Embed Size (px)
Citation preview
![Page 1: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/1.jpg)
13 Congenital Neck Masses (Non-vascular)A.W.DuNCAN
CONTENTS
13.1 Introduction 17513.2 Imaging Investigations 17613.3 Lymphangioma 17713.3.1 Embryology of the Lymphatic system 17713.3.2 Types of Lymphangioma 17713.4 Thyroglossal Duct Cyst 18113.5 Thornwaldt's Cyst 18313.6 Branchial Cleft Anomalies 18313.7 Piriform Sinus Fistula (Abscess) 18513.8 Thymic Cyst 18613.9 Cervical Extension of the Mediastinal Thymus 18713.10 Dermoid/Epidermoid Cyst 18713.11 "Plunging" Ranula 18813.12 Ectopic Thyroid Gland 18813.13 Sternomastoid "Tumour" 190
13.14 Congenital Teratoma 19113.15 Cervical Neuroblastoma 19213.16 Laryngocele 19313.17 Lung Herniation 19313.18 Thyroid Gland Hemiagenesis 19413.19 Midline Cervical Cleft 19413.20 Bronchogenic Cyst 19513.21 Lingual Thyroid Gland 19513.22 Congenital Vascular Lesions 19513.22.1 Haemangioma 19513.22.2 Varix of the Jugular Vein 19513.22.3 Carotid Artery Aneurysm 19513.22.4 Cervical Aortic Arch 19613.23 Rare Congenital Tumours, Cysts and Infections 19613.24 Summary 196
References 196
13.1Introduction
Neck masses are common in the paediatric age group.Most are congenital or inflammatory in origin, theremaining are vascular or, rarely, malignant lesions.The site and age at presentation can strongly aid diag-
A.W.DuNCANConsultant Paediatric Radiologist, Senior Clinical Lecturer inPaediatric Radiology, University of Bristol, Bristol Royal Hospital for Children, Paul O'Gorman Building, Upper MaudlinStreet, Bristol, BS2 8BJ, UK
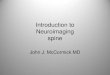
nosis. Malignant lesions are rarely present at birth,although occasionally cervical neuroblastoma maypresent at this time. Most congenital masses presentin infancy and early childhood. They may presentbecause they have become infected. The site alonecan indicate the probable diagnosis. As a general rule,most midline lesions are benign. The site is determined by the embryology, and even a limited knowledge of the embryology helps to determine the probable diagnosis. Branchial abnormalities develop frompaired branchial arches, and therefore lie laterally,usually in relation to the anterior border of the sternomastoid muscle. Piriform sinus fistula, which maydevelop into an abscess, is a paired structure andtherefore lies laterally. Similarly the rare lung herniation, bronchogenic cyst, sternomastoid tumour andcongenital sympathetic chain neuroblastoma, arisefrom paired structures and will lie laterally. The thyroid gland, although lying more medial than theabove structures, is a paired structure and a lesionarising from one lobe will lie lateral to the midline.The embryology of a central structure such as thethymus and thyroid, which descend into the neck,results in pathology along the midline track. Dermoid cysts can lie anywhere, but usually those inthe central nervous system and in the neck are midline. Fig. 13.1 shows the locations of these congenitalanomalies.
The presentation of the lesion is also an aid to thediagnosis. Many congenital lesions will present in thenewborn period or early years, although some havea delayed appearance, becoming symptomatic dueto enlargement or infection. Inflammatory lesionsrarely present at birth but develop in early childhood,and some of them may be secondarily infected congenital lesions. Malignant lesions are extremely rarein the neck at birth and usually present in older children and adolescents. Inflammatory lesions tend tobe painful and tender with erythema, whereas malignant lesions tend to be painless solid masses.
Masses that present in older children can oftenbe differentiated on the basis of the history, withcongenital masses being present for a considerable
S. J. King et al. (eds.), Pediatric ENT Radiology© Springer-Verlag Berlin Heidelberg 2003
![Page 2: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/2.jpg)
176
UNGUAl.TMYROID Gl.AHD:
MOSTCOIlIlON
LESS COMMONSUBUNGUAl.
STERNUM ------j
.....-"-------BRANCHIAL VESTIGE(CARTILAGE OR BOtlE)
-r----- SUBSTERNAL TMYROID
A. W.Duncan
Fig. 13.1. The anatomical sites of congenitalneck masses
period, inflammatory masses for a few days, and neoplastic lesions for a few months.
The most common neck mass in a young child islymphatic malformation or cystic hygroma.
13.2Imaging Investigations
A tentative diagnosis can be made with a fair degreeof accuracy on the basis of history and clinical examination, but the imaging investigations add confirmatory evidence and also avoid potentially seriouserrors such as removal of the patient's only thyroidtissue in an ectopic thyroid gland.
The first line of investigation is usually ultrasonography, which can differentiate cystic from solidmasses and is invaluable since most congenitaland inflammatory lesions have a cystic component(TELANDER and FILSTON 1992). It can also showthe extent of the lesion if small, but larger lesionsare better evaluated by magnetic resonance imaging(MRI). Calcifications and bone erosion can be betteridentified by plain films or computed tomography(CT), but these are rarely of any clinical value, whileboth CT and plain radiography add less in termsof spatial relationships than MRI and also irradiatethe child. However, if MRI is not available then CTcan show the lesion. Contrast enhancement is usuallyonly necessary in CT for showing the vessels, as most
congenital lesions will show very little enhancementunless there is infection; in the latter case there will beenhancement of the capsule or surrounding tissues.In general terms, for MRI, T1 weighting gives goodspatial relationships and T2 will show any oedema.STIR sequences with fat suppression show oedemato greater advantage, but will also confirm the fatcontaining structures seen in teratomas. Contrastenhancement is usually not necessary. Coronal andaxial scans will show most lesions, although midlinelesions are better seen with the sagittal sections.Cystic lesions usually have a low signal on T1 and ahigh signal on T2 consistent with fluid, although thismay be modified if there has been haemorrhage. Thewall of the cyst and surrounding tissue is usually oflow signal on T2 but can be high if there is inflammation, and may at times be difficult to differentiatefrom a neoplastic lesion.
Occasionally it may be necessary to perform contrast studies if there is encroachment on the alimentary tract causing dysphagia or there are lesions associated with a sinus tract. Lesions associated with apercutaneous tract ending blindly can be shown bywater-soluble contrast, but it is usually consideredmeddlesome to do this as it has the potential forintroducing infection.
In most cases small lesions can be adequatelyassessed by ultrasound. They are described below inrelative descending frequency which will vary withage of the child.
![Page 3: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/3.jpg)
Congenital Neck Masses (Non-vascular)
13.3Lymphangioma
These are congenital lymphatic malformations (LM's),usually of a localised nature, and involve dilated lymphatic spaces. They can occur anywhere in the bodybut are most common in the head, neck and axilla.LM's can be characterized by the size of the cysts present into microcystic, macrocystic or mixed lesions(MULLIKEN et al. 2000). Conventionally LM's havebeen subdivided into 1) cystic hygroma, 2) cavernouslymphangioma, 3) capillary lymphangioma, 4) vasculolymphatic lymphangiohaemangioma and they willbe discussed under these subheadings.
Most lymphangiomas present at birth, and 90%within the first 2 years oflife. 75% oflymphangiomasoccur in the neck, most commonly in the posteriortriangle, sometimes with extension into the mediastinum. Presentation at birth is most commonly as anasymptomatic mass, although if it is large in size itmay cause respiratory difficulty due to compressionof the airway. The morbidity or mortality attachedto lymphatic malformations, unless they are associated with chromosomal abnormalities such as Turner's syndrome and fetal hydrops, is low.
13.3.1Embryology of the Lymphatic System
To understand the types of lymphangioma, a reviewof the theories behind the embryology is helpful. Following arterial and venous development in the jugular region there are endothelial buds which sproutfrom the veins and unite to form plexuses. Thesedevelop into paired jugular sacs. Later the jugularsacs enlarge and maintain a single communicationwith the internal jugular vein.
There is continued growth with extensions intothe soft tissues and between muscles, to the posterior compartment of the neck, and other extensionsbetween the structures of the neck. This sproutingcontinues, ultimately forming lymph vessels permeating all the tissues, following the blood vessels andtheir branchings.
There are various theories of the pathogenesis oflymphangioma. These include failure of the lymphatics to drain into the veins results in isolated lymphatic channels, particularly the larger and more central cystic hygromas (WEINGAST 1988). Other authorsfavour sequestration of the lymphatic tissue early inembryogenesis with a failure to join the normal centrallymphatics (PHILIPS 1981). This explains the periph-
177
eral location of capillary or cavernous lymphangiomas. The small lymphatic channels are presumablyrelated to their primordium at which sequestrationoccurs, which results in a fine network of lymphatics.
Yet another theory postulates abnormal buddingof lymphatic structures. These aberrant buds losetheir connections with the lymphatic primordia andeventually canalise to form lymphatic cysts (LEE1980). These cysts can grow in an uncontrolled, disorderly manner and can penetrate and destroy anatomical structures. This helps to explain the permeativenature of many lymphatic malformations, particularly of the cavernous lymphangiomas. The aberrantprimary bud may explain the formation of the moredilated cystic hygromas near the primordial lymphsac (ZADVINSKIS et al. 1992).
Athough theories of pathogenesis related to theembryologycan explain some of the appearances, someauthors feel that many of the appearances are relatedto the anatomical location which determines the histological characteristics. Where there is loose fatty tissuesuch as in the neck, growth is unimpeded, leading to theformation of a macrocystic LM or cystic hygroma. Inother locations such as the cheek or tongue, expansionis curtailed, resulting in a mixed lesion.Where the tissueis much tougher, such as in the epidermis and dermis,the malformation is smaller and results in the formation of a microcystic LM (BILL and SUMNER 1965).
13.3.2Types of Lymphangioma
13.3.2.1Cystic Hygroma
Cystic hygroma is the most common form of LM and isusually macrocystic. It usually occurs in isolation, butit may occur with more generalised abnormalities suchas Turner's syndrome (45 XO chromosome karyotype).These are frequently seen in aborted fetuses and arebelieved to form as a result of failure of the juguloaxillary lymphatic sac to drain into the internal jugularvein (SMITH 1982). The accumulation of fluid causesprogressive dilatation of the lymphatics, resulting ina cystic hygroma. There is secondary dilatation ofthe lymphatic channels that drain the extremitiesand chest, resulting in peripheral lymphoedema andhydrops. If lymphatic drainage is re-established, thecystic hygroma may regress and result in the typicalneck webbing seen in Turner's syndrome (SMITH 1982).Whatever the true embryology of these malformations,in all instances obstruction is a feature (Fig. 13.2).
