Embed Size (px)
Citation preview

Journal of Diabetes and Its Comp
Medical records as sources of data on cardiovascular disease
events in persons with diabetesB
Barbara E.K. Kleina,T, Ronald Kleina, Patrick E. McBrideb,
Jennifer O. Reinkea, Michael D. Knudtsona
aDepartment of Ophthalmology and Visual Sciences, University of Wisconsin, Madison, WI 53726, USAbCardiovascular Medicine, University of Wisconsin, Madison, WI 53726, USA
Received 16 April 2004; received in revised form 16 June 2005; accepted 21 June 2005
Abstract
Purpose: The aim of this study is to evaluate medical records as a source of data on cardiovascular disease over a 20-year interval.
Methods: Participants in a population-based cohort of persons with Type 1 diabetes were asked whether they had been told by a doctor that
they had several specific cardiovascular events. In addition, they were asked when and where they were hospitalized for myocardial
infarction, stroke, surgical procedures, and for other conditions and procedures. The medical care institution was contacted to obtain copies of
the relevant hospitalization. Results: Overall, the confirmation of the self-reported events was 86.0% when medical records were obtained.
Percent confirmed variedwith the diagnosis. Reports of poor circulation in the lower extremities were confirmed in 42.6%, strokewas confirmed
in 70%, and coronary bypass surgerywas confirmed in 100% of cases. The success of obtainingmedical records was greater for those events that
were reported to have occurred more recently than those reported further in the past, especially when 10 or more years had elapsed.Conclusion:
Medical record confirmation of reported cardiovascular events in persons with Type 1 diabetes was high for some events when medical records
could be obtained but was lower for bpoor circulationQ to the legs and stroke possibly related to the lack of specificity of our questions, to
incorrect attribution of symptoms by the respondent, or to inaccurate recall of a physician’s examination.Medical record confirmation was better
for more recent than past events. Therefore, when hard copy documentation is needed, it should be sought within 10 years of the event.
D 2006 Elsevier Inc. All rights reserved.
Keywords: Cardiovascular disease; Cerebrovascular accident; Diabetes mellitus, Type 1; Medical records; Myocardial infarction
1. Introduction
Microvascular abnormalities (e.g., retinopathy and nephr-
opathy) are the hallmark of diabetes mellitus. It has been
suggested that large vessel disease in those with diabetes is
related to the antecedent microvascular abnormalities
(Morrish, Stevens, Fuller, Jarrett, & Keen, 1991; Yodaiken,
1976). We investigated this hypothesis in a population of
persons who had participated in the Wisconsin Epidemio-
1056-8727/06/$ – see front matter D 2006 Elsevier Inc. All rights reserved.
doi:10.1016/j.jdiacomp.2005.06.008
B This work was supported by grant HL59259.
T Corresponding author. Department of Ophthalmology and Visual
Sciences, University of Wisconsin, 610 North Walnut Street, Room 409
WARF, Madison, WI 53726, USA. Tel.: +1 608 263 0276; fax: +1 608
263 0279.
E-mail address: [email protected] (B.E.K. Klein).
logic Study of Diabetic Retinopathy (Klein et al., 2004).
Medical records and self-reports are frequently utilized to
ascertain outcomes in medical research. The accuracy of self-
reports is critical to the methodology of long-term studies of
health outcomes. It is becoming increasingly difficult to
access relevant medical records. We describe here our
experience with obtaining medical record data to document
macrovascular events in a population-based study of persons
with long duration diabetes.
