantify student attitudes
towards the doctor–patient relationship and differences
in attitudes between students in early and later years of
medical school.
Methods
Study sample
We assessed student attitudes towards the doctor–
patient relationship among students in 2 consecutive
first-year classes (academic years 1997–98 and 1998–
99) and in the third- and fourth-year medical classes
(academic year 1998–99) at a large US medical school
(> 150 students per class). Our study institution has a
4-year curriculum divided into pre-clinical (first
18 months, mostly classroom-based) and clinical (fol-
lowing 30 months, mostly patient care- or ward-based)
curricula. Since no major curricular changes were made
at this institution during the tenure of each of these
student classes, all experienced essentially identical
curricula. We collected data on gender from all
students and additional demographic data from stu-
dents in the fourth-year class.
Gender and attitude data among first-year students
were collected as part of a first-year history and physical
examination course. Students completed an optional
survey during this course at the mid-point of the first
year. Data on attitudes and gender in third-year
students were collected throughout the 1998–99
academic year during a 4-week family medicine clerk-
ship. All students in our sample began clinical clerk-
ships in the 18th month of medical school (January of
the second year), so the third-year students in our study
had been exposed to a variety and number of clinical
rotations for at least 6 months before data collection.
Each third-year student completed a survey at the
beginning of their family medicine rotation.
In addition to data collected from first and third-year
students as part of pre-clinical or clinical coursework,
we administered an anonymous survey to fourth-year
students during a school-wide gathering in the autumn
of the 1998–99 academic year. This survey collected
information on student attitudes, gender, ethnicity, age,
medical specialty of interest, major field of undergra-
duate degree, type of undergraduate degree (BA versus
BS), extracurricular coursework during medical school
(such as music or language lessons), and first degree
family members in the medical professions. The med-
ical specialty of interest was classified as ‘primary care’
if students responded with internal medicine, paediat-
rics, or family and community medicine as their
specialty choice. The major field of undergraduate
degree was classified as science and technology-
oriented for undergraduate majors in science, engin-
eering, and other technology-oriented fields such as
computer science.
Measurement of student attitudes
Student attitudes toward the doctor–patient relation-
ship were measured using a previously validated
instrument.6 The Patient–Practitioner Orientation
Scale (PPOS) is an 18-item instrument originally
designed to be administered to either doctors or
patients. It measures an individual’s attitudes toward
the doctor–patient relationship along two dimensions
termed ‘sharing’ and ‘caring’, respectively. The sharing
dimension consists of 9 items that measure the degree
to which the respondent believes that power and
control should be shared between doctor and patient,
and the degree to which doctors should share informa-
tion with the patient. Examples of sharing items
include: ‘the doctor’s agenda is the one that should
direct the course of the medical interview’ and ‘often it
is in the patient’s best interests if he⁄she does not have a
full explanation of his⁄her medical condition’. The
caring dimension consists of nine items that measure
the extent to which the respondent cares about the
value of warmth and support in the relationship, and
the degree to which the respondent thinks the doctor
should inquire about psychosocial issues and employ a
holistic approach to medical care. Examples of caring
items include: ‘a good bedside manner is the most
important thing a doctor can bring to a sick patient’ and
‘to understand their patients, doctors must explore
relevant sources of stress in their patients’ lives’.
Key learning points
Despite calls for patient-centred care curricula, we
found attitudes among later-year students to be
significantly less patient-centred than attitudes
among students in earlier years of medical school.
Ethnic and gender differences in patient-centred
attitudes exist among medical students.
Ongoing dialogue in medical education should
focus on innovative strategies that challenge
students and teachers alike to critically examine
their own views toward the provision of patient
care.
Medical student attitudes • P Haidet et al. 569
� Blackwell Science Ltd MEDICAL EDUCATION 2002;36:568–574
Respondents were asked to rate their agreement or
disagreement with individual items on a 6-point scale.
The overall PPOS score was computed as the mean of
the scores for the 18 items. Sharing and caring scores
were computed as the mean of the scores for the nine
items in each dimension, respectively. For this study,
we calculated mean scores to range from a value of 1
( ¼ doctor-centred or paternalistic) to 6 ( ¼ patient-
centred or egalitarian).
