Embed Size (px)
Citation preview

AP R I L 2007 ■ VO LU M E 17, NUMBER 4
Also Inside:■ PET/CT Outpaces Modalities Used Separately in Staging Colorectal Cancer■ Ankle MR Study Exemplifies Role of Imaging in Diagnosis and Treatment■ Radiology Has Growing Stake in Cervical Cancer Trial■ RSNA Highlights™ Debuts in Phoenix
Advance Registration for RSNA 2007
Begins April 23
Medical Simulation Hailed as Turning Point in Radiology Training
Phot
o co
urte
sy o
f th
e A
rizo
na S
imul
atio
n Te
chno
logy
and
Edu
cati
on C
ente
r.

AP R I L 2007
E D I T O RBruce L. McClennan, M.D.
C O N T R I B U T I N G E D I T O RRobert E. Campbell, M.D.
M A N A G I N G E D I T O RLynn Tefft Hoff
E X E C U T I V E E D I T O RNatalie Olinger Boden
E D I T O R I A L A D V I S O R SDave Fellers, C.A.E.
Executive DirectorRoberta E. Arnold, M.A., M.H.P.E.
Assistant Executive DirectorPublications and Communications
E D I T O R I A L B O A R DBruce L. McClennan, M.D.,
ChairSilvia D. Chang, M.D.Colin P. Derdeyn, M.D.Richard T. Hoppe, M.D.David M. Hovsepian, M.D.Valerie P. Jackson, M.D.Jonathan B. Kruskal, M.D., Ph.D.Steven M. Larson, M.D.Hedvig Hricak, M.D., Ph.D.,
Board LiaisonSarah S. Donaldson, M.D.,
Board Liaison
C O N T R I B U T I N G W R I T E R SNicole Grasse, M.A.Caroline McNeilLocke PeterseimMarilyn Idelman Soglin
G R A P H I C D E S I G N E RAdam Indyk
2 0 0 7 R S N A B O A R D O F D I R E C T O R SGary J. Becker, M.D.,
ChairmanHedvig Hricak, M.D., Ph.D.,
Liaison for Publications andCommunications
Burton P. Drayer, M.D., Liaison for Annual Meeting and Technology
George S. Bisset III, M.D., Liaison for Education
Sarah S. Donaldson, M.D., Liaison for Publications andCommunications
N. Reed Dunnick, M.D.,Liaison for Science
R. Gilbert Jost, M.D.,President
Theresa C. McLoud, M.D., President-elect
RSNA NewsApril 2007 • Volume 17, Number 4
Published monthly by the Radiological Societyof North America, Inc., 820 Jorie Blvd., OakBrook, IL 60523-2251. Printed in the USA.
POSTMASTER: Send address correction“changes” to: RSNA News, 820 Jorie Blvd., Oak Brook, IL 60523-2251.
Nonmember subscription rate is $20 per year;$10 of active members’ dues is allocated to asubscription of RSNA News.
Contents of RSNA News copyrighted ©2007 bythe Radiological Society of North America, Inc.
Letters to the EditorE-mail: [email protected]: 1-630-571-7837RSNA News820 Jorie Blvd.Oak Brook, IL 60523
SubscriptionsPhone: 1-630-571-7873 E-mail: [email protected]
Reprints and PermissionsPhone: 1-630-571-7829Fax: 1-630-590-7724E-mail: [email protected]
RSNA Membership 1-877-RSNA-MEM
1 Announcements2 People in the News4 My Turn
Feature Articles 5 Medical Simulation Hailed as Turning Point
in Radiology Training7 RSNA Highlights™ Debuts in Phoenix8 PET/CT Outpaces Modalities Used Separately
in Staging Colorectal Cancer10 Radiology Has Growing Stake in Cervical
Cancer Trial12 Ankle MR Study Exemplifies Role of Imaging
in Diagnosis and Treatment
Funding Radiology’s Future®
14 R&E Foundation Donors
15 Journal Highlights16 Program and Grant Announcements17 Radiology in Public Focus19 RSNA: Working for You20 Exhibitor News21 Meeting Watch24 Product News25 RSNA.org

1R S N A N E W SR S N A N E W S . O R G
ANNOUNCEMENTS
NPI Deadline is May 23
RADIOLOGISTS are among theproviders required by the HealthInsurance Portability and Account-
ability Act of 1996 (HIPAA) to use onlya national provider identifier (NPI) instandard transactions as of May 23.
There are several ways to obtain anNPI:• Completing an application online at
nppes.cms.hhs.gov.
• Completing a paper application/updateform and mailing it to an NPI Enumer-ator, a special contractor hired by theCenters for Medicare and MedicaidServices (CMS). More information isavailable at 1-800-465-3203.
• Giving permission to a CMS-approvedElectronic File Interchange Organiza-tion to obtain an NPI for the provider.
More information is available at
www.cms.hhs.gov/NationalProvIdentStand/. A story about the NPI appeared inthe November 2006 issue of RSNA News.
Implementation of NIH Reform Act Under WayThe National Institutes of Health (NIH) hasnamed an ad hoc working group to carry out theprovisions of the NIH Reform Act of 2006,signed by President Bush in January.
Chaired by NIH DeputyDirector Raynard Kington,M.D., Ph.D., the workinggroup comprises NIH direc-tors and other leaders in leg-islation, policy, management,communications, extramural andintramural activities and budget, as well as repre-sentation from the Office of the General Counsel.
Key provisions in the act relate to NIH’sDivision of Program Coordination, Planning andStrategic Initiatives, Common Fund, Council ofCouncils and Scientific Management ReviewBoard, as well as authorization of appropriations,reorganization and reporting. The act is the thirdomnibus reauthorization in NIH history and thefirst in 14 years.
Legislation Calls for Two-Year Moratorium on DRA CutsCongress is considering the Access to MedicareImaging Act of 2007, bipartisan legislation call-ing for a two-year moratorium on the medicalimaging reimbursement cuts included in theDeficit Reduction Act (DRA) of 2005.
The bill, introduced Feb. 28 by Rep. CarolynMcCarthy, D-N.Y., and co-sponsored by 25 rep-resentatives, also calls for a GovernmentAccountability Office analysis of the DRA cuts’impact on patient access to medical imaging,particularly in rural and medically underservedareas.
Passed by Congress in February 2006, the DRA capped the techni-cal component of reimbursement for physician office imaging to thelesser of the Hospital Outpatient Prospective Payment System orMedicare Fee Schedule payment.
India Launches First Teleradiology NetworkA group of institutions in India has collaborated to establish the nation’sfirst teleradiology network. The network was developed by KakarlaSubbarao Radiological and Imaging Educational Sciences Trust, CareFoundation, U.S. Electronics and Electronics Corporation of India. Thefirst sites connected were the Care Hospital in Hyderabad to the MaaScan and Research Centre in Guntur.
MEDICAL IMAGING COMPANY NEWS
Work Begins at Siemens Biomarker Facility ■ Siemens Medical Solutions, of Malvern, Pa., has opened its Molecular Imag-ing Biomarker Research facility. Siemens said the new facility is the next steptoward its goal of becoming the first full-service diagnostics company, inte-grating in vivo and in vitro imaging capabilities. Looking to bring several newagents to the market over the next 5–10 years, scientists at the new facilitywill focus largely on oncology and neurology along with inflammation andmicrofluidics/nanotechnology research.
VIEWING TECHNOLOGY
Tip of the MonthCR and DR images can be greatly under-exposed and still have normal densityand contrast. Too little radiation mayyield too much noise and thereforeobscure the findings.
American Association of Physicists in Medicine
Rep. Carolyn McCarthy,D-N.Y.

2 R S N A N E W S A P R I L 2 0 0 7
PEOPLE IN THE NEWS
HatteryNamed HonoraryECR MemberRobert R. Hattery, M.D.,(center), immediatepast-president of RSNA,was named an honorarymember of the EuropeanCongress of Radiology(ECR) last month inVienna, Austria. Dr. Hat-tery is executive directorof the American Boardof Radiology. Presenting Dr. Hattery with honorary membership are Nicholas Gourt-soyiannis, M.D., immediate past-president of the European Society of Radiology (left)and Christian J. Herold, M.D., immediate past-president of ECR.
Also named an ECR honorary member was Kaori Togashi, M.D., of Kyoto, Japan.Philippe Grenier, M.D., of Paris, and Robert E. Steiner, M.D., of London, received the ECRgold medal. Presented with the ECR Special Presidential Award was Elias A. Zerhouni,M.D., director of the National Institutes of Health.
Segal, Korobkin toReceive SUR LifetimeAchievement AwardsThe Society of Uroradiology(SUR) will present LifetimeAchievement Awards toArthur J. Segal, M.D., andMelvyn T. Korobkin,M.D., at its joint meetingthis month with the Societyof Gastrointestinal Radiolo-gists (SGR) and the Euro-pean Society of UrogenitalRadiology. Dr. Segal is chairof the Department of Diag-nostic Imaging at RochesterGeneral Hospital inRochester, N.Y. Dr.Korobkin is a professor ofradiology at the Universityof Michigan in Ann Arbor.
Also at the meeting,SGR will award its Walter B. Cannon Medal to Bronwyn Jones, M.D., aprofessor of radiology and director of the Swallowing Center at Johns Hop-kins Hospital in Baltimore. Robert L. Lebowitz, M.D., a staff radiologistat Children’s Hospital Boston and a professor of radiology at Harvard Med-ical School in Boston, will receive the SUR gold medal.
Smoron Honored by ChicagoRadiological Society
THE Chicago Radiological Society willpresent Geoffrey L. Smoron, M.D.,with its Distinguished Service Award
this month. Dr. Smoron is president of Mid-west Radiation Oncology Con-sultants in Elgin, Ill.
Dr. Smoron received hisM.D. degree from Loyola Uni-versity and completed a resi-dency at Northwestern Univer-sity, both in Chicago. A com-missioned officer in the U.S.Naval Reserve, he served ashead of the nuclear medicineand radiation therapy branchesin the Department of Radiology
at the Great Lakes Naval Regional MedicalCenter in Illinois. He also taught at North-western University Medical School for morethan 25 years and was medical director ofthe School of Radiation Therapy Technologyat Provena St. Joseph Hospital in Elgin. Heis a past-president of the Chicago Radiologi-cal Society and has held leadership positionsin many other radiologic societies, includingRSNA.
Arthur J. Segal, M.D. Melvyn T. Korobkin, M.D.
Bronwyn Jones, M.D. Robert L. Lebowitz, M.D.
Geoffrey L. Smoron,M.D.
Kaori Togashi, M.D.
Philippe Grenier, M.D.

SIR Presents Awards
THE Society of InterventionalRadiology presented goldmedals to Rolf W. Günther,
M.D., Eugene Klatte, M.D., andJulio Palmaz, M.D., during itsannual meeting last month.
Dr. Günther has been a profes-sor and chair of the Department ofDiagnostic Radiology at theAachen University of Technologyin Germany since 1984. Dr. Klatteis a distinguished professor in theDepartment of Radiology at theIndiana University School of Medi-cine in Indianapolis, where hechaired the Department of Radiol-ogy for 20 years.
Dr. Palmaz helped invent thePalmaz-Schatz stent that was FDAapproved in 1994. He is a professorin the Department of Radiologyand chief of cardiovascular andspecial interventional radiology at the University of Texas Health Science Centerat San Antonio.
The SIR Foundation presented its Leaders in Innovation Award to Robert I.White Jr., M.D., whose concept of multidisciplinary care for the treatment ofhereditary hemorrhagic telangiectasia (HHT) has been adopted by physiciansworldwide. Dr. White is director of Yale University’s Vascular Malformation Clinical and Research Group.
3R S N A N E W SR S N A N E W S . O R G
PEOPLE IN THE NEWS
Rolf W. Günther, M.D. Eugene Klatte, M.D.
Julio Palmaz, M.D.
Cruea to Head Academy ofRadiology Research Renee Cruea, M.P.A., is the newexecutive director of the Academy ofRadiology Research. Cruea had beenthe academy’s government relationsdirector since1998. In addi-tion to manag-ing day-to-dayoperations forthe Washing-ton-basedorganization,she will over-see its newCoalition forImaging & Bioengineering Research.
Cruea succeeds Ed Nagy, whohad served as executive directorsince 1995. Nagy passed away inJuly 2006.
Prior to joining the academy,Cruea worked with the Washingtonlobbying firm Rae Evans & Associ-ates. She is also founder and presi-dent of “Sugar Mommas,” an organi-zation for women who have type 1diabetes and are mothers to youngchildren.
IN MEMORIAM:
Reynold F. Brown, M.D.1971 RSNA PresidentReynold F. Brown, M.D.,died Dec. 29, 2006.Known for his work inestablishing safeguardsand standards for radiationexposure, Dr. Brown wasa clinical professor in theDepartment of Radiologyat the University of Cali-fornia, San Francisco anddirector of the university’s Radiologic HealthSciences Education Project. He also servednumerous organizations charged withincreasing radiation protection and chairedthe former RSNA Radiation Safety Commit-tee. Dr. Brown received the RSNA goldmedal in 1973.
IN MEMORIAM:
Paul A. Riemenschneider, M.D. Paul A. Riemenschneider, M.D., anRSNA gold medalist in 1990, died Janu-ary 29.
Dr. Riemenschneider completed hisradiology residency at Peter BentBrigham Hospital (now Brigham andWomen’s Hospital) in Boston, and servedas a medical officer in the U.S. Navy. Hewent on to develop and chair the Depart-ment of Radiology and the radiology res-idency program at Syracuse MemorialHospital and later served as a professorand chair of the Department of Radiology at Upstate Medical Cen-ter in Syracuse. From 1964 until his retirement in 1988, Dr.Riemenschneider served as chief of diagnostic radiology at SantaBarbara Cottage Hospital in California.
He also received the gold medals of the American College ofRadiology and American Roentgen Ray Society.
Robert I. White Jr.,M.D.
Renee Cruea, M.P.A.
Paul A. Riemenschneider,M.D.
Reynold F. Brown, M.D.

