Embed Size (px)
Citation preview

Medical Grade Telecom Networks by
Prabhat Kulshreshtha, B.Sc.
Report
Presented to the Faculty of Graduate Studies
of the University of Alberta
in Partial Fulfilment
of the Requirements
for the Degrees of
Master of Engineering
Master of Business Administration
The University of Alberta
August 2006

- i -
Medical Grade Telecom Networks by
Prabhat Kulshreshtha, B.Sc.
APPROVED BY
SUPERVISING COMMITTEE:
_________________________
_________________________

- ii -
Medical Grade Telecom Networks by
Prabhat Kulshreshtha, MEng, MBA
The University of Alberta, 2006
SUPERVISORS: John Doucette, Roy Suddaby
ABSTRACT
A number of very compelling factors are expediting the integration of technology
into the healthcare sector. This integration is of significant importance to any healthcare
stakeholder since such technology can: help reduce loss of life, facilitate global
collaboration, reduce annual operating expenditures, and of course greatly increase
productivity. This work presents a full economic and technical study concerning the state
of e-healthcare today (2006) with a focus on Canada and Alberta in particular with
specific case studies from around the world. In particular, the dominant healthcare
applications place unique constraints on the underlying telecom networks. Our industry
analysis not only reveals the technical requirements of state-of-the-art networks, but it
also reveals strategic opportunities. Most notably we present current trends in
availability design as well as the organizations that are responsible for e-healthcare
deployments. We also outline the growing issue around protocol standardization since
many current deployments are unable to communicate seamlessly with other sites. A
significant opportunity exists for a protocol translator to allow communication between
disparate systems. The data and material we present can also be of great value for e-
healthcare related market research.

- iii -
VITA Prabhat Kulshreshtha was born in Winnipeg, Manitoba on December 10, 1978, the son of
Nand and Chhaya Kulshreshtha. After graduating from Harry Ainlay High School,
Prabhat matriculated to the University of Alberta. There he completed the academic and
work experience requirements of the Bachelor of Science in Electrical Engineering
Cooperative Program. The majority of his work experience during this degree was at
Nortel Networks in various design roles. Upon graduation in 2001, Prabhat accepted
employment at a telecom start-up, Innovance Networks, as a network designer. Later in
2004, he returned to the University of Alberta to complete the MBA /MEng Program.
This report was typed by the author.

- iv -
Table of Contents 1. INTRODUCTION............................................................................................................................... 1
1.1. MEDICAL APPLICATIONS.............................................................................................................. 2 1.2. DOMINANT APPLICATIONS ........................................................................................................... 3
2. PICTURE ARCHIVING AND COMMUNICATION SYSTEM .................................................. 5 2.1. INTRODUCTION............................................................................................................................. 5 2.2. PACS COMPONENTS .................................................................................................................... 6
2.2.1. Modalities ............................................................................................................................... 7 2.2.2. Campus Network..................................................................................................................... 8 2.2.3. Storage Area Network ............................................................................................................ 9 2.2.4. Local Monitors ..................................................................................................................... 10 2.2.5. DICOM................................................................................................................................. 11 2.2.6. Application Layer ................................................................................................................. 11
3. ELECTRONIC HEALTH RECORDS ........................................................................................... 13 3.1. INTRODUCTION........................................................................................................................... 13 3.2. SCANDINAVIA ............................................................................................................................ 15
3.2.1. Kingdom of Denmark............................................................................................................ 15 3.2.2. Kingdom of Sweden .............................................................................................................. 18 3.2.3. The Baltic e-Health Project .................................................................................................. 20
3.3. INTERNATIONAL EHR DEPLOYMENT PROGRAMS ...................................................................... 22 3.4. ELECTRONIC HEALTH RECORD STANDARDS .............................................................................. 23
4. COMPETITIVE STRUCTURE ..................................................................................................... 24 4.1. PICTURE ARCHIVING AND COMMUNICATION SYSTEM VENDORS ............................................... 24 4.2. ELECTRONIC HEALTH RECORD VENDORS.................................................................................. 25
4.2.1. HIMSS EHRVA..................................................................................................................... 25 4.2.2. OpenEHR.............................................................................................................................. 26 4.2.3. IBM....................................................................................................................................... 26
4.3. OPTICAL NETWORK VENDORS ................................................................................................... 27 5. CANADA ........................................................................................................................................... 28
5.1. CANADA HEALTH INFOWAY....................................................................................................... 28 5.1.1. Background........................................................................................................................... 28
5.2. ALBERTA SUPERNET.................................................................................................................. 29 5.2.1. Background........................................................................................................................... 29 5.2.2. Implementation Strategy....................................................................................................... 31 5.2.3. SuperNet Users ..................................................................................................................... 32
5.3. NORTH NETWORK ...................................................................................................................... 33 5.4. MBTELEHEALTH........................................................................................................................ 34
6. CANADIAN IT SURVEY ................................................................................................................ 35 6.1. METHODOLOGY ......................................................................................................................... 35 6.2. IT BUDGETS ............................................................................................................................... 35 6.3. SATISFACTION LEVELS............................................................................................................... 36 6.4. BARRIERS TO IT IMPLEMENTATION............................................................................................ 37 6.5. STRATEGIC PRIORITY OF CLINICAL SYSTEMS ............................................................................ 38

- v -
7. HEALTHCARE IN ALBERTA ...................................................................................................... 39 7.1. PAPER RECORDS ......................................................................................................................... 40 7.2. ELECTRONIC HEALTH RECORDS ADOPTION............................................................................... 41 7.3. PHARMACIES.............................................................................................................................. 42 7.4. INTEROPERABILITY .................................................................................................................... 43 7.5. INFRASTRUCTURE ...................................................................................................................... 44
8. FUTURE TRENDS........................................................................................................................... 45 8.1. PACS......................................................................................................................................... 45 8.2. EHR........................................................................................................................................... 46 8.3. PRIVACY ISSUES......................................................................................................................... 47 8.4. IMPLICATIONS FOR PRACTITIONERS ........................................................................................... 48 8.5. INTEROPERABILITY .................................................................................................................... 49 8.6. NETWORK AVAILABILITY .......................................................................................................... 50 8.7. LEGACY DATA ........................................................................................................................... 52
9. CONCLUSION ................................................................................................................................. 53 10. REFERENCES............................................................................................................................. 54

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 1
1. Introduction
While health care professionals spend more than 80% of their time manipulating
information, they often do not perceive themselves as doing so [1]. This makes the
health profession ideally suited for technology integration to help manage information.
While technology provides many productivity gains, over time technological complexity
has also substantially increased. Most healthcare facilities now maintain a technology
group staffed with engineers who maintain and update their systems.
There are some unique macroscopic trends in healthcare visible today. Due in
part to increased global trade and travel, the spread of disease quickly crosses regional
divisions. Clearly, tracking the spread of disease and healthcare information sharing
between countries is becoming increasingly important. A single global effort is
logistically impossible so this effort must be decentralized into regions. Scandinavia has
demonstrated the greatest progress in this regard and they are often viewed as e-
healthcare pioneers. Scandinavian countries first built respective national IT
infrastructures and are now attempting to integrate themselves together. We will discuss
Scandinavia in great depth in section 3.2.
This report will outline the current trends in healthcare technology in detail along
two dimensions. The first dimension is regional. Regional technologies offer
productivity gains within a facility with some external benefits as well. The second
dimension is macroscopic inter-facility technologies. These technologies help to
integrate multiple regions together with the obvious ultimate goal of world-wide

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 2
integration. Key market stakeholders and conditions will be examined along with
specific case studies outlining recent deployments and trends.
This report will begin by providing a comprehensive analysis of current medical
applications to illustrate the nature of medical technology as it pertains to
telecommunications. Since the industry is marked by significant interest from both
public and private firms, we will then examine both the competitive environment as well
as publicly funded initiatives around the world with particular focus within Canada. We
will conclude with forward looking ideas and provide inspiration for future
developments.
1.1. Medical Applications Very simply, medical grade networks are those networks that support medical
telecom applications. Symbiotically, these applications specify network design and
performance criterion necessary to facilitate them.
The following is a comprehensive list of applications in common use today at
healthcare facilities:
1. Patient Care Systems (PCS): PCS is similar to a point of sales system often
used by retailers. Customer visits, interaction details and billing information are
all stored and generated here.
2. Pharmaceutical Systems: These systems are responsible for drug procurement,
distribution, and delivery.
3. Core Patient Information Systems: Some facilities have centralized databases
that contain patient information.
4. Laboratory Information Systems: These systems facilitate remote
appointments and lab result inquiries between administrators and labs.
5. Decision Support Systems (DSS): These consist largely of databases with a user
interface for the purpose of aiding practitioners in making decisions.
6. Radiology Information Systems (RIS): RIS helps radiology clinics manage
patient flow.
7. Picture Archiving and Communications Systems (PACS): PACS enables
digital archiving of medical images.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 3
8. Community Health Systems: CHS is typically a web-based solution for health
facilities to engage the public. Halifax has such a web-portal at www.hfch.org
9. Tele-health: Tele-health systems allow physicians to remotely diagnose and in
some case operate on patients.
10. Administrative Systems
11. Human Resource Systems
12. Education and Training Systems
1.2. Dominant Applications Over the next 10 years, our research suggests that network designers will find two
applications to be of most relevance due to their integrative nature. They will be
introduced here and subsequently analyzed in detail. The first application, which is very
rapidly emerging is Electronic Health Records (EHR). EHR involves digitizing paper
records and deploying networks to connect those who require access to this information.
The second application is the Picture Archiving and Communications Systems (PACS).
PACS involves storing and accessing digital images produced by medical equipment
directly rather than converting them to physical form and storing them in paper files.
Technically, the main benefit of both EHR and PACS comes from the digital
nature of the new format, allowing
electronic manipulation and
instantaneous diagnostics. In
addition to the significant cost
savings, these applications tend to
consolidate the slew of
applications in use today. Among
other benefits is the reduction in
complexity and administration.
The final application worth mentioning is tele-health. There are multiple
definitions of tele-health ranging from any healthcare application using
Picture Archiving and
Communication System
Electronic Health Records
Patient Care
Pharmaceutical
Core Patient Information
Community Health
Laboratory
RIS
Picture Archiving and
Communication System
Electronic Health Records
Patient Care
Pharmaceutical
Core Patient Information
Community Health
Laboratory
RIS