2. Methods
Institutional review board approval was obtained for all
participants at each phase of the Wisconsin Epidemiologic
Study of Diabetic Retinopathy, and individual informed
lications 20 (2006) 224–227
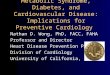
Table 1
Cardiovascular events questionnaire
Have you ever been told by a physician that you had angina—that is, pressure in the chest on exertion due to heart disease? Yes, No, Don’t Know
Have you ever been told by a physician that you have had a heart attack? Yes, No, Don’t Know
Have you had a coronary bypass? Yes, No, Don’t Know
Have you had a coronary angioplasty or stent? Yes, No, Don’t Know
Have you ever been told by a physician that you have had a stroke (apoplexy, cerebral vascular accident)? Yes, No, Don’t Know
Have you had surgery to the brain or neck to prevent or correct a stroke? Yes, No, Don’t Know
Have you ever had a doctor or other medical person tell you that you have poor circulation to legs or feet? Yes, No, Don’t Know
Have you had a toe(s) or foot surgically amputated due to infection or poor circulation? Yes, No, Don’t Know
Have you had a leg surgically amputated due to infection or poor circulation? Yes, No, Don’t Know
Have you ever had surgery to your hands, legs, or feet for circulation problems other than for varicose veins
(or an amputation or accident or carpal tunnel)?
Yes, No, Don’t Know
How many times have you been hospitalized overnight or longer since we last spoke with you on (Date of last interview)? Count or Don’t Know
Are any of these hospitalizations in addition to what you have already reported? Yes, No, Don’t Know
Table 2
Medical records and confirmation of cardiovascular events
Event
Number
of records
requested
Number of
received (% of
those requested)
Number of
confirmation (%
of those received)
All events 837 615 (73.5) 529 (86.0)
Myocardial infarction 71 57 (80.3) 50 (87.7)
Coronary
angioplasty/stent
46 37 (80.4) 34 (91.9)
Poor circulation to legs 164 108 (65.9) 46 (42.6)
Amputation, toe 38 28 (73.7) 27 (96.4)
Amputation, leg 23 20 (87.0) 19 (95.0)
Angina 78 58 (74.4) 46 (79.3)
Stroke 23 20 (87.0) 14 (70.0)
Operation to
prevent stroke
3 3 (100) 2 (66.7)
Circulatory
operation on legs
28 23 (82.1) 16 (69.6)
Coronary artery bypass 55 49 (89.1) 49 (100)
Miscellaneous
hospitalizations
308 227 (73.7) 226 (99.6)
B.E.K. Klein et al. / Journal of Diabetes and Its Complications 20 (2006) 224–227 225
consent was obtained for each visit. In 1979–1980, all
persons with diabetes diagnosed before they were 30 years
of age, who were taking insulin, and who were receiving
care in an 11-county area of southern Wisconsin were
identified (Klein et al., 1984). There were 1210 such
persons; 996 of them participated at baseline in a study of
the prevalence of diabetic retinopathy. The initial study
evaluation included a medical history, measurements of
blood pressures, glycosylated hemoglobin, height, weight,
urinalysis, dilation of the pupil of the eye, and the taking of
seven standard photographic fields of the ocular fundus of
each eye. Participants responded to a medical history
questionnaire at each examination. Pertinent to the current
investigation were responses to interviews conducted
between 1996 and 2001, when study participants were
asked whether a physician had told them that they had had
angina, a heart attack, stroke, poor circulation in their legs,
coronary angioplasty, coronary bypass, surgery in their head
or neck to prevent a stroke, or surgery for circulation in their
legs. For each positive response, we recorded the date and
place of the relevant hospitalization for the condition if they
were hospitalized for it. In addition, we asked for the date
and name of the hospital for any additional hospitalizations
(Table 1). We requested consent from each person reporting
an event to obtain the medical record for each relevant event
and for miscellaneous hospitalizations. All records received
were reviewed by one of the authors (JOR) for correctness
of name of participant and hospital, date of reported event,
and so on. When discrepancies were detected, hospitals
were recontacted up to three times in an attempt to obtain
the appropriate record. These medical records were
reviewed using standard protocols adapted from those
developed for the Women’s Health Initiative (Section 2;
Clinical Centers for the Clinical Trial and Observational
Study of the Women’s Health Initiative East/West. WHI
Protocol Manual, 1997; Writing Group for the Women’s
Health Initiative Investigators, 2002) by a single investi-
gator (PEM). The review protocol described electrocardio-
gram characteristics, cardiac enzyme levels, specific
characteristics of stroke, recorded descriptions of chest pain
for angina and leg pain for the diagnosis of poor circulation
in the legs, and for the procedures listed above. The
reviewer was masked as to the self-report. Miscellaneous
hospitalizations were defined as overnight hospitalizations
for reasons other than cardiovascular events.