Statistical analysis
We used factorial analysis of variance to examine the
effect of gender, year of medical school, and their
interaction on mean PPOS scores (overall PPOS, caring
subscore, sharing subscore). Since mean PPOS values
did not differ significantly between the two first-year
classes (academic years 1997–98 and 1998–99,
P ¼ 0Æ3, Student’s t-test) and since the addition of
the 1997–98 data did not alter the findings of our
analyses, we combined all first-year students’ data in
our reported results. We used linear regression to
examine associations between mean PPOS score and
month of data collection among third-year students.
For fourth-year students, we examined the relation-
ships between PPOS scores (overall PPOS, caring
subscore, sharing subscore) and demographic variables
using linear regression for age and Student’s t-test for
dichotomous variables.
Results
We identified 673 eligible students, of whom 510
(76%) completed the PPOS instrument. Distribution
of students by year and gender is shown in Table 1.
The average total PPOS score for the entire cohort was
4Æ57 (± 0Æ48 SD). Total PPOS scores ranged from 2Æ50
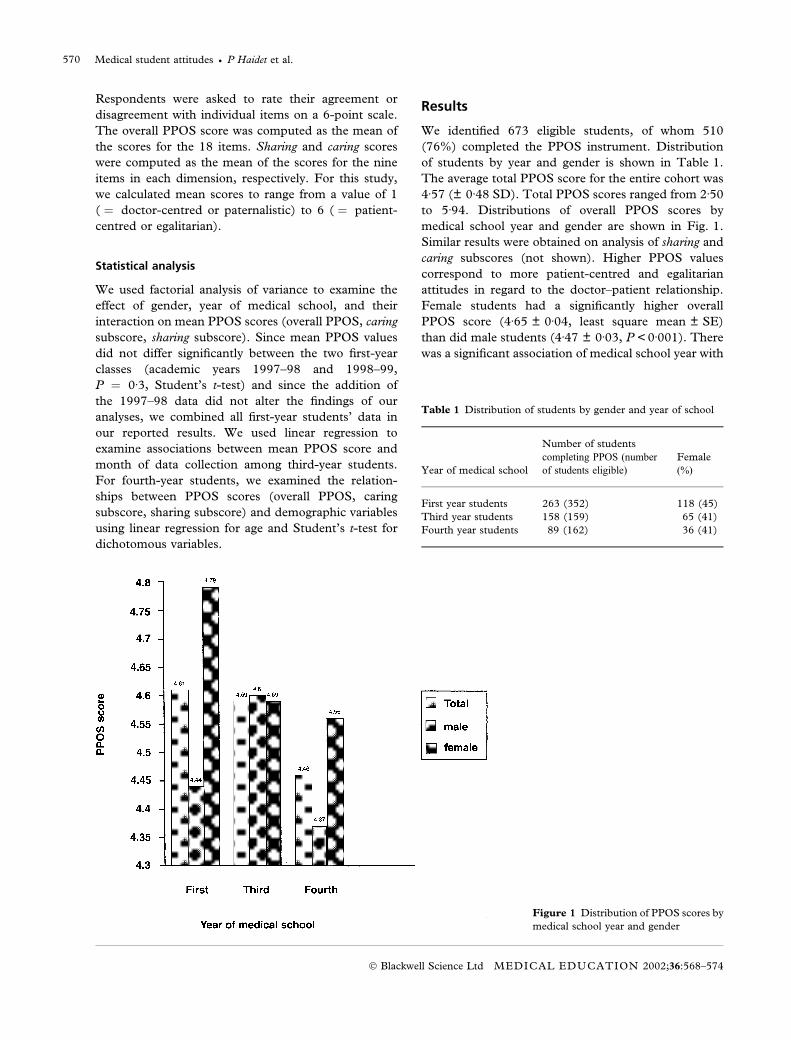
to 5Æ94. Distributions of overall PPOS scores by
medical school year and gender are shown in Fig. 1.
Similar results were obtained on analysis of sharing and
caring subscores (not shown). Higher PPOS values
correspond to more patient-centred and egalitarian
attitudes in regard to the doctor–patient relationship.