Paul C. Lauterbur, Ph.D., and SirPeter Mansfield, Ph.D., who sharedthe 2003 Nobel Prize in Medicine fortheir early discoveries in MR imaging,were inducted in February into theNational Inventors Hall of Fame.
Dr. Lauterbur, who died March 27,was a professor of chemistry, bio-physics and computational biology andbioengineering and a DistinguishedUniversity Professor of medical infor-mation sciences at the University ofIllinois in Urbana.
Dr. Mansfield is an emeritus pro-
fessor of physics at the Univer-sity of Nottingham in England.
Dr. Lauterbur received theRSNA gold medal in 1987 andthe gold medal of the AmericanRoentgen Ray Society in 2005.Drs. Lauterbur and Mansfieldreceived the gold medal of andhonorary membership in theInternational Society for Mag-netic Resonance in Medicine.
They were among a Hall of Fameclass of seven living inductees and nineposthumous recognitions that included
the inventors of non-toxic weed killerand the automotive airbag.
4 R S N A N E W S A P R I L 2 0 0 7
What Are Our Priorities?
ITHOUGHT this question might promptsome readers to pause and read thismonth’s My Turn column. This
provocative inquiry truly reflects mytopic. As I walked around RSNA 2006,I heard “water cooler” dis-cussions like the following:“I could make so much moremoney if I moved to …”;“Our resident just took a jobwith a starting salary of …”; “She justgot a signing bonus of …”; “I took thejob because they have a ‘nighthawk’service”; and “They get three monthsoff per year …”
What I didn’t hear, on the otherhand, were phrases such as: “Thatgroup does high-quality patient care,”“This facility is very patient-centric”and “I was disappointed to have hadthis complication and need to figure outhow to avoid it in the future.”
We are fortunate to be part of an
exciting profession thatserves patients and clinicians.We should never lose sight ofour responsibilities—we arephysicians first. When I
started my radiol-ogy career aftermany years as aclinician, I had toget over the fact
that some clinicians didn’tconsider us “real doctors.”
Patients entrust their lives to ourbrains, eyes and hands. Our decisionsprofoundly affect clinical managementand, ultimately, patient outcome. Weshould never forget that behind everyradiographic study we perform andinterpret is a patient; otherwise, we losethe respect of our clinical colleagues.Arguably, our patient commitment hasalready waned, putting us at risk of“commoditizing” our specialty.
Trivializing our respon-sibility toward the patientmeans turning our backs onwhy we chose our nobleprofession. As the theme ofRSNA 2006 indicated, med-ical professionalismrequires us to put ourpatients above all else. Atthe risk of sounding like apedagogue, I challenge eachof us to maintain our pro-
fessional values, continue the quest forhigh-quality care and, above all,remember why we are here.
So, what really are your priorities?
My TurnONE RADIOLOGIST’S VIEW
George S. Bisset III,M.D.
George S. Bisset III, M.D., is the RSNA BoardLiaison for Education. Dr. Bisset is a professorof radiology and pediatrics and vice-chair ofthe Department of Radiology at Duke Univer-sity Medical Center in Durham, N.C.
Paul C. Lauterbur,Ph.D.
Sir Peter Mansfield,Ph.D.
MR Imaging Pioneers Inducted Into Inventor Hall of Fame
Imag
e co
urte
sy o
f U
nive
rsit
y of
Illi
nois
at
Urb
ana-
Cham
paig
n.
PEOPLE IN THE NEWS
Send news about yourself, a colleague or your department to [email protected], 1-630-571-7837 fax, or RSNA News, 820 JorieBlvd., Oak Brook, IL 60523. Please include your full name and telephone number. You may also include a non-returnable color
photo, 3x5 or larger, or electronic photo in high-resolution (300 dpi or higher) TIFF or JPEG format (not embedded in a document). RSNA News maintainsthe right to accept information for print based on membership status, newsworthiness and available print space.
MY TURN

5R S N A N E W SR S N A N E W S . O R G
Medical Simulation Hailed as NextRevolution in Radiology Training
LAST FALL at the University of Arizona(U.A.) College of Medicine inTucson, a CT technician notified a
radiology resident of a patient’s reac-tion to contrast medium. The residenttalked to the patient, who reported feel-ing itchy. The resident administeredBenadryl, but the patient’s blood pres-sure and heart rate increased. Next try-ing epinephrine, the resident found thepatient starting to wheeze. The residentput the patient on oxygen, to littleeffect. Faced with the prospect of ana-phylactic shock, the resident decided tointubate the patient and, for the firsttime in his career, performed the proce-dure on his own.
Tense though the situation was, itdidn’t take place in the hospital andnobody was at risk. The dramaunfolded in U.A.’s simulation labora-tory, where residents learn to performand manage procedures on variousdevices. The hybrid simulator used inthis case combines computers withinterface devices, such as automatedmannequins, to create close-to-real-lifepractice situations.
The whole scenario, including theintubation procedure,was extremely realistic,said Elizabeth A.Krupinski, Ph.D., aresearch professor inthe Department ofRadiology Research atU.A. “You could seethe resident’s stress lev-els rising,” said Dr.Krupinski, whodesigned the trainingwith William Berger, M.D., director ofU.A.’s Diagnostic Radiology Resi-dency Program. Each session is video-taped and reviewed with the resident
performing the simulated procedures.The resident then receives more train-ing to correct mistakes and then repeatsthe simulation.
The Arizona Simulation Technol-ogy and Education Center, known as
the SimLab, is in thevanguard of a youngand growing field.Interventional radiol-ogists in particularhave increasing inter-est in simulation,especially for itspotential to providetraining withoutpatient risk, said GaryJ. Becker, M.D., pro-
fessor of vascular and interventionalradiology at U.A.
“It moves the entire learning experi-ence, with diagnosis and treatment
under stress, to a low-stakes environ-ment away from the patient’s bedside,”said Dr. Becker, 2007 RSNA BoardChairman and an associate executivedirector of the American Board ofRadiology (ABR).
Procedural simulation in medicinebegan with anesthesiology and resusci-tation training in the 1980s, and its usein interventional radiology goes backabout a decade. Only three small com-panies now make interventional radiol-ogy simulators, all for training inimage-guided interventions such ascarotid stenting and angioplasty. Somealso simulate endovascular proceduresin the leg or kidney.
Growth AreasOther applications are on the horizon,said Steven Dawson, M.D., associate
It moves the entire learning
experience, with diagnosis
and treatment under
stress, to a low-stakes
environment away from
the patient’s bedside.
Gary J. Becker, M.D.
FEATURE HOT TOPIC
Continued on next page
University of Arizona radiology resident Josh Morais, M.D., performs endotrachealintubation as he manages a simulated life-threatening reaction to iodinated con-trast material in the Arizona Simulation Technology and Education Center. At leftis Alyson E. Knapp, Sim Lab program coordinator and curriculum developer. Inthis scenario, Knapp serves as a radiologic technologist assisting Dr. Morais inmanaging the patient.
Phot
o co
urte
sy o
f th
e A
rizo
na S
imul
atio
n Te
chno
logy
and
Edu
cati
on C
ente
r.

6 R S N A N E W S A P R I L 2 0 0 7
professor of radiology at Harvard Med-ical School and program lead for med-ical simulation at Massachusetts Gen-eral Hospital’s Center for Integration ofMedicine and Innovative Technology.Managing rare but dangerous situationslike the contrast medium reaction isone example.
Another application is managingstroke in its early stages. If more firstresponders were trained to performendovascular procedures, many morestrokes could be halted and their effectsreversed, said Dr. Dawson, a presenter at“Oncologic Image-Guided Interventions:Opportunities for Collaboration,” a con-ference held in February in Washingtonto encourage collaboration among indus-try, academia and federal agencies. “It isa growth area and could have a hugepublic health impact,” he said.
Another growth area is patient-spe-cific simulation—placing a patient’s
CT or MR images ona simulator andrehearsing a proce-dure just prior to per-forming it. The firstsuch “virtual reality”carotid stenting tookplace recently atEmory Hospitals inAtlanta, as reportedby Christopher Cates,M.D., and colleaguesin the Jan. 17, 2007,issue of The Journalof the American Med-ical Association.
Caps on residents’work hours, the trendtoward more outpa-tient procedures andthe increase in nonin-vasive diagnostic pro-cedures have all
decreased the direct contact radiologyresidents have with patients, saidexperts. Simulation can help fill the gap.
Simulation’s unique advantages,such as its potential to measure per-formance, also make it attractive in cer-
tification examinations,said Dr. Becker. The ABRFoundation just took itsfirst step in that directionwith a grant to James Dun-can, M.D., Ph.D., an assis-tant professor of radiologyat Washington Universityin St. Louis, to developimage-guided biopsy simu-lation with cross-sectionalimaging as part of the cer-tification exam.
Simulation could alsohelp measure milestoneachievement during residency. “Theneed to integrate skills and reach mile-stones within the context of graduatemedical education can be satisfied inlarge measure by simulation once wehave a robust menu of simulators thatcan do what we need them to do,” saidDr. Becker.
Next StepsHow to get that robust menu is theoverall challenge facing the youngfield. Endovascular simulators are stillin their infancy—some use fluoroscopicimages that are somewhat lifelike, butthere are still many nuances of feedbackand control in real-life patients that sim-ulators cannot yet provide, Dr. Beckersaid.
Given the limited applicationsoffered so far, little planning has goneinto where simulation can fit into a com-prehensive course curriculum. Asimprovements are made in simulatortechnology and new applications aredeveloped, the challenge will be todesign course-specific simulators thatcan also provide performance evaluation.
The Joint International SimulationTask Force, which includes RSNA, theCardiovascular and Interventional Soci-ety of Europe (CIRSE) and Society ofInterventional Radiology (SIR), has out-lined steps needed to meet these chal-lenges. They include offering valida-tion—proof that the skills acquired insimulation do transfer to patient care—as well as establishing performance
measures and identify-ing points in the curricu-lum at which to insertsimulation.
For now, the taskforce recommends thatsimulation be limited tocertain early stages oftraining, such as teach-ing the correct sequenc-ing of steps in a proce-dure. Simulation cannotyet be regarded asequivalent to trainingon actual patients due
to the lack of validation, according totask force guidelines published in theFebruary 2006 issue of the Journal ofVascular and Interventional Radiology.
The task force emphasized that sim-ulation will never replace managingreal patients. Nevertheless, task forceleaders Derek Gould, M.D., of CIRSEand Aalpen A. Patel, M.D., of SIR, giv-ing a joint presentation at the MedicineMeets Virtual Reality meeting in LongBeach, Calif., in February 2007, articu-lated an optimistic vision. By 2010,they said, “a growing number of vali-dated interventional radiology simula-tion training modules will have beenshown to transfer skills and reduce pro-cedural error, be delivering clinicalbenefit to patients and have been inte-grated into a standardized interven-tional radiology training curriculumand certifying exam.”
Creating simulators to meet thisvision will take experts in variousfields, said Dr. Dawson, currently theU.S. leader for the task force. “Hugechallenges revolve around issues ofphysics, mathematics, computer graph-ics and physiology models,” he said,adding that educational psychologistsand others in the human factors fieldsare also needed to design simulatorsthat are educationally sound withdefined metrics and performance indi-cators.
“It’s a daunting task,” he said, “butone worthy of national attention.” ■■
Learn MoreAdditional information aboutthe institutions, conferencesand articles mentioned inthis story is available online.■ Arizona Simulation Tech-nology and Education Centerwww.astec.arizona.edu■ Medicine Meets VirtualReality 15www.nextmed.com/mmvr_virtual_reality.html■ “Use of Virtual Reality Sim-ulation for Mission Rehearsalfor Carotid Stenting”jama.ama-assn.org/cgi/content/extract/297/3/265-a■ “Simulation Devices inInterventional Radiology: Validation Pending”www.jvir.org/cgi/content/full/17/2/215
Continued from previous page
Elizabeth A. Krupinski, Ph.D.University of Arizona