![Page 4: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/4.jpg)
178 A.W. Duncan
Fetal cystic hygroma
Generalised lymphaticdefect
Localised lymphaticdefect
Progression
Severe Mild
No hydrops
Resolution
difficulty. Extension of such lesions into the thoracicinlet may result in stridor, cyanosis or apnoea whenimpinging on the trachea, or dysphagia when impinging on the oesophagus or tongue.
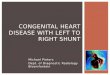
Plain radiographs of the neck and chest may showextension into the mediastinum and displacement andcompression of the airways. Ultrasonography is theeasiest non-invasive investigation and is usually thefirst line of study; it will demonstrate multiple septatedcystic spaces filled with hypoechoic fluid (Fig. 13.3a).These may be infiltrative, making it difficult to distinguish them from adjacent tissue. If complicatedby haemorrhage into the cystic structures, the fluidbecomes echogenic (Fig. 13.3b) and may result in
Fig. 13.2. Course of fetal cystic hygroma. (Reproduced withpermission from ZADVINSKIS et al. 1992)
The solitary cystic hygroma is the most commonpresentation, resulting from failure of re-anastomosisand failure ofthe lymphatic system to drain. This resultsin multilocular cystic malformations which occur inapproximately 1in 12,000 births (STRINGEL 1993). Theyhave a predilection for the left side of the neck, mostprobably because the thoracic duct enters the subclavian vein on that side. They are lined by endothelialcells and produce lymphatic fluid. This results in a gradual but sometimes rapid enlargement with compression and stretching of the adjacent structures. Eightypercent of cystic hygromas occur in the neck.
Most cystic hygromas (75%-80%) are present atbirth, 90% by the age of 2 years (TELANDER andFILSTON 1992) and 3%-10% extend into the mediastinum (Castellote et al. 1999). They are usually discrete,soft, mobile, painless, non-tender, cystic masses, usually in the posterior triangle of the neck, and varyin size up to several centimetres in diameter. As theycontain fluid they transluminate. Primarily they arepainless, but one-third present with infection and mayshow clinical features of erythema or tenderness. Theymay rapidly grow in size as a result of this infectionor haemorrhage into the cyst with or without trauma.Lymphangiomas located in the floor of the mouthand tongue are especially prone to bleed, leading toenlargement and airway compression (VAZQUEZ et al.1995). Unless complicated, they are often asymptomatic, but because of their large size they may causecompression of the airways and result in respiratory
a
b
Fig. 13.3a,b. Cystic hygroma. a Ultrasonogram of a small cystichygroma where there are multiple small cysts all of which arehypoechoic, indicating there has been no haemorrhage. Thesmaller cysts tend not to have any haemorrhage and are therefore hypoechoic. b Ultrasound shows large cysts, which arehypoechoic, containing fluid. Others are hyperechoic, showingtheir proteinaceous nature, which is most likely due to somehaemorrhage into the cyst
Webbed neckPeripheral oedemaAbnormal
lymphangiogram
Isolated cystichygroma
![Page 5: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/5.jpg)
a
b
Congenital Neck Masses (Non-vascular)
fluid levels. Where the haemorrhage is mixed withthe fluid uniformly, the cystic spaces may simulate asolid structure due to the echogenic nature of the fluid(Fig. 13.3b), although the movement of the echogenicmaterial under transducer pressure usually identifiesareas of haemorrhage. A larger lesion will be betterdemonstrated by CT or MRI (Fig. 13.4); MRI is theinvestigation of choice (Fig. 13.5) since it can evaluatethe extent of the lesion and, particularly, its extensioninternally into the vital structures (Fig. 13.6) and downinto the mediastinum. A low signal on II-weightingand a high signal on TZ-weighting will indicate fluidcontent. It may show fluid layering due to haemorrhage. Intravenous contrast medium will demonstrateits relationship to the vessels, however it is usuallyunnecessary to give contrast medium. In CT and MRIcontrast-enhanced scans may show enhancement ofthe septa (Fig. 13.4). MRI, because of its multi-planarnature, can best show the structure and may showassociated venous anomalies (DALLEY 1996). Haemorrhage into the lymphangioma may cause acute presen-
179
b
Fig.l3.5a,b. Cystic hygroma. a CT scan shows a massive lymphangioma involving both sides of the neck. The hypodenseareas are due to fluid-filled cystic spaces. The more solidelements could be residual normal tissue or microcysticlymphangiomatous component of the lymphangioma. b Samepatient. Sagittal section II-weighted MRI shows the lymphangioma much better, demonstrating extension to the floor ofthe mouth. The brighter signal in the lower portion may wellrepresent small areas of haemorrhage
..Fig. l3Aa, b. Cystic hygroma. a CT with contrast shows a cystichygroma in the neck displacing the oropharynx. It has multiple enhancing septa. It is of uniform low attenuation, indicating fluid. b Coronal T2-weighted MRI shows the septa wellwithout contrast medium
a
![Page 6: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/6.jpg)
180
Fig. 13.6. Cystic hygroma. T2-weighted MRI shows the moreinfiltrative nature of some cystic hygromas, with medial extension into the posterior pharyngeal space
Fig. 13.7a, b. Cystic hygroma with recent haemorrhage. a Plainfilm shows the massive prevertebral soft tissue opacity displacing the airway forwards. b Same patient. CT scan showsthe massive cystic hygroma displacing the airway forwardsand to the left side. The central area of increased density probably represents haemorrhage, with some fluid levels of bloodand clear fluid of the cystic hygroma
tation due to its sudden increase in size with associated respiratory difficulties (Fig. 13.7).
Although spontaneous regression can occur, itonly occurs in 6% of cases (CASTELLOTE et a1. 1999).Aspiration alone is often unproductive as re-accumulation of fluid occurs, but there has been somesuccess with various sclerosing agents with complexcystic hygromas that cannot be completely surgicallyexcised.
A full account of the imaging and treatment ofLM's is given in Chap. 20.
13.3.2.2 Cavernous Lymphangioma
Cavernous lymphangioma is composed of mildlydilated cavernous lymphatic spaces that are muchsmaller than the cystic hygroma and are usually subcutaneous in location. They occur in the tongue andsalivary glands. They penetrate between structuresrather than destroying them. They therefore haveless clear-cut margins than cystic hygroma. As theyarise in more solid structures which give resistanceto growth, they tend to be permeative and smaller.
A.W.Duncan
"\ '~~.
j. '" .' 1
~-~.'c .•-~·-- ~ ..
They have a low signal on Tl-weighted MRI and ahigh signal on T2-weighted scans.
13.3.2.3 Capillary Lymphangioma
Capillary lymphangioma is not only the leastcommon form of lymphangioma and not commonlyseen in the neck, but it is also uncommon in children.Up to 25% of these lesions are first seen in patientsover 45 years old.
13.3.2.4 Lymphangiohaemangiomas
Lymphangiohaemangiomas are part of a vascularlymphatic malformation, probably form from anembryologically abnormal bud and retain their original venous communication.
Ultrasound may show multiple high echoes fromthe walls of these small cysts. There may be largervessels passing through the mass on its periphery,which on Doppler imaging can often show bloodflow. This, however, depends on the amount of thehaemangioma component and the degree of flow. The
a
b
![Page 7: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/7.jpg)
Congenital Neck Masses (Non-vascular)
investigation of choice is MRI, which can demonstrate the mass - usually high signal on T2-weightedscans - but without the large cystic spaces. If MRI isnot available then CT scans will show a low-attenuation mass between vessels, and the vascular areas willenhance with contrast medium.
13.4Thyroglossal Duct Cyst
These occur most commonly in the region of the hyoidbone and are the most common midline lesion of theneck in children, accounting for 70% of all congenitalneck lesions (SANTIAGO et al. 1985). They are rarelynoted at birth, but usually present in the first 5 yearsof life, often with infection at between 2 and 10 years.A third of patients present at over 20 years of age(BROWN and AZIZKHAN 1998). Infection is commondue to communication with the base of tongue andconsequent exposure to oral bacteria. Embryologicallythey form from a persistence of the thyroglossal duct,a remnant of which is seen in 7% of the population(EWING et al. 1999). The thyroid gland forms as adiverticulum from the anterior wall of the pharynx,later identified by the foramen caecum in the posterior tongue. This diverticulum descends, reaching itsnormal position anterior to the trachea. During itsdescent there is a connection by the thyroglossal ductto the tongue, which ultimately disappears.
The hyoid bone develops simultaneously from thesecond branchial arch and thus this duct, after passingthrough the tongue, maintains an intimate relationship with the central portion of the hyoid bone to connect with the thyroid gland (ELLIS and VAN NOSTRAND1977). This probably explains the common occurrenceof the thyroglossal duct cyst at the hyoid bone.
Persistence of the thyroglossal duct may occurand, if segments of this duct fail to regress, maydifferentiate into epithelial blind cysts (NOUJAIM etal. 1997). When the epithelial cells cease to remaininactive, secretions are produced and form enlargingcysts (TODD 1993). More than 50% contain normalthyroid tissue in their walls, which may be functional (OKSTAD et al. 1986). A thyroglossal cyst canlie anywhere from the foramen caecum to the normalthyroid position suprasternally (WADSWORTH andSIEGEL 1994). The cysts lie in the midline, 80% at orjust below the hyoid bone. Some reports suggest over95% split equally at or below the hyoid bone (AHUJAet al. 2000a). Occasionally they may be slightly lateral to the midline. There is usually no external open-
181
ing unless there is infection resulting in spontaneousdrainage, which helps to differentiate it from branchial cleft cyst (MICKEL and CALCETERRA 1983). Ifthe tongue is protruded, the cyst moves cephaladbecause of its connection with the base of the tongue.The cyst itself is lined by epithelium and containscolourless, viscous secretion.
Occasionally thyroglossal cysts lie in unusual situations, 3% being sublingual and 10% suprasternal(ROWE 1995). They are usually soft, smooth and nontender although they will become warm, tender, painful and oedematous if infected, and may well have afistula draining externally.