Female students had a significantly higher overall
PPOS score (4Æ65 ± 0Æ04, least square mean ± SE)
than did male students (4Æ47 ± 0Æ03, P < 0Æ001). There
was a significant association of medical school year with
Figure 1 Distribution of PPOS scores by
medical school year and gender
Table 1 Distribution of students by gender and year of school
Year of medical school
Number of students
completing PPOS (number
of students eligible)
Female
(%)
First year students 263 (352) 118 (45)
Third year students 158 (159) 65 (41)
Fourth year students 89 (162) 36 (41)
Medical student attitudes • P Haidet et al.570
� Blackwell Science Ltd MEDICAL EDUCATION 2002;36:568–574
PPOS score (P ¼ 0Æ03). The pattern of change in
PPOS scores across classes differed between females
and males. The average class scores for females
decreased with increasing years of school, while the
male classes demonstrated an increase followed by a
decrease in PPOS scores from the first- to the fourth-
year class. This interaction between gender and year of
medical school was statistically significant (P < 0Æ001).
Since the PPOS instrument was administered to
third-year students throughout the year during rotation
through a family medicine core clerkship, we analysed
the association between the month of the year in which
students completed the instrument and overall PPOS
score. The month of the year in this analysis reflects
that amount of experience in other clinical rotations
prior to the family medicine clerkship. While this
analysis did not show a statistically significant associ-
ation of the month of the year with PPOS scores, there
was a trend toward PPOS scores being progressively
more doctor-centred among students who completed
data collection later in their third year (P ¼ 0Æ07).
We collected additional demographic data in the
survey that we administered to fourth-year students.
These data are detailed in Table 2. Among the non-
European-American students, 63% identified their
ethnicity as Asian, 23% identified their ethnicity as
Hispanic, and 9% identified their ethnicity as African.
Three demographic variables had significant associ-
ations with overall PPOS scores in fourth-year students.
These data are shown in Table 3. Female students,
students who reported their ethnicity as European-
American, and students who reported a primary care
specialty choice demonstrated significantly more
patient-centred scores than students who were male,
of non-European-American ethnicity, or reported non-
primary care specialty career choices (P < 0Æ05 for each
comparison). Age, educational background, extracurri-
cular coursework, and family background did not show
significant associations with PPOS scores. Slight trends
were seen toward higher (more patient-centred) scores
in students who reported non-science and technology
majors and students who reported extracurricular
activities, but they were not statistically significant
(P ¼ 0Æ16, P ¼ 0Æ11, respectively). Analysis of shar-
ing subscale scores revealed additional associations with
demographic variables. Higher sharing scores indicate a
greater belief in shared power between doctor and
patient and in the doctor’s sharing of information with
the patient. Females, European-American students,
students choosing primary care specialties, students
who reported non-science and technology majors and
students who reported extracurricular activities had
higher sharing scores (P < 0Æ05 for each comparison).
The type of undergraduate degree, advanced degrees,
age, and family background were not significantly
associated with sharing scores.
Discussion
Despite the emphasis placed by medical educators,
health care administrators, and practising doctors on
the importance of curricula that foster patient-centred
attitudes among medical students,7 our data suggest
that the attitudes of students in the later years of
medical school are more doctor-centred or paternalis-
tic than those of students in earlier years. Doctor-
centred attitudes have been shown to be associated
Table 2 Demographic characteristics of fourth-year students
(n ¼ 89)
Characteristic n (%)
Primary care specialty choice 44 (49)
European-American ethnicity 45 (51)
BS undergraduate degree 46 (52)
Science and technology undergraduate major 55 (62)
Advanced degrees (Masters, PhD or equivalent) 10 (11)
Extracurricular activities 28 (31)
Family members in the medical professions 45 (44)
Mean age (SD) 25 (2Æ3)
Table 3 Total and subscale PPOS scores via demographic in
fourth-year students*
Demographic
variable Total PPOS Caring Sharing
Gender: female
(male)
4Æ57 (4Æ37)� 4Æ51 (4Æ43) 4Æ62 (4Æ31)�
Ethnicity: European-
American
(non-Euro-American)
4Æ57 (4Æ32)� 4Æ55 (4Æ38)� 4Æ59 (4Æ28)�
Specialty choice:
primary care
(non-primary care)
4Æ56 (4Æ34)� 4Æ55 (4Æ39)� 4Æ56 (4Æ30)�
College major:
non-science (science)
4Æ53 (4Æ40)� 4Æ47 (4Æ46) 4Æ59 (4Æ33)�
Extracurricular
activity: yes (no)
4Æ56 (4Æ40)§ 4Æ49 (4Æ45) 4Æ63 (4Æ34)�
College degree:
BA (BS)
4Æ42 (4Æ47) 4Æ44 (4Æ49) 4Æ40 (4Æ46)
Family in the
medical profession:
yes (no)
4Æ44 (4Æ45) 4Æ45 (4Æ48) 4Æ43 (4Æ42)
* All scores are mean scores, n ¼ 89.