7R S N A N E W SR S N A N E W S . O R G
RSNA Highlights™ Debutsin Phoenix
ENTHUSIASTIC attendees of RSNA’snew annual conference option,RSNA Highlights™, hailed the
inaugural outing as convenient, colle-gial and concentrated.
“The conference provided an excel-lent overview of many topics importantto daily practice,” said Ian Peterkin,M.D., an RSNA member in privatepractice in Washington. “Many expertsin diagnostic imaging from around thecountry, as well as international speak-ers, shared their knowledge and experi-ence with superb lectures.”
Held Feb. 26–28 at the J.W. Mar-riott Desert Ridge Resort & Spa inPhoenix, RSNA’s first educational con-ference drew 300 attendees. Amongthem was Yusuf Mnyusiwalla, M.D., ofWaterloo, Ontario.
“I haven’t been to an RSNA[annual] meeting in 15 years—it’s justbecome too big,” said Dr. Mnyusiwalla.“I like the small size of this Highlightsmeeting and the location. It’s a niceplace to bring family.”
RSNA Highlights was designed forradiologists who can’t attend the annualmeeting, or those who attend but findthey can’t get to every lecture theywant. Four topics were covered in fourrefresher courses apiece and two “hottopics” courses were offered as well.RSNA Highlights attendees also hadimmediate access to select electroniceducation exhibits from RSNA 2006—a feature that was a definite hit withattendee Alton Baker, M.D., of Birm-ingham, Ala.
“This is genius!” said Dr. Baker, ofthe education exhibits and RSNA Ser-vices area. “This is a chance for the col-legiality you’d like to see at the RSNAmeeting. I just had breakfast with peo-ple from L.A., San Francisco and
Phoenix.”Dr. Baker said he also felt more
able to focus on the educational coursesat Highlights than at the RSNA annualmeeting. “At the annual meeting, Ispend so many hours looking at equip-ment, it reduces the time for hearingpapers and going to courses,” he said.
Others echoed Dr. Baker’s com-ments, noting that the sheer volume ofopportunities that make the RSNAannual meeting so popular can alsomake it distracting. Highlights, theysaid, gave them a chance to “hone inon topics.” Attendees also welcomedthe opportunity to complete self-assess-ment modules, which contribute to the
American Board of Radiology Mainte-nance of Certification process.
Highlights participants alsoapplauded the conference location.While much of the country was shiver-ing in below normal temperatures,Phoenix saw highs in the 60s and 70s.
RSNA Highlights 2008 will be heldFeb. 18–20 at the Ritz-Carlton/J.W.Marriott Orlando, Grande Lakes inFlorida. Course emphasis will includecardiac imaging, head and neck imag-ing, thoracic imaging and breast imag-ing. More details will be announced infuture issues of RSNA News and on theWeb at RSNA.org/highlights. ■■
(clockwise, from top left:) Elliot K. Fishman, M.D.,delivered the keynote address at RSNA Highlights™2007. In the RSNA Services area, attendees couldaccess the Internet, purchase RSNA educationalproducts and learn about RSNA membership andbenefits. Attendees could also access select elec-tronic education exhibits from RSNA 2006. Theconference drew more than 300 attendees.
FEATURE EDUCATION

8 R S N A N E W S A P R I L 2 0 0 7
PHYSICIANS and their patients havereason to be intrigued by a recentstudy showing the potential of
positron emission tomography (PET)and computed tomography (CT) as awhole-body imaging procedure toimprove colorectal cancer staging.
In a prospective study of 47patients who had clinical findings andoptical colonoscopy suggesting primarycolorectal cancer, researchers at Uni-versity Hospital Essen in Germanyfound tumor, lymph node and metasta-sis (TNM) staging was correctly deter-mined by PET/CT colonography in 37of 50 lesions (74 percent). TNM stag-ing was correctly determined by CTfollowed by PET (CT + PET) in 32lesions (64 percent) and by whole-bodyCT alone in 26 lesions (52 percent).
Patients underwent whole-bodyPET/CT colonography one day aftercolonoscopy. Study findings appear inthe Dec. 6, 2006, issue of The Journalof the American Medical Association.
Few studies have explored stagingcolorectal cancer withPET/CT, said leadresearcher Patrick Veit-Haibach, M.D., formerlya radiologist in theDepartment of Radiologyat University HospitalEssen. He said he con-ducted the study becausehe felt image quality inPET/CT had been com-promised in the past.
“The CT component was used onlyas a morphological landmark,” he said.“This was the first study of true inte-grated hybrid imaging using state-of-
the-art radiological imaging protocolsin PET/CT.”
Combined Report Available ImmediatelyWhile acknowledging opticalcolonoscopy as the standard for cancerdetection and tissue sampling, Dr. Veit-Haibach and colleagues noted thatmany additional imaging tests are
needed to check if thedisease has spread tothe lymph nodes andother organs. Theytheorized fusing func-tional with morpho-logical data could helpclinicians stage tumorsand plan treatment.
“We think this is alogistical advantage forreferring physicians
and patients, because we can provide acombined, one-step report on the sameday,” said Dr. Veit-Haibach, now anuclear medicine physician in the
Department of Nuclear Medicine at Uni-versity Hospital in Zürich, Switzerland.
In determining N-stage withPET/CT colonography and CT alone,Dr. Veit-Haibach and colleagues used a0.7 cm node threshold, which was ofparticular note to Ronald M. Summers,M.D., Ph.D., a senior investigator withthe Department of Diagnostic Radiol-ogy at the National Institutes of HealthClinical Center. Noting that the 0.7 cmthreshold is a third smaller than the 1 cm standard for investigators today,Dr. Summers said, “Radiologists shouldtake a closer look at this.”
The study revealed a statisticallysignificant advantage for PET/CT overconventional staging in defining T-stage—information that is critical inrectal cancer as neoadjuvant therapy isweighed against resection alone, saidDr. Veit-Haibach.
It’s important for a surgeon to haveaccurate information about higher T-stages because other organs may be
PET/CT Outpaces ModalitiesUsed Separately in Staging Colorectal Cancer
We think this is a logistical
advantage for referring
physicians and patients,
because we can provide a
combined, one-step report
on the same day.
Patrick Veit-Haibach, M.D.
Patrick Veit-Haibach, M.D.University Hospital, Zurich
Ronald M. Summers, M.D., Ph.D.National Institutes of Health Clinical Center
FEATURE SCIENCE

9R S N A N E W SR S N A N E W S . O R G
involved, Dr. Veit-Haibach added. Ofthe four patients in his study for whomPET/CT changed patient management,three had abnormalities which weredetected in organs other than the colon.
Bowel Preparation Still a Drawback While physicians can appreciate thequick, integrated report offered byPET/CT—which facilitates quicklystarting patients on needed therapies—patients also reap psychological andphysical benefits from not having toundergo different imaging proceduresseparately. In fact, in the German studyCT and PET were performed on thesame scanner, not separate scanners ashad been the clinical norm in the past.This may have overestimated the accu-racy of CT + PET for TNM staging, Dr.Veit-Haibach said.
PET/CT colonography isn’t withoutits drawbacks for patients, however.Bowel preparation for the patient can bevery uncomfortable, as it involves awater enema that must be retained for ahalf-hour. Researchers used water afterdetermining that colonic distension bycarbon dioxide or air could require addi-tional air inflation during the procedure,due to intestinal absorption of the gaswhich may cause misregistered images.
While the digital bowel cleansingbeing investigated by vendors won’t beavailable for some time, said Dr. Veit-
Haibach, burden to the patient has beeneased by reducing the procedure timefrom 30 minutes to 20 minutes.
Dr. Summers said it is important toremember that this research focusesonly on patients with colorectal can-cer—a relatively small patient popula-tion compared to the huge screeningpatient population envisioned to benefitfrom standard CT colonography. “CTcolonography does find cancers verywell—almost 100 percent,” he said. Healso noted that researchers have previ-ously used CT colonography to stagecolorectal cancers; it is the added bene-fit of PET, as shown in this study, thatis of great interest.
Bottom line, said Drs. Veit-Haibachand Summers, the new study illumi-nates some intriguing and innovative
developments which require still moreinvestigation. “This is a new way to usean existing technology to providepotential new information in the stagingof colorectal cancer, particularly for T-stage and N-stage,” said Dr. Summers.
Dr. Summers said he’d like to seethese results replicated and validated ona larger scale, with a larger number ofpatients, at different medical centers andusing even newer PET/CT scanners thatreduce the exam time. “In theory, thismay become a more useful test as theequipment improves, such as PET/CTdetectors with thinner slices,” he said. ■■
RADIOTHERAPY delivery is a prognosticfactor for locoregional recurrence rate
(LRR) in rectal cancer and is influenced byfactors including treatment center and sched-ule, German and Austrian researchers haveconcluded.
Rainer Fietkau, M.D., of the University ofRostock in Germany, and colleagues analyzeddata from 788 patients with rectal cancer todetermine radiotherapy’s impact on LRR anddisease-free survival (DFS) at five years.Results of their study appear in the March15, 2007, issue of the International Journal ofRadiation Oncology * Biology * Physics.
Noting significant differences in radiother-apy delivery patterns among the 10 treat-ment centers involved in the study, Dr.Fietkau and colleagues defined radiotherapyas adequate if delivered in less than 49 daysfor adjuvant or less than 44 days for neoad-juvant, or with a minimum radiation dose of4700 cGy for adjuvant or 4300 cGy forneoadjuvant.
The researchers found that 137 patients notreceiving radiotherapy had a 29.6 LRR and55.1 percent DFS, while 71 patients receivedinadequate radiotherapy but had a 21.2 LRRand 57.4 percent DFS. The 580 patients
whose radiotherapy was deemed adequate hada 6.8 percent LRR and 69.1 percent DFS.
The researchers also noted that postopera-tive radiotherapy significantly influencedLRR while radiotherapy delivered preopera-tively did not.
The abstract for “Rectal cancer delivery ofradiotherapy in adequate time and with ade-quate dose is influenced by treatment center,treatment schedule, and gender and is prog-nostic parameter for local control: Results ofstudy CAO/ARO/AIO-94” can be foundonline at www.rtsource.com/periodicals/rob/article/PIIS0360301606033499/abstract.
❚
Radiotherapy Delivery Influences Rectal Cancer Outcomes but Accuracy Depends on Several Factors
■ To read the abstract for “Diagnostic Accu-racy of Colorectal Cancer Staging withWhole-Body PET/CT Colonography,” go tojama.ama-assn.org/cgi/content/abstract/296/21/2590.
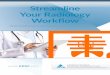
Slightly Thickened Bowel Wall at the Left Colonic Flexure and T2 Tumor(a) This small lesion was missed by CT imaging (T0) (arrowhead). (b) and (c): CorrespondingPET/CT colonography and PET alone demonstrated elevated glucose metabolism, indicating acolorectal cancer (arrowheads). The PET/CT scan suggested a T2 tumor, which was verified bysubsequent hemicolectomy with histopathological evaluation.Reprinted from The Journal of the American Medical Association 2006;296:2590-2600. Veit-Haibach, P., et. al. “Diagnostic Accuracy of Colorectal Cancer Staging With Whole-Body PET/CT Colonography.” © 2006, with permission from the American Medical Association.
ba c
CT Alone PET/CT PET Alone