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 4
telecommunications to remote diagnosis and even remote surgery. The definition used in
this report refers to video conferencing applications for medical professionals. As an
example, in some cases, a physician must gain the approval of a specialist before
administering treatment. This is particularly a concern in rural locations where
specialists often do not reside. To bridge this distance, video conferencing has been
implemented in a number of regions. As a result, these specialists can visually assess the
situation and in many cases, approval can be granted immediately. However, medical
professionals are also turning towards web-cam technology since the technology has
substantially improved and it offers many other conveniences. Video conferencing, for
example, typically has a dedicated room where patients must be transported. However, it
is more convenient to hold the conference in which ever room the patient currently
resides. Furthermore, current collaboration tools allow electronic document sharing.
This gives the specialist access to the original document rather than trying to view it
through a television monitor. Obviously this reduces errors as well.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 5
2. Picture Archiving and Communication System
2.1. Introduction Many healthcare facilities still use physical film and transparencies for medical
imaging applications. However, digital imaging technology is quickly replacing old
paper-based methods. The Picture Archiving and Communication System (PACS) is an
integrated system used to manage medical images and related data. The visionary
concept for PACS was first presented at a conference of the Society for Optical
Engineering (SPIE) in 1982 [2]. Optical networks dominate deployments due to the high
bandwidth demands that this application places. After years of evolution, PACS
technology finally matured in the late 1990s and is now considered commercially robust.
In fact recent customer approval ratings are among the highest. Currently, PACS
suppliers and analysts alike estimate annual global growth of approximately 20% over the
next five years. [3]
Given the widespread integration of digital technologies in our society, benefits of
PACS-type systems are now largely axiomatic. However, in addition to instant file
access and electronic diagnosis, there are other benefits perhaps unique to healthcare
facilities. Some of these are listed below.
• Facilities are required to keep images for up to 20 years and in some cases, for life
[4]. The probability of misplacing, damaging, or theft of a physical image is quite
high with equally high legal ramifications. While no system is capable of
eliminating all risks, PACS can significantly curb them.
• Particularly in large facilities, a library must be maintained and staffed to
catalogue the records of thousands of patients. Storage and maintenance costs can
be dramatically reduced with the use of PACS.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 6
• PACS can virtually eliminate operating costs related to physical film and image
handling. For example, Concord Hospital, NH [5] a 300-bed facility spent only
$73,000 on film after the first year of implementation. Their annual costs had
typically been $504,000. The corresponding reduction in chemical consumption
is also better for the environment.
• Overall patient care efficiency reduces patient wait times and increases patient
flow.
Originally PACS was used in Radiology clinics because at the time such clinics
produced the highest volume of images. Later with the emergence of other imaging
equipment such as MRIs, uses of PACS were progressively broadened.
While the healthcare industry has taken leadership in the area of digital image
libraries, many other sectors can also benefit from this technology. For example, the
United States Navy maintains over 237 million drawings and over 15 million technical
manuals [6]. The corresponding annual maintenance cost is approximately $4 billion.
Clearly there are obvious crossover benefits.
2.2. PACS Components PACS can largely be described by its constituent elements.
1. Imaging Modalities
2. Campus Network
3. Storage Area Network (SAN)
4. Local Monitors
5. Digital Imaging and Communications in Medicine (DICOM)
6. Application Layer

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 7
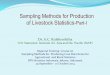
The following diagram outlines a typical PACS implementation.
CAMPUS NETWORK
MODALITIES
SAN NETWORK
MONITORS
Internet
REMOTE ACCESS
2.2.1. Modalities For health professionals, the term ‘modality’ is defined as a therapeutic method or
agent that involves the physical treatment of a disorder. Specifically, these agents
include MRI, X-Ray and CT scanners. The images produced from patient studies
originate from these instruments. Listed below are some common file sources and sizes
[7].
Modality Image Dimensions Images /study File size per study
Ultrasound 256 × 256 × 8 25 1.5-MB
MRI 512 × 512 × 8 50 13-MB
Computed
Tomography (CT)
1024 × 1024 × 8 50 50-MB
Mammographic Image 4096 × 5120 × 12 4 160MB
4D CT 2-GB

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 8
These image sizes are by no means static. Equipment manufacturers continuously
increase the resolution of the images produced. As an example, early CT scanners
produced 512 × 512 pixel images. Current improvements represent a 4 times increase in
file size. Furthermore, cost indifference and ease of use creates incentives for physicians
to increase the study size. Due to these factors, the total size per study is expected to
increase over time.
2.2.2. Campus Network Network bandwidth is of particular importance for PACS implementation. File
sizes produced by equipment are not uniform and data traffic cannot be easily estimated.
In health facilities, there may be load spikes of a few gigabytes. Hence networks should
not be designed based on average load nor can they be designed based on current peak
loads. Due to increasing file sizes, a facility must estimate future file sizes or ensure
scalability on demand.
Some academics have attempted to study traffic trends in PACS implementations
but statistical distribution predictions have so far been weak. As a result, network design
is currently based on worst-case scenarios. There is also anecdotal evidence that facilities
are guided by successful designs used elsewhere and simply copy the same setup. The
following table outlines some healthcare facilities and the core network speed they chose
to implement. It appears as though Gigabit Ethernet is the most common
implementation. At this speed, given 50% bandwidth utilization, a practitioner can
expect to wait about 13 seconds to download a 100MB file.
Facility Beds Core speed Availability Requirement
Vendor
Central DuPage 394 10-Gbps 99.999% Cisco
Clarian Health 1340 10-Gbps 99.999% Cisco
Austin Radiological Association 1.25-Gbps 99.999% LightPointe
Aurora Health Care 129 1-Gbps N/A Enterasys
Orlando Regional Healthcare 1,640 1-Gbps N/A Nortel