� P < 0Æ05, Student’s t-test. � P ¼ 0Æ16, Student’s t-test.
§ P ¼ 0Æ11, Student’s t-test.
Medical student attitudes • P Haidet et al. 571
� Blackwell Science Ltd MEDICAL EDUCATION 2002;36:568–574

with lower patient satisfaction8 and may contribute to
decreased trust in the doctor–patient relationship. The
doctor-centred attitudes among senior students that
this study demonstrates may be associated with a
decline in senior students’ patient-centred behaviours
that others have observed.9 Medical sociologists and
anthropologists suggest that methods for managing
work, mistakes and emotions, in addition to the
language and manner of presentation that students
acquire during their training, direct students away
from patient-centred patterns of interactions in both
peer groups and with patients.5,10–12 These data sug-
gest that the culture of medicine and the structure of
medical education erode patient-centred attitudes in
spite of the international movement toward patient
satisfaction and patient-centred care. Unfortunately,
the influence of socialization on the practice of
medicine is difficult to mediate with curricular inter-
ventions alone. Medical educators have noted that
interventions timed during the pre-clinical years and
intended to foster patient-centred attitudes and behav-
iours are often overshadowed by the powerful experi-
ences of the clinical years as embodied in the informal,
or ‘hidden’ curriculum.5 Our data would support this
observation, since third-year students demonstrated a
progressive trend toward doctor-centred attitudes as
successive cohorts completed the PPOS during the
course of this initial clinical year. In order to be
maximally effective, we believe that educational inter-
ventions intended to foster patient-centred attitudes
and behaviours must occur during the clinical years
and must counter-balance the experiences embodied in
the ‘hidden’ curriculum that foster the opposite.
Ideally, patient-centred attitudes should be nurtured
in the setting of patient care through active learning
approaches and strong patient-centred role-modelling
by respected attending doctors.13
The differences we observed in student attitudes
between the first-, third-, and fourth-year classes
demonstrated different patterns according to gender.
While the average class scores for female students
were less patient-centred in later years of school, the
scores among males were most patient-centred
during the third year. Early ethnographic research
on medical students shows that students enter
medical school with a high degree of idealism, which
declines during the first 2 years of their education
and increases at the start of their clinical years when
students begin to see more patients.14 To the extent
that the construct of ‘patient-centredness’ as meas-
ured by the PPOS aligns with ‘idealism’ as observed
in this early research, our quantitative results among
males (the gender about which early ethnographic
accounts were written) seem to corroborate this
qualitative finding.
In a previous study, freshman female medical stu-
dents were shown to have more patient-centred atti-
tudes than male students.15 Our present study shows
that this difference between female and male students
exists in the fourth year of medical school as well. This
difference in attitudes may be linked to demonstrated
differences in gendered patterns of communication
among male and female doctors.16 It has been sugges-
ted that the patient-centred communication pattern
employed by women doctors may account for demon-
strated differences according to gender of doctor in a
diverse array of patient outcomes, including satisfaction
and provision of preventive services such as hormone
replacement therapy.17 Further study and understand-
ing of the nature and development of this gender
difference in attitudes toward the doctor–patient rela-
tionship may significantly inform efforts to eliminate
disparities by gender in the provision of high quality
medical care.
In this study, we demonstrated a strong association
between student ethnicity and patient-centred atti-
tudes. We hypothesize that this observation can be
explained by cultural differences in students’ views of
the ‘ideal’ doctor–patient relationship. For example, the
majority of non-European-American students in our
sample identified themselves to be of Asian ancestry.