10 R S N A N E W S A P R I L 2 0 0 7
RADIOLOGISTS now have double thereasons to join a new a clinicaltrial looking at lymph node metas-
tasis in patients with cervical cancer. Atrial initially set to test only PET againstsurgery has expanded to evaluate MRimaging with a new agent.
A joint effort of the American Col-lege of Radiology Imaging Network(ACRIN) and the Gynecologic Oncol-ogy Group (GOG), the ACRIN6671/GOG 0233 trial will launch thisspring at eight sites. Launch wasdelayed several months by complexpreparations, not the least of which wasobtaining FDA approval for the newMR contrast medium, ferumoxtran-10,to be used as an investigational newdrug (IND) agent.
GOG principal investigator MichaelA. Gold, M.D., an associate professorof obstetrics and gynecology at theUniversity of Oklahoma Health Sci-ences Center, conceived of the initialconcept for the trial in 2000. “We werelooking at newer modalities for imag-ing, mainly PET scans, to see if theywould be useful toolsfor finding lymph nodemetastasis from locore-gionally advanced cer-vical cancer,” said Dr.Gold. While early cer-vical cancers can betreated with surgery, hesaid, many centersdon’t perform surgeryat all and rely entirely on imaging tolook for lymph node metastasis toguide chemotherapy and radiation treat-ments in advanced cervical cancer.
Some centers, such as the Univer-sity of Oklahoma, prefer to do pre-operative mini-surgical explorations ofthe lymph node bed in search of metas-
tasis. Studies have suggested that suchexplorations can alter treatment deci-sions in as many as 40 percent ofpatients compared to those who onlyhad imaging with no surgery, said Dr.Gold. However, he added, the explo-rations can also delay treatment andraise their own risks and possible com-plications. Hence, his search for better
lymph node imagingapproaches began.
Need for RadiologistsRecognizedAfter three years ofdeveloping the study,Dr. Gold said he andhis GOG colleaguesrealized that “as
oncologists, radiation oncologists andmedical oncologists, we see and treat alot of cervical cancers, but we’re notimagers, so we don’t really have theknowledge to run an image-based studylike this.” They subsequently presentedthe idea of a PET study to the NationalCancer Institute’s Cancer Therapy
Evaluation Program and ACRIN.It was at that point that the study’s
ACRIN protocol principal investigator,Mostafa Atri, M.D., Dipl., Epid.,became involved. Head of the abdomi-nal division of the University ofToronto’s Medical Imaging Depart-ment, Dr. Atri said he and ACRIN rec-ognized innovations and agents thatcould be tested alongside PET. Theysuggested combining the modalitiesinto a new proposal that added MRimaging with the ferumoxtran-10 andcombined PET with CT.
“Traditionally we have used CTand MR imaging to look for lymphnode metastasis mainly using size-based criteria,” said Dr. Atri. “In thisstudy we are looking for metastatic fociin the lymph nodes, so we are not rely-ing on the size criteria.
While the PET/CT scans of thelymph nodes will identify disease basedon increased activity, the MR imageswith ferumoxtran-10 will show diseasebased on a lack of absorption, said Dr.Atri. Ferumoxtran-10 is an ultrasmall
Radiology Has Growing Stakein Cervical Cancer Trial
As oncologists, radiation
oncologists and medical
oncologists, we see and treat
a lot of cervical cancers,
but we’re not imagers.
Michael A. Gold, M.D.
Michael A. Gold, M.D.University of Oklahoma
Mostafa Atri, M.D., Dipl., Epid.University of Toronto
FEATURE CLINICAL TRIALS

11R S N A N E W SR S N A N E W S . O R G
Conflicting attitudes about participating inclinical trials—uncertainty about trusting theexperimenters, fear of the trial itself and hopethat the research will result in medicalprogress—may hinder women’s willingness toparticipate, according to recent study con-ducted at the Wake Forest University Schoolof Medicine in Winston-Salem, N.C.
The study, published in the February2007 issue of the Journal of Health Care forthe Poor and Underserved, focused particu-larly on black women and low socio-economic status white women.
“Enrolling representative populations isessential to the generalizability of study find-ings,” write researchers Deborah F. Farmer,
Ph.D., Sharon A. Jackson, Ph.D., and MarkA. Hall, J.D., of the Department of SocialSciences and Health Policy. Women andminorities continue to be under-representedin clinical trials despite a 1993 Congressionalmandate that they be included, theresearchers note.
For the study, 72 women—52 blackwomen from a range of income levels and 20low-income white women—were placed in10 focus groups. Asked about clinical trials,participants expressed fear at subjectingthemselves to procedures or drugs not usedbefore and distrust of clinical investigators asself-promoting, but also talked of hope thatresearch would prevent and cure diseases.
The subjects also cited other reasons,including time constraints, lack of day careand fear of medical procedures, for not want-ing to participate in clinical trials. The solu-tion, the Wake Forest team concludes, is foracademic centers to become more involvedwith minority and low socioeconomic statuscommunities so that scientists and citizensmay become partners in addressing healthproblems.
The abstract for “Attitudes of AfricanAmerican and Low Socioeconomic StatusWhite Women toward Medical Research”can be accessed at muse.jhu.edu/login?uri=/journals/journal_of_health_care_for_the_poor_and_underserved/v018/18.1farmer.html.
❚
Fear, Distrust Hold Women Back From Clinical Trial Participation
superparamagnetic iron oxide agentpicked up by macrophages in the nor-mal lymph nodes, resulting in “defects”in the nodes where they are occupiedby metastasis.
The ACRIN-GOG trial will use abrand of ferumoxtran-10 called Com-bidex. Dr. Atri said the Combidex man-ufacturer, Advanced Magnetics Inc.,had considered using the study to gainFDA approval, but instead has decidedto pursue approval while the trial isongoing.
Surgery to Confirm Imaging Accuracy Dr. Gold said the trial will involve 325patients with stage IB2, IIA>4 cm andstages IIB to IVA cervical cancers.
While past single-site trials havetested the effectiveness of PET/CTscanning of the lymph nodes, said Dr.Gold, this trial will not only be largerbut will also use the “gold standard”—surgical exploration following imagingto determine if the scans were accurate.
Dr. Gold said the trial will “be aslowly evolving process,” beginningwith the eight sites this spring andexpanding to more sites in about sixmonths. The study is starting with sitesthat anticipate enrolling 10 or morepatients a year, said Dr. Gold, so that“we can get a good sense of how wellthe trial works before other sites, which
may not see that many patients, getinvolved.” Both Drs. Atri and Goldexpect the trial to run about three years.
For a center to participate, it mustbe affiliated with both ACRIN andGOG, as well as be ACRIN accreditedfor PET/CT and MR imaging and havea recruited surgeon willing to followthe trial’s protocols for the removal ofthe patients’ lymph nodes followingimaging.
For future stages of the trial, inves-tigators will be looking for centers thatcan enroll a minimum of five cases peryear, said Dr. Atri. Once a site isapproved, its radiology principal inves-
tigator will undergo training in per-forming and interpreting ferumoxtran-10 MR imaging.
Dr. Gold said he is excited aboutthe start of the trial and welcomed radi-ologists’ participation. “This is mybrainchild,” he said. “I’ve worked sohard for seven to eight years to get it tothis point, so the more interest amongthe imaging community, the better.” ■■
■ Centers interested in participating in thetrial can go to www.acrin.org/6671_proto-col.html or contact ACRIN Project ManagerBernadine Dunning [email protected].
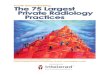
MR Using Ferumoxtran-10 Contrast MediumBenign internal iliac node in a patient with prostate cancer. (a) Precontrast axialT2-weighted gradient-echo MR image shows a small hyperintense left groin lymphnode (arrow). (b) Postcontrast image obtained 24 hours after ferumoxtran-10shows homogenous signal drop due to ferumoxtan-10 uptake indicating no malig-nant infiltration. Images courtesy Mukesh Harisinghani, M.D., Center for Molecular Imaging Research, Massachusetts General Hospital.
ba

12 R S N A N E W S A P R I L 2 0 0 7
Ankle MR Study ExemplifiesRole of Imaging in Diagnosisand Treatment
ANEW STUDY showing that MRimaging of the ankle improveddiagnostic confidence in more
than 70 percent of patients could bemore significant for those outside theradiology specialty than those within it,some radiologists said.
In a study led by Philip Bearcroft,M.D., and colleagues in the UniversityDepartment of Radiology at Adden-brooke’s Hospital in Cambridge, Eng-land, ankle MR changed managementplans for 35 percent of 91 orthopedicfoot and ankle patients. Findings werepublished in the November 2006 issue ofthe American Journal of Roentgenology.
The study results might seem obvi-ous at first glance, but there’s more toconsider, said Mark J. Kransdorf,M.D., a professor of radiology at theMayo Clinic College of Medicine andconsultant in the Department of Radi-ology at the Mayo Clinic in Jack-sonville, Fla.
“Those who have no exposure toankle imaging may not realize howimportant it is to patient management,”said Dr. Kransdorf. “To non-imagers,this information may not only be new,but may also help them make moreintelligent choices when assessing theirpatients.”
MR Influences Clinician ConfidenceWhile MR imaging is widely acceptedas an accurate diagnostic tool, therehave actually been few studies quanti-fying the effect of ankle MR on clini-cal diagnosis and patient management,said Dr. Bearcroft.
“We know we can obtain goodimages of the ankle and make accurate
diagnoses, but how do we know weactually make a difference to a referringclinician or even to a patient?” he asked.“The study was designed to determinewhether performing MR examinationsactually made a difference.”
The researchers studied 91 casesreferred from a single orthopedic footand ankle surgeon to a regional teach-ing hospital over an 18-month period,where diagnosis and proposed manage-ment were made before and after theMR imaging in each case. Measuringdiagnostic confidence with a visualanalog scale, researchers found MRimaging was “a useful tool of exclu-sion,” allowing the clinician to excludemany diagnoses that had been consid-ered before imaging. In addition, therewas an increase in diagnostic certaintywith which the remaining diagnoseswere made, with the number consid-ered “very likely” or “definite” increas-ing from 20 percent before imaging to88 percent afterward.
Mark E. Schweitzer, M.D., a pro-fessor of radiology and orthopedic sur-gery and chief radiologistat the New York Univer-sity Hospital for JointDiseases, said the study’ssignificance lies in illus-trating how imaging canchange a physician’s con-fidence in a diagnosis and, to somedegree, whether a person should go tosurgery.
“The holy grail of imaging is howit affects patient outcome,” said Dr.Schweitzer.
Prior to the use of MR imaging,patients in the study had an average of
2.3 possible diagnoses. After MRimaging, the number of diagnoses perpatient reduced to 1.2.
“In 69 percent of all diagnosesentertained before imaging, there was asignificant change in the confidencewith which they were considered afterimaging,” said Dr. Bearcroft.“Although in some cases the clinician
was considering thecorrect diagnosis priorto imaging, MR imag-ing increased confi-dence in that diagno-sis.”
The study does haveits limitations. Dr. Schweitzer noted itis difficult to separate the images fromthe interpretation. “It is hard to know ifthe MR images are what changed thesurgeon’s mind or if it was the inter-pretation of the radiologist,” he said.
The fact that diagnostic confidencechanged in more than two-thirds of
The holy grail of
imaging is how it affects
patient outcome.
Mark E. Schweitzer, M.D.
Philip Bearcroft, M.D.Addenbrooke’s Hospital
FEATURE MEDICINE IN PRACTICE

13R S N A N E W SR S N A N E W S . O R G
patients referred from a single experi-enced foot surgeon, said Dr. Bearcroft,demonstrates how difficult it is evenfor someone with great clinical experi-ence to differentiate between the vari-ous clinical entities that present withsimilar symptoms in the foot. In 66percent of the cases studied, he said,the referring physician felt that hisunderstanding of the disease had eitherdepended upon, or had been improvedby, MR imaging.
Of the 35 percent of patients forwhom MR imaging changed manage-ment plans, 31 percent ultimatelyunderwent a less invasive treatment.
Also of particular note, said Dr.
Bearcroft, is the fact that in the 34 per-cent of patients for whom MR imagingwas less helpful to the clinician, thepatients had symptoms of a meniscoidlesion—a condition that is difficult tosee on conventional MR.
More studies like this would bewelcome, said Dr. Schweitzer. “Theaudience for this kind of study isn’tnecessarily other radiologists. It shouldbe referring clinicians and otherproviders, because it will change howthey use radiology,” he said. ■■
Stress fracture in a 76-year-old man.Sagittal T1-weighted spin-echo MR image showsa subtle stress fracture (arrows) in the posteriorcalcaneus with prominent associated edema.Image courtesy of Mark J. Kransdorf, M.D.
ANOTHER ankle imaging study has revealeda high miss rate for a type of lateral
process talus fracture—an inversion and dorsi-flexion of the ankle also known as the “snow-boarder fracture”—that can cause chronicpain, nonunion and premature osteoarthritis.
Kevin Cunneely, M.D., and his colleaguesat the University of Utah in Salt Lake Citybegan their study after observing an inci-dence of lateral process talus fractures muchhigher than that indicated by the medical lit-erature, where they make up less than 1 per-cent of documented ankle injuries.
“We knew we were seeing more than thatand we were wondering if it was becausewe’re in Utah, which is snowboarding coun-try,” Dr. Cunneely said in a presentation atRSNA 2006.
Dr. Cunneely and colleagues retrospec-tively evaluated radiographs of ankle fracturesfrom a Level 1 trauma center over a three-year period. In cases where the researchersidentified lateral process fractures, they alsoreviewed CT and MR images—if available—to confirm their diagnoses.
Out of 1,480 radiographs of ankleinjuries, researchers found 130 lateral processfractures, an 8.8 percent incidence. Of these,48 (3.2 percent) involved the subtalar joint.
Twenty-seven cases also included CTimages, all of which confirmed the fractures.
Of 82 nonarticular fractures, 13 (16 per-cent) were properly diagnosed. Of 48 articu-
lar fractures, 34 (71 percent) wereproperly diagnosed. Fractures wereless likely to be recognized in sen-ior patients or in association withpilon and calcaneal fractures.
“We not only found that thistype of fracture occurred at ahigher rate than what was reportedin the literature, but also the missrate was significantly higher thanwhat was acceptable,” said Dr.Cunneely.
The significance of misdiagnosis dependson the degree of fracture. A Type 1 fracture,the least severe, is nonarticular. Types 2 and3 are articular and can result in intense,chronic pain and osteoarthritis. Prospectivediagnosis was poor for nonarticular fractures,said Dr. Cunneely, however, patient manage-ment is likely unaffected as the fractures aregenerally treated conservatively.
Of greater concern, he noted, was the missrate of 29 percent for articular fractures,given the high rate of chronic pain and pre-mature osteoarthritis associated with thoseinjuries.
Lateral process fracturesgenerally present as an anklesprain and can cause persist-ent pain. A variety of factorsis likely responsible for whythey are so commonly missed,said Dr. Cunneely, notingthat the fractures can be verysubtle and in some cases otherinjuries may distract fromtheir diagnosis.
Adding that the majorityof lateral process fractures studied could havebeen accurately diagnosed radiographically,Dr. Cunneely urged more care when diag-nosing ankle injuries and recommended theuse of CT.
Despite the “claim to fame” of lateralprocess talus injury as the “snowboarder frac-ture,” researchers concluded that the wintersport bias did not play a role in the higherincidence. They found that just 43 percentoccurred during the winter sport season,with the peak number of injuries occurringin June.
❚
Snowboarder Study Finds Common Ankle Fracture Often Missed
■ Note: This article was adapted from a story that appeared in the RSNA 2006 Daily Bulletin.The daily newspapers from the annual meeting are availableonline at RSNA.org/bulletin.■ To read the abstract of Dr. Cunneely's presentation, “High Incidence of Missed Diagnosisof a Common Ankle Fracture,” go to the RSNA Meeting Program at rsna2006.rsna.org. Thedirect link is rsna2006.rsna.org/rsna2006/V2006/conference/event_display.cfm?em_id=4434072.
Kevin Cunneely, M.D.
■ To read the abstract for "MRI of the Ankle:Effect on Diagnostic Confidence and PatientManagement," go to www.ajronline.org/cgi/content/abstract/187/5/1327.

