-
MEDICAL MICROBIOLOGY I
Lesson 9
Streptococcus and Diseases
-
Streptococcus
The genus Streptococcus is a diverse collection of Gram positive
cocci typically arranged in pairs or chains
Most species are facultative anaerobes, and Most species are
facultative anaerobes, and some grow only in an atmosphere enhanced
with carbon dioxide (capnophilic growth)
Their nutrient requirements are complex, necessitating the use
of blood- or serum-enriched media for isolation
-
Streptococcus
-
Streptococcus
Carbohydrates are fermented, resulting in the
production of lactic acid
Catalase negative
Most -haemolytic strains and some - Most -haemolytic strains and
some -
haemolytic and non-haemolytic strains
possess group-specific antigens, most of which
are cell wall carbohydrates
-
Streptococcus
These antigens can be readily detected by immunologic assays and
have been useful for the rapid identification of some streptococcal
pathogens
Most -haemolytic and non-haemolytic streptococci do not possess
the group-specific cell wall antigens
These organisms must be identified from their physiologic
properties
-
Streptococcus pyogenes
2 species of streptococci are classified in group A:
S. pyogenes (flesh-eating bacteria)
S. angionosus
S. pyogenes is the most common pathogen S. pyogenes is the most
common pathogen
S. pyogenes is an important cause of a variety of suppurative
and non-suppurative diseases
They are the most common cause of bacterial pharyngitis, these
organisms have become notorious because they can cause dramatic,
life-threatening diseases
-
Streptococcus pyogenes
-
Streptococcus pyogenes
1. Physiology and Structure
0.5 - 1.0 m, spherical cocci that form short chains in clinical
specimens and longer chains when grown in liquid media
Growth is optimal on enriched blood agar media but it is
inhibited if the medium contain high concentration of glucose
After 24 hrs incubation, 1 - 2 mm white
colonies with large zones of -haemolysis are observed
-
Streptococcus pyogenes
Encapsulated strains may appear mucoid on
freshly prepared media but wrinkled on dry
media
Non-encapsulated colonies are smaller and Non-encapsulated
colonies are smaller and
glossy
Cell wall: peptidoglycan (gram positive); within
the cell wall are group-specific and type-
specific antigens
-
Streptococcus pyogenes
2. Group-Specific Carbohydrates
The group specific carbohydrate, which
constituents approximately 10% of the dry
weight of the cell, is a dimer of N-weight of the cell, is a
dimer of N-
acetylglucosamine and rhamnose
This antigen is used to classify group A
streptococci and distinguish them from other
streptococcal groups
-
Streptococcus pyogenes
3. Type-Specific Proteins
The M protein is a major type-specific protein
associated with virulent streptococci
M proteins are subdivided into class I and class M proteins are
subdivided into class I and class
II molecules
The type I M proteins have the constant (C)
exposed, whereas antibodies do not develop
against the C region of class II M proteins
-
Streptococcus pyogenes
-
Streptococcus pyogenes
This appears to be important for patients who
develop rheumatic fever, because their disease
is mediated by strains with the class I M
proteinsproteins
A secondary type-specific protein that is useful
epidemiologic marker for bacterial strains that
fail to express the M protein is the t protein
(trypsin-resistant)
-
Streptococcus pyogenes
4. Other Surface Components
M-like proteins, lipoteichoic acid and F-protein
The M-like proteins are encoded by a complex
of more than 20 genes that comprises the of more than 20 genes
that comprises the
emm gene superfamily
These genes are responsible for M proteins, M-
like proteins, and other immunoglobulin-
binding proteins
-
Streptococcus pyogenes
Lipoteichoic acid and F protein facilitate binding
of host cells by complexing with fibronectin,
which is present on the host cell surface
Capsule-composed of hyaluronic acid Capsule-composed of
hyaluronic acid
containing repeating molecules of glucuronic
acid and N-acetylglucosamine; prevent
phagocytosis by providing physical barrier
between the opsonic complement proteins