During the 20-year follow-up examination, electrocardio-
grams were obtained according to the EPICARE protocol
(EPICARE Center of the Department of Public Health and
Sciences of Wake Forest University School of Medicine).
They were graded by the Nova code (Rautaharju et al., 1990).
3. Results
We obtained interview data from 704 of the original
cohort; 273 had died, and 19 could not be located. The mean
age of our study participants at the time of requesting the
records was 40.8 (F11.1) years, with a range of 18–80 years
of age. We confined these analyses to the first reported event
of each type in the 704 persons. Records were requested and
reviewed for 837 events, and other hospitalizations and were
reviewed between 1997 and 2001. Table 2 describes the

B.E.K. Klein et al. / Journal of Diabetes and Its Complications 20 (2006) 224–227226
results of these efforts for all cardiovascular events and for
each individual endpoint. Six hundred and fifteen of the 837
requested records were received (73.5%). For all endpoints,
529 (86.0%) were confirmed by record review. The percent
of records received of those requested differed by diagnosis
from 65.9% of those for poor circulation in the legs to 89.1%
of those for coronary bypass surgery.
The most commonly reported endpoints were poor
circulation to the legs and angina. For the former, 46/108
(42.6%) was confirmed and for the latter, 46/58 (79.3%) was
confirmed by record review. Percent confirmed differed by
diagnosis for other endpoints as well. For coronary events
aside from angina, the confirmation rate was, in general, high
ranging from 87.7% for myocardial infarction to 100% for
coronary artery bypass surgery. Reports of miscellaneous
hospitalizations were highly accurate because there were no
specific procedures or diagnostic tests necessary to confirm
this, only a discharge summary or progress note that
demonstrated the person was admitted and kept overnight.
The participant was not asked to recall any details other than
the year (give or take one year) and institution.
Table 3 describes the percent confirmed by the time
interval between the interview date (1996–2001) and the
date of the event (1978–2001). The proportion of records
received decreased slightly with duration up to 9 years; the
proportion was much decreased after 10 or more years. The
proportion of confirmations of self-reported event when
records were received was greater for events more recent
than 10 years compared with those occurring 10 or more
years before. There were too few of most events to estimate
this effect for each endpoint. There was no evidence to
suggest that any particular event was more likely to have
occurred at a different duration from the time of record
request than any other event.
Reasons for lack of confirmation included participants’
refusal to consent or to give complete information relating to
the particular event (4.1% of all reported events), medical
facility did not send records in response to our inquiries
(these were repeated up to three times; 20.7%), or the
records sent were incomplete (12.1%).
There were nine cases of definite or probable myocardial
infarction (Nova codes 5.1 or 5.2) among the participants
who had electrocardiograms (n=557) at the 20-year exam.
Seven of these occurred in those 71 persons who had
reported myocardial infarction.