14 R S N A N E W S A P R I L 2 0 0 7
RESEARCH & EDUCATION OUR FUTURE
Research & Education Foundation DonorsTHE Board of Trustees of the RSNA Research &
Education Foundation and its recipients ofresearch and education grants gratefully acknowl-edge the contributions made to the FoundationJan. 19 – Feb. 16, 2007.
Donors who achieve milestones with theircumulative giving are recognized through theFoundation’s Visionary Donor Program.
For more information on Foundation activi-ties, go to RSNA.org/foundation.
$1,500 – $4,999 Jhon & Jeffrey T. Hall, M.D.
$500 – $999Kim D. Burroughs, M.D.Nancy J. & Robert E. Campbell, M.D.In honor of Mrs. Alice FerrisIn memory of Mrs. Elizabeth MacEwanIn memory of Paul A. Riemenschneider, M.D.
Constance Whitehead & M. Paul Capp, M.D.In memory of George R. Barnes Jr., M.D.
Paul J. Friedman, M.D.Ann M. Lewicki, M.D.Mark S. Ridlen, M.D.
Donors who give $1,500 or more in the giving year qualify for membership in thePresidents Circle. Their names are shown in bold face.
$200 – $499Anton M. Allen III, M.D.Donald H. Altman, M.D.Saba & Muhammed S. Anwer, M.D.Ronald S. Arellano, M.D.Beatriz & Francisco A. Arredondo, M.D.Wynemia & James G. Arterburn, M.D.Raymond L. Baraldi Jr., M.D.Pauline Kwok, M.D. & James BartyzelChristian P. Behrenbruch, Ph.D.A. Oscar Beitia, M.D.Timothy A. Berka, M.D.Paul A. Bilow, M.D.Melinda H. Blue, M.D.Einat Blumfield, M.D. & Anthony BlumfieldA. Joseph Borelli Jr., M.D.Tommie & Morton A. Bosniak, M.D.Douglas C. Brown, M.D.Nancy L. Brown, M.D. & William M. BrownLisa & C. David Burtner, M.D.David W. Bynum, M.D.Danny Chang, M.D.Richard H. Christenson, M.D.Mary Mackiernan, M.D. & Robin D. ClarkAnn G. Archer, M.D. & Anderson CobbTeresa Castillo & Marco A. Corres, M.D.Andres O. Crame, M.D.James M. Crotty, M.D.Francisco De La Cruz, M.D.Luis Donoso-Bach, M.D.Dakir L. Duarte, M.D.Evelyn & Jerome Dubowy, M.D.Melissa & Robert R. Edelman, M.D.Erwin H. Engert Jr., M.D.Celeste & Glenn Forbes, M.D.Alan S. Friedman, M.D.Elizabeth Orvoen-Frija, M.D. & Guy Frija, M.D.
Connie J. Gapinski, M.D., Ph.D.Brigid M. Gerety, M.D.Vishan L. Giyanani, M.D.Marc J. Gollub, M.D.Jack A. Goode, M.D.Stefaan Gryspeerdt, M.D.Richard F. Grzybowski, D.O.William A. Guyette, M.D.William J. Halden Jr., M.D.William S.C. Hare, M.D.Jeffrey M. Hartwick, M.D.Anita E. Hawkins, M.D.Charles I. Heller, M.D.Todd M. Hertzberg, M.D.Helen M. Higgins-Minetti, M.D.
Leo Hochhauser, M.D.Alan D. Hoffman, M.D.Clara & Bentley A. Hollander, M.D.Sachiko & Zenichiro Hombo, M.D.Robert S. Isaacs, M.D.Miyuki & Keiichi Ishigame, M.D., Ph.D.Ashok B. Jain, M.D.Russell Karp, M.D.James A. Kenney Jr., M.D.Sukehiko Koga, M.D.Anthony L. Kudirka, M.D.Yen-Zen Kuo, M.D.Colleen & Roby Lal, D.O.Patricia Silva, M.D. & Richard E. Latchaw, M.D.
Henri E.A.S.J. Lemmers, M.D.Ellen & Robert M. Lerner, M.D.Luc M. Linster, M.D.Deborah G. Longley, M.D.Danielle Bajakian & Robert A. Lookstein, M.D.
Angelique & James L. Lowry, M.D.Robert L. Mac Carty, M.D.Angela & David R. Marcantonio, M.D.Kristin & Jeffrey S. McClellan, M.D.Mona & Brian D. Meagher, M.D.Christopher J. Mehall, M.D.Mehran Midia, M.D.Elizabeth & Michael T. Miller, M.D.John J. Molitor Jr., M.D.Shelly & Arthur L. Mulick, M.D.Susan A. Mulligan, M.D. & Mark J. Mulligan, M.D.
Yarisis Rosa & Gil M. Narvaez-Soto, M.D.Wafa & Richard W. Naufal, M.D.Antonio Nelson, M.D.Andrew S. Novick, M.D.Michelle & Richard R. Ozmun Jr., M.D.Tatjana Pavlovic, M.D. & Zivojin Pavlovic, M.D.
Thomas W. Peltola, M.D.Rebecca G. Pennell, M.D.Sophia B. Peterman, M.D., M.P.H.William R. Pfeiffer, M.D.Sarah G. Pope, M.D.Judith & Niels Powell, M.D.Michelle & Kurian J. Puthenpurayil, M.D.Michael F. Quinn, M.D.Francisco J. Rita, M.D.Ronald P. Robinson, M.D.George I. Rosenberg, M.D.Tsuneo Saga, M.D.Sadayuki Sakuma, M.D., Ph.D.Guillermo Ruben Sanchez, M.D.Jose Carlos Sanchez, M.D.Satoshi Sawada, M.D.Andrew H. Shaer, M.D.Rajul D. Shah, M.D.Patricia Silva, M.D.Jesse B. Smith, M.D.Becky & Gregory B. Smith, M.D.Lori Verdol Smithson, M.D.Martin Steinhoff, M.D.Gill M. Taylor-Tyree Sr., M.D.Peggy & Michael S. Tenner, M.D.W. Phillips Tinkler, M.D.Bruce S. Turlington, M.D.Rommel G. Villacorta, M.D.Sony Chong & Kao-Lun Wang, M.D.Katherine & Ralph P. Wells, M.D.Liva Andrejeva-Wright, M.D. & David WrightMasashi Yamashiro, M.D.
Stanley Yang, M.D.Huei-mei & Wen C. Yang, M.D.
$199 OR LESSAnnie & Mitchell D. Achee, M.D.Michael D. Ames, M.D.Teresa & Thomas M. Anderson, M.D.Ronald C. Arildsen, M.D.Gunter J. Augustin, M.D.Katherine & Craig M. Banull, M.D.Gerald R. Berg, M.D.Mary & James P. Blakely, M.D.Richard D. Borden, M.D.Marcos P.F. Botelho, M.D.Karen T. Brown, M.D.Joel A. Budin, M.D.Kathran Moy Chan, M.D.Kyung Ae Lee & Samuel Chang, M.D.Hsiu-Chien Tsui & Chin-Yu Chen, M.D.Joseph M. Chin, M.D.Toby & Allen J. Cohen, M.D., Ph.D.Mary E. Cunnane, M.D.Anil Kumar Dasyam, M.D.Adam J. Davis, M.D.Charles J. DeMarco, M.D.Gustav Dietrich, M.D.Jonathan D. Dodd, M.D.David J. Dowsett, M.Sc., Ph.D.Kathryn A. Draves, M.D.Paul E. Dybbro, M.D.Steven M. Eberly, M.D.Tova & James P. Eisenberg, M.D., Ph.D.Iyabo & Anthony U. Eka, M.B.B.S.Susan W. Fan, M.D.Ana Cristina & Renato Campos Soares de Faria, M.D.
Angela J. Feyerabend, M.D.Anna K. Rusztyn-Fitz & Charles R. Fitz, M.D.
Susan & James D. Fraser, M.D.Judith & G. Donald Frey, Ph.D.James T. Friedland, M.D.Akira Fujikawa, M.D.Noor Gajraj, M.D.Simona Gaudino, M.D.Peter W. Gendall, M.D.Ronald B.J. Glass, M.D.Adam M. Gray, M.D.W. Lawrence Greif, M.D.Jim Greve, M.D.Angelyn Gunn, M.D.Munetaka Haida, M.D., Ph.D.Neil J. Halin, D.O.Susan Hattori-Oyama, M.D.Wang He, M.D.Alison & Hayden W. Head III, M.D.Kathy Golucke-Heredia & Sergio L. Heredia, M.D.
Brian J. Holloway, M.B.B.Ch.Abi Raymer & Brooks A. Horsley, M.D.Laura A. Hotchkiss, M.D. & Bruce L. Hotchkiss
Nancy & John R. Howard, M.D.Connie & George F. Hromyak Jr., M.D.Steffen Huber, M.D.Andrew J. Hwang, M.D.Vasavi Rajagopal & Saravanan Kasthuri, M.D.
Satomi Kawamoto, M.D.Nadine Koff, M.D. & David A. Koff, M.D.Cynthia Reese & Keith Y. Kohatsu, M.D.
Eli Konen, M.D.Elizabeth & Jay L. Korach, M.D.Madonna L. Kral, M.D.Andrew Ku, M.D.Shawn L. Laferriere, D.O.Phyllis & Philip H. Lapidus, M.D.Claudia A. Lawn, M.D.Maximiliano R. Lloret, M.D.Giselle Alvarez de la Campa & Fernando J. Lopez, M.D.
Manuel A. Madayag, M.D.David C. Madoff, M.D.Mary T. & Melvin A. Magidson, M.D.Fanny E. Moron, M.D. & Carlos MartinezDiane & Robert A. Maxey, M.D.Valdemar Moreno-Ford, M.D.Richard P. Moser III, M.D.Kristine M. Mosier, D.M.D., Ph.D.Erika Kim, M.D. & Andreas MuellerLuigi Natale, M.D.Thelma J. & Luther S. Nelson, M.D.Fukiat Ongseng, M.D.Susanj S. Patel, M.D.Christine L. Petersen, M.D.Cheryl A. Petersilge, M.D.Francisco Plancarte, M.D.Jeffrey S. Pollak, M.D.Ilias Primetis, M.D.Lorentz G. Quekel, M.D., Ph.D.Steven S. Raman, M.D.Magdalena Ramirez Arellano, M.D.Maurice M. Reeder, M.D.Frank M. Rembert, M.D.Jan Rijkmans, M.D.Roberto Rivera, M.D.Robert B. Roach, M.D.Klaus Ruedisser, M.D.Yoko Saito, M.D.Aram Salem, M.D.Jerome M. Sampson, M.D.Sergio De Los Santos Sanchez, M.D.Mark J. Sands, M.D.Michael F.H. Schocke, M.D.Chunilal P. Shah, M.D.James H. Short, M.D., Ph.D.Andreas F. Siraa, M.D.Keith M. Spellman, M.D.Susan G. & Richard J. Sukov, M.D.Karen & Michael A. Sullivan, M.D.David C. Swanson, M.D.Yu Ming Tang, M.B.B.S.Sayuri & Noboru Tanigawa, M.D.Catherine & Bernard L. Tassin, M.D.Satoru Tazawa, M.D.Serge Tcheng, M.D.Renate Tewaag, M.D.Panagiotis V. Tsirkinidis, M.D.Giuseppe Vadala, M.D.Michael E. Waldman, M.D.Ivy M. Warsinski, M.D.Edward C. Wheeler, M.D.Rodrick A. Williams, M.D.Michael A. Winkler, M.D.Masaki Yamamuro, M.D.Kan Ying, M.D.Shigeyuki Yoshida, M.D.