bound to the bacterial surface and phagocytic
cells
-
Streptococcus pyogenes
5. Pathogenesis and Immunity
The virulence of group A streptococci is determined by the
ability of the bacteria to adhere to the surface of host cells,
invade into the epithelial cells, avoid opsonisation and the
epithelial cells, avoid opsonisation and phagocytosis, and produce
a variety of toxins and enzymes
More than 10 different bacterial antigens have been demonstrated
to mediate adherence to host cells, with lipoteichoic acid, M
proteins, and F protein the most important, as well as other
antigen
-
Streptococcus pyogenes
The internalisation is believed to be important for maintenance
of persistent infections (e.g.recurrent streptococcal pharyngitis)
as well as invasion into deep tissues
Streptococcus pyogenes has multiple Streptococcus pyogenes has
multiple mechanisms for avoiding opsonisation and phagocytosis
M-related proteins interfere with phagocytosis, peptidase block
chemotaxis of neutrophils and mononuclear phagocytes
-
Streptococcus pyogenes
6. Pyrogenic exotoxins
The streptococcal pyrogenic exotoxins (Spes), originally called
erythrogenic toxins are produced by lysogenic strains of
streptococci and are similar to the toxin produced in and are
similar to the toxin produced in Corynebacterium diphtheriae
3 immunologically distinct heat-labile toxins (SpeA, SpeB and
SpeC) have been described in S. pyogenes and in rare strains of
groups C and G of streptococci
-
Streptococcus pyogenes
The toxins act as superantigens, interacting
with both macrophages and helper T cells with
the release of interleukin-1 (IL-1), IL-2, and IL-
6, tumour necrosis factor- (TNF- ) and TNK-6, tumour necrosis
factor- (TNF- ) and TNK-
and interferon-
These cytokines mediate a variety of important
effects, including the shock and the organ
failure seen characteristically inpatients with
streptococcal toxic shock syndrome
-
Streptococcus pyogenes
7. Streptolysin S and O
Streptolysin S is an oxygen-stable, non-
immunogenic, cell-bound haemolysin that can
lyse erythrocytes, leukocytes and plateletslyse erythrocytes,
leukocytes and platelets
Streptolysin S is produced in the presence of
serum (serum dependence) and is responsible
for the characteristic -haemolysis seen on
blood agar media
-
Streptococcus pyogenes
Streptolysin O is oxygen-labile haemolysin
capable of lysing erythrocytes, leukocytes,
platelets, and cultured cells
Antibodies are readily formed against Antibodies are readily
formed against
streptolysin O, a feature differentiating it from
streptolysin S, and are useful for documenting
recent group A infection (ASO test)
Streptolysin O is irreversibly inhibited by
cholesterol in skin lipids
-
Streptococcus pyogenes
8. Streptokinases
2 forms: streptokinase A and B
These enzymes can lyse blood clots and may
be responsible for the rapid spread of be responsible for the
rapid spread of
Streptococcus pyogenes in infected tissues
Anti-streptokinase antibodies are also a useful
marker for infection
-
Streptococcus pyogenes
9. Deoxyribonucleases
4 immunologically distinct DNases: A to D
These enzymes are not cytolytic but can depolymerise free DNA
present in pus
This process reduces the viscosity of the This process reduces
the viscosity of the abscess material and facilitates spread of the
organisms
Antibodies developed against DNase B are an important marker of
cutaneous Streptococcus pyogenes infections
-
Streptococcus pyogenes
10.C5a Peptidase
Complement component C5a mediates
inflammation by recruiting and activating
phagocytic cellsphagocytic cells
C5a peptidase disrupts this process by
degrading C5a
-
Clinical Diseases
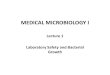
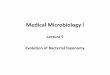
1. Pharyngitis
This develops 2 - 4 days after exposure to the pathogen, with an
abrupt onset of sore throat, fever, malaise, and headache
The posterior pharynx can appear The posterior pharynx can
appear erythematous with an exudate, and cervical lymphadenopathy
can be prominent
50% of patients with strep throat have pharyngeal or tonsilar
exudates
-
Pharyngitis Strep Throat
-
Clinical Diseases