Table 3
Time between event and when self-reported by confirmation status
Duration
(years)
Number of
records requested
Number of records
received (% of
those requested)
Number confirmed
(% of those received)
0–1 309 243 (78.6) 203 (83.5)
2–4 343 260 (75.8) 226 (86.9)
5–9 112 83 (74.1) 71 (85.5)
10+ 72 44 (61.1) 29 (65.9)
4. Discussion
Self-reported history of specific diseases has been found
to be reliable and useful in other studies of several different
morbidities (Ivers, Cumming, Mitchell, & Peduto, 2002;
Sangha, Stucki, Liang, Fossel, & Katz, 2003; Tormo,
Navarro, Chirlaque, & Barber, 2000). However, the reli-
ability varies with the specific disease (Bergmann et al.,
1998; Desai, Bruce, Desai, & Druss, 2001; Klungel, de Boer,
Paes, Seidell, & Bakker, 1999). We have found that
participant-reported history of a doctor-diagnosed coronary
heart disease, including a variety of categories in persons
with Type 1 diabetes, was high. In the Cardiovascular Health
Study (CHS), at the baseline examination, 16.6% of men and
8.3% of women reported a history of myocardial infarction
(Psaty et al., 1995). This was confirmed for 76.6% for men
and 65.1% for women. For persons not reporting a
myocardial infarction, 4.4% of men and 3.2% of women
had electrocardiographic evidence of a previous myocardial
infarction. We note that the age range in the CHS was 65 and
older (Fried et al., 1991). The younger age of our study
participants may have been associated with the somewhat
better accuracy of our self-reports. We did not attempt to
obtain medical records for study participants until the
20-year follow-up of our cohort, and even then, we only
had resources to follow-up for reported events (including
bmiscellaneousQ hospitalizations). Nonetheless, we were
able to confirm 50 of the 71 self-reported cases of
myocardial infarction. The proportion of cases confirmed
varied with the specific cardiovascular diagnosis. The
percent confirmed was poorest for poor circulation in the
legs (42.6%). This likely reflects the lack of etiologic
specificity for the symptoms of numbness, tingling, and loss
of sensation in the lower extremity which could be attributed
to neuropathy or impaired circulation. For this diagnosis,
there were often cases (53%) when peripheral angiography
or ultrasound was performed and no pathology of vessels or
measurable peripheral pulses were noted. It is possible that
self-report of poor circulation reflects errors in patient’s
attribution of the cause of symptoms or differences in
definition of bpoor circulation.Q Our questionnaire did not
include queries as to specific symptoms or signs of bpoorcirculation.Q Even if we had included questions aimed at
distinguishing between bpoor circulationQ and neuropathy, it
is uncertain that the study participants or we would be likely
to classify the cause of such symptoms correctly. It is also
unclear as to whether the physician’s explanation to a
participant or that individual’s remembrance of such a
discussion would be accurate.
We were hampered in our ability to retrieve medical
records because in some cases records were destroyed by
hospitals and in some cases hospitals no longer existed. In
some cases, the relatively long interval between the event
and our attempts to retrieve the records likely accounted for
the 222 (27%) cases when hospitals did not return requested
records. In addition, in a few cases, participants refused to

B.E.K. Klein et al. / Journal of Diabetes and Its Complications 20 (2006) 224–227 227
give consent for us to obtain the records or hospitals refused
to release them. Recent changes in privacy regulations and
the climate of trust may make it more difficult to obtain
such records in the future causing researchers to depend
more on self-report. While self-reporting of a doctor’s
diagnosis may lead to misclassification, so might depending
on retrieval of appropriate medical records. We note that the
recency of event was associated with a higher percentage of
obtainable records, and so if medical record confirmation is
critical, this should be attempted as soon as possible after
the event is reported.
We obtained electrocardiograms at the 20-year follow-up
examination. The number of persons with past myocardial
infarction according to Nova code criteria was only nine.
This suggests that this is not a good measure of the burden
of myocardial infarction in those with Type 1 diabetes.
In summary, this study demonstrates that patient self-
reports of cardiovascular disease events are correlated with
actual documented cardiovascular heart disease events, but
the strength of the correlation varies with the specific event.
However, if the event is more than 10 years ago, the
reliability of the patient self-report and availability of related
medical records drops significantly. Therefore, participants
in prospective studies should be urged to update their health
histories and report any new events. Retrospective reviews
are most accurate if the event has occurred within the prior
decade. Substantial effort is required on the part of research
staff to obtain medical documentation of clinical events.
Acknowledgments
The authors thank Lisa Grady for technical support of
this manuscript.
References
Bergmann, M. M., Calle, E. E., Mervis, C. A., Miracle-McMahill, H. L.,
Thun, M. J., & Heath, C. W. (1998). Validity of self-reported cancers in
a prospective cohort study in comparison with data from state cancer
registries. American Journal of Epidemiology, 147, 556–562.