Others have noted that the fundamental nature of the
doctor–patient relationship in terms of power-sharing
and holistic care tends to vary among cultures, and that
social norms in certain Asian cultures tend to favour a
more doctor-centred relationship.18 We hypothesize
that students enter medical school with their own
specific views of the ‘ideal’ doctor–patient relationship,
views that are shaped by diverse factors, including
social and cultural norms, gender, past experience as
patients, and portrayals of doctors in various mass
media. These ‘baseline’ impressions of the doctor–
patient relationship may be especially important in
determining students’ attitudes toward patient-centred
care upon graduation from medical school. We argue
that a critical developmental task for student doctors is
to develop awareness and understanding of the back-
ground of their own views toward patient-centred care.
Since ethnic differences between doctors and patients
are often barriers to partnership and communication in
the doctor–patient relationship, such an awareness may
help students to manage the relational dynamics
between themselves and patients of different ethnicity
more effectively. In addition, awareness of personal
views and biases has been proposed as an essential
ingredient for high quality patient care and teaching.19
Medical student attitudes • P Haidet et al.572
� Blackwell Science Ltd MEDICAL EDUCATION 2002;36:568–574

The PPOS instrument may be useful towards this end
in that it provides information that individual students
can use as a first step toward examining and developing
personal awareness of their own views.
It is important to note that our study measured
attitudes toward patient-centred care rather than actual
patient-centred behaviours. While it is difficult for us to
predict the clinical significance of relatively patient-
centred or doctor-centred scores without additional
outcome data, previous work with the PPOS has
demonstrated important links between doctor or stu-
dent attitudes and patient outcomes. Krupat and
colleagues previously demonstrated that patient-
centred attitudes among doctors are associated with
high degrees of patient satisfaction.8 In addition, we
previously demonstrated that patient-centred attitudes
among third-year medical students are associated with
higher standardized patients’ ratings of those students’
humanism.20 We assume that the mechanism through
which these favourable outcomes are achieved concerns
patient-centred behaviours exhibited by the doctor,
although this assumption remains to be tested. In our
ongoing work, we will be examining associations
between students’ attitudes and their communicative
behaviours with both standardized patients and ward
patients.
Our study has several limitations. Since we used a
cross-sectional design, the comparisons we made
between classes of medical students may not be indic-
ative of attitude changes that occur in individual students
as they progress through medical school. Another
limitation is the relatively small sample size for examining
the association of personal attributes to PPOS scores, as
well as the absence of second-year medical students in
our study. A larger sample may have statistical power to
show differences in overall PPOS scores that were
suggested by the sharing subscale analysis. In our
ongoing investigation, we are collecting demographic
and PPOS information from all medical students with
the statistical power to determine more accurately the
relative impacts of various demographic factors on
student attitudes and changes in attitudes over time.
The generalizability of our results is limited by our
collection of data at only one institution. However, the
curriculum at our study institution is relatively similar
to that at many other medical schools. At this
institution, all students receive formal instruction in
doctor–patient communication and ethics during the
pre-clinical years and they all participate in a weekly
longitudinal ambulatory care experience during the
clinical years. In addition, all students in the first-year
cohort receive feedback on communication skills
through the use of an objective structured clinical
examination (OSCE) with standardized patients. Given
the similarity between these types of patient-centred
curricula and those of other schools, we believe our
results to be indicative of general trends in attitudes of
medical students.
In conclusion, we have assessed the attitudes of
medical students toward the doctor–patient relation-
ship and shown these attitudes to be less patient-
centred among later-year classes of medical students.
Our hope is that these results will stimulate an ongoing
dialogue among educators, deans, and administrators
that will lead to innovative strategies in medical
education that challenge students and teachers at all
levels to critically examine their own views toward the
provision of patient care.
Contributors
PH conceptualized the research question. All contrib-
utors were involved in planning the research. PH, JED,
DAP, TC, ET and JCR worked on the design of the
study. PH, JED, TC, ET and JCR were involved in its
implementation. LH and TC contributed to design of
data analysis. PH, JED, DAP, LH and TC analysed the
data. PH and DAP drafted and revised the manuscript.
JED, LH, TC, ET and JCR carried out critical revision
of the manuscript.
The opinions and findings contained herein are those
of the authors and do not necessarily represent the
views of the US Department of Veterans Affairs, Baylor
College of Medicine, the University of California Davis
School of Medicine, or Augustana College.