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 9
Facility Beds Core speed Availability Requirement
Vendor
Peninsulas Health Care Corp 305 1-Gbps 99.999% 3Com
Queens Medical Center 526 1-Gbps N/A N/A
San Antonio Community Hospital 330 1-Gbps N/A N/A
North Kansas City Hospital 351 622-Mbps N/A N/A
Scalability is another advantage of optical networks. In fact Nortel’s networks
can be upgraded in 1Mbps increments on-demand to a maximum of 10-Gbps [8]. Since
most current commercial transponders operate up to 10Gbps, this feature is a
consequence of the design. Obviously beyond this speed additional equipment must be
installed.
2.2.3. Storage Area Network Statistically, image data obtained within the last year is accessed 80% of the time.
The remaining 20% of data queries are for older files [9]. Legally, data must be retained
from 5 to 7 years, depending on local policies. For some infants, data may need to be
held until maturity. As a result, to reduce administrative complexity, some facilities
simply retain records for life.
Clearly much of the data resident on a system is hardly accessed. As a result, a
healthcare facility typically divides its data strategy into three categories: online, near-
online, and offline [10]. Online data is stored on magnetic hard drives and can be
accessed very quickly. A DVD jukebox with a robot arm controller is an example of
near-online access because this technique introduces access delay. Tape drives are an
example of an offline strategy because to access a single file requires the full tape to be
read.
For online data, Storage Area Network (SAN) architecture seems to be most
favoured due to high reliability and scalability. However, even SAN was not originally
designed to support the large file sizes in PACS. To increase reliability, data is typically
stored in 2 independent servers and possibly in a backup tape. A SAN would typically be
designed to hold data for one year.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 10
For older data, a DVD jukebox is often advocated, with some caveats. This
choice is driven entirely by cost. The cost per megabyte is lower for optical memory than
for magnetic memory. However, since the price of commercial magnetic memory falls
every year, a facility is encouraged to make purchases in yearly increments. Furthermore
many decision-makers are concerned with obsolescence of removable media. [11] They
feel that, much like floppies, one day computers may no longer be sold with DVD
readers, in favour of a new technology, and all their backup data will become
inaccessible. Information lifecycle management is therefore very important to
practitioners. In the event of disaster recovery, manually feeding tapes into the system
and saving the data to the proper database can potentially take months. In contrast, an
automated system can significantly reduce complexity and time.
2.2.4. Local Monitors Medical imaging devices produce images with greater than 256 shades of grey.
This level of contrast is required to make the required diagnosis. As a result a PACS
library must be equipped with the appropriate monitors. These monitors must have at
least 8-12 bits of grey information per pixel.
Such facilities have traditionally been equipped with black and white monitors;
however, a strong business case for purchasing colour monitors now exists. The latest
ultrasound equipment, for example, can produce images in colour. This adds an
additional requirement for the monitors.
The grey-scale requirement places restrictions on where images can be diagnosed.
In one respect this limitation is innocuous since most external networks are ill-equipped
to service the required bandwidth demands anyway. For example, a 100-MB file could
take over an hour to download using a DSL connection. However, for those physicians
that need to access these images, low resolution jpegs are often made available through a
web-server. Clearly these images should not be used to make detailed diagnostics but
they do provide decision makers with some information.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 11
2.2.5. Digital Imaging and Communications in Medicine (DICOM) DICOM is the underlying protocol that imaging modalities use for
communication. Different levels of the DICOM protocol include information
management services, image quality, reporting mechanisms, and security. [12]
The information management component regulates the basic image transfer and
storage process. For example, DICOM ensures that a local image cannot be deleted until
the file has both been copied to another location and the responsibility for that file has
been transferred to the new location. This reduces the likelihood of accidental erasure.
Image reproducibility between sites has also been a source of consternation. The
DICOM standard ensures that an image viewed on different monitors or printed on
different printers is produced identically. This includes specific monitor settings such as
contrast and brightness. Also, annotations that physicians make to the image are
preserved by the DICOM standard. Previously, there was no common platform with
which to do this.
DICOM also allows a user to attach a structured report. This report is digitally
linked to the image. File management and orphaned pictures are also of particular
concern and this feature helps to reduce both these problems.
Lastly DICOM has a built-in user logging mechanism so that images can not be
manipulated without the receiver noticing. DICOM also incorporates standard
encryption methods when transmission is across a public network.
A major concern with DICOM is that while it is a protocol with growing adoption
rates, many vendors are tweaking the standard with custom enhancements [13]. These
enhancements reduce interoperability between systems.
2.2.6. Application Layer The various components of PACS integrate together at the applications layer.
This places PACS application vendors at a unique advantage. Not only do these vendors
claim to understand the full integration process, but their brand is also the most visible
since users log into the system using their software.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 12
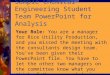
Bandwidth management is a key issue with PACS. Phillips, a PACS vendor, has
devised an innovative technique to avoid downloading the entire file at once. Using the
mathematical concept of wavelets, the image is essentially stored in parts. A portion of
the image is downloaded at the lowest resolution and as the user desires greater
resolution, higher components of the image are downloaded. This technique is
particularly beneficial when the underlying network is of lower speed. In fact, Phillips is
so confident in this method that it
guarantees 99.99% availability regardless of
the network bandwidth. Phillips claims that
theirs is the highest availability guarantee in
the industry [14].
Certainly the cost of any PACS
implementation depends on a number of
factors but a rough estimate can be made
based on the number of beds. A 300-bed
facility can face implementation costs between $5 million to $7 million plus annual
maintenance charges which are estimated at 8% of the implementation cost [15]. To
entice purchasers, many vendors have moved to a “pay-per-study” business model. A
customer would pay continuous fees to view, distribute and store images rather than pay
upfront capital costs. For those facilities without the budget to make large purchases, this
model allows easy cost amortization of such equipment over time.
Cost-per-view also alleviates another significant burden facilities face. Namely,
medical facilities rarely have the technical expertise to source and deploy a functional
system. As a result larger facilities have had to hire the requisite expertise. In contrast,
cost-per-view vendors typically agree to provide and service all the underlying
equipment. Medical facilities benefit from the resulting reduction in complexity.
Source: Phillips Global PACS

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 13
3. Electronic Health Records
3.1. Introduction Electronic Health Records (EHR) is an enabling technology that is redefining how
medical practitioners store and communicate patient information. Globally, medical
information is largely transacted using paper documents and the sector is eager to
capitalize on the benefits offered by electronic formats.
An EHR is an electronic version of patient health information stored in a
predetermined template. Each patient-practitioner encounter results in an EHR entry.
This information can include but is not limited to:
• Demographics
• Progress notes
• Medical history (personal and family)
• Laboratory data
• Radiology data
• Medication conflicts
The global push towards electronic records has largely come from the concrete
benefits that they offer. Specifically, the success of Danish and Swedish implementations
has motivated other governments to follow their lead. Indeed, the Scandinavians have
proved that electronic records not only improve the patient delivery process but that they
also reduce the total cost of delivery as well. The following advantages are among the
most quoted.
• The accuracy and completeness of the data reduces the likelihood of medical
errors. In 2000, the Institute of Medicine (U.S.) submitted a report to Congress
indicating that between 44,000 and 98,000 people die in Hospitals each year due
to medical errors. Among the strategies presented to cope with the situation was
to form a national reporting system [16].

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 14
• Once implemented the cost savings are enormous. A recent 2005 American
federal study by Project Hope has estimated a cost saving of US $77.8 billion per
year [17]. In Canada, the federally funded Infoway has estimated savings of CAD
$3.4 billion [18]. Denmark, a country of 5 million people currently saves €60
million each year [19]. In all cases, the cost savings are many orders of
magnitude greater than the cost of implementation.
• The electronic format lends itself to instant computerized diagnostics and
complex search criteria. The EHR system can also be used to track the
macroscopic progress of disease within a country. This is particularly useful
when tracking pandemics.
• Patients appear to be comfortable with their data being stored electronically.
Security concerns are not particularly high either. PriceWaterhouseCoopers
(2001) found that that 92% of Canadians are at least “somewhat willing” to carry
EHR smart cards [20]. Accenture (2005) found that U.S. citizens would even be
willing to pay $60/yr for this electronic service [21].
• EHR systems can automatically create progress notes per patient visit. This
reduces physician’s paperwork and expedites patient delivery.
Electronic records are often referred to as Electronic Health Records (EHR) as
well as Electronic Medical Records (EMR). This difference is not simply a matter of
semantics; there is specific meaning behind each. EMR are those records that medical
practitioners work on. A user has full read/write access to these records and they contain
notes specific to the physician. When the EMR is released by the practitioner, it turns
into an EHR. The EHR is then shared between facilities as a read-only document. The
EHR contains the final information and all work-in-progress notes are stripped away.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 15
3.2. Scandinavia Any discussion of Electronic Health Records would be incomplete without
mentioning Scandinavia. Namely Denmark and Sweden provide the strongest success
stories about how EHR can be implemented.
3.2.1. Kingdom of Denmark
Denmark is the smallest of the
Scandinavian countries with a population of 5
million inhabitants. Much like U.K., Denmark
is a constitutional Monarchy with both a Queen
and Prime Minister. Denmark typically
follows socialist leanings and is considered to
be a welfare state with one of the highest taxation systems in the world. As such,
Denmark has a public healthcare system and its 14 Counties are responsible for providing
universal, free, and equal access services. Despite being a decentralized system, the
Danish Counties have cooperated with one another for the national e-health program.
MedCom, the Danish e-health program was founded in 1994 [22]. Perhaps the
greatest accomplishment has been the successful cooperation between authorities,
organizations, and private firms with stakes in the Danish healthcare system. MedCom
has passed through five iterations starting with MedCom I to MedCom V.
MedCom I can be attributed to the efforts of the County of Funen, which
proposed a vision to develop a national system to electronically communicate messages
between healthcare stakeholders. The first system transferred electronic lab results from
hospitals to the office of a General Practitioner. Over the following two years, features
were increased. The objective of MedCom I was to develop and test a working
Electronic Data Interchange (EDI) system using the public internet with secure VPN
tunnels.
Source: en.wikipedia.org

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 16
MedCom II followed the success of the localized MedCom I implementation.
The program was expanded nationally and involved thousands of healthcare
professionals. The pure “EDI” standard was narrowed to cater to specific healthcare
needs and the EDIFACT standard was adopted as the communication protocol. Dentists,
home care, and other telemedicine pilot projects were introduced. By 1999 electronic
communication had been significantly adopted in primary care facilities.
MedCom III was responsible for consolidating all the systems and streamlining
the delivery process. The focus shifted from technology development to patient quality
assurance. The structure of the electronic reports were formed and agreed to by large
healthcare focus groups.
MedCom IV introduced an internet strategy. The Danish Health Portal was
introduced and provided a direct access point for citizens to the healthcare network. This
system allows patients to book appointments, conduct email consultations with GPs, and
renew prescriptions.
MedCom V is currently underway with a number of new enhancements to the
MedCom systems. These include a number of structural reforms that are meant to
include more regions and increase supply chain robustness.
As a result
today in Denmark, all
paper messages have
been converted to
electronic formats. To
illustrate, when a
General Physician (GP)
prescribes a laboratory
test, the appointment is
automatically booked
for the patient. This
obviously speeds up the
Source: Presentation by Henrik Jensen (europa.eu.int) - 2003 ehealth
conference.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 17
patient queuing process and once the results are obtained, they are instantly transmitted to
the GP. Simultaneously, the various agents are reimbursed by the public insurance
agency.
There have been a number of reasons for the success of MedCom [23]. Firstly,
the Counties have provided great support to the practitioners. A Data Consultant visits
all practices regularly to train staff on the system. This also provides two-way
communications for staff to offer new ideas. A user can call a national help desk to ask
for advice or instructions. For new GPs, the County helps to set up the infrastructure to
connect to the network. Secondly, MedCom set strong standards. The program obligated
the Counties to participate so there was little room for debate. Furthermore, technology
vendors participated throughout MedCom’s evolution so they could provide
implementation insights. Finally, cultural acceptance has helped to promote adoption.
Those GPs not connected to MedCom are considered to have archaic practices while
connected practices are viewed more favourably and tend to attract more patients.
The final analysis [24] proves that MedCom has resulted in substantial savings for
the Danes. Estimates indicate that the system has freed up 50 minutes per day in a
normal GP’s practice. Since
virtually all stakeholders now
communicate electronically, the
number of phone calls placed to
hospitals has been reduced by 66%.
Compared with the old paper based
method, each new electronic
message costs €2.3 less. In 2003,
the annual cost savings were €60
million per year. These are certainly
extraordinary results and have
inspired governments around the
world to follow the Danish example.
Source: Danish Center for Health Telematics
(MedCom IV: status, plans and projects).