Clinical Centers for the Clinical Trial and Observational Study of the
Women’s Health Initiative East/West. WHI Protocol Manual, Vol. 8—
Outcomes, pp. 1–7, Version 8/15/1997.
Desai, M. M., Bruce, M. L., Desai, R. A., & Druss, B. G. (2001). Validity
of self-reported cancer history: A comparison of health interview data
and cancer registry records. American Journal of Epidemiology, 153,
299–306.
Fried, L. P., Borhani, N. O., Enright, P., Furberg, C. D., Gardin, J. M.,
Kronmal, R. A., Kuller, L. H., Manolio, T. A., Mittelmark, M. B.,
Newman, A., et al. (1991). The Cardiovascular Health Study: Design
and rationale. Annals of Epidemiology, 1, 263–276.
Ivers, I. Q., Cumming, R. G., Mitchell, P., & Peduto, A. J. (2002). The
accuracy of self-reported fractures in older people. Journal of Clinical
Epidemiology, 55, 452–457.
Klein, B. E., Klein, R., McBride, P. E., Cruickshanks, K. J., Palta, M.,
Knudtson, M. D., et al. (2004). Cardiovascular disease, mortality, and
retinal microvascular characteristics in type 1 diabetes: Wisconsin
Epidemiologic Study of Diabetic Retinopathy. Archives of Internal
Medicine, 164, 1917–1924.
Klein, R., Klein, B. E., Moss, S. E., DeMets, D. L., Kaufman, I., & Voss, P.
S. (1984). Prevalence of diabetes mellitus in southern Wisconsin.
American Journal of Epidemiology, 119, 54–61.
Klungel, O. H., de Boer, A., Paes, A. H., Seidell, J. C., & Bakker, A.
(1999). Cardiovascular diseases and risk factors in a population-
based study in The Netherlands: Agreement between questionnaire
information and medical records. Netherlands Journal of Medicine,
55, 177–183.
Morrish, N. J., Stevens, L. K., Fuller, J. H., Jarrett, R. J., & Keen, H.
(1991). Risk factors for macrovascular disease in diabetes mellitus: The
London follow-up to the WHOMultinational Study of Vascular Disease
in Diabetics. Diabetologia, 34, 590–594.
Psaty, B. M., Kuller, L. H., Bild, D., Burke, G. L., Kittner, S. J., Mittelmark,
M., et al. (1995). Methods for assessing prevalent cardiovascular
disease in the Cardiovascular Health Study. Annals of Epidemiology,
5, 270–277.
Rautaharju, P. M., MacInnis, P. J., Warren, J. W., Wolf, H. K., Rykers, P.
M., & Calhoun, H. P. (1990). Methodology of ECG interpretation in the
Dalhousie program: NOVA CODE ECG classification procedures for
clinical trials and population health surveys. Methods of Information in
Medicine, 29, 262–274.
Sangha, O., Stucki, G., Liang, M. H., Fossel, A. H., & Katz, J. N. (2003).
The Self-Administered Comorbidity Questionnaire: A new method to
assess comorbidity for clinical and health services research. Arthritis
and Rheumatism, 49, 156–163.
Tormo, M. J., Navarro, C., Chirlaque, M. D., & Barber, X. (2000).
Validation of self diagnosis of high blood pressure in a sample of
the Spanish EPIC cohort: Overall agreement and predictive values.
EPIC Group of Spain. Journal of Epidemiology and Community
Health, 54, 221–226.
Writing Group for the Women’s Health Initiative Investigators. (2002).
Risks and benefits of estrogen plus progestin in healthy postmenopausal
women. Principal results from the Women’s Health Initiative Random-
ized Controlled Trial. Journal of the American Medical Association,
288, 321–333.
Yodaiken, R. E. (1976). The relationship between diabetic capilloropathy
and myocardial infarction: A hypothesis. Diabetes, 25, 928–930.