The typical ultrasonographic appearance was originally described as an anechoic,well-defined cyst withincreased acoustic through-transmission, between 5mm and 25 mm in diameter, sometimes with a smallbeak at the attachment to the thyroglossal duct (Fig.13.8). Most lesions have thin walls, they are usuallyunilocular. The cyst fluid is usually described asanechoic, but more recent studies suggest that frequently it is hyperechoic, probably due to proteinaceous material secreted by the wall lining (WADSWORTH and SIEGEL 1994). In a more recent studyanechoic lesions were uncommon (13%), complexheterogeneous echo patterns were more frequent(30%), and a uniform homogeneous pseudo-solidappearance was the most common (AHUJA et al.2000a). The last appearance, however, can be clarifiedby applying pressure to the transducer, which willdisturb the proteinaceous contents of the fluid, producing echoes which move, showing the true cysticnature of the structure (AHUJA et al. 2000A). Thecomplex heterogeneous internal echogenic appearance is caused by debris and septa. Posterior enhancement, which occurs in cystic lesions, only occurs in
Fig. 13.8. Thyroglossal duct cyst. Ultrasound shows the typical hypoechoic fluid in the cyst, with a small beak (arrows)representing the thyroglossal duct pointing cephalad
![Page 8: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/8.jpg)
182
approximately half of the cases, and is less likely tobe seen in the pseudo-solid type. Most lesions areunilocular with thin walls, but some are thick-walledwith internal debris due to inflammation. Although itis uncommon, about 1% of duct cysts may be malignant (WEISS and ORLICH 1991), and therefore thepresence of a true solid component in the cyst suggests the possibility of malignant degeneration intocarcinoma, usually a papillary carcinoma (HAYES andMARLOW 1968) - although this is very rare in children (DAVIES and CYCOES 1977).
Ultrasound should also show the presence of anormal thyroid gland.
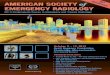
MRI is usually unnecessary but clearly shows thelesion with low signal on Tl-weighted scans (Fig.13.9a) and high signal with T2 weighting due to thefluid within the cyst, with the sagittal sections showing the superior extent of the thyroglossal duct (Fig.13.9b). If MRI is not available, CT shows the lesion,which occasionally can be very large (Fig. 13.10).
The clinical differential diagnosis includes ectopic thyroid tissue, dermoid cyst, sebaceous cyst, submentallymphoiditis, cystic hygroma, haemangioma,lipoma and, exceedingly rarely, neoplasm. Lingualand sublingual thyroid may simulate thyroglossalduct cyst, and inadvertent removal of the only thyroid tissue will produce hypothyroidism.
Ultrasound will differentiate solid from cysticstructures and therefore exclude ectopic thyroidtissue, dermoid cyst and sebaceous cyst. Lipomashave a feathery pattern with multiple bright echoesat right angles to the transducer surface (AHUJA et al.1998). Cystic hygromas have multiple cystic spaces.They also tend to lie more laterally. Off-midline thyroglossal duct cysts may clinically be mistaken forbranchial cleft cysts, and may be a problem as thesetwo entities show similar sonographic appearances
A. W.Duncan
(AHUJA et al. 2000b). Lymphadenopathy is usuallyeasy to differentiate, being hypoechoic with echogenic hila and vascular malformations show flowwith Doppler ultrasonography. There may be phleboliths in some cases.
The treatment for non-infected cases is completeexcision by the Sistrunk technique (SISTRUNK 1928).This involves excision of the thyroglossal duct with acentral portion of the hyoid bone and the thyroglossal tract that will ultimately open into the oral cavityand foramen caecum.
Some authorities suggest that thyroid functiontests and isotope scanning should be carried outprior to surgery to ascertain that there is normalfunction. A euthyroid patient with midline and infrahyoid thyroglossal cyst should be tested for thyroidstimulating hormone (TSH) (RADKOWSKI et a1.1991).If TSH is normal, radioisotope scintigraphy is unnecessary. TSH, radioisotope scintigraphy and MRIshould be carried out in suprahyoid lesions includingthe lingual site (TODD 1993). Routine preoperativeradioisotope scanning to ensure that the thyroglossal duct does not contain thyroid tissue is generallynot recommended because the surgery would haveto take place irrespective of the findings. If thereis significant thyroid tissue on a pathological specimen, postoperative thyroid function tests will identify patients requiring replacement therapy (FILSTON1989). In view of the attendant risk of removing ectopic thyroid tissue which has been mistaken for thyroglossal duct cysts, ultrasonography is imperative inall cases prior to surgical removal of the mass, to confirm the presence of a normal thyroid gland (BREWISet al. 2000). Thyroid function tests and radioisotopescans are recommended if the patient is hypothyroid or when no gland is seen on ultrasound (LIMDUNHAM et al. 1995).
a
Fig. 13.9a, b. Thyroglossalduct cyst. a Axial Tlweighted image of thyroglossal duct cyst whichappears isodense to muscleand splits the anteriorstrap muscles with ananterior left paramedialcomponent. b Sagittal T2weighted image. The highsignal in the thyroglossalduct cyst extends in anarrow tract from the levelof the hyoid bone downto the thyroid. (Reproduced with permissionfrom HARDING HAM and
b GOLDING 2000)
![Page 9: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/9.jpg)
Congenital Neck Masses (Non-vascular)
Fig.B.10. CT. Large thyroglossal cyst from base of tongue distending the suprahyoid portion of the neck. (Reproduced withpermission from TODD 1993)
13.5Thornwaldt's Cyst
This cyst of Thornwaldt's bursa forms as a bulge onthe posterior-superior wall of the nasopharynx dueto closure of the sac's drainage duct. The pharyngeal bursa is an embryonic remnant occurring in 3%of healthy adults (BIURRuN et al. 1992) due to anadhesion between the notochord and the pharyngealectoderm. It is usually small, although it may reachseveral centimetres in diameter. It is usually of noclinical significance unless it becomes infected. If itdoes become symptomatic it presents between theages of 15 and 30 years. It is usually found as anincidental finding on an MRI scan (BOUCHER et al.1990), with the typical appearance of fluid-filled cyst,low-signal on Tl- and high-signal on T2-weightedsequences (EDWARDS 1993), and in one series hasbeen reported in as many as 20% of cases on MRI,although without histological proof (BATTINO andKHANGURE 1990).
13.6Branchial Cleft Anomalies
Branchial cleft anomalies include cysts, sinuses, fistulae and cartilaginous remnants with skin tags. They
183
are a third as common as thyroglossal duct cysts(TODD 1993). Internal cysts and fistulae of the pharynx are rare. The nomenclature of branchial derivatives is as follows: a fistula is a patent, duct-like structure, having both external cutaneous and internalpharyngeal orifices. An external sinus is blind-ending space extending inwards from the skin. An internal sinus is a blind-ending space extending outwardsfrom the orifice in the pharynx. Both these sinusesare thought to be non-obliterated branchial pouches.Cysts are spherical or ovoid spaces with no communication to the pharynx or skin, lying along thetract of the branchial pouch or cleft (SKANDALAKISand TODD 1993). Ninety-five percent ofbranchial cleftderivatives arise from the second cleft and occur atthe anterior border of the sternomastoid and near theangle of the mandible (HARNSBERGER 1995). Firstbranchial cleft anomalies usually give rise to lesionsin the submandibular and preauricular regions, e.g.cyst near the lower pole of the parotid, and are rare.Third and fourth cleft anomalies are even rarer andare potential tracts that may give rise to fistulae (Hardingham and Golding 2000). Occasional deep cystshave been attributed to third and fourth pouch remnants (Gray and Skandalakis 1972).
Branchial cleft tracts or sinuses are most commonly seen in the first decade; branchial cleft cystusually presents in the second decade. The sinusesand fistulae are seen along the lower third of the anterior border of the sternomastoid muscle. The opening is usually of pin-point size and exudes mucoidmaterial. They may appear bilaterally. Second branchial cleft cysts can occur along the same tract as fistulae from the supraclavicular region, from behindthe mandible to the tonsillar fossa. The most commonsite is above the level of the hyoid bone in a higherlocation than fistulae, most commonly near the bifurcation of the carotid artery just below the angle ofthe jaw. Branchial cleft cysts may arise if the sinustract orifice becomes occluded (BRowN and AZIZKHAN 1998). Clinically they appear, unless infectionintervenes, as painless swellings along the upper thirdof the anterior border of the sternomastoid behindthe angle of the mandible. They range in diameterfrom 1 to 10 em and usually do not have any connection to the exterior (TELANDER and FILSTON 1992),although a sinus tract or fistula may open anteriorlyabove the clavicle or in the tonsillar fossa (HARDINGHAM and GOLDING 2000). They present in infancy or,more often, later, in the young adult, because of infection or trauma. Branchial vestiges may occur whenthere is failure of disappearance of branchial cartilages, apart from those which form ligaments and
![Page 10: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/10.jpg)
184
bones. Cartilaginous or bone remnants may veryrarely present in infancy, embedded in the anteriorborder of the lower third of the sternomastoidmuscle.
Diagnosis in many cases can be made by inspection. Sinus tracts usually do not require any investigation, and the use of water-soluble contrast is usually considered inappropriate because of the risk ofinfection (TAPPER 1993).
Branchial cleft cysts can be identified by ultrasound, which shows the location of the cyst anteriorto the upper portion of the sternomastoid musclesand lateral to the carotid sheath. It may have highechogenicity due to cholesterol crystals,keratin,cellular debris or secondary infection, and have a pseudosolid appearance (REYNOLDS and WOLINSKI 1993). If
A. W.Duncan
further evaluation is needed, contrast-enhanced CTdemonstrates a uni- Olr multilocular cyst with a thinuniform wall. The contents are of water density ormay be of higher attenuation if there is infection. Awall does not generally enhance unless infection hasoccurred.
MRI demonstrates the anatomy to much greateradvantage. The lesion is usually seen as a roundedcyst posterior to the mandible and anterolateral tothe major vessels, often displacing the sternomastoidmuscle posteriorly. A beak extending between theinternal and external carotid arteries (Fig. 13.11)ispathognomonic for second branchial cleft cyst (HARDING HAM and GOLDING 2000). On MRI the cyst contents, like any fluid, show as low signal on Tl- andhigh signal on T2-weighted images. If there are blood,
a
c
b
Fig. B.lla-c. Second branchial cleft cyst. a Axial andb coronal T2-weighted images show a cyst in the rightposterior submandibular region with a beak pointingtowards the pharynx. c Axial STIR image. A large leftsecond branchial cleft cyst lies between the submandibular gland anteriorly and the sternomastoid mnscleposteriorly with the carotid artery displaced medially.(Reproduced with permission from HARDING HAM andGOLDING 2000)
![Page 11: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/11.jpg)
Congenital Neck Masses (Non-vascular) 185
a b
Fig. B.12a, b. Infected second branchial cleft cyst. a Axial CT. The cyst has a thick enhancing wall due toinfection which makes it indistinguishable from a simple abscess or from a cystic neoplasm on imaging. b MRISTIR image. This infected cyst has extensive surrounding oedema and may well be mistaken for a neoplasm.It would therefore require biopsy in addition to drainage. (Reproduced with permission from HARDING HAM
and GOLDING 2000)
protein or cholesterol crystals in the cyst, the Tlweighted images may have a higher signal. A septummay be identified within the cyst and the cyst isdemonstrated within the carotid sheath. If there isinfection, the walls become irregular and thick (Fig.13.12a) with internal debris and lymphadenopathy.This, with surrounding oedema, may well have theappearance of a malignant process (Fig.13.12b).