15R S N A N E W SR S N A N E W S . O R G
Imaging Prostate Cancer: AMultidisciplinary Perspective
AS THE longstanding role of imagingin assessing prostate cancer
becomes ever more important in guid-ing treatment selection and planning,there still exists no consensus regardinguse of the many modalities available.
In an article inthe State of theArt section of the April issue of Radiol-ogy (RSNA.org/radiologyjnl), HedvigHricak, M.D., Ph.D., of MemorialSloan-Kettering Cancer Center in NewYork, and colleagues provide a multi-disciplinary perspective on the optimalrole of imaging in the detection andstaging of prostate cancer, as well as intreatment planning and follow-up.
Specifically, Dr. Hricak and col-leagues offer comprehensive, evidence-based explanations of the followingmodalities:• Transrectal ultrasonography• CT• MR, including dynamic contrast-
enhanced MR and MR spectroscopy• Radionuclide bone scanning• Positron emission tomography (PET)
Noting the substantial progressalready made in imaging prostate can-cer, Dr. Hricak and colleagues con-clude, “It is hoped that advances in
imaging, and future advances in molec-ular imaging, will contribute to long-term improvements in morbidity fromprostate cancer and patients’ quality oflife and to a decrease in mortality fromprostate cancer that we are now justbeginning to see.”
Journal HighlightsThe following are highlights from the current issues of RSNA’s twopeer-reviewed journals.
RSNA JOURNALS
PET/CT scans of osseous metastasis in the posterior element ofthoracic spine. (a) Coronal fluorodeoxyglucose positron emission tomography (FDG PET) scanshows focal increased activity in left posterior spine (arrow). (b) TransversePET/CT overlay scan shows that focal lesion corresponds to metabolically activebone metastasis in the posterior vertebra (arrow).(Radiology 2007; 243:28–53) © RSNA, 2007. All rights reserved. Printed with permission.
ba
RSNA Members Enjoy Journals, Annual MeetingFree subscriptions to Radiology and RadioGraphics andattending the annual meeting free of charge are themost valuable RSNA benefits, according to membersresponding to a recent RSNA survey.Relative Value of Select RSNA Services1 Radiology subscription2 RadioGraphics subscription3 Annual meeting4 Access to continuing medical education5 Educational products6 Free access to self-assessment modules7 RSNA News8 Discounted admission to educational courses
held outside annual meeting9 Career Connection
10 CME Credit RepositorySource: 2006 RSNA Member Needs Assessment Survey
Proto Participates in ECR Editors ForumRadiology EditorAnthony V. Proto,M.D., (right) joinedRobert J. Stanley,M.D., (left), editor-in-chief of theAmerican Journalof Roentgenology,and Albert L.Baert, M.D., Ph.D.,editor-in-chief ofEuropean Radiol-ogy, for “Ask the Editors: Discuss Your Most Burning Questionsand Problems,” a forum held during the European Congress ofRadiology (ECR) last month in Vienna, Austria. Among the issuesaddressed by the editors were duplicate submissions and qualityof research.
© ES
R -
Euro
pean
Soc
iety
of
Radi
olog
y /
Har
ry S
chif
fer

16 R S N A N E W S A P R I L 2 0 0 7
RSNA JOURNALS
WITH THE use of bone marrow transplantation
continually on the rise, radiolo-gists must know how to useultrasonography, CT and MRto detect a range of potentialcomplications.
Described in an article inthe March-April issue ofRadioGraphics (RSNA.org/radiographics) are the basicprinciples of and indicationsfor pediatric bonemarrow transplan-tation, the range of potentialclinical complications and theimaging manifestations ofthose complications. Specifi-cally, lead author Daniel S.Levine, M.B.Ch.B., of the Hos-pital for Sick Children andUniversity of Toronto, and col-leagues address the followingcomplication types:• Pulmonary, including intersti-
tial pneumonitis
• Abdominopelvic, includinggraft-versus-host disease
• Musculoskeletal, includingchronic atrophy of subcuta-neous tissues
• Central nervous system,including intraparenchymaland intraocular hemorrhage
• Paranasal, including sinusitis “The increasing use of
bone marrow transplantation totreat a range of malignant and
nonmalignantconditions man-
dates that radiologists be famil-iar with the range of potentialcomplications and the associ-ated imaging appearances,” Dr. Levine and colleagues con-clude.
Imaging the Complications of Bone MarrowTransplantation in Children
Invasive fungal sinusitis in a 6-year-old girl,three months after bone marrow transplantationfor aplastic anemia.(a) Axial CT image shows bilateral maxillary sinus opacifica-tion, complete on the left, and premalar soft-tissue swellingand infiltration. (b) Axial CT image shows periorbital soft-tissue swelling and a subperiosteal abscess (arrow) withdestruction of the orbital plate of the ethmoid bone.(RadioGraphics 2007;27:307-324) © RSNA, 2007. All rights reserved. Printed with permission.
EDUCATION RESEARCH
Program and Grant Announcements
Continued on page 20
b
a
This article meets the criteria for1.0 AMA PRA Category 1 Credit™.
Revitalizing the Radiology Research EnterpriseApplication Deadline Extended Through April 23
RSNA is accepting applications for theRevitalizing the Radiology ResearchEnterprise (RRRE) program site visitsto evaluate the departmental and insti-tutional research environment. TheRRRE program is designed to help aca-demic radiology and radiation oncologydepartments improve their ability tosupport and conduct radiologic
research. Six depart-ments will be selectedfrom applications madeby departments of radiology, radiationoncology and nuclear medicine.
In addition, a 1½ day workshop tobe held Oct. 19–20 at RSNA Headquar-ters in Oak Brook, Ill., will focus onchallenges to and strategies for con-
ducting research in radi-ology and radiationoncology departments.
For more information, contact TracySchmidt, M.S., at [email protected] 1-630-368-3751.

17R S N A N E W SR S N A N E W S . O R G
RSNA JOURNALS
Press releases have been sent to the medical news media for the following articlesappearing in the April issue of Radiology (RSNA.org/radiologyjnl):
in Public Focus
Portal Vein Embolizationand Autologous CD133+
Bone Marrow Stem Cellsfor Liver Regeneration:Initial Experience
COMBINING portal vein embolization(PVE) and intraportal somatic stem
cell application can significantly improvehepatic regeneration prior to extendedliver resection, reducing time to surgeryin patients with extensive hepatictumors, German researchers have found.
Günter Fürst, M.D., and colleaguesat Heinrich-Heine-University of Dues-seldorf found that six patients treatedwith PVE and CD133+ bone marrowstem cells (BMSCs) experienced atwofold higher average daily hepaticgrowth rate than seven patients whounderwent PVE alone. This resulted in areduction of the time to surgery by anaverage of 18 days.
For almost half of patients requiringextended hepatectomy, an anticipatedfuture liver remnant volume (FLRV)below 25 percent of total liver volumeposes an increased risk of postoperativemorbidity and mortality, Dr. Fürst andcolleagues note.
“Recent progress in stem cellresearch and cell transplantation spurred
our attempt to augment preoperativeliver regeneration and shorten the timeto sufficient expansion of the FLRV,”they state, adding that they choseCD133+ stem cells based on their
hepatic capacity as demonstrated inprevious studies.
Transverse CT scans from patient with hepatocellular carcinoma (black arrow)obtained (a) before and (b) 14 days after portal vein embolization (PVE) and intra-portal CD133+ bone marrow stem cell (BMSC) application. (a) Preinterventional CTvolumetry revealed total liver volume of 1317 mL, tumor volume of 177 mL andfuture liver remnant volume (FLRV) of 217 mL (white arrows). Preoperative relativeleft lateral liver volume ratio was 19 percent. (b) Postinterventional CT volumetryrevealed marked hypertrophy of segments II and III (white arrows), indicated byFLRV of 440 mL, preoperative relative left lateral liver volume ratio of 39 percent,relative gain of 103 percent and hepatic daily gain rate of 15.9 mL/d.(Radiology 2007;243:171–179) © RSNA, 2007. All rights reserved. Printed with permission.
LUNG radiofrequency (RF) ablationimproves survival and local tumor
control outcomes in patients whosecases are unsuitable for surgery,according to a new study.
Caroline J. Simon, M.D., and col-leagues at Brown Medical School/
Rhode Island Hospital in Providenceretrospectively evaluated 153 patientswho underwent percutaneous CT-guided lung tumor RF ablations andfound:• Overall long-term survival rates for
stage I non-small cell lung cancer
(NSCLC) were 78 percent at oneyear, 57 percent at two years, 36 per-cent at three years and 27 percent atfour and five years.
• Overall long-term survival rates forstage IV colorectal lung metastases
Pulmonary Radiofrequency Ablation: Long-term Safety and Efficacyin 153 Patients
Continued on next page
ba

were 87 percent at one year, 78 per-cent at two years and 57 percent atthree, four and five years.
• Local tumor progression-free rates fortumors 3 cm or smaller were 83 per-cent at one year, 64 percent at two
years, 57 percent at three years and47 percent at four and five years. Fortumors larger than 3 cm, rates were45 percent at one year and 25 percentat two, three, four and five years.
“Surgery is usually the treatment ofchoice for localized cancers, but only
20 percent of all NSCLCs diagnosedare suitable for potentially curativeresection,” the researchers note.(Radiology 2007;243:268-275) © RSNA, 2007.All rights reserved. Printed with permission.
18 R S N A N E W S A P R I L 2 0 0 7
Media Coverage of Radiology
IN February, media outlets carried 333news stories generated by articles
appearing in Radiology. These storiesreached an estimated 57 million people.
News releases promoted findingsfrom Radiology studies on intracranialhemorrhage in babies after vaginalbirth (Radiology 2007;242:535-541)and contrast-enhanced MR angiogra-phy for assessment of the supra-aorticarteries (Radiology 2007;242:600-609).In addition, a special news release wasissued to draw attention to an editorialon the possible association betweenMR contrast agents and nephrogenicsystemic fibrosis (Radiology2007;242:647-649).
Coverage highlights include print
placements in the Washing-ton Post, Los Angeles Times,Seattle Times, Kansas CityStar, South Florida Sun-Sen-tinel, Fort Worth Star-Telegram, Lexington HeraldLeader, Augusta (Georgia)Chronicle , MontereyCounty (California) Herald,The Capital (Annapolis,Md.) and The News &Observer (Charlotte, N.C.), as well asthe Canadian publications VancouverSun, Calgary Herald, Edmonton Jour-nal and Montreal Gazette.
Broadcast placements includenumerous stories on regional televisionstations including KNBC-TV (Los
Angeles), WMAQ-TV (Chicago),WBAL-TV (Balti-more), KUSA-TV(Denver), WFSB-TV(Hartford, Conn.),WCCO-TV (Min-neapolis), KING-TV(Seattle), WKYC-TV(Cleveland), WFLA-TV (Tampa, Fla.) and
KSDK-TV (St. Louis). Prominent Webplacements include Yahoo! News,MSNBC.com, forbes.com, latimes.com,washingtonpost.com, abcnews.com andboston.com.
RSNA JOURNALS
Pulmonary Radiofrequency Ablation: Long-term Safety and Efficacyin 153 PatientsContinued from previous page
CT Screening for Lung Cancer: Diagnoses Resulting from the New YorkEarly Lung Cancer Action Project
ANNUAL CT screening for lung cancerresults in the identification of a
high proportion of patients with early-stage lung disease, according to a newreport by the New York Early LungCancer Action Project (NY-ELCAP).
Led by Principal Investigator Clau-dia I. Henschke, Ph.D., M.D., 21 inves-tigators at 12 institutions throughoutNew York State conducted 6,295 base-line and 6,014 annual repeat screenings.The study was an expansion of theEarly Lung Cancer Action Project con-ducted at two institutions in New YorkCity.
With diagnostic work-up recom-mended for participants with positiveresults at baseline or repeat screenings,101 lung cancer diagnoses were madeat initial screening and 20 at repeat.Diagnoses in three other participantswere prompted by symptoms before thefirst scheduled repeat screening.
The researchers note that a highproportion of patients had no clinicalevidence of metastases when biopsywas recommended in the baseline andrepeat screenings.
The findings also illustrate the ben-efit of updating the ELCAP screening
regimen to take advantage of techno-logical advances, Dr. Henschke andcolleagues note. “In particular, ourfindings showed the importance ofupdating the definition of a positiveresult to accommodate the finer colli-mation provided by multidetector rowCT and the improved potential forinterpretation with high-resolutionmonitors,” they write.(Radiology 2007;242:239-249) © RSNA, 2007.All rights reserved. Printed with permission.