Acknowledgements
The authors would like to acknowledge Harlan Nelson
MS for assistance in data management, Claire Huckins
PhD for assistance in data collection, and Nelda P
Wray MD MPH and Edward Krupat PhD for com-
ments and suggestions on earlier versions of the
manuscript. Data contained in this report were presen-
ted in part at the 22nd Annual Meeting of the Society of
General Internal Medicine, April 1999, San Francisco,
California, USA, and at the 110th Annual Meeting of
the Association of American Medical Colleges, October
1999, Washington DC, USA.
Funding
Dr Haidet is supported by a career development award
from the Office of Research and Development, Health
Services R&D Service, US Department of Veterans
Affairs.
Medical student attitudes • P Haidet et al. 573
� Blackwell Science Ltd MEDICAL EDUCATION 2002;36:568–574

References
1 Simpson M, Buckman R, Stewart M et al. Doctor–patient
communication: the Toronto consensus statement. BMJ
1991;303:1385–7.
2 Stewart M, McWhinney IR, Buck CW. The doctor–patient
relationship and its effect upon outcome. J Royal College
General Practitioners 1979;29:77–82.
3 Stewart M. What is a successful doctor–patient interview? A
study of interactions and outcomes. Social Sci Med
1984;19:167–75.
4 Schmidt H. Integrating the teaching of basic sciences, clinical
sciences, and biopsychosocial issues. Academic Med
1998;73:S24–31.
5 Hafferty FW. Beyond curriculum reform: confronting medi-
cine’ hidden curriculum. Academic Med 1998;73:403–7.
6 Krupat E, Putnam SM, Yeager C. The fit between doctors
and patients: can it be measured? J General Intern Med
1996;11 (Suppl.):134.
7 The Medical School Objectives Writing Group. Learning
objectives for medical student education – guidelines for
medical schools. Report 1 of the Medical School Objectives
Project. Academic Med 1999;74:13–8.
8 Krupat E. The practice orientations of doctors and patients.
The effect of doctor–patient congruence on satisfaction.
Patient Education and Counselling 1999;39:49–59.
9 Pfeiffer C, Madray H, Ardolino A, Willms J. The rise and fall
of students’ skill in obtaining a medical history. Med Educ
1998;32:283–8.
10 Atkinson P. Training for certainty. Social Sci Med
1984;19:949–56.
11 Good BJ. Medicine, Rationality, and Experience: an Anthropo-
logical Perspective. Cambridge: Cambridge University Press; 1994.
12 Haas J, Shaffir W. Becoming Doctors: the Adoption of a Cloak of
Competence. Greenwich, Connecticut: JAI Press; 1991.
13 Branch WT Jr, Kern D, Maidet P, Weissmann P, Gracey CF,
Mitchell G, Inui T. The patient–physician relationship.
Teaching the human dimensions of care in clinical settings.
JAMA 2001;286:1067–74.
14 Becker HS, Geer B, Hughes EC, Strauss AM. Boys in White:
Student Culture in Medical School. Chicago: Chicago University
Press; 1961.
15 Krupat E, Hiam CM, Fleming MZ, Freeman P. Patient-
centredness and its correlates among first year medical stu-
dents. Int J Psychiatry 1999;29:347–56.
16 West C. Routine Complications. Bloomington, Indiana: U Press;
1984.
17 Seto TB, Taira DA, Davis RB, Safran C, Phillips RS. Effect of
doctor gender on the prescription of oestrogen replacement
therapy. J General Intern Med 1996;11:197–203.
18 Kleinman AM, Eisenberg L, Good B. Culture, illness and
care. Clinical lessons from anthropological and cross-cultural
research. Ann Intern Med 1978;88:251–8.
19 Novack DH, Epstein RM, Paulsen RH. Toward creating
doctor-healers. fostering medical students’ self-awareness,
personal growth, and well-being. Academic Med 1999;74:516–
20.
20 Haidet P, Dains JE, Paterniti DA, Chang T, Tseng E, Rogers
JC. Medical students’ attitudes toward patient-centred care
and standardized patients’ perceptions of humanism: a link
between attitudes and outcomes. Academic Med 2001;76
(Suppl.):S42–S44.
Received 28 February 2001; editorial comments to authors 21 June
2001, 2 November 2002; accepted for publication 13 December 2001
Medical student attitudes • P Haidet et al.574
� Blackwell Science Ltd MEDICAL EDUCATION 2002;36:568–574





