The differential diagnosis includes necrotic neuraltumour, cervical abscess, submandibular gland cyst,cystic lymphangioma, necrotic malignant tumourand inflammatory lymphadenopathy (HARDING HAMand GOLDING 2000). Early surgical excision is advisedbecause of the high risk that the cysts may becomeinfected.
13.7Piriform Sinus Fistula (Abscess)
The piriform sinus is a rare branchial pouch anomaly(Choi and Zalzal 1995). Most piriform sinus fistulaeare located on the left side of the neck, sometimes witha sinus tract through the left lobe of the thyroid gland.The sinus tract extends from the apex of the piriformsinus to the thyroid region. It is rarely detected unlessinfected, when it presents as a neck abscess, draining
sinus, acute suppurative thyroiditis or even mediastinal abscess (LEE 1999). The fistulae may presentin childhood or adulthood. They commonly presentas painful neck swellings, with patients experiencingfever and painful dysphagia over a period of yearsfrom childhood. Often the patients have undergonemultiple surgical procedures with only temporary resolution of the abscess. There is no gender preferenceand patients have been reported from as early 2 daysto as late as 67 years of life (BURGE and MIDDLETON1983; PARK and PARK 1993). 93% of the fistulaeare left-sided (GODIN et al. 1990), although bilateraland right-sided presentations have been recorded.Although there may be recurrent episodes, the firstsymptoms start before 14 years of age (LEE 1999).Contrast studies usually demonstrate the fistula witha tract running from the left piriform fossa to theexterior in the lower neck (Fig. 13.13). It is advisableto perform the contrast study 2 months after acuteinfection since the oedematous tract may not permitpassage of contrast into the tract (LEE 1999). Thefistula can also be demonstrated by endoscopy, butfalse negative results may occur (COTE and GIANOLI1996). In the acutely infected stage, CT or MRI willdelineate the extent of the infection. Treatment is bycomplete excision of the fistulous tract, performedsoon after the contrast study when the patient hasbeen free of infection for a period of time.
![Page 12: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/12.jpg)
186
Fig. 13.13. Piriform sinus fistula. Barium swallow demonstrates a fistula tract extending from the apex of the left piriform sinus to the lower neck near the clavicle. (Reprinted withpermission from LEE 1999)
13.8Thymic Cyst
Thymic cysts originate from the persistence ordegeneration of the thymopharyngeal ducts. They areknown as one of the rarest congenital neck masses,but are probably under-recognised since many areasymptomatic and may well be discovered incidentally (SPIGLAND et al. 1990). They are usually on theleft side of the neck and in about 50% of cases arecontinuous with the mediastinum, due to the fact thatthe thymus embryologically develops in the neck andmigrates to the superior mediastinum. This mediastinal extension requires different management fromother congenital neck masses (KELLEY et al. 1997).The thymus develops as an outgrowth from the ventral aspect of the third pharyngeal pouch, whichdivides into a dorsal wing, to become the inferiorthyroid gland, and a ventral wing, which becomes thethymus gland (SPIGLAND et al. 1990). The thymusdescends into the mediastinum. It is therefore notuncommon for thymic tissue to remain in the neck:prevalence has been reported to be as high as 21 %
A. W.Duncan
(LAU et al. 1984). These thymic anomalies may besolid or cystic. The solid thymic tissue is most likelydue to arrest of thymic tissue during the descent ofthe gland; these entities are usually small and donot present clinically. Cystic thymic tissue usuallypresents clinically, similar to other congenital neckanomalies. There are several theories as to the originof the thymic cyst, but the most plausible are cysticdegeneration of the Hassall's corpuscles, and cysticchange to the remnants of the thymopharyngeal duct(SPEER 1938; SPIGLAND et al. 1990). This duct formsas a tubeless structure by elongation of the dorsalwing of the third pharyngeal pouch. It usually atrophies and disappears, but may remain and becomecystic (KELLEY et al. 1997). Most cysts are multilocular with clear or straw-coloured fluid. Occasionallythey may be semi-solid with necrotic debris and oldblood. Cholesterol crystals have been found withinthe lumen, suggesting previous haemorrhage. Ulceration of the epithelial wall occurs, and there may beinfection resulting in fibrous tissue development. Thecyst wall can vary in thickness from a few millimetresto a centimetre (KELLEY et al. 1997).
Cervical thymic cysts usually present in the firstdecade of life and 75% at less than 20 years. There is2:1 male-to-female dominance. The cysts are usuallysolitary but may be multiple (HYDE et al. 1944). Mostpatients have an antecedent history of the presenceof mass for 6-9 months, sometimes presenting orincreasing in size due to infection or haemorrhage(KELLEY et al. 1997). Fluctuation in size with recentupper respiratory infection is a relatively commonfinding (WAGNER et al. 1998). The cysts are foundin the lower third of the neck anterior to and extending beneath the sternomastoid muscle, but they mayoccur in the trachea, posterior pharynx and piriformsinus. Dysphagia, dyspnoea, hoarseness or cervicalpain occurs in up to 10% of patients due to compression and displacement of the adjacent structures.With large congenital thymic cysts, severe respiratorycompromise may occur, especially in neonates, dueto extrinsic compression or intrinsic obstruction bythe mass within the trachea. This is particularly thecase if there is mediastinal extension. The mass mayextend into the mediastinum as a solid or cystic massor a fibrous cord. Occasionally there may be vocalcord paralysis due to traction on the recurrent laryngeal nerve. Pericardial tamponade has been reported(McLEOD and KARANDY 1981). Valsalva manoeuvremay produce transient increase in size due to vascular engorgement or transmitted intrathoracic pressure (KELLEY et al. 1997). This does not occur witha branchial cyst, which helps differentiate the two
![Page 13: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/13.jpg)
Congenital Neck Masses (Non-vascular)
lesions. Most thymic cysts are congenital in origin,but infection, neoplasm, radiation therapy, traumaand thoracotomy may all be aetiological agents(MURAYAMA et al.1995). The clinical differential diagnosis includes cystic hygroma, cystic thymic tumouror teratoma with cystic change, abscess, lymphadenopathy, thyroid adenoma, parathyroid cyst, branchial cleft cyst, dermoid and epidermoid cyst, or, ifmidline in location, thyroglossal duct cyst (KELLEY etal. 1997; CASTELLOTE et al. 1999).
The first imaging modality for differentiating theselesions is ultrasound. A thymic cyst may appear asa homogeneous, non-homogeneous or cystic mass(KELLEY et al. 1997). It may show mediastinal extension, and if this is suspected then a chest X-ray isrequired. This may be more difficult to evaluate inyounger children under 2 years of age when thethymus is normally present. If the cyst is large, MRIis the investigation of choice as it shows the detailedanatomy in multiple planes as well as better tissuecharacterisation. The cyst is well defined, often withthin septa, and lies partially within the carotid sheath.The fluid contents have a low signal on Tl-weightedimages, but this may be higher if there is blood orprotein in the cyst. High signal will occur in fluidfilled lesions on T2-weighted scans. MRI or, whenthis is not available, CT will show the thymic originof tissue by demonstrating mass within the carotidsheath and connection to the thymus and mediastinum (LAu et al. 1984). On CT the thymic cystappears as a large, homogeneous mass of water density (Fig. 13.14). Fine-needle aspiration has not beenuseful as an aid to diagnosis (LYONS et al. 1981).Complete surgical excision of the cyst is the recommended treatment, and the possibility of mediastinalextension should always be considered even if thishas not been definitely demonstrated prior to sur-
Fig. 13.14. Thymic cyst. CT scan shows a large left cysticmass with deviation of the airway to the contralateral side.(Reprinted with permission from KELLEY et al. 1997)
187
gery. Partial excision of the cyst may be necessaryto relieve symptoms in the neonate unless separatemediastinal thymic tissue has been identified byimaging (GILMORE 1941; SPIGLAND et al. 1990).
13.9Cervical Extension of the MediastinalThymus
When there is incomplete descent of the thymus, itmay remain as a solid midline structure at the thoracic inlet. Although up to 40% of infants may havethymic tissue in the neck, it is only rarely that itpresents as a small midline mass (ZARBO et al. 1983;BENSON et al. 1992). It may lie laterally, more commonly on the left side. Most are asymptomatic, apartfrom the neck swelling, but hypertrophied tissue mayrarely cause dyspnoea or dysphagia due to compression (LEWIS 1962). Malignancy has been reported(GRAY and SKANDALAKIS 1972). Ultrasonography,CT and MRI will show the imaging features of anormal thymus, and may demonstrate the connection with the mediastinal thymus (Fig. 13.15).
Fig. 13.15. Cervical thymus. Oblique sagittal Tl-weightedimages. MRI shows extension of the thymus from the anteriormediastinum to the lower neck (arrows). (Reprinted with permission from CASTELLOTE et al. 1999)
13.10Dermoid/Epidermoid Cyst
Dermoid and epidermoid cysts develop due to ectodermal elements being buried beneath the skin(BROWN and AZIZKHAN 1998). Dermoid cysts containglandular elements, which differentiates them from
![Page 14: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/14.jpg)
188
epidermoid cysts. They both contain sebaceous material (McAvoy and ZUCKERBRAUN 1976). Althoughdermoid cysts are common lesions in the head andneck of young children, they usually present in thehead rather than the neck. When they occur in theneck they usually lie in the mid superior cervicalregion, overlying or above the hyoid bone. In thislocation they may be confused with a thyroglossalduct cyst. However ,because they lie subcutaneouslyand are mobile, the clinical examination differentiates a dermoid cyst from a thyroglossal duct cyst.This is of clinical importance as a simple excision of adermoid cyst can be done intact and requires no dissection to find any extension internally (TELANDERand FILSTON 1992). An enlarged lymph node overlying the hyoid bone should be included in the diagnosis of a thyroglossal duct cyst or dermoid. Investigation is rarely necessary, but ultrasound can easilydifferentiate the solid-looking mass due to fat andkeratin of the dermoid from a cystic structure orcharacteristic lymph node (TEELE and SHARE 1991).Although rare, malignant transformation has beenreported in dermoid cysts (McAvoY and ZUCKERBRAUN 1976).