19R S N A N E W SR S N A N E W S . O R G
RSNA MEMBER BENEFITS
Working For YouRSNA CommitteesRSNA News continues its series highlighting the work of RSNA’s volunteer commit-tees with a look at the new International Advisory Committee. The committee cur-rently includes 10 international representatives from five continents.
International Advisory Committee
THE International Advisory Committeeadvises the RSNA Board of Directors on theimpact that Society activities and programs
have on international membersand attendees at the annual meet-ing. The committee also offers aninternational perspective on RSNA publications,governance and both traditional and Web-basededucational programs. In addition, the committeehelps guide the promotion of Society member-ship internationally.
At their first meeting at RSNA 2006, com-mittee members pledged to help identify candi-dates for RSNA’s editorial boards and commit-
tees and international faculty forrefresher courses. The committeealso addressed travel and lodging
issues for international annual meeting attendees.The chair of the committee is Christian J.
Herold, M.D., of Vienna, Austria.
Christian J. Herold, M.D.
Working for youCOMMITTEE PROFILE
MOC File Added to RSNA MOC ResourcesThe MOC File is the latest serviceoffered by the RSNA Education Centerto assist members in meeting mainte-nance of certification (MOC) require-ments.
Available at RSNA.org/education/MOC, the MOC File gives RSNA
members a central loca-tion to store electronicdocuments, such as aCME action plan, pertaining to theirpersonalized MOC program.
Other services that help membersfulfill MOC requirements as designated
by the AmericanBoard of Radiol-ogy (ABR) are
also available online. They include self-assessment modules (SAMs), My Prac-tice Profile, My CME Action Plan andthe RSNA CME Credit Repository.
RSNA Attends ECRExecutive Director Dave Fellers, C.A.E., (left),and 2007 President R. Gilbert Jost., M.D.,were among the RSNA representatives onhand when the Society’s new booth premieredat the European Congress of Radiology lastmonth in Vienna, Austria. People interestedin RSNA could talk with representatives andobtain informational materials at the booth,which features a plasma screen displayingSociety facts and images as well as a com-puter terminal where visitors may explorebenefits offered at RSNA.org.
Radiology Editor Anthony V. Proto, M.D.,also answered booth visitors’ questions aboutarticle submissions and other aspects of thejournal.
The booth’s next stop will be the GermanCongress of Radiology, May 16–19 in Berlin.
If you have a colleague who would like to become an RSNA member, you can download an application at RSNA.org/mbrapp or contact the RSNA Membershipand Subscriptions Department at 1-877-RSNA-MEM [776-2636] (U.S. and Canada), 1-630-571-7873 or [email protected].

20 R S N A N E W S A P R I L 2 0 0 7
Tools for Success in the Practice of RadiologyJune 29–30 • RSNA Headquarters in Oak Brook, Ill.
This customized, interactive seminarfeaturing sessions on leadership, plan-ning, staff development and quality andsafety will help participants confidentlymanage day-to-day issues on the job. Claire E. Bender,M.D., of the Mayo Clinic College of Medicine in Rochester,Minn., is directing the course. Moreinformation is available atRSNA.org/education/RSNA_shortcourses.cfm or by callingthe RSNA Education Center at 1-800-381-6660 x7772.
EDUCATION RESEARCH
Program and Grant Announcements
Online RegistrationNow Open
RSNA Outstanding Researcher and Educator AwardsNomination deadline–June 15
The 2007 RSNA Outstanding Researcher and OutstandingEducator awards will honor one senior physician or scientistin each award category who has made a career of significantcontributions to the field of radiology or radiologic sciencesthrough research or teaching/education.
To nominate an individual for one of these awards, senda letter of nomination and one or more corroborating lettersof support, along with the nominee’s complete curriculumvitae, to Scott Walter, M.S., Senior Manager, Grant Adminis-tration, at [email protected]. More details are available atRSNA.org/Foundation/RecognitionAwards.cfm.
Continued from page 16
Eighty exhibitor personnel representing 56 companiesmet with RSNA staff in March to learn about 2007exhibiting rates and exhibit floor plans, as well as rulesand regulations and deadlines.
RSNA TechnicalExhibit ServicesManager JohnJaworski (left) talkswith Diane Wilhelmof Berlex Laborato-ries at the planningmeeting. Behindthem are floor plansfor the RSNA 2007technical exhibition.
Exhibitors Prepare for RSNA 2007
EXHIBITOR NEWS RSNA 2007
Sponsored by RSNA,the American RoentgenRay Society (ARRS)and Association of Uni-versity Radiologists
(AUR), this programdemonstrates the impor-tance of research in
diagnostic radiology,illustrates the excite-ment of research careersand introduces residentsto successful clinical
radiologyresearchers. Suc-
cessful applicants willbe assigned to either aseminar held during
RSNA 2007 or theARRS annual meetingin 2008. Radiologydepartments are invitedto nominate one second-year resident. Eightyresidents will beselected to participate.
Advanced Course in Grant WritingApplication Deadline – July 1
This course helps junior faculty membersprepare and submit a National Institutesof Health, National Science Foundationor equivalent grant application. Thecourse will consistof four two-day sessions at RSNA Headquarters in OakBrook, Ill., over a nine-month periodbeginning in September 2007.
More information about these programs, including applications, isavailable at RSNA.org/research/educational_courses.cfm.
RSNA/AUR/ARRS Introduction to Research ProgramApplication Deadline – July 15

21R S N A N E W SR S N A N E W S . O R G
MEETING WATCH RSNA 2007
News about RSNA 2007
Important Dates for RSNA 2007April 15 Abstract submission deadlineApril 23 RSNA/AAPM member registration and
housing opensMay 21 Non-member registration and housing opensJune 18 Course enrollment opensNov. 5 Final advance registration, housing and
course enrollment deadlineNov. 25–30 RSNA 93rd Scientific Assembly and Annual
Meeting
Registration FeesBY 11/5 ONSITE
$0 $100 RSNA Member, AAPM Member
$0 $0 Member Presenter
$0 $0 RSNA Member-in-Training, RSNA Student Member and Non-Member Student
$0 $0 Non-Member Presenter
$130 $230 Non-Member Resident/Trainee
$130 $230 Radiology Support Personnel
$620 $720 Non-Member Radiologist, Physicist or Physician
$620 $720 Hospital or Facility Executive, Commercial Research andDevelopment Personnel, Healthcare Consultant, Industry Personnel
$300 $300 One-day registration to view only the Technical Exhibits area
For more information about registering for RSNA 2007, visit RSNA2007.RSNA.org, e-mail [email protected] or call 1-800-381-6660 x7862.
RSNA President Welcomes Attendeesin Online VideoHear 2007 RSNA PresidentR. Gilbert Jost, M.D.,describe the plethora ofopportunities available at theRSNA annual meeting in ashort welcome video postedat RSNA2007.RSNA.org.
Advance Registrationand Housing OpensApril 23, BrochureAvailable RSNA 2007 advance registrationand housing opens April 23 forRSNA and AAPMmembers. Non-mem-ber registration andhousing opens May 21.
The Advance Reg-istration and Housingbrochure will be avail-able in electronic for-mat only. Go to RSNA.org/regis-ter and click on the PDF file.
International VisitorsApply Early for Your Visa
Personalized invitation letters are availableat RSNA2007.RSNA.org. Click on Interna-tional Visitors, a section of the annual meet-ing Web site that also includes importantinformation about visa applications. Visaapplicants are advised to apply as soon asthey decide to travel to the United Statesand at least three to four months in advanceof their travel date. It is recommended thatinternational visitors start the visa processnow. For more information go to:• www.unitedstatesvisas.gov• travel.state.gov/visa• nationalacademies.org/visas
Also, as part of the Western Hemi-sphere Travel Initiative (WHTI), theU.S. government is now enforcing newpassport requirements for all air travelersentering or re-entering the United Statesfrom Canada, Mexico, Central and SouthAmerica, the Caribbean and Bermuda.
Information is available at: • www.dhs.gov• travel.state.gov/travel/cbpmc/cbpmc_
2223.html• www.getapassportnow.com/
Registering for RSNA 2007There are four ways to register for RSNA 2007:
➊ InternetGo to RSNA.org/register. Use yourmember ID number from the RSNA News label ormeeting flyer sent to you. If you have questions,send an e-mail to [email protected].
➋ Fax (24 hours)1-800-521-60171-847-940-2386➌ Telephone (Monday–Friday, 8:00 a.m.–5:00 p.m. CT)1-800-650-70181-847-940-2155
➍ MailExperient/RSNA 2007108 Wilmot Rd., Suite 400Deerfield, IL 60015-5124USA
Fastest wayto register!

22 R S N A N E W S A P R I L 2 0 0 7
8:30 AM 9:00 AM 9:30 AM 10:00 AM 10:30 AM 11:00 AM 11:30 AM 12:00 PM 12:30 PM 1:00 PM
8:30 AM 9:00 AM 9:30 AM 10:00 AM 10:30 AM 11:00 AM 11:30 AM 12:00 PM 12:30 PM 1:00 PM
8:30 AM 9:00 AM 9:30 AM 10:00 AM 10:30 AM 11:00 AM 11:30 AM 12:00 PM 12:30 PM 1:00 PM
8:30 AM 9:00 AM 9:30 AM 10:00 AM 10:30 AM 11:00 AM 11:30 AM 12:00 PM 12:30 PM 1:00 PM
8:30 AM 9:00 AM 9:30 AM 10:00 AM 10:30 AM 11:00 AM 11:30 AM 12:00 PM 12:30 PM 1:00 PM
8:30 AM 9:00 AM 9:30 AM 10:00 AM 10:30 AM 11:00 AM 11:30 AM 12:00 PM 12:30 PM 1:00 PM
8:30 AM 9:00 AM 9:30 AM 10:00 AM 10:30 AM 11:00 AM 11:30 AM 12:00 PM 12:30 PM 1:00 PM
Sunday11/25
Saturday11/24
Effective Retirement Plans and Distribution Strategies PS01
AAPM/RSNA Physics Tutorial for Residents PS10
Opening Session PS30 Scientific Sessions SSA
Oncodiagnosis Panel PS31
Radiologist Assistants Program RA11
Pediatric Radiology Series VP11
Refresher Courses RC200s
Refresher Courses RC300s
Associated Sciences Refresher Course AS31
Essentials Course ES31
Associated Sciences Refresher Course AS32
Essentials Course ES32
Quality Improvement Program QI31 Quality Improvement Program QI32
Pediatric Radiology Series VP31
Refresher Courses RC500s
Associated Sciences Refresher Course AS41
Case-based Review: Pediatrics CP41
Essentials Course ES41
Molecular Imaging Program MI41 Molecular Imaging Program MI42
Scientific Sessions SSK
Associated Sciences Refresher Course AS42
Case-based Review: Pediatrics CP42
Essentials Course ES42
Musculoskeletal Radiology Series VS41
Refresher Courses RC600s
Refresher Courses RC800s Scientific Sessions SST
Case-based Review: MR CM51
Scientific Sessions SSQ
Case-based Review: MR CM52
Scientific Sessions SSG
Scientific Sessions SSC
Associated Sciences Refresher Course AS21 Associated Sciences Refresher Course AS22
Case-based Review: Neuroradiology CN21 Case-based Review: Neuroradiology CN22
Case-Based Review: Interventional Radiology CI31 Case-Based Review: Interventional Radiology CI32
Gastrointestinal Radiology Series VG31
Neuroradiology Series VN31
Gastrointestinal Radiology Series VG21
Musculoskeletal Radiology Series VS21
Pediatric Radiology Series VP21
Mentored Cardiac CT Case Review
Monday11/26
Tuesday11/27
Wednesday11/28
Thursday11/29
Friday 11/30
Radiologist Assistants Program RA12 Radiologist Assistants Program RA13
PlenarySessions
RefresherCourses
MultisessionCourses
Special FocusSessions
ScientificSessions
Programs Key
BOOST RO21 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO22 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO31 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO32 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO41 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO42 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO51 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO52 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
Lunch, Visit Posters, Education Exhibits & Technical ExhibitsTechnical Exhibit HoursSun. – Wed. 10:00 AM – 5:00 PMThursday 10:00 AM – 2:00 PM
Lakeside Learning Center HoursSunday 8:00 AM – 6:00 PMMon. – Thu. 7:00 AM – 10:00 PMFriday 7:00 AM – 12:45 PM
MEETING WATCH RSNA 2007 ■ PRELIMINARY PROGRAM