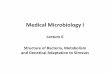
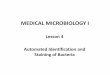
2. Scarlet Fever
A complication of streptococcal pharyngitis that occurs when the
infecting strain is lyosogenised by a temperate bacteriophage that
stimulate the production of a pyrogenic that stimulate the
production of a pyrogenic exotoxin
Within 1 to 2 days after the initial clinical symptoms of
pharyngitis develop, a diffuse erythematous rash initially appears
on the upper chest and then spreads to the extremities
-
Scarlet Fever
-
Clinical Diseases
The area around the mouth is generally
spared, as are the palms and sole
A yellowish white coating initially covers the
tongue and is later shed, revealing a red, raw tongue and is
later shed, revealing a red, raw
surface beneath (strawberry tongue)
The rash disappears over the next 5 - 7 days
and is followed by desquamation
-
Clinical Diseases
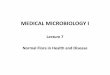
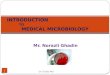
3. Pyoderma (Impetigo)
A confined, purulent (pyo) infection of the skin (derma) that
primarily affects exposed areas (e.g. face, arms, legs)
Through direct contact Through direct contact
Vesicles develop and then become pustules (pus-filled vesicles),
which then rupture and crust over
The regional lymph nodes can become enlarged, but systemic signs
of infection (e.g.fever, sepsis) are uncommon
-
Pyoderma
-
Clinical Diseases
Pyoderma is seen primarily in young children
(2 - 5 years old) with poor personal hygiene
and occurs primarily in warm, moist summer
monthsmonths
The strains of streptococci that cause skin
infections are different from those that cause
pharyngitis, although pyoderma serotypes can
colonise the pharynx and establish a persistent
carriage state
-
Clinical Diseases
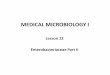
4. Erysipelas
An acute infection of the skin
Patients experience local pain and
inflammation (erythema, warmth), lymph inflammation (erythema,
warmth), lymph
node enlargement, and systemic signs (chill,
fever, leukocytosis)
The involved skin area is typically raise and
distinctly differentiated from the uninvolved
skin
-
Erysipelas
-
Clinical Diseases
5. Cellulitis
Typically involves the skin and deeper
subcutaneous tissue, and the distinction
between the infected and non-infected skin is between the
infected and non-infected skin is
not clear
Precise identification of the offending
organism is necessary because many different
microbes can cause cellulitis
-
Cellulitis
-
Clinical Diseases
6. Necrotising Fasciitis
An infection that occurs deep in the subcutaneous tissue,
spreads along the fascial planes and is characterised by an
extensive destruction of muscle and fatdestruction of muscle and
fat
The organism is introduced into the tissue through a break in
the skin
Initially there is evidence of cellulitis, after which bullae
form and gangrene, and other systemic symptoms develop
-
Necrotising Fasciitis
-
Clinical Diseases
Systemic toxicity, multi-organ failure and death
(>50%) are the hallmarks of this disease
Fasciitis must be treated aggressively with the
surgical debridement of non-viable tissuesurgical debridement of
non-viable tissue
-
Clinical Diseases
7. Streptococcal Toxic Shock Syndrome
Most patients initially experience soft tissue inflammation at
the site of the infection and pain as well as non-specific
symptoms, such as fever, chills, malaise, nausea, vomiting and
diarrhoeachills, malaise, nausea, vomiting and diarrhoea
The pain intensifies as the disease progresses to shock and
organ failure
Patients with streptococcal disease are bacteremic, and most
have necrotising fasciitis
Susceptible: HIV, diabetic, cancer, heart or pulmonary disease
and varicella-zoster viral infection patients
-
Clinical Diseases
8. Other Disease
I. Suppurative
Puerperal sepsis
Lymphangitis Lymphangitis
Pneumonia
II. Non-suppurative
Rheumatic fever
Acute glomerulonephritis
-
Lymphangitis
-
Laboratory Diagnosis
Microscopic: Gram stain
Antigen detection: immunologic test using
antibodies that react with the group-specific
carbohydrate in the bacterial cell wall, e.g. carbohydrate in
the bacterial cell wall, e.g.