13.11"Plunging" Ranula
Ranulas are not true congenital lesions, but areacquired inflammatory retention cysts of the sublingual salivary gland due to duct stenosis or occlusion(QUICK and LOWELL 1977) which may be congenital. This sublingual salivary cyst usually presentsbeneath the tongue as a glistening mass in the floorof the mouth. It was given its name by Hippocratesbecause of its likeness to the belly of a little frog. The"plunging" ranula is an uncommon lesion resultingfrom rupture of the duct and extravasation of thisfluid containing amylase into the submental region,where it presents as a pseudocyst without an epitheliallining (BROWN and AZIZKHAN 1998). If midline,it may sometimes be confused with the thyroglossal duct cyst (KHAFIF et al. 1975). Other differential diagnoses include a midline cervical dermoidand lymph node (TELANDER and FILSTON 1992).Ultrasound will demonstrate the cystic nature ofthe lesion. MRI demonstrates the thin-walled cysticcollection with an intermediate signal on Tl- anda high signal on T2-weighted scans consistent withfluid, the bulk of the lesion being in the submandibular space with a characteristic connection to the
A. W.Duncan
floor of the mouth (Fig. 13.16) (HARDINGHAM andGOLDING 2000). It can be seen on CT, but this hasthe disadvantage of involving radiation and doesnot give the same spatial relationship or tissuecharacterisation.
13.12Ectopic Thyroid Gland
The thyroid gland appears embryologically as a midline diverticulum of the pharyngeal floor between thefirst and second branchial arches (SADLER 1990). Theregion of the tongue where the thyroid develops isthe site of the foramen caecum. The thyroid diverticulum becomes bilobed and descends into the neck.As the thyroid descends it remains connected tothe pharyngeal pouch by the thyroglossal duct. Thethyroid diverticulum descends anterior to the hyoidbone and larynx and arrests just inferior to the thyroid cartilage and upper tracheal rings. Any abnormality in this descent may result in an ectopic location of the thyroid gland. This is usually at the baseof the tongue, below the tongue, or in a pre-laryngealand substernal position. The ectopic thyroid glanditself is usually of no consequence. However, if it lieshigh in the neck and is mistaken for a thyroglossalcyst, there may be a problem if it is inadvertentlyremoved, as this will result in profound hypothyroidism (LEUNG et al. 1995).
The ectopic thyroid gland is extremely rare, witha prevalence of 1 per 100,000-300,000 persons, and isreported to occur in 1 per 4,000-8,000 patients withthyroid disease (YEUNG et al. 1987). Although a congenital lesion, it usually presents later in life with adifferential diagnosis of epidermoid cyst, lymphadenopathy, lipoma, lymphangioma, sebaceous cyst and,rarely, midline branchial cyst. Any midline neck massmerits clinical examination of the thyroid gland inaddition to the mass, to ensure that the normal thyroidgland is detected. If a normal gland is not detected, orif ectopic thymus tissue is suspected, ultrasonographyshould be performed (NOYEK and FRIEDBERG 1981).An ectopic thyroid gland presenting as a mass will, onultrasound, have the same characteristics as a normalthyroid gland, and ultrasound will also show its relationship to other structures. MRI or CT will confirmthis, although this is rarely necessary. If there is stilldoubt, radionuclide scanning should show the location, size and activity of the functioning thyroid tissue(Fig. 13.17). There is a full discussion of radionuclidescanning of the thyroid gland in Chap. 23.
![Page 15: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/15.jpg)
a
a
Congenital Neck Masses (Non-vascular)
Fig. 13.16a, b. Plunging ranula. a Axial and b coronal T2-weighted images of the left-sided plungingranula extending into the sublingual and submandibular spaces. (Reproduced with permission fromHARDING HAM and GOLDING 2000) b
b
189
Fig.13.17a, b. Ectopic thyroid gland. Scintigraphy demonstrates a the anterior and b the lateral projection of the lingual thyroid
An ectopic thyroid gland is usually associatedwith normal thyroid function in children (GRANT
et al. 1978). However, it may be associated withhypothyroidism in 33% of patients (NEINAS et al.1973). The gland secretes thyroxine but in insufficient amounts (LEUNG 1986). It is therefore important to estimate T4, T3 and TSH in all patients withectopic thyroid. Hypothyroidism may become manifest in periods of physiological stress and goitremay develop within the ectopic thyroid gland. If a
child is asymptomatic and euthyroid with ectopicthyroid gland, no treatment is necessary apart fromcontinued observation. Where there is deficiency ofthe thyroid hormone, elevated TSH levels or physiological impairment due to obstruction, or glandenlargement producing disfigurement, then thyroid supplements are advocated. Some authorities(KANSAL et al. 1987) suggest that there should belifelong thyroxine suppression to prevent enlargement of the gland.
![Page 16: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/16.jpg)
190
13.13Sternomastoid "Tumour"
Congenital sternomastoid "tumour" is part of a spectrum of abnormality causing congenital torticollis.Torticollis varies from a palpable sternomastoid mass,through thickening of the sternomastoid muscle, tothe final group due to postural head tilt or oculartorticollis. The last group shows no detectable organicabnormality of the sternomastoid muscle and may bedue to some localised muscular dysfunction resultingin an imbalance in the action of the muscles, leadingto torticollis (GOLDEN et al. 1999). It may present asa sign of ocular torticollis due to a squint or, in theolder age group, cerebellar tumour, or cervical rotarysubluxation. Congenital neck anomalies can occur inassociation with vertebral anomalies, particularly ofthe cervical vertebrae. Torticollis is the most commonmuscular presentation of craniovertebral junctionanomalies in older children (MANALIGOD et al.1999).There is another disorder, benign paroxysmal torticollis, which is an episodic functional disorder ofunknown aetiology occurring in the first few monthsof life, with the child's head tilted to one side for afew hours or days without any associated signs. Thedisorder is self-limiting. It is important to recognisethe difference in order to avoid carrying out numerous investigations (DRIGO et al. 2000).
Congenital muscular torticollis or sternomastoidtumour, or "fibromatosis colli" as it is also known, isof debatable aetiology but the high rates of obstetrical complications leads some authorities to the conclusion that birth trauma is probably the main aetiological factor (Ho et al. 1999). However, there areother theories that suggest that the presence of maturefibrous tissue in the neonate would indicate that thecondition occurs prior to birth and is more likely tobe the cause rather than the effect of obstetrical problems. There is further support for this view - that thecondition is caused by intrauterine position - sincethere is an association of congenital dislocation ofthe hip and tibial torsion with torticollis (BROWN andAZIZKHAN 1998). Fibrosis and shortening of the sternomastoid muscle pulls the head and neck toward theaffected side (ARMSTRONG et al. 1965). Pathologicallythere is fibrous tissue between bundles of normalmuscle (MIDDLETON 1930). Clinically there is no predilection for the side or sex of the patient. The mass isusually noted between 2 and 8 weeks of age, and themajority before 6 months (Ho et al. 1999). The childpresents with a characteristic posture with face andchin tilted away from the affected side and the headtilted toward the ipsilateral shoulder.
A.W. Duncan
Ultrasonography shows increased echogenicity dueto the fibrous tissue (Fig. 13.18). The normal sternomastoid muscle is hypoechoic with the facial planesinterspersed with the muscle producing thin, linear,echogenic lines. The presence of a "tumour" is demonstrated by the increased echogenicity and alsoincreased size. In classical cases there is a fusiformmuscle enlargement, but at times there may be generalised muscle enlargement only. Although generallyhyperechoic, the "tumour" is occasionally hypoechoicand sometimes has mixed echogenicity (BEDI et al.1998). The ultrasonographic appearances correlatewith the pathology and Hsu (Hsu et al.1999) classifiedthem into four types: (1) fibrotic mass in the involvedmuscle; (2) diffuse fibrosis mixed with normal muscle- the most common, accounting for over three-quarters of cases; (3) diffuse involvement of the musclewithout any normal muscle (uncommon type); (4)fibrotic cord in the involved muscle, the rarest type.Types 1 and 4 are more likely to undergo surgicaltreatment, type 3 much less so. The lower third of themuscle is most commonly involved, but with increasing severity the whole of the muscle becomes involved.In severe cases, without appropriate treatment, facialand cranial asymmetry will develop within 6 months.
The majority of cases of neonatal torticollisrespond to physiotherapy and postural changes, forcing the infant to look to the contralateral side. Mildcases need observation only. Development of facialhemihyperplasia is the main reason for surgical intervention. However, the ultimate decision of whethersurgical intervention is necessary is clinical andit may necessitate serial ultrasound examinations(Fig. 13.19) to aid clinical judgement.
Fig. 13.18. Sternomastoid tumour. This shows a typical hyperechoic thickened sternomastoid tumour compared with thenormal muscle
![Page 17: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/17.jpg)
a
c
Congenital Neck Masses (Non-vascular)
13.14Congenital Teratoma
Teratomas are a rare cause of neck masses; although10% of childhood teratomas occur above the level ofthe clavicles (BERRY et al.1969),only 3% occur in thecervical region (JORDAN and GAUDERER 1988) andmost of these present in the newborn period. Theymay obstruct the airway and be life-threatening, andmay be associated with maternal polyhydramnios(HAJDU et al. 1966). When found in the neck theyhave an intimate relationship to the thyroid gland,although there is no evidence to suggest that they arisefrom the gland. Almost all are congenital in origin.The cells of a teratoma arise from pluripotential primordial germ cells and may give rise to many tissues foreign to the organ in which they originate.
191
Brain tissue is the most frequent component,but othertissues such as bronchoepithelium, thyroid elements,cartilage and ependymal cysts are also found.
Congenital teratomas are invariably benign compared with those presenting later in life (FILSTON1994). Serum a-fetoprotein and ~-HCG levels areoften elevated.