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 18
3.2.2. Kingdom of Sweden
There are many similarities between
Sweden and Denmark. Sweden is also a
constitutional monarchy, symbolically ruled by
King Gustaf. He governs a population of about
9 million (almost twice that of Denmark)
spread over 450,000 sq. km (ten times bigger
than Denmark).
The nation is marked by generous social benefits for its citizens. The government
covers all medical costs such as childcare, healthcare and dental care through a publicly
funded system. Financing for these services has typically come from high taxation.
However, the Swedish tax system is currently facing reformatory pressure. Membership
with the E.U. has resulted in abuse of its programs and the country is also attempting to
attract business to improve its economic standing. As a result, the country has lowered
corporate tax rates and other taxes may fall as well.
Sweden is divided into 21 Counties. Much like in Denmark, Swedish Counties
have a high degree of regional autonomy. These Counties are largely self-governed by a
counsel of elected and appointed members. Healthcare services are among the main
responsibilities for the Counties.
A 2005 study conducted by Robert Huggins Associates, (a think tank in Wales)
found that Stockholm, Sweden is the leading location for IT Knowledge outside the US
[25]. High tech firms such as Song Networks, Saab Dynamics, and Optillion are among
many sources of national telecommunication expertise. This centre of competency is
particularly beneficial for a country implementing a national IT health network.
The Swedish Electronic Health initiatives can be traced to the efforts of the seven
Counties that led its development in 1998. The network is called Sjunet. ‘Sju’ is the
Swedish word for seven and was chosen to honour the founding Counties. The pilot
project was funded by the Counties and the federal ITHS R&D fund. In 2001 Carelink,
an independent body responsible for national healthcare ICT was established.
Source: en.wikipedia.org

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 19
The first iteration of Sjunet used the internet with VPN tunnels [26]. Connection
was provided by Telia, the Swedish telecommunications carrier. Five years since
inception, Sjunet purchased its own dedicated IP optical network from Song Networks.
This dedicated network provides greater availability
and has built-in redundancy. Each County accesses
Sjunet with a 10-100Mbps connection. The higher
bandwidth of Sjunet has enabled some interesting
applications. Firstly, videoconferencing has become
more ubiquitous fostering greater communication
among physicians. Secondly, Sjunet has also
incorporated a national population database and
various other e-Government services related to
healthcare monitoring and administration.
Sjunet connects over 80 hospitals, 800 primary
care centres, 900 pharmacies and a large number of
GPs. The solution is highly scalable and can easily be connected to new institutions.
Currently, the core bandwidth is 1 Gbps but this can presumably be upgraded as well.
This bandwidth seems to adequately service the current national needs.
Since the administrative and development costs are distributed among the
Counties, each County pays €12,000 per year for a 10Mbps connection [27]. The costs
are incrementally higher if the County desires greater bandwidth. In any case, this is an
insignificant sum when compared to other alternatives. In fact, Uppsala County
conducted an in depth cost-benefit analysis and found that Sjunet saves them €600,000
per year [28]. The savings are largely attributed to improved collaboration, lower staff
costs and reduced physical transportation of paper documentation.
Source: carelink.se

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 20
3.2.3. The Baltic e-Health Project
Denmark, Sweden and Norway have all established impressive national IT health
networks. The differences are rather minor. Given the success of these national
networks, in 2005 the European Union initiated a transnational project by allocating
European Regional Development Funds to this cause. The initial vision was to provide
rural locations with the same healthcare benefits as their urban counterparts. It was
hoped that such projects would not only foster multinational cooperation but also stave
rural migration [29].
The pilot project, the Baltic
Health Network (BHN), consists of five
hospitals in five separate countries [30]:
1. Funen Hospital (Denmark)
2. Västerbotten County Counsil
(Sweden)
3. St. Olav's Hospital (Norway)
4. East-Tallinn Central Hospital
(Estonia)
5. University Hospital (Lithuania)
Interestingly Denmark, and in
particular, the County of Funen has
again taken the lead role in
implementing BHN.
Initial clinical trials are in the areas of e-Radiology and e-Ultrasound. The intent
of these trials is to verify the reproducibility of the data once it has traversed the network.
To this end, an image is transmitted to two hospitals simultaneously and physicians
diagnose the images independently. Preliminary analysis reveals that the discrepancy in
diagnosis is less than 10% between hospitals. Hospitals in Denmark, Estonia and
Source: www.baltic-ehealth.org

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 21
Lithuania are responsible for e-Radiology while Norway and Sweden are focused on e-
Ultrasound.
Blurring of national boundaries in Europe has resulted in highly mobile
populations [31]. In many cases people work in one country and live in another. Ideally,
Swedish citizens would have access to their medical information in Denmark. A
significant technical challenge is that while all nations have implemented the EDIFACT
standard, each country has adapted the standard in slightly different ways [32]. Hence a
Danish GP can not simply send an EDIFACT prescription directly to a Swedish
pharmacy. Multinational implementation requires that either standardization be achieved
or protocol translators be installed at interface points. There are a number of other issues
that arise as well:
1. Legal jurisdiction and responsibilities.
2. Cultural differences.
3. Language barriers.
4. Billing jurisdictions.
The goal of the designers of the Baltic Health Network is to increase use and
expand its size and scope. Other facilities or regions are welcome to participate provided
that they prove that their own regional network is secure and that they have reason to join
the BHN. Clearly there is much technical as well as political work to be done before the
Baltic e-Health initiative is complete but these first steps are vital to demonstrate
feasibility.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 22
3.3. International EHR Deployment Programs Perhaps inspired by the success of Scandinavia, many governments have set up e-
Health Programs to implement electronic health records. In many cases, substantial
funds have been devoted to this cause with non-partisan steering committees.
From a macroscopic perspective, once a large number of countries implement and
interconnect their EHRs, a number of benefits emerge. Modern diseases such as SARS
and the more recent Bird Flu cross international boundaries freely. A global EHR system
could provide extensive statistics regarding the spread of illness that may yield
illuminating correlations. Additionally, such a network would facilitate greater informal
collaboration between countries in addition to formal publications. This could expedite
medical progress and promote best practices.
Country Program Target Deployment date Australia Integrated Health Record and
Information System - part of the HealthConnect programme
Canada National program for a pan-Canadian electronic health record - a major part of Canada Health Infoway
50% of the population by 2010
Denmark Implementation of electronic health records in hospitals, community health care and general practice
2003 -
England A major part of Connecting for Health (NHS, England)
2010 (for all patients in England)
Finland Implementation of national interoperable electronic patient records
2007
France Dossier médical personnel (DMP) - personal health record
By July 2007 (for all French citizens over the age of 16)
New Zealand Health Information Strategy for New Zealand, 2005 (HIS-NZ)
USA A major part of the Health Information Technology Plan
"Most Americans" by 2014. ("Participation by patients will be voluntary.")
Hong Kong Introduction of a patient-held medical record system in all General Out-patient Clinics (Hong Kong Hospital Authority initiative).
2007
Singapore EMR Exchange (EMRX) - Initiative by the Singapore Ministry of Health and the two public healthcare clusters to share information held on EMRs across all public hospitals and polyclinics.
From April 2004

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 23
3.4. Electronic Health Record Standards As noted earlier, standard harmonization is a critical issue. Not only are there a
number of organizations developing standards but regional implementations of the same
standards also differ.
Currently, HL7 (CDA) appears to be the most popular in North America and a
majority of the vendors produce HL7 compliant products.
Standards Description ISO 18308 Clinical and technical requirements for an Electronic Health
Record Reference Architecture "that supports using, sharing, and exchanging electronic health records across different health sectors, different countries, and different models of healthcare delivery". (2004)
ASTM Committee E31.19 Standards on Electronic Health Record Content and Structure
CEN 13606 The European electronic healthcare record interoperability standard (2004). Includes: EHR reference model, archetype interchange specification, reference archetypes and term lists, security functions, exchange models to support communication.
Health Level 7 (HL7) v3 Messaging standard to support communications "between hospital and physician record systems and between EMR systems and practice management systems" (2003).
Health Level 7 (HL7) Clinical Document Architecture (CDA)
An XML-based generic model for the representation and transfer of clinical documents. "CDA is being used also in electronic health records projects to provide a standard format for entry, retrieval and storage of health information." The CDA release 2.0 was approved as an ANSI standard in May 2005.
ASTM Continuity of Care Record (CCR)
A projected XML document standard for a summary of personal health information (data set) to help achieve interoperability between medical records and to ensure "a minimum standard of health information transportability when a patient is referred or transferred to, or is otherwise seen by, another provider."
e-MS (Electronic Medical Summary)
A projected standard for the Canadian province of British Columbia for an e-MS minimum dataset, messaging standards and technical architecture to support integrated health information management.
Health Level 7 (HL7) RIM Reference information model: "a single, all-encompassing model of the data structures that healthcare applications can exchange" (University of Manchester). "The RIM is an essential part of the HL7 Version 3 development methodology, as it provides an explicit representation of the semantic and lexical connections that exist between the information carried in the fields of HL7 messages" [HL7].
EDIFACT Developed by the United Nations, this is a generic standard to exchange standard messages. It allows multi-country and multi-industry adoption. Variants of this standard have been developed by both Sweden and Denmark for their national EHR standards.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 24
4. Competitive Structure
4.1. Picture Archiving and Communication System Vendors Healthcare Information and Management Systems Society (HIMSS), a reputable
business journal catering to the healthcare market, conducted a global survey in 2005 to
understand PACS market share breakdown [33]. The results show that GE Healthcare
Technologies commands the largest share of the market. However, the high degree of
market fragmentation suggests that each vendor has comparable value propositions and
that none has yet captured the market.
GE Healthcare Technologies, 20%
Phillips Global PACS, 12%
FUJIFILM Medical Systems, 12%
Siemens Medical Solutions, 11%
Others, 45% Other vendors with roughly 10% market share each include:
• AGFA-Gavaert
• Mortsel
• McKesson Corp