23R S N A N E W SR S N A N E W S . O R G
1:00 PM 1:30 PM 2:00 PM 2:30 PM 3:00 PM 3:30 PM 4:00 PM 4:30 PM 5:00 PM 5:30 PM 6:00 PM
1:00 PM 1:30 PM 2:00 PM 2:30 PM 3:00 PM 3:30 PM 4:00 PM 4:30 PM 5:00 PM 5:30 PM 6:00 PM
1:00 PM 1:30 PM 2:00 PM 2:30 PM 3:00 PM 3:30 PM 4:00 PM 4:30 PM 5:00 PM 5:30 PM 6:00 PM
1:00 PM 1:30 PM 2:00 PM 2:30 PM 3:00 PM 3:30 PM 4:00 PM 4:30 PM 5:00 PM 5:30 PM 6:00 PM
1:00 PM 1:30 PM 2:00 PM 2:30 PM 3:00 PM 3:30 PM 4:00 PM 4:30 PM 5:00 PM 5:30 PM 6:00 PM
1:00 PM 1:30 PM 2:00 PM 2:30 PM 3:00 PM 3:30 PM 4:00 PM 4:30 PM 5:00 PM 5:30 PM 6:00 PM
1:00 PM 1:30 PM 2:00 PM 2:30 PM 3:00 PM 3:30 PM 4:00 PM 4:30 PM 5:00 PM 5:30 PM 6:00 PM
AAPM/RSNA Physics Tutorial on Equipment Selection PS20
Real Estate Investments PS11
NIH Grantsmanship Workshop PS12
Refresher Courses RC100s Image Interpretation Session PS40
Pediatric Radiology Series VP12
RSNA/NCI Interventional Oncology Series
Associated Sciences Refresher Course AS33
Essentials Course ES33
Quality Improvement Program QI33 Quality Improvement Program QI34
Pediatric Radiology Series VP32
RSNA/NCI Interventional Oncology Series
RSNA/NCI Interventional Oncology Series
Imaging Symposium PS90
Molecular Imaging Program MI43 Molecular Imaging Program MI44
Annual Oration in Radiation Oncology PS70 Scientific Sessions SSM Special Focus Sessions SFN
Case-based Review: Pediatrics CP43
Essentials Course ES43
Case-based Review: Pediatrics CP44
Essentials Course ES44
RSNA/AAPM Symposium PS80 Special Focus Sessions SFS Refresher Courses RC700s
Case-based Review: MR CM53 Case-based Review: MR CM54
Scientific Sessions SSJ Refresher Courses RC400s
Associated Sciences Refresher Course AS34
Essentials Course ES34
New Horizons Lecture PS50
AAPM/RSNA Basic Physics Lecture for the RT PS51
Annual Oration in Diagnostic Radiology PS60
Scientific Sessions SSE Special Focus Sessions SFF
Associated Sciences Refresher Course AS23 Associated Sciences Refresher Course AS24
Case-based Review: Neuroradiology CN23 Case-based Review: Neuroradiology CN24
Physics Symposium PS52
Case-Based Review: Interventional Radiology CI33 Case-Based Review: Interventional Radiology CI34
RSNA/NCI Interventional Oncology Series
RSNA/NCI Interventional Oncology Series
Mentored Cardiac CT Case Review
Radiologist Assistants Program RA14 Radiologist Assistants Program RA15 Radiologist Assistants Program RA16
BOOST RO23 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO24 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO33 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO34 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO43 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO44 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO53 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)
BOOST RO54 (Bolstering Oncoradiologic and Oncoradio- therapeutic Skills for Tomorrow)

24 R S N A N E W S A P R I L 2 0 0 7
Product News
Information for Product News came from the manufacturers. Inclusion in this publication should not be construed as a productendorsement by RSNA. To submit product news, send your information and a non-returnable color photo to RSNA News, 820 Jorie
Blvd., Oak Brook, IL 60523 or by e-mail to [email protected]. Information may be edited for purposes of clarity and space.
RADIOLOGY PRODUCTS
PRODUCT UPGRADE
Embedded MIP and MPR ToolsNovaRad Corporation (www.novapacs.com) has releasedNovaPACS 6.6 with embedded MIP (maximum intensityprojection) and MPR (multiplanar reconstruction) tools tobuild and view 3Dimages directly fromthe picture archivingand communicationsystem (PACS) work-station.
Traditionally, post-processing reconstructions are not completed on the PACS,but at a proprietary workstation at or near the PACS work-station. Radiologists can reconstruct any study, in any for-mat, directly from NovaPACS.
A Health Insurance Portability and Accountability Act(HIPAA)-compliant fingerprint touch login solution knownas BIOPOD is also now available for NovaPACS and itscompanion radiology information system, NovaRIS. Thesecure touch login eliminates the need for passwords.
PRODUCT UPGRADE
Anti-Infection Central Venous Access
ARROW INTERNATIONAL (www.arrowintl.com) has addedChloraPrep to the majority of its U.S.-distributed centralvenous access kits. Orange-tinted ChloraPrep highlights
the prepped area and comes with a sterileapplicator containing 2 percentchlorhexidine, rec-ommended by theCenters for DiseaseControl and Preven-tion, which deliversantibacterial activity forat least 48 hours even inthe presence of bloodand organic matter. Theapplicator’s triangularhead allows for precise preppingaround catheter lines and is designed forhands-off application. Manufactured by Enturia, Inc., Chlora-Prep is included exclusively with Arrow International kits.
FDA CLEARANCE
Faster Uterine Fibroid Treatment InSightec Ltd. (www.insightec.com) has received FDA approval forsoftware that significantly speeds up the treatment time of itsExAblate® 2000 MR-guided focused ultrasound (MRgFUS) sys-tem, while ensuring safety and efficacy. The FDA also approvedthe ExAblate 2000 to be used with a 3.0 Tesla MR scanner, in
addition to 1.5 Tesla units.Used to treat uterine fibroids,
the new version of the ExAblate2000 uses an “interleaved”mode of treatment, targeting dif-ferent parts of the fibroid toallow recently ablated tissue tocool while the focus moves toother areas. This reduces thecooling time required. Anothernew feature, allowing physi-
cians to leverage the beam steering a phased array transducer,maximizes the energy in the focal point and allows significantlymore volume to be treated for the same amount of energy applied.
FDA CLEARANCE
Patient Positioning CapabilityVarian Medical Systems (www.varian.com) hasreceived FDA clearance for the patient position moni-toring capabilities added to its RPM™ respiratory gat-ing system. The system is used to synchronize imag-ing and radiation therapy treatment with a patient’srespiratory cycle. The new feature detects any motionthat may compromise the accuracy of the treatment.
The RPM system works by placing a reflectivemarker box on the patient’s chest or abdomen andmonitoring its motion using special cameras posi-tioned in the treatment room. While the previous sys-tem monitored the motion of the marker block only inthe vertical dimension, the new version of the RPMsystem analyzes the marker block motion as it movesup and down, forward and back and side to side. Anew display on the system’s console immediatelyalerts the radiation therapy technologist if the patientshifts in any direction beyond the natural range ofmotion and should be repositioned.

25R S N A N E W SR S N A N E W S . O R G
RSNA ON THE WEB
RSNA.orgThe New Career ConnectionCheck out changes to the RSNA job Web site at RSNA.org/career.
Larger icons helpCareer Connec-tion visitors zeroin on what theywant to do.
Information about thelatest salary trendscan help employersand job seekers alike.
In response torequests fromusers, informationabout the cost toadvertise onCareer Connectionhas been placedprominently onthe page.
OTHER WEB NEWS
Papers of Nobel Prize Molecular BiologistAvailable
THE National Library of Medicine, a part of theNational Institutes of Health, has released an exten-
sive selection from the papers of molecular biologist andscience administrator Harold E.Varmus, M.D., on its Pro-files in Science Web site at www.profiles.nlm.nih.gov.The Profiles now include the personal and professionalrecords of 21 notable scientists.
In 1989, Dr. Varmus and his long-time collaborator J. Michael Bishop, M.D., shared the Nobel Prize inPhysiology or Medicine for their “discovery of the cellu-lar origin of retroviral oncogenes.”
EconnectionsYouronlinelinks toRSNA
Radiology OnlineRSNA.org/radiologyjnlRadiology Manuscript CentralRSNA.org/radiologyjnl/submitRadioGraphics OnlineRSNA.org/radiographicsRadioGraphics RGXPressRSNA.org/rgxpressRSNA News rsnanews.orgEducation PortalRSNA.org/educationRSNA CME Credit RepositoryRSNA.org/cmeCME GatewayCMEgateway.orgRSNA Medical ImagingResource CenterRSNA.org/mircRSNA Career ConnectionRSNA.org/careerRadiologyInfo™
RSNA-ACR patient informa-tion Web site RadiologyInfo.orgRSNA Press ReleasesRSNA.org/mediaMy RSNA Profile & BenefitsRSNA.org/memberservicesRSNA Research & Education FoundationMake a DonationRSNA.org/donateCommunity of ScienceRSNA.org/cosCQI InitiativeRSNA.org/qualityMembership ApplicationsRSNA.org/mbrappRSNA Membership DirectoryRSNA.org/directoryRSNA 2007RSNA2007.RSNA.orgRSNA Highlights 2008RSNA.org/Highlights
RSNA.org
The left-handtaskbar
includes new“How To” linksand can serve
as a quick to do list.
Quick links to RSNA Newsstories help all Career Connection users keep up-to-date on what’s happeningin radiology practice.

Medical Meetings May – June 2007
NONPROFIT ORG.U.S. POSTAGE
PAIDPERMIT #186
EASTON, PA 18042
RSNA News820 Jorie Blvd.Oak Brook, IL 605231-630-571-26701-630-571-7837 [email protected]
CALENDAR
JUNE 3–7European Society of Pediatric Radiology (ESPR), 44th AnnualCongress, The Meliá Barcelona Hotel, Spain • www.espr2007.info
JUNE 7–10Society for Imaging Informatics in Medicine (SIIM), AnnualMeeting, Rhode Island Convention Center, Providence • www.siim2007.org
JUNE 7–10Caribbean Society of Radiologists, 14th Congress, Grand Barbados Beach Resort, Carlisle Bay • www.csor.org
JUNE 9–14American Society of Neuroradiology (ASNR), 45th AnnualMeeting and Neuroradiology Education and Research Founda-tion Symposium 2007, Hyatt Regency Chicago • www.asnr.org/2007
JUNE 11–13UK Radiological Congress (UKRC), Annual Meeting, G-MEX and Manchester International Convention Centre,United Kingdom • www.ukrc.org.uk
JUNE 15–16American Society of Interventional and Therapeutic Neuro-radiology (ASITN), 5th Annual Practicum, Sheraton ChicagoHotel & Towers • www.asitn.org
JUNE 21–24Clinical Magnetic Resonance Society (CMRS), Annual Meeting,Hilton La Jolla Torrey Pines, California • www.cmrs.com
JUNE 28–JULY 1Canadian Association of Radiologists (CAR), Annual Meeting,St. John’s, Newfoundland • www.car.ca
NOVEMBER 25–30RSNA 2007, 93rd Scientific Assembly and Annual Meeting,McCormick Place, Chicago • RSNA2007.rsna.org
FEBRUARY 18-20, 2008RSNA Highlights™, Ritz-Carlton/J.W. Marriott Orlando,Grande Lakes, Florida • RSNA.org/Highlights
MAY 6–9Radiology Business Management Association (RBMA), 2007 Radiology Summit, America’s Center, St. Louis • rbma.org/conferences/radiology_summit/index.php
MAY 6–11American Roentgen Ray Society (ARRS), 107th Annual Meeting,Grande Lakes Orlando, Fla. • www.arrs.org
MAY 14–18World Conference on Interventional Oncology (WCIO) and Societyof Thermal Medicine (STM), Joint Annual Meeting, WashingtonHilton Hotel • www.wcio2007.com
MAY 16–19German Radiology Society, 88th German Radiology Congress,Messe Berlin • www.roentgenkongress.de
MAY 19–23American College of Radiology (ACR), Annual Meeting and Chapter Leadership Conference 2007, Hilton Washington • www.acr.org
MAY 19–25International Society for Magnetic Resonance in Medicine(ISMRM) and European Society for Magnetic Resonance in Medicine and Biology (ESMRMB), Joint Annual Meeting, International Congress Center, Berlin • www.ismrm.org
MAY 25–28Radiology Society of Puerto Rico (SRPR), 11th Annual Meeting,Westin Rio Mar Beach Resort, Río Grande • www.srpr.org
MAY 26–29 American College of Medical Physics, Annual Meeting, Renais-sance Harborplace Hotel, Baltimore • www.acmp.org/meetings.php
JUNE 1–4American Society of Radiologic Technologists (ASRT)/ Associationof Educators in Imaging and Radiologic Sciences (AEIRS), AnnualConference, Hyatt Regency Albuquerque, N.M. • www.asrt.org/content/eventsandconferences/annualconference2007/ac07startpage.aspx
JUNE 2–6Society of Nuclear Medicine (SNM), Annual Meeting, Washington • interactive.snm.org