Congenital lesions give rise to problems duringpregnancy and delivery because of the size of thetumour. Polyhydramnios occurs in up to 19% ofcases due to impairment of swallowing, which ismore common with the larger lesions (WELCH 1986;FILSTON 1994). The large size also results in obstructedlabour, premature labour and sometimes stillbirth(WELCH 1986). Even after delivery mortality may ariseas a result of respiratory compromise, and even withsurgery it occurs in 10% of cases. Without treatment
b
d
e
Fig.13.19a-e. Ultrasonograms of the evolution of the sternomastoidtumour. a Longitudinal section shows the slightly hypoechoic centralportion of the sternomastoid, which is increased in bulk comparedwith the narrow normal lower end of the sternomastoid muscle.b The transverse section shows the prominent bulk of the sternomastoid tumour. c A week later, the longitudinal section shows thetumour becoming more hypoechoic in relation to the muscle. dTransverse sections comparing the two sides of the neck show theincreased bulk on the left compared with the normal muscle on theright. e Two months later the longitudinal section shows the massreducing and becoming more uniform in thickness rather than afocal tumour. The echogenicity is returning to more normal muscle
![Page 18: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/18.jpg)
192
the mortality can be between 80% and 100% (WELCH1986). Congenital teratomas are frequently recognised in utero by ultrasonography, which gives a greatadvantage in preparing for delivery and subsequentimmediate postnatal care, particularly in relation torespiratory compromise by the effect of the mass onthe airways. The teratoma presents as a large, usuallyunilateral mass with a differential diagnosis of cystichygroma. It may be difficult to distinguish teratomasfrom cystic hygromas when they are extremely largeand cystic, but calcification, which is seen in 50%of teratomas on plain films, will help to distinguishbetween the two conditions (WELCH 1986). Ultrasound will demonstrate thin-walled cysts and calcification, if present, by increased echogenicity withacoustic shadowing. CT will show calcification andcystic lesions. If calcification is not present, distinction from cystic hygroma may be difficult. MRI showsthe extent of the tumour and its spatial relationshipsto much better advantage than CT. It also gives bettertissue characterisation and involves no radiation. Itusually shows a multi-loculated cystic structure witha high signal on T2-weighted scans due to fluid withinthe cyst. The presence of fat, giving a high signal onTl-weighted images, a low or absent signal on STIRsequences, and a signal void from calcification willhelp to distinguish it from cystic hygroma (GREEN etal. 1998) (Fig. 13.20). Formed structures resemblingfingers or limbs have been described, and there maybe intradural extension (FULMER et al.1997).
Even after surgical removal there may be problemsrelated to pulmonary insufficiency and chondromalacia due to the mass effect in utero (LARSEN et al.1999), and hypothyroidism has been reported following excision of a large cervical teratoma. If identifiable thyroid tissue is not seen at the conclusion ofsurgical removal, a thyroid function test should beperformed postoperatively (CHOWDHARY et al.1998).Follow-up with determination ofserum a-fetoproteinand B-HCG levels is usually used to detect tumourrecurrence in those cases that are malignant.
13.15Cervical Neuroblastoma
Neuroblastomas are probably all congenital in origin,originating from the neural crest, and therefore willoccur anywhere there is sympathetic neural tissue.They are a common malignant tumour in infancy,although rare in the cervical region. Most neuroblastomas occur below 5 years of age, and cervical neuro-
A. W.Duncan
Fig. 13.20a, b. Congenital teratoma. a Axial T2-weighted MRIdemonstrates the large tumour with cystic components withseveral fluid levels. b Oblique sagittal inversion recovery section shows the high signal due to fluid. The dense signal voidprobably represents some calcification, with a slightly highsignal around representing haemorrhage
blastoma under 1year of age; sometimes they presentsoon after birth, with stridor, dyspnoea and swallowing difficulties in addition to the visible mass (TAlet al. 1997). The tumour has a favourable prognosiscompared with neuroblastoma at other sites, probably in part due to its early visible presentation. Whenpresenting other than in the newborn period, themasses are commonly mistaken for infectious adenitis (ABRAMSON et al. 1993). Serum and urinarycatecholamine concentrations are usually elevated.The first examination to be carried out is most likelyultrasonography, which will show a solid mass withvascular displacement and possibly narrowing of thevessels. If there is calcification, this will show as echogenic areas with acoustic shadowing (Fig. 13.21a).Plain chest X-ray will show any calcifications and anyintrathoracic extension, which may also be seen on
a
b
![Page 19: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/19.jpg)
Congenital Neck Masses (Non-vascular) 193
Fig. 13.21a-c. Congenital neuroblastoma. a Longitudinal ultrasound shows a large cervical mass with areas of hyperechogenicity probably representing calcification. b Axial CT scanshows a large tumour on the right with slightly lower attenuation than adjacent muscle, with small areas of increased attenuation probably representing calcification. There is displacement of the airway to the left side with some narrowing. cMIBG 1231 scan, anterior projection, shows high uptake of theisotope in the neuroblastoma
ultrasound. Destructive bone changes may be seen,although since the lesion is usually detected earlythese are rare. MRI is the investigation of choice toshow the extent of the lesion and also any intraspinal extension. CT (Fig. 13.21b) will show calcificationto better advantage than MRI. Cervical neuroblastoma may present as Horner's syndrome. However,Horner's syndrome with no evidence of a mass onclinical examination or ultrasound, and with normalvanillylmandelic acid levels and no other clinicalsigns such as heterochromia, requires no furtherinvestigation (GEORGE et a1. 1998). There is highuptake of MIBG (metaiodobenzylguanidine) in neuroblastoma in most cases (Fig. 13.21c). The welldifferentiated form of neuroblastoma, ganglioneuroblastoma, may also occur but is extremely rare(AL-JASSIM 1987).
13.16Laryngocele
Laryngoceles are not truly congenital lesions unlessone considers that the weakness in the laryngeal ventricle is of congenital origin and responsible for dilatation. They usually occur as a result of increasedintraglottic pressure. An internal laryngocele is morecommon and presents as stridor. The rarer externallaryngocele presents as a lateral neck mass, oftenincreasing in size with a Valsalva manoeuvre. Ultrasound is of little value in uncomplicated casesbecause the air-filled sac produces artefact. Plainfilms will show an air-filled lateral structure (Fig.13.22). Laryngoceles may be imaged by CT or MRI,which demonstrates a unilocular air- or fluid-filledcyst (Fig. 13.23). Fluid levels may be seen. Externallaryngoceles lie mainly within the submandibularspace and may communicate through the thyrohyoidmembrane to the internal component, although thismay have collapsed and not be visible (HARDING HAMand GOLDING 2000).
13.17Lung Herniation
Lung herniation is protrusion of the lung beyond theconfines of the thorax. The herniation may be cervical, intercostal or diaphragmatic. Most lung herniations are acquired due to trauma or surgery or secondary to a neoplastic or inflammatory process, or
c
a
b
![Page 20: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/20.jpg)
194
else spontaneous, although 20% are considered to becongenital (BHALLA et al. 1990; MONCADA et al. 1996).Congenital cervical herniation is due to agenesis ofSibson's fascia. Most are asymptomatic or present witha few infrequent or vague symptoms. Clinically theyappear as a painless, rhythmic bulge of the supraclavicular region that increases with respiratory effort(MONCADA et al. 1996). Congenital cervical lung herniation has been described with multiple hernia, leading to the theory that it may be a defect in the coelomicmesoderm (ZAGLUL and ODITA 1995). The diagnosiscan be established with a plain radiograph showingherniation at the apex into the neck. This is accentuated by a Valsalva manoeuvre. In most cases notreatment is required but just reassurance, althoughif the herniation is large, clinically progressive orcauses respiratory distress, surgical intervention maybe necessary (GONZALES-DEL-REY and CUNHA 1990).In addition to the symptoms a cosmetic problem maywell also arise, requiring repair of the fascial defect(BRONSTHER et al. 1968). One should also be awareof the possibility of a pneumothorax in this group ofpatients (DEVGAN and BRODEUR 1976).
Fig. 13.22. Laryngocele. The appearance is of an air-filledcavity on the lateral projection, which would be compatiblewith a laryngocele or oesophageal diverticulum. Oral contrast,however, does not fill it and suggests that this is not related tothe oesophagus. In fact, it actually represented duplication ofthe larynx, which has a similar appearance
A.W.Duncan
Fig. 13.23. Axial CT shows bilateral externallaryngoceles. Theleft laryngocele contains only air. On the right there are airfluid attenuation contents together with a soft tissue attenuation component which would suggest infection or malignancy.(Reproduced with permission from HARDING HAM and GOLD
ING 2000)
13.18Thyroid Gland Hemiagenesis
Hemiagenesis of the thyroid gland presents as anuncommon mass due to hypertrophy of a single thyroid lobe or due to thyroid dysfunction. It is morefrequently seen on the left side and may be an incidental finding (DE REMIGIS et al. 1985. Functionalhemiagenesis, identified scintigraphically, can be differentiated from anatomical hemiagenesis by ultrasonography, which on the transverse section showsabsence of one side of the gland with a normalappearing contralateral side and isthmus, producing the so-called hockey stick sign (Vazquez et al.1995). Scintigraphy identifies functioning tissue. Ifthe gland is non-functioning, it will be seen on ultrasound. If it is true hemiagenesis, it will not be seenon either modality.
13.19Midline Cervical Cleft
This unusual anomaly appears as a long, linear skindefect but can occasionally be associated with scarring contracture, which can produce a small masseffect.
![Page 21: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/21.jpg)
Congenital Neck Masses (Non-vascular)
13.20Bronchogenic Cyst
These are rare congenital lesions that usually arisenear the hilar region, presenting due to infectionor compression of vital structures. They have beendescribed as an unusual cause of a lump in the neck(RAPADO et al. 1998).
13.21Lingual Thyroid Gland
Thyroid rests may occur anywhere along the thyroglossal duct. The majority lie near the foramencaecum of the tongue. Occasionally a goitre may resultin airway obstruction. Ectopic tissue in 77% of casesis the only functioning thyroid tissue (VAZQUEZ et al.1995). In congenital hypothyroidism ultrasonographyis usually performed when a normally located glandis not felt (MILLER 1985). Thyroid scintigraphy willconfirm this (Fig. 13.17). However, if the tissue is nonfunctioning it will yield false negative results.
13.22Congenital Vascular Lesions
These may present as masses. The reader is referredto Chap. 20 for a full discussion of vascular lesions.
13.22.1 Haemangioma
Haemangiomas are the most common congenitallesions of the head and neck in childhood, occurring in about 2.5% of all newborn infants ( MacCollum and Martin 1956). They are uncommon in theneck apart from the back of the neck. They occurpredominantly in the skin and mucosa but can beinvasive. Cutaneous haemangiomas present primarily in infants and young children. The capillary typeusually involutes spontaneously while the cavernoustype regresses only when it has been present frombirth (Edwards 1993). The capillary types tend tothe appearance of a flattened strawberry and haveno mass effect. Cavernous types have large vascularspaces and are compressible, being raised above theskin with a warty granular surface (Potter 1976).Mixed capillary and cavernous types produce theraised vascular strawberry naevi. Haemangiomaswith cavernous components may grow massively.