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 25
4.2. Electronic Health Record Vendors There are a number of EHR vendors also yet none has managed to capture any
significant share of the market. The following table lists a subset of the many vendors in
this sector.
A4 Health Systems AllMeds, Inc.
Companion Technologies Draeger Medical, Inc.
eMedical Files, Inc. Systems GE Medical Systems Information
Technologies
IBM Integrated Medical Records iMedica Corp.
JMJ Technologies, Inc. McKesson
MEDCOM Information Systems, Inc. NextGen Healthcare Information Systems
Siemens Medical Solutions Health Systems SolCom, Inc.
VantageMed Corp. VitalWorks
WebMd Intergy IDX Systems Corp.
A number of factors have promoted fragmentation of this market but the most
significant factor is the lack of interoperability. One of the basic EHR requirements is
that systems communicate seamlessly. Even slight implementation differences between
two systems using the same standard will impair communication. As noted earlier, the
Baltic Health Network is experiencing such problems even though member countries use
the EDIFACT standard.
4.2.1. HIMSS EHRVA Recognizing the importance of interoperation, 21 enterprising vendors decided
that collaboration is the key to success for all. To this end, they have created the HIMSS
Electronic Health Record Vendor Association (EHRVA) with the intent to promote a
certification process, interoperability, performance and quality measures, and to deal with
other EHR issues [34].

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 26
This attempt at collaboration presents some interesting strategic issues. Firstly,
by promoting a certification process, EHRVA is attempting to raise barriers for those
vendors unwilling or unable to join their collective. Secondly, EHRVA is chaired by
Charlene Underwood of Siemens Medical Solution. Regardless of their intent, it will be
interesting to see if competitive pressures challenge this alliance.
4.2.2. OpenEHR OpenEHR, an open source community of developers, has also attempted to solve
the integration issue [35]. OpenEHR is a fully functioning EHR system which also
addresses interoperation between both HL7 and EDIFACT standards. If successful, this
may help to bridge systems using either standard. With chapters across the globe,
OpenEHR has already been deployed in many facilities. Most notably, in 2002 the
Australian government selected OpenEHR as the basis for their national EHR
deployment project.
While open source may appear to be a great way to promote interoperability, open
source projects of this magnitude and scope have limitations. As a related example, if a
company chooses to migrate to the open source UNIX operating system, the code often
needs to be frozen so that the firm can provide internal support. This is particularly
important if a firm sells an operating system as part of an integrated product. Open
source software changes too frequently to provide the level of stability often needed.
Furthermore, open source software is rarely supported by the development community.
4.2.3. IBM In May 2005, IBM launched Federated Records Management System [36]. This
system allows companies to manage electronic health records generated by a variety of
vendors. Once the system reads a record, it converts it to human and machine readable
XML and then converts it back to the required format. Moreover an operator can manage
multiple systems from a unified access point. The system can also link to both structured
and unstructured data, such as related documents. IBM would also like to eventually
integrate this system with other IBM software such as Lotus Notes to provide even

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 27
greater flexibility. Even if IBM fails to gain majority market share, this product may be
the critical link required to harmonize multiple systems.
To test the effectiveness of their solution, IBM launched an internal EHR
initiative for its employees in 2005. Initially employees will input their own data
manually through a web portal. Later the system will begin to integrate insurance claim
systems to automatically update employee information.
4.3. Optical Network Vendors Despite the pioneering efforts of optical engineers in the field of e-healthcare,
optical networks are no longer application drivers. Today, optical networks are much
easier to deploy than their predecessors and they can support virtually unlimited
bandwidth. As a result networks are no longer bottlenecks and teams of specialists are
not needed for deployments. As a consequence they are increasingly viewed as
commodities. To curb commoditization, vendors have adopted some unique strategies.
Since there is natural synergy between the network infrastructure and the application
layer, some vendors have entered into informal alliances. Others have leveraged other
integrated product lines to provide a more comprehensive solution.
Major optical equipment vendors serving the healthcare market include:
• ADVA Optical
• Alcatel
• Cisco Systems
• Nortel Networks

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 28
5. Canada
5.1. Canada Health Infoway
5.1.1. Background Similar to other federal governments, Canada is committed to implement a
national Electronic Health Record (EHR) strategy. The Canadian government’s goal is to
have electronic health records available for over 50% of Canadians by the end of 2009.
The Canada Health Infoway is an independent organization tasked with managing $1.2
billion of public funds specifically for EHR projects [37].
Infoway Corporate Members are Deputy Ministers of Health appointed by each
province. The Board of Directors is comprised of members from various public and
private organizations.
Infoway has determined nine investment programs that will lead to the desired
national EHR network:
1. Registries: comprehensive identification of patients, healthcare practitioners, and
healthcare facilities
2. Diagnostic Imaging Systems: migration of digital images to a PACS system
3. Drug Information Systems: database to compare prescriptions with patient history
to avoid adverse interactions.
4. Laboratory Information Systems: electronic communication of lab results.
5. Telehealth: health care delivery regardless of distance.
6. Public Health Surveillance: national identification, management and control of
infectious disease.
7. Interoperable EHR: integration of medical information among disparate systems.
8. Innovation and Adoption: rapid deployment of EHR.
9. Infostructure: interoperability and standard harmonization.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 29
5.2. Alberta SuperNet
5.2.1. Background The Alberta SuperNet represents a public-private partnership between the
Government of Alberta and Bell Canada to create a provincial high-speed IP health
network [38]. There are a number of similarities between the Alberta SuperNet and the
various other national networks presented in this report. Namely, the network has the
primary objective of integrating rural and urban communities. Clearly
telecommunications equipment will not eliminate this divide but it is a good first step.
The SuperNet project had the following objectives:
• Reduce the “digital divide” by providing rural locations with the same quality of
resources enjoyed by their urban counterparts.
• Provide reasonably priced internet access to residents, regardless of their location,
with bandwidth comparable to xDSL or Cable.
• Provide rural schools with access to specialized teachers through video
conferencing equipment.
• Integrate communication needs of both rural and urban healthcare facilities
through a common network.
• Connect all provincial government offices together through a highly reliable and
secure dedicated network.
• Provide a common telecommunications platform for communication between all
public libraries.
The Alberta SuperNet is now operational in most of the targeted communities.
Shortly, SuperNet will connect all 4,200 facilities within 429 communities. These
facilities include libraries, schools, government offices and healthcare centres.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 30
The Alberta SuperNet
is particularly distinctive
from other such health
networks in one regard:
SuperNet has been opened to
private competition. In other
words, any business can
connect to SuperNet for a fee
and resell the bandwidth
commercially. As an
example, an ISP such as TELUS could connect SuperNet to its own equipment and sell
commercial internet connections to any residential or business customer that is linked to
SuperNet. A SuperNet subcontractor, Axia and the Network for Emerging Wireless
Technologies (NEWT) have created the Alberta SuperNet Certification and Showcase
Lab. The Lab provides smaller ISPs, without technical sophistication, the guidance they
need to connect their equipment to SuperNet’s.
Furthermore, public institutions do not automatically gain high speed connections
for free. They must pay a capped government rate to connect to Alberta SuperNet.
Presumably this is to reduce free-riding and to promote financial stewardship. However,
in the case of libraries, which provide public-good services, this focus on financials may
arguably be diametrically opposed to the initial project objectives.
The Government of Alberta hopes that the resulting competition will help to
provide competitive access to remote users as well as provide enough revenue to cover
the cost of network operation and maintenance.
Obviously the Alberta SuperNet differs in political ideology from the
Scandinavian networks. The Scandinavians follow socialist leanings while Alberta has
more capitalist tendencies. Interestingly, both have arrived at the similar conclusion
regarding the need for rural /urban telecom integration. Differences in implementation
could provide insights regarding which combination of approaches will yield the most
optimal results.
PoP
Health Facility
Library School
GovernmentHomes Businesses
PoP
Health Facility
Library School
GovernmentHomes BusinessesHomes Businesses
Source: www. albertasupernet.ca