enzyme immunoassay (EIA)
Culture: haemolysis on blood agar media
Identification: bacitracin
Antibody detection: ASO test, anti-DNase test
-
Bacitracin Test
-
Streptococcus agalactiae
Streptococcus agalactiae is the only species
that carries the group B antigen
This organism was initially recognised as a
cause of puerperal sepsis, later known as an cause of puerperal
sepsis, later known as an
important cause of septicaemia, pneumonia,
and meningitis in newborn children, as well as
a cause of serious disease in adults
-
Streptococcus agalactiae
-
Streptococcus agalactiae
1. Physiology and Structure
Gram positive cocci (0.6 - 1.2 m) that form
short chains in clinical specimen and longer
chains in culture
They grow well in nutritionally enriched media
and in contrast with a narrow zone of -
haemolysis
Some strains (1-2%) are non-haemolytic,
although their prevalence may be
underestimated because non-haemolytic strains
are not screened for the group B antigen
-
Streptococcus agalactiae
Strains of S. agalactiae can be subdivided on
the basis of the 3 serologic markers:
The B antigen or group-specific cell wall
polysaccharide antigen (composed of polysaccharide antigen
(composed of
rhamnose, N-acetylglucosamine, and galactose)
Type-specific capsular polysaccharides (Ia, Ib, II
to VIII)
The surface protein, C protein
-
Streptococcus agalactiae
2. Pathogenesis and Immunity
Antibodies developed against the type-specific
capsular antigens of group B streptococci are
protective, a factor that partly explains the protective, a
factor that partly explains the
predilection of this organism for neonates
Genital colonisation with group B streptococci
has been associated with increased risk of
premature delivery
Group B streptococci produce several enzymes,
including DNases, hyaluronidase, neuraminidase,
protease, hippurase, and haemolysins
-
Clinical Diseases
Early-Onset Neonatal Disease
Bacteremia, pneumonia, or meningitis
Late-Onset Neonatal Disease
Acquired from an exogenous source (e.g. mother, another
infant). Bacteremia with meningitis
Infections in Pregnant Women
Bacteremia; secondary complication: endocarditis,
meningitis, and osteomyelitis, are rare
Infections in Men and Non-Pregnant Women
Bacteremia, pneumonia, bone and joint infections, and skin
and soft tissue infections; mostly among
immunocompromised person
-
Streptococcus pneumoniae
1. Physiology and Structure
Encapsulated
Older cells decolorise readily and appear Gram
negativenegative
Colonies of encapsulated strains are generally
large (1 - 3 mm) on blood agar; smaller on
chocolatised or heated blood agar, round and
mucoid; colonies of non-encapsulated strains are
smaller and appear flat
-
Streptococcus pneumoniae
-
Streptococcus pneumoniae
-
Streptococcus pneumoniae
The choline is unique to the cell wall of
Streptococcus pneumoniae and plays an important
regulatory role in cell wall hydrolysis
Choline must be present for activity of the Choline must be
present for activity of the
pneumococcal autolysin, amidase, during cell
division
2 forms of teichoic acid: one exposed on the cell
surface and similar form covalently bound to the
plasma membrane lipids
-
Streptococcus pneumoniae
The lipid bound teichoic acid in the bacterial
cytoplasmic membrane is called F antigen because
it can cross-react with the Forssman surface
antigens on mammalian cells
-
Streptococcus pneumoniae
2. Pathogenesis and Immunity
Colonisation and migration
Surface protein adhesions and secretory IgA proteases
and pneumolysin (cytotoxin similar to streptolysin O)and
pneumolysin (cytotoxin similar to streptolysin O)
Tissue destruction
Pneumolysin, hydrogen peroxide and
phosphorylcholine in the bacterial cell wall
Phagocytic survival
Capsule
-
Streptococcus pneumoniae
3. Clinical Diseases
Pneumonia
Sinusitis and Otitis media
Meningitis Meningitis
Bacteremia
-
Otitis Media