195
Although present at birth, most do not becomenoticeable until after the first month of life. Most willinvolute spontaneously, but a small proportion maybecome quite large and present a difficult management problem due to airway obstruction, involvement of vital organs, cardiac failure or coagulationproblems due to platelet trapping.
The first investigation of a mass suspected to bea haemangioma is ultrasonography, which will showhypoechoic areas with echogenic septations. The capillary areas, due to echoes from the walls of the vessels, may show as an echogenic region. The echogenicity can also be due to thrombosis. For the moreextensive lesions, MRI or, if that is not possible,CT demonstrates the extent of the lesion. Contrastenhanced CT will show the vascular nature of thelesion.
Most haemangiomas require no more than observation unless they become a clinical managementproblem, when more aggressive therapy may beneeded. A full account of the imaging and management is given in Chap. 20.
13.22.2Varix of the Jugular Vein
Localised swelling in the neck during strammg,coughing or crying may be due to fusiform dilatation of the jugular vein. This is readily shown byultrasound demonstration of its expansion on theValsalva manoeuvre, and also by the presence of flowon Doppler imaging (KOVANLIKAYA et al. 1990).
13.22.3Carotid Artery Aneurysm
Carotid artery aneurysms are extremely rare in children, trauma and infection being the usual causeswhen they do occur. Congenital carotid artery aneurysms due to a defect in the arterial wall areeven rarer and may be a manifestation of a generalised connective tissue disorder, such as Ehlers-Danlos, Marfan's, Kawasaki's or Maffucci's syndromes(VAZQUEZ et al. 1995). They can readily be evaluatedby ultrasound.
13.22.4Cervical Aortic Arch
The high position of the aortic arch may manifestitself due to compression of the airways or oesopha-
![Page 22: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/22.jpg)
196
gus producing respiratory difficulties or dysphagia.It is usually a right-sided aortic arch and may beassociated with other cardiac or vascular anomalies(DOORENBOS et al. 1991). It may be asymptomatic.Very occasionally this congenital extension of theaortic arch into the neck may produce a pulsatileneck swelling (MURRAY and NEGRETTE 1989). Asa mass in the neck it can be identified by ultrasound and its nature determined with flow identifiedby Doppler ultrasonography. Plain films may showindentation of the trachea. Tl-weighted MRI willshow the high position of the arch passing throughthe thoracic inlet (CASTELLOTE et al. 1999).
13.23Rare Congenital Tumours, Cystsand Infections
Very rare congenital tumours such as rhabdoid tumour(COSTES et al. 1997), neurofibroma (KOKANDKAR et al.1994), fibrosarcoma (Fig. 13.24) (BooN et al. 1995) andforegut cysts (COHEN et al. 1985) may present as neckmasses. Congenital infections such as tuberculosis canpresent with neck masses but rarely do (THORA et al.1985). Parathyroid cysts are rare and of questionableembryonic origin. They usually present in the adult asa painless neck mass that is occasionally symptomatic(GRAY and SKANDALAKIS 1972).
Fig. 13.24. Fibrosarcoma. Axial CT scan of the neck withintravenous contrast shows a large mass in the right side ofthe neck displacing the airway anteriorly and laterally. It haspatchy enhancement, particularly of the rim
A.W. Duncan
13.24Summary
Congenital neck lesions are a common finding in thepaediatric age group and must be differentiated fromlesions from other causes. Clinical examination willindicate the nature of most lesions. Ultrasonography is the first line of investigation; it can differentiate between cystic and solid lesions, and in manyinstances will reveal the nature and extent of thelesion. When the lesion has a solid component it isalways important to identify a normal thyroid glandto ensure that the only functioning thyroid tissue isnot removed at surgery. Larger lesions are evaluatedby MRI, particularly Tl-weighted sequences, for thespatial relationships, or, if MRI is not available, CT.Occasionally isotope studies are needed to identifyfunctioning thyroid tissue, and a contrast swallowmay in rare instances aid diagnosis.
References
Abramson SJ, Berdon WE, Ruzal-Shapiro C, et al (1993) Cervicalneuroblastoma in 11 infants - a tumour with a favourableprognosis. Clinical and radiological findings. Pediatr Radiol23:253-257
Ahuja AT, King AD, Kew J, et al (1998) Head and neck lipoma:ultrasound appearances. Am J NeuroradioI19:505-508
Ahuja AT, King AD, Metreweli C (2000a) Sonographic evaluation of thyroglossal duct cysts in children. Clin Radiol55:770-774
Ahuja AT, King AD, Metreweli C (2000b) Second branchial cleftcysts: variability of sonographic appearances in adults. AJNRAm J NeuroradioI21:315-319
Al-Jassim AH (1987) Cervical ganglioneuroblastoma. J Laryngol-Otol101:296-301
Armstrong D, Pickerell K, Felter B, et al (1965) Torticollis. Ananalysis of 271 cases. Plast Reconstr Surg 35:14-19
Bhalla M, Leitman BS, Stern E, et al (1990) Lung hernia: radiographic features. AJR Am JRoentgenoI154:51-53
Battino RA, Khangure MS (1990) Is that another Thornwaldt'scyst on MRI? Australas Radiol34 (1) Feb:19-23
Bedi DG, Jotin SD, Swischuk LE (1998) Fibromatosis colli ofinfancy: variability of sonographic appearances. J Clin Ultrasound 26:345-348
Benson MT, Dalen K, Mancuso AA, et al (1992) Congenitalanomalies of the branchial apparatus, embryology and pathological anatomy. Radiographies 12:943-960
Berry CL, Keeling J, Hilton C (1969) Teratomata in infancy andchildhood: a review of 91 cases. J Patho198:241
Bill AA, Sumner DS (1965) A unified concept of lymphangiomaand cystic hygroma. Surg Gynecol Obstet 120:79-86
Biurrun 0, Olmo A, Barcelo X, et al (1992) Thornwaldt's cyst.The experience of a decade. An Otorrinolaringol Ibero Am19:179-189
Boon LM, Fishman SJ, Lund DP, et al (1995) Congenital fibrosarcoma masquerading as congenital haemangioma: reportof two cases. J Pediatr Surg 30:1378-1381
![Page 23: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/23.jpg)
Congenital Neck Masses (Non-vascular)
Boucher RM, Hendrix RA, Guttenplan MD (1990) The diagnosisof Thornwaldt's cyst. Trans Pa Acad Opthalmol Otolaryngol42:1026-1030
Brewis C, Mahadevan M, Bailey CM, et al (2000) Investigationand treatment of thyroglossal cysts in children. J R Soc Med93:18-21
Bronsther B, Coryllos E, Epstein B, et al (l968) Lung hernia inchildren. J Pediatr Surg 3:544-550
Brown RL, Azizkhan RG (1998) Pediatric head and neck lesions.Pediatr Clin North Am 45:889-905
Burge D, Middleton A (1983) Persistent pharyngeal pouch derivatives in the neonate. J Pediatr Surg 18:230-234
Castellote A, Vazquez E, Vera J, et al (l999) Cervico-thoraciclesions in infants and children. Radiographics 19:583-600
Choi SS, Zalzal GH (l995) Branchial anomalies: a review of 52cases. Laryngoscope 105:909-913
Chowdhary SK, Chituis M, Perold J, et al (l998) Hyperthyroidism in a neonate following excision of a cervical teratoma.Pediatr Surg Int :212-213
Cohen SR, Thompson JW, Brennal LP (l985) Foregut cysts presenting as neck masses. A report on three children. Ann OtolRhinol Laryngol 94:433-436
Costes V, Medioni D, Durand L, et al (1997) Undifferentiated softtissue tumor with rhabdoid phenotype (extrarenal rhabdoidtumor). Report of a congenital case associated with medulloblastoma in a brother. Ann Pathol 17:41-43
Cote DN, Gianoli GT (l996) Fourth branchial cleft cysts. Otolaryngol Head Neck Surg 114:95-97
Davies MR, Cywes S (l977) Children with thyroid carcinomas.S Afr Med J 52:223-226
De Remigis PD, Angelo M, Bondaduce S, et al (l985) Comparison of ultrasound scanning and scintiscanning in the evaluation of thyroid hemiagenesis. J Clin Ultrasound 13:561-563
Devgan BK, Brodeur AE (1976) Apical penumatocele. Arch Otolaryngol 102:121-123
Doorenbos BM, Mooyaart EL, Hoorntje JC (l991) MR diagnosis of a right cervical arch. J Comput Assist Tomogr15:864-866
Drigo P, Carli G, Laverda AM (2000) Benign paroxysmal torticollis of infancy. Brain Dev 22:169-172
Edwards MK (l993) Magnetic resonance imaging of the headand neck. Dental Clin North Am 37:591-611
Ellis PDM, van Nostrand AWP (l977) The applied anatomy ofthyroglossal duct remnant. Laryngoscopy 87:765-770
Ewing CA, Kornblut A, Greeley C, et al (l999) Presentationof thyroglossal ducts in adults. Eur Arch Otorhinolaryngol256:136-138
Filston HC (l989) Common lumps and bumps of the head andneck in infants and children. Pediatr Ann 18:180-186
Filston HC (l994) Haemangiomas, cystic hygromas, teratoma ofthe head and neck. Semin Pediatr Surg 3:147-159
Fulmer BB, Wilkins RH, Oakes WJ, et al (l997) Midline dorsalappendages. Pediatr Neurosurg 27:242-245
George ND, Gonzales G, Hoyt CS (l998) Does Herner's syndrome in infancy require investigation? Br J Ophthalmol82:51-54
Gilmore JR (1941) Some developmental abnormalities of thethymus and parathyroids. J Pathol 52:213-218
Godin MS, Kearns DB, Pranski SM, et al (l990) Fourth branchial pouch sinus: principles of diagnosis and management.Laryngoscope 100:174-178
Golden KA, Beals SP, Littlefield TR, et al (1999) Sternocleidomastoid imbalance versus congenital muscular torticollis:
197
their relationship to positional plagiocephaly. Cleft PalateCraniofac J 36:256-261
Gonzalez-del-Rey J, Cunha C (l990) Cervical lung herniationassociated with upper airway obstruction. Ann Emerg Med19:935-937
Grant DB, Hulse JA, Jackson DB, et al (1978) Ectopic thyroid:residual function after withdrawal treatment in infancy andlater childhood. Acta Paediatr Scand 78:889-892
Gray SW, Skandalakis JE (l972) The pharynx and its derivatives. In:Embryology for surgeons. Saunders, Philadelphia, pp15-61
Green JS, Dickinson FL, Rickett A,et al (l998) MRI in the assessment of a newborn with cervial teratoma. Pediatr Radiol28:709-710
Hajdu SI, Farugue AA, Hajdu EO, et al (l966) Teratoma of theneck in infants. Am J Dis Child III :412
Hardingham C, Golding S (2000) A guide to branchial derivatives and cysts in the face and neck. Radiol Now 17:2:14-17
Harnsberger HR (l995) Handbook of head and neck imaging.Mosby Year Book, St Louis
Hayes LL, Marlow JF Jr (l968) Papillary carcinoma arising in athyroglossal duct cyst. Laryngoscope 78:2189-2193
Ho BC, Lee EH, Singh K (l999) Epidemiology presentation andmanagement of congenital muscular torticollis. SingaporeMed J 40:675-679
Hsu TC, Wang CL, Wong MK, et al (1999) Correlation of clinicaland ultrasonographic features in congenital muscular torticollis. Arch Phys Med Rehab 80:637-641
Hyde TL, Sellers ED, Owen M (l944) Thymic cyst of the neck.Texas J Med 39:539-540
Jordan RB,Gauderer MW (l988) Cervical teratoma: an analysis.Literature review and proposed classification. J Pediatr Surg23:583-591
Kansal P, Sakati N, Rifai A, et al (1987) Lingual thyroid diagnosisand treatment. Arch Intern Med 147:2046-2048
Kelley DJ, Gerber ME, WiIIging JP (l997) Cervicomediastinalthymic cysts. Int J Pediatr OtorhinolaryngoI39:139-146
Khafif RA, Schwartz A, Fiedman E (l975) The plunging ranula.J Oral Surg 33:537-541
Kokandkar HR, Vyas AS, Kumbhakarna NR, et al (l994) Congenital plexiform neurofibroma with a sarcomatous nodulein a three-month old child. Indian J Cancer 31:130-132
Kovanlikaya I, Gunbay MV, Pirnar T, et al (1990) Swollen neck inchildren: a report of two cases. Pediatr Radiol 20:485-486
Larsen ME, Larsen JW, Hamersley SL, et al (l999) Successfulmanagement of fetal cervical teratoma using the EXIT procedure. J Matern Fetal Med 8:295-297
Lau HT, Barlow BA, Gandhi RP (l984) Ectopic thymus: presenting as a neck mass. J Pediatr Surg 19:197
Lee F (l999) Occult congenital pyriform sinus fistula causingrecurrent left lower neck abscesses. Head Neck 21:671-676
Lee K (l980) Surgery of cyst and tumours of the neck. In: Paparella M, Shurich D (eds) Otolaryngology. Saunders, Philadelphia,p 2987
Leung AK (l986) Ectopic thyroid gland and thyroxine-bindingglobulin excess. Acta Paediatr Scand 75:872-874
Leung AK, Wong AL, Robson WLM (1995) Ectopic thyroid glandsimulating a thyroglossal duct cyst: a case report. Can J Surg38(l):87-89
Lewis MR (1962) Persistence of the thymus in the cervical area.J Pediatr 61 :887-893
Lim Dunham JE, Feinstein KA,Yousefzadeh DK, et al (l995) Sonographic demonstration of a normal thyroid in patients withthyroglossal duct cyst. AJR Am J RadioI164:1489-1491
![Page 24: [Medical Radiology] Pediatric ENT Radiology || Congenital Neck Masses (Non-vascular)](https://reader030.pdfslide.us/reader030/viewer/2022020408/5750933d1a28abbf6bae669d/html5/page/24.jpg)
198
Lyons TJ, Dickson JAS, Varienal S (1981) Cervical thymic cysts.J Pediatr Surg 24:241-243
MacCollum DW, Martin LW (1956) Hemangiomas in infancyand childhood. A report based on 6479 cases. Surg ClinNorth Am 36:1647-1663
Manaligod JM, Bauman NM, Menezes AH, et al (1999) Cervicalvertebral anomalies in patients with anomalies of the headand neck. Ann Otol Rhinol Laryngoll08:925-933
McAvoy JM, Zuckerbraun L (1976) Dermoid cysts of the headand neck in children. Arch OtolaryngoI102:529-531
Mcleod DM, Karandy EJ (1981) Aberrant cervical thymus: arare cause of acute respiratory distress. Arch Otolaryngol107:179-180
Mickel RA, Calceterra TC (1983) Management of recurrent thyroglossal duct cysts. Arch Otolaryngoll09:34-36
Middleton DS (1930) The pathology of congenital torticollis. BrJ Surg 18:188-204
Miller JH (1985) Lingual thyroid gland: sonographic appearance. Radiology 156:83-84
Moncada R, Vade A, Rosado W, et al (1996) Congenital andacquired lung hernias. J Thorac Imaging 11:75-82
Mulliken JB, Fishman S1, Burrows PE (2000) Vascular anomalies.Curr Probl Surg 37:517-584
Murayama S. Murakami J, Watanabe H, et al (1995) Signalintensity characteristics of mediastinal cyst masses on T1weighted MRI. J Comput Assist Tomogr 19:188-191
Murray J, Negrette J(1989) An unusual cause ofpulsatile neck swelling:report of a case of cervical aortic arch. Scott Med J 34:568-569
Neinas FW,Gorman CA,Devine KD (1973) Lingual thyroid.Clinical characteristics of 15 cases. Ann Intern Med 79:205-210
Noujaim S,Arpasi P, Bennett DF, et al (1997) Imaging thyroglossal duct anomalies. Radiologist 4:235-241
Noyek AM, Friedberg J (1981) Thyroglossal duct and ectopicthyroid tissue. Otolaryngol Clin North Am 14:187-207
Okstad S, Mair MB, Sundsfjord JA, et al (1986) Ectopic thyroidtissue in the head and neck. J OtolaryngoI15:152-155
Park BW, Park CS (1993) Pyriform sinus fistula. Yonsei Med J34:386-390
Philips H (1981) Intrauterine fetal hygromata: sonographicdetection. Am J Radiol 136:799-802
Potter EL (1976) Tumours. In: Potter EL, Craig JM (eds) Pathology of the fetus and the infant, 3rd edn. Year Book, Chicao,pp 177-206
Quick CA, Lowell SH (1977) Ranula and the sublingual salivarygland. Arch Otolaryngoll03:397-400
Radkowski D,Arnold J, Healy GB,et al (1991) Thyroglossal ductremnants. Pre-operative evaluation and management. ArchOtolaryngol Head Neck Surg 117:1378-1381
Rapado F, Bennett JD, Stringfellow JM (1998) Bronchogenic cyst:an unusual cause of a lump in the neck. J Laryngol Otol112:893-894
Reynolds JH, Wolinski AP (1993) Sonographic appearances ofbranchial cysts. Clin Radiol 2:109-110
Rowe MI (1995) Neck lesions. In: O'Neill JA, Grasfeld JL, Fonkalsrud EW, et al (eds) Essentials of pediatric surgery. MosbyYear Book, St Louis
Sadler TW (1990) Langman's medical embryology. Williamsand Wilkins, Baltimore, pp 312-313
Santiago W, Rybak LP, Bass RM (1985) Thyroglossal duct cystsof the tongue. J OtolaryngoI14:261-264
A.W.Duncan
Sistrunk WE (1928) Technique of removal of cysts and sinusesof the thyroglossal duct. Surg Gynecol Obstet 46: 109-112
Skandalakis JE, Todd NW (1993) The pharynx and its derivatives. In: Skandalakis JE, Gray SW (eds) Embryology for surgeons, 2nd edn. Williams and Wilkins, Baltimore, pp 17-64
Smith DW (1982) Recognizable patterns of human malformation: genetic, embryologic and clinical aspects, 3rd edn.Saunders, Philadelphia
Speer FD (1938) Thymic cysts: a report of a thymus presentingcysts of three types. N Y Med Coil Flower Hosp Bull 1:42-50
Spigland N, Bensoussan AL, Blanchard H, et al (1990) Aberrantcervical thymus in children: three case reports and reviewof the literature. J Pediatr Surg 25:1196-1199
Stringel G (1993) Haemangiomas and lymphangiomas. In:Ashcroft KW, Holder TM (eds) Pediatric surgery, 2nd edn.Saunders, Philadelphia
Tai CF, Lee KS, Chen IH (1997) Primary cervical neuroblastomain infants. J Formos Med Assoc 96:561-564
Tapper D (1993) Head and neck sinuses and masses. In: AshcraftKW, Holder TM (eds) Pediatric surgery, 2nd edn. Saunders,Philadelphia, pp 923-934
Teele RL, Share JC (1991) Ultrasonography of infants and children. Saunders, Philadelphia, pp 73-90
Telander RL, Filston HC (1992) Review of head and necklesions in infance and childhood. Surg Clin North Am72:1429-1447
Thora S, Chansoria M, Kaul KK (1985) Congenital tuberculosis:a case with unusual features. Indian J Pediatr 52:425-427
Todd NW (1993) Common congenital anomalies of the neck.Surg Clin North Am 73:599-610
Vazquez E, Enriquez G, Castellote A, et al (1995) US, CT andMR imaging of the neck lesions in children. Radiographics15:105-122
Wadsworth DT, Siegel MJ (1994) Thyroglossal duct cysts:variability of sonographic findings. AJR Am J Radiol163:1475-1477
Wagner CW, Vincur CD, Weintraub WH, et al (1988) Respiratory complications in cervical thymic cysts. J Pediatr Surg23:657-660
Weingast GR, Hopper KD, Gottesfeld SA et al. (1988) Congenital lymphangiectasia with fetal hygroma: a report of twocases with co-existent Down's syndrome. J Clin Ultrasound16:663-668
Weiss SD, Orlich CC (1991) Primary papillary carcinoma ofa thyroglossal duct cyst: a report of a case and literaturereview. Br J Surg 78:87-89
Welch KJ (1986) The oropharynx and jaws. In: Welch KJ, Randolph JG, Ravitch MM, et al (eds) Pediatric surgery, vol 1,4th edn. Year Book, Chicago, pp 513-515
Yeung VT, Loong EP, Cockram CS (1987) Cretinism and lingularthyroid in an adult. Postgrad Med J 63:881-883
Zaglul HF,Odita JC (1995) Multiple hernias: a defect in the celomic mesoderm? Am J Med Genet 57:537-539
Zadvinskis DP, Benson MT, Kerr HH, et al (1992) Congenitalmalformation of the cervico-thoracic lymphatic system:embryology and pathogenesis. Radiographics12:1175-1189
Zarbo RJ, Areen RG, McClatchey KD, et al (1983) Thyropharyngeal duct cyst: a form of cervical thymus. Ann Otol RhinolLaryngoI92:284-288