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 31
5.2.2. Implementation Strategy SuperNet is touted as one of the most sophisticated communications networks in
North America. The 12,000 kilometre network consists of both fibre optic and
microwave links. Clearly the fibre optic links provide the greatest reliability and
bandwidth but some regions are characterized by adverse landscapes that make fibre
installation problematic. These landscapes are traversed by microwave systems. Such
microwave links represent only 16% of the network infrastructure.
A number of private companies were responsible for bring SuperNet to life. The
Government of Alberta designated Bell Canada as the prime contractor. In turn Bell
Canada partnered with 27 subcontractors with various specializations. The network itself
was design by Axia NetMedia and implemented by Bell Canada. Due to its role, Axia
holds a prominent position as well.
Products from various manufacturers resulted in the functioning physical layer.
The fibre optic cables with standard single mode fibres were purchased from Alcatel.
Their EZ-Prep cables were chosen due to their high reliability. In some locations, Bell
Canada simply purchased fibre previously installed by 360Networks. Cisco’s ONS
15454 SONET Multiservice Platform lights up
these fibres using Gigabit Ethernet. Hence the total
core bandwidth is 1Gbps. Also, Cisco’s MPLS
routers were used for the routing layer. Nortel’s
WIMAX transponders were deployed for the
wireless connections.
The Government of Alberta allocated $193
million for SuperNet’s construction. The
remaining $120 million was invested by Bell
Canada.
As an investor, Bell Canada enjoys various
privileges and has specific responsibilities.
SuperNet has both a Base Area Network (shown as
bold in the figure) and an Extended Area Network.
Bell Canada owns the Base Area Network which Source: www. albertasupernet.ca

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 32
connects 27 of the larger cities and communities. The Alberta Government owns the
remaining extended network. As contractors, Bell Canada and Axia NetMedia are
responsible for the operation and maintenance of the entire network.
As part of the agreement, Bell Canada is designated as the Provider of Last Resort
(POLR). Under the terms of the agreement, if no other ISP provides high-speed service
by April 2006, Bell Canada must provide access comparable to xDSL to any resident
upon request. The offered rate must also be equivalent to urban rates. Due to this
disincentive, Bell Canada announced that all residential rural communities will be
connected by April 2006. All public institutions will be connected by June 2006 and the
network will be fully operational by September 2006.
5.2.3. SuperNet Users As a result of open competition, a number of large network providers have
already connected to SuperNet. TELUS, for example, currently provides various services
to rural customers including VoIP. Smaller ISPs including Xplornet are also attempting
to provide internet to these underserved areas. CA*NET has estimated that a rural
business currently spending $2,000/month on a T1 line would pay about $820/month as a
result of SuperNet [39].
Alberta Health and Wellness recently announced that it is migrating to digital
images. It intends to become completely filmless by 2008 and has set aside $177 million
for this task. Alberta Health and Wellness plans to use SuperNet for its telecom
infrastructure. Transmitted images will include x-ray and MRI images. Mammography
scans present greater technological challenges so they will not be immediately digitized.
In Alberta, Electronic Health Records are communicated over the public internet
(like in Denmark). Therefore, while the Alberta SuperNet is not used as a dedicated EHR
network, SuperNet does facilitate internet connections for rural communities.
The expediency with which organizations such as Alberta Health and Wellness
proceeded to utilize SuperNet suggests that many other Health facilities will follow.
Applications may include image transfer, administration or simply internet connection.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 33
5.3. North Network Ontario launched a provincial network to connect underserved and rural
communities in Ontario in 1998 called North Network [40]. Prior to installation, Ontario
spent $20 million a year on air ambulance services alone. The initial network was
dedicated to video conferencing applications. This allowed remote physicians to consult
specialists unavailable in their locale before administering treatment.
The first iteration of North Network connected 4 communities but today 111
communities are interconnected by this network. Similar to Scandinavia, this network is
publicly funded. The Ontario Ministry of Health and Long Term Care provides the
largest contribution towards annual expenditures. Extra funds required for upgrades and
improvements come from a variety of federal and provincial sources. Unlike Alberta,
this is a closed network exclusively for healthcare use.
Since its introduction, the network has been upgraded to IP from ISDN. The
infrastructure was provided by Cisco using a MPLS routing layer. This 2002 upgrade has
allowed delivery of other services
including Electronic Health Records
(EHR) and digital radiology image
transfer. Agfa’s IMPAX system has
been installed for the PACS
application layer. End sites now
experience data rates from 400kbps
to 1Mbps. Compared with Alberta’s
more recent network, North Network
is rather slow. However, the
benefits of the technology are so
great that users happily accept the
longer download times.
Source: www.northnetwork.com

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 34
5.4. MBTelehealth Launched in 2001 by the Winnipeg Regional Health Authority, MBTelehealth is
an IP network connecting 26 rural and urban sites [41]. Winnipeg is the province’s
medical hub and prior to MBTelehealth, patients requiring significant medical treatment
had to travel to Winnipeg, where 95% of clinical specialists reside. Reducing this travel
time was the prime motivator for the project. Connected facilities include hospitals and
other larger health centres. MBTelehealth has focused on the areas of clinical diagnosis
and education via videoconferencing. The province would like to become a leader in e-
healthcare training.
While the project is deemed successful by any measure, Manitoba’s diminutive
economic climate presented a number of challenges. For example, loss of key medical
professionals delayed or terminated projects. Also, since IBM is among the few high
tech companies in the region, internal IBM restructuring led to substantial delays as an
alternative could not be found.
MBTelehealth is also publicly funded with contributions from Canada Health
Infostructure Partnership Program (CHIPP)
as well as Manitoba Health. Major project
vendors included Manitoba Telecom
Services AMD, Adcom, and Cisco
Systems.
Over time, there has been much
collaboration and sharing between
MBTelehealth and North Network.
CA*Net has acted as the bridge between
the two networks. Clinical and educational
services were shared with 11 northwestern
sites in Ontario. With integration in mind,
Canadian Health Infoway initiated the
telehealth starter toolkit. The toolkit will further promote knowledge sharing between
these two networks.
Source: www.mbtelehealth.ca

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 35
6. Canadian IT Survey
6.1. Methodology First, we shall review the results of an IT survey conducted by Canadian
Healthcare Technology in 2002 [42]. The survey is relatively recent and includes 104
stratified random hospitals across Canada. Respondent were CIOs and senior IT
healthcare professionals. Clearly we do not have access to such individuals so we must
rely on the results of this previous report.
6.2. IT Budgets On average, hospitals have an operating budget of $92.5 million dollars and
approximately 2% of this budget is allocated to IT expenditure. The following table
breaks down the budgets for different IT activities.
Mean Annual Expenditure per facility
Allocation Total Per bed
Hardware Acq. 28% 486,920 1,689.23
Software Acq. 21% 365,190 1,266.92
Support 42% 730,380 2,533.84
Misc. 9% 156,510 542.97
Total IT Budget 100% $1,739,000 $6,032.96
There appears to be clear indications that IT budgets are under funded by over 2%
of the annual budget and budgets need to double to significantly gain from the
productivity IT offers. For example, 36%-37% of respondents did not have a disaster
recovery program in place. Furthermore, security and confidentiality programs appeared
to lack funding as well. In an attempt to curb these potential threats, IT budgets were
targeted to increase by 20% for 2003.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 36
It is important to mention that simply increasing budgets is only part of the
solution. Arguably, the most important factor is the formulation of a well-planned
strategy backed by dynamic individuals to implement it. However, these other factors are
much more subjective and such reports assume that the facility will use the funds in an
appropriate manner.
6.3. Satisfaction Levels Satisfaction with Vendor Support
Software application / No. of users Satisfied (%) Neutral (%) Dissatisfied (%)
Core Patient Information / 88 68 16 16
Financial / 96 68 19 14
RIS / 53 64 30 6
Pharmaceutical systems / 78 63 22 15
Patient Care Systems (EMR) / 52 62 19 19
Laboratory Systems / 64 58 23 19
PACS * / 19 47 32 21
Decision Support Systems / 36 53 33 14
Community Health Systems / 29 48 38 14
HR Systems / 61 44 31 25
Educational training / 36 28 56 17
* Caution: Small base
Vendor satisfactions in Eastern Canada seem to be somewhat higher than
satisfaction levels in the west. Generally the size of hospitals is larger in the East with
correspondingly larger budgets. Clearly these budgets would invite greater vendor
attention.
Generally, it appears as though vendor satisfaction levels have room for
improvement. The surprising result is that of PACS. Our discussion with healthcare
professionals and our research indicates that PACS has been well received by the medical
community. New PACS initiatives appear to be quite frequent. Either, as the survey

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 37
indicates, there were not enough samples to make a confident conclusion or earlier PACS
vendors did not have the resources to provide adequate support.
The survey found that the first seven software applications are considered by IT
decision makers as adding tremendous value to the operation of the hospital. These
applications have also been quickly accepted by users.
6.4. Barriers to IT Implementation Barrier to IT implementation / No. of respondents
Barrier (%)
Neutral (%)
No Barrier (%)
Mean (Rank)
Lack of operating funds / 104
79 10 11 1.9 (1)
Lack of capital funds / 104
77 12 12 1.9 (1)
Shortage of IT personnel / 104
59 23 18 2.4 (2)
Shortage of Clinical personnel /103
49 28 23 2.7 (3)
Lack of capacity to change / 104
39 31 30 2.9 (4)
Shortage of administrative staff / 104
39 25 37 3.1 (5)
Technical inability to provide quantitative benefits / 104
35 29 37 3.0 (6)
Lack of understanding of IT by top management / 104
31 23 46 3.2 (6)
Lack of organizational vision or strategic direction / 104
23 37 40 3.2 (6)
Legislation (i.e. security & privacy laws) / 104
22 30 48 3.4 (7)
These results reflect senior IT executive’s perception that they are under funded.
Clearly there must be an element of self-reporting bias in these results. However, one
result that we found in our own research is that facilities often lack the personnel to
implement IT strategy. This has prompted vendors to provide services that require little
maintenance.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 38
6.5. Strategic Priority of Clinical Systems Clinical System / No. of respondents Priority
(%)
Neutral
(%)
No Priority
(%)
Mean
(Rank)
Hospital-wide electronic patient
records / 104
69 19 12 3.9 (1)
Region-wide electronic patient
records / 104
58 12 25 3.5 (2)
Electronic access to outside
physicians / 103
52 21 27 3.5 (2)
Image management, PACS / 104 49 14 37 3.2 (3)
Implementing decision support
systems / 104
42 30 28 3.2 (3)
It appears as though EHR is of high priority for most hospital facilities. Since
healthcare in Canada is publicly owned and the government is planning for a national
EHR initiative, this result is not surprising. In fact, since 2002 we would expect these
numbers to increase further. An interesting consequence of this priority is that PACS
implementation has been pushed to number three.
The item “electronic access to outside physicians” is somewhat vague. Does this
mean rural access through video conferencing or does it mean remote access for a
physician working from home or other remote sites? The exact definition may be quite
important. We have dealt extensively with rural access in our report however we have
not explored remote network access through DSL or cable in the same level of detail.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 39
7. Healthcare in Alberta
To understand the current state of e-healthcare in Alberta, we contacted a number
of patient point-of-contacts in the major cities of Edmonton and Calgary. The offices we
contacted included those of General Practitioners, laboratories and walk-in clinics. These
included both single-site and multi-site operations. Most such clinics are managed and
run by Administrative Assistants who are also responsible for the electronic systems.
Since gaining the attention of these gatekeepers is easier than obtaining an interview with
the doctor, we relied on their input. Naturally we found a lack of technology
sophistication and knowledge so the results we obtained are general and come from a
user perspective.
We have interviewed roughly 25 offices and assured them that specific
information would remain confidential. In the following sections we will report on the
general nature and direction of IT adoption in Alberta.
Office Type Edmonton Sample Calgary Sample
General Practitioner 12 2
Walk-in Clinics 3 1
Laboratories 2 1
Pharmacies 2 0
It is important to stress that the data presented is not meant to provide statistical
significance. The intent was simply to obtain a general understanding of the e-healthcare
climate in Alberta. Certainly we expect technology adoption and general trends in the
offices we interviewed to be similar to other offices in the province; however our data
cannot make this guarantee.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 40
7.1. Paper records Office Type Number in Sample
Paper based systems 15
Electronic Health Records (partially) 6
Electronic Health Records (exclusively) 0 * Not including pharmacies
There are surprisingly many offices that are still using paper records exclusively.
More than half of our interviewees interact with their patients in this traditional way.
These offices also suggested that there is no foreseeable plan to convert to electronic
form either. Certainly for smaller sites, the cost-benefit analysis is not skewed in favour
of electronic records.
Other offices have chosen to implement electronic health records but use them
exclusively for new patient interactions. Older files are simply maintained in the
traditional way. This is not surprising since migration to a fully electronic form is a
difficult process.
No office in our sample exclusively relied on electronic methods.
Again, we stress that patterns in our data may not be statistically significant;
however, we did find some interesting results. There appears to be a clustering effect in
terms of adoption. For example in South Edmonton, many of the clinics have adopted
EHR to some degree while in other locations, customer interactions still appear to be
transacted using paper methods. This clustering effect is consistent with adoption models
including recent theories by Michal Porter [43]. Essentially, once one clinic adopts a
technology, clinics nearby benefit from observable case studies and can also benefit from
the implementation expertise of that clinic. However, it appears as though clinics still
prefer not to share electronic health records with one another.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 41
7.2. Electronic Health Records Adoption Electronic health records have typically been well received by those who have
implemented the technology. Users have expressed that the new records both save time
and are easy to manage.
However, we must note that at least one correspondent mistook software that
helps to make patient appointments as electronic health records. Only by asking what
types of data these records contained did we uncover this confusion.
One particular chain of centrally managed clinics is particularly interesting. They
have chosen not only to adopt electronic health records, but they also exchange these
records between regional sites. The system identifies patients by their Alberta health card
number and hence each patient has a unique entry. Presumably the cost-benefit-analysis
was in favour of this electronic medium and saved document transportation costs (fax or
snail mail) between sites as patients moved. Intuitively one would expect the e-
healthcare business case for a large organization to be stronger than a single-site
operation.
Multi stakeholder integration of Danish calibre is still years away. In fact, even
some laboratories are not yet connected to other medical clinics. As a result test results
are still often faxed to the proper physician. Laboratory staff has expressed eagerness to
adopt an electronic method due to the anticipated efficiency. However, the staff was
unsure which clinics they would be connected to but they suggested that such
installations are about one year away. Unwilling to wait for the deployment of such
systems, another laboratory had chosen to simply post results on the internet. This is a
rather innovative solution that bypasses EHR but there is much manual data entry
required by both sender and receiver.
Pharmacists also operate fairly independently. Once a patient is prescribed
medicine, he/she can take the paper prescription to a local pharmacy (e.g. Shoppers Drug
Mart). The electronic networks of Scandinavia appear to be many years away.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 42
7.3. Pharmacies We spoke with representatives from two of Western Canada’s largest retail
pharmaceutical chains. Both seem to view EHRs adoption differently.
The first chain has adopted a proprietary database within which it creates and
maintains medical information from customer interactions. Using this database a
Pharmacist can identify and mitigate potentially adverse drug interactions. However, the
individual database systems in these chains do not communicate with other outlets so a
savvy consumer should return to the same location every time. Of course over-the-
counter prescriptions or any other prescriptions that do not flow through the pharmacy
are not captured in their database so there is a very finite probability that adverse drug
interactions could still occur. Their rationale is that some information is better than no
information.
The Pharmacist we spoke with was well acquainted with the EHR effort and
validated the vision that eventually all medical stakeholders would be connected through
a common EHR portal. In the case of Alberta, the portal is called Alberta Netcare [44].
Progress, according to the Pharmacist, is slowly taking place and while many
practitioners have embraced the technology, many more have not. To exemplify the
speed of adoption, he claims that at a 1994 Pharmacist conference it was suggested that
by 1995 text based connectivity would arrive. Clearly this did not happen. Since then
the vision has grown and become more elaborate but as our own research indicates,
progress has been very slow. According to the Pharmacist, included in the vision is the
requirement that all Pharmacists will communicate using the CPha standard. This is
certainly different that the HL7 EHR standard and obviously will create even more
complexity during integration. In any case, this Pharmacy will continue to operate as
before until greater EHR progress has been made.
The second chain does not have a proprietary database. Instead it is fully
connected with Alberta Netcare and can read any current EHR. The Pharmacist
presented the same rationale: since these records contain full patient information, they are
able to make better diagnoses and reduce adverse drug interaction. Since most EHRs are
currently issued by hospitals, these records are also incomplete representations of a
patient’s medical history. The Pharmacist recognized this deficiency but pointed out that

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 43
not every stakeholder will be connected immediately. During the early stages of any
such project, this is an intuitive consequence.
7.4. Interoperability The differences in the software interfaces of the EHR implementation by the GPs
we visited suggest that there are multiple variants of EHR software currently being used.
This is yet another example of integration impediments. In fact deployments appear to be
quite isolated. For example, in private GP’s offices, the EHRs are only for internal use.
In the case of a chain of walk-in clinics, the central planner had chosen to deploy a
system that would allow all offices to share EHRs. But again, this deployment is isolated
to the clinics that share common management.
When compared to the tight standardization in Scandinavia, the organic growth in
Alberta seems to be macroscopically disorganized. It seems that individuals have made
unique choices without considering larger interoperability benefits. If systems continue
to develop disparately then integration may never be possible. Therefore, as we have
mentioned earlier, there is certainly a very strong opportunity for an application that can
enable seamless communication. Without integration, many of the macroscopic benefits
we outlined earlier, such as tracking the spread of disease, can not be realized.
Arguably these are public good applications and hence fall under the domain of
the government. While the Canadian government may not be able to set strict standards
like the Danish government did, perhaps the Canadian government can provide macro-
level leadership. A strong business case does exist for the Canadian government to
undertake this integration activity. Currently the Canadian Health Infoway is allocating
funds to promote regional electronic health record deployments but these funds are
simply helping to intensify this interoperability divide. Perhaps the next step is for the
Infoway to take an active role in designing an interoperability solution. If the Infoway
prefers a passive role, outsourcing this task to a private contractor would also yield the
desired results.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 44
A private solution may also be viable. Much of our research has uncovered that
the primary deterrent for adoption is installation complexity and short-term inefficiencies.
If an Internet Service Provider could present a standardized package that includes the
appropriate software, internet connection and a consultant to set up the solution, they
could potentially capture a sizable market. Moreover, by centralizing this process, such a
company could ensure interoperability between sites. This solution would also inherently
be “EHR exchange ready.” Once a common infrastructure is deployed, it would be
incrementally simple to introduce the ability for EHR exchange. Such a project may also
meet the requirements of Infoway funding as explained earlier.
7.5. Infrastructure Sites can be grouped into roughly three categories regarding network
infrastructure.
1. No telecommunications equipment.
2. Basic internet services. Some laboratories make patient data available through
on-line portals. GPs with internet access can view results immediately.
3. Private networks. Multiple related sites (chain of clinics) have some sort of
private VPN that allows communication between sites but restricts internet
access.
Naturally, the Administrators were unaware how or who provided this
infrastructure. Furthermore, we did not uncover the use of video conferencing in the
offices we contacted.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 45
8. Future Trends
8.1. PACS Networks for the pioneering healthcare applications were much slower than those
deployed today. The 1-Gbps capacity in use today seems to be adequately suited for
most applications; however, there does not yet appear to be significant surplus
bandwidth. In the coming years the available bandwidth will likely increase and the
resulting surplus will correspondingly increase. Based on the internet usage trends,
economical deployment of 1-Tbps systems may not be unreasonable within 10 years.
Once a significant surplus of bandwidth is available, application dynamics will change.
Firstly, there will likely be a shift to more user-friendly applications and
bandwidth rationing will be eliminated. The lifecycle of other technology products have
also followed this same general trend. For example, as computer processing power
increased, applications became more user-friendly at the expense of processing
efficiency. Similarly, websites now consume greater bandwidth due to complex
graphical interfaces and online databases. All these examples suggest that technology
maturity results in increased levels of user-friendliness at the expense of efficiency.
Following this trend, future PACS images will be available on-demand with the ability to
view relevant images within studies based on different criteria. A practitioner will also
be able to retrieve multiple relevant patient studies to compare symptoms before making
diagnoses. The process will be rapid with many configuration options. In other words,
the future PACS user will have much greater control over how and which images are
accessed.
Secondly, the future intra-facility user will be able to access all healthcare data
from anywhere rather than from specific terminals. Momentum Healthware [45], based
out of Winnipeg, Manitoba has come close to this vision. Their tablet interface allows
users to access electronic health records from anywhere within a facility with a wireless

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 46
network. However, there is still
much needed work. Ideally,
battery-life will be improved to
over 24-hours so a physician can
operate it for a full day.
Obviously, the monitor would
meet the grey-scale requirements
needed for imaging applications.
Reducing weight, thickness, and
heat emissions will always be beneficial so that carrying the unit does not become
cumbersome. Moreover, such units will require greater wireless bandwidth and
coverage. Not only will users be able to communicate with others but the network will
be able to triangulate the user’s position. This would allow a central dispatcher to
determine and contact that practitioner who is closest to an emergency. The positive
effects of this level of mobility are endless.
8.2. EHR The issue of most importance regarding electronic health records is that of data
management. With millions of patients, searching for the desired data becomes a
difficult task. The solution is again tied with the theme of this chapter. That is, the
creation of a user friendly interface will eventually become more important than the
current technology efforts surrounding data creation and storage. Perhaps Google can
serve as a role model; they have implemented a method that can mine and manage data
most effectively.
Anecdotal evidence, at least in Alberta, suggests that healthcare professionals
working in hospitals are quick to adopt collaboration tools that allow them to share
information in real-time. This movement began with video conferencing but the portfolio
of such real-time tools is growing. Conversations with Albertan practitioners suggest that
webcam technology combined with other on-line tools is quickly replacing conventional
video conferencing. Following this trend to its natural conclusion suggests that the EHR
infrastructure will facilitate multiple specialist opinions at the same time for any given
Source: www.momentum.ca (Jan 2006)

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 47
record. Perhaps Session-In-Protocol (SIP), the technology behind instant messaging will
connect available professionals, resulting in multiple instant diagnoses.
Unlike Engineering, the healthcare profession seems to lack a centralized and
global repository of technical information such as the IEEE journal. There appears to be
great progress being made in biomedical engineering and nanotechnology applications
for healthcare. The resulting combined body of knowledge is distributed among varied
sources but many of these sources are managed by engineers. Clearly the complexity of
the healthcare profession warrants a global dedicated peer-reviewed database. The global
infrastructure provided by EHR naturally promotes such connectivity and it may provide
the impetus for this kind of collaborative change.
8.3. Privacy Issues As with any centralized database, the issue of privacy always remains of
paramount importance. The fundamental question is that of ownership and who has
access to the data. If the state owns the data then can the state access private information
to locate and identify potential criminals? If a private firm owns the data can the data be
mined or sold for marketing purposes?
There are some key problems associated with e-healthcare privacy issues. Firstly,
recall that one motivation for large scale electronic health records is the ability to track
the progression of disease. This requires on-going access to patient data and restrictive
privacy laws would reduce the effectiveness of this tool. Secondly, e-healthcare involves
a number of stakeholders. It is simple for a GP to ensure data privacy but policing all
related professionals is a very difficult task.
One method to mitigate such problems is to provide the patient with control over
which parties can access their data. This could be provided in the form of a blanket
waiver or access can be provided on a case by case basis. For specific data mining
applications, an automated search tool could be used to access patient information. The
tool would return only pertinent aggregate results without individual information. This is
largely the model that Google currently uses to place advertisements in their email
service and has so far been very effective.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 48
8.4. Implications for Practitioners Firstly, we must make a distinction between private clinics and hospitals. As our
investigations within Alberta uncovered, clinics use EHRs in their most basic form. In
fact most doctors still favour paper-based records. In clinics with EHRs, it appears that
doctors are responsible for entering prescriptions and diagnoses but much of the
administrative work such as entering lab results are left for Administrative Assistants.
Previously these Assistants were responsible for filing paper documents so it would
appear as though their work load has either stayed constant or perhaps slightly decreased.
Our conversation with hospital physicians uncovered a different situation. These
physicians appear to be responsible for both clinical and clerical work. They seemed
very quick to adopt technology that increases their productivity. Moreover, they appear to
be collaborating with multiple stakeholders so they are also quick to experiment with new
collaboration tools.
A recent 2005 commentary by Lori Rosmus addresses many of the changing
professional roles due to healthcare technology [46]. Her comments may help to explain
the relatively slow rate of adoption in private clinics. As we have mentioned earlier,
short term inefficiencies due to training and installation is perceived as a primary
deterrent.
Ms. Rosmus also notes some interesting political challenges. For example, some
pharmacists are unwilling to join a centralized system because doing so would give
physicians complete access to their patient information thereby “intruding into their
scope of practice.” Based on our interviews with the Pharmacists, their professional roles
may certainly be evolving. Currently, they describe their primary function as making
medical diagnoses and attempting to reduce adverse drug interactions. However, if
Doctors and Pharmacists both have access to the same information, would the Doctor not
be able to make such diagnoses prior to writing the prescription? In fact modern EHR
software often automatically scans for conflicting prescriptions. Eventually would
Pharmacists simply be double checking the advice of GPs and their software? This
potentially bleak future may certainly explain Ms. Rosmus’ comments. Divisive
developments between these two professionals are already beginning to take place in
Alberta. Pharmacists can now refill medication if the Physician is unavailable.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 49
Pharmacists may soon be able to write new prescriptions as well. Moreover, in
Newfoundland, Pharmacists are implementing an on-line pharmacy network. These
activities, which are undoubtedly empowering Pharmacists, seem to challenge the
collaborative spirit and intent of EHR. Assuming that these independent solutions and
dedicated databases can be integrated in the future, the process will certainly pose
difficulties.
Ms. Rosmus also examines the effect of EHR for nurses. Systems such as EHR
also require significant data entry and Nurses, for example, may be resistant to adopting
the technology since “the burden of data entry” may fall upon them. Again, this is a very
likely, though unfortunate consequence of digitization.
8.5. Interoperability When studying both EHR and PACS we found that though there is a strong
degree of protocol standardization taking place, there are still interoperability issues.
Most notably, the Baltic nations found that while all systems used the EDIFACT
protocol, customized implementations resulted in a lack of seamless communication.
Currently in most of the world, it appears as though HL7 is emerging and a dominant
standard but even HL7 has multiple variants. There continues to remain a strong
opportunity for a vendor to develop a versatile interface tool that can harmonize multiple
systems.
While most PACS implementations are currently regional there is every reason to
believe that with technological maturity and the elimination of bandwidth rationing,
PACS will merge with EHR systems. In other words, once text-based communication is
deployed and proven, national systems will begin to share other types of files including
the images from PACS. This will create even greater data sharing complexities. For
example, some sort of “digital wrapper” will be required that can both aggregate and
extract different data types.
A key factor is also that of language. The Rosetta Project is an ambitious venture
to catalogue all human languages and they have currently reached a count of 2,376 [47].
If one only considers the word’s dominant languages [48] they are:
1. Chinese (937,132,000)

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 50
2. Spanish (332,000,000) 3. English (322,000,000) 4. Bengali (189,000,000) 5. Hindi /Urdu (182,000,000) 6. Arabic (174,950,000) 7. Portuguese (170,000,000) 8. Russian (170,000,000) 9. Japanese (125,000,000) 10. German (98,000,000)
The point is that even if perfect electronic interoperability can be reached on a
global scale, the issue of language interoperability still remains. Despite being touted as
a global society the world is still highly segregated. Will English emerge as a standard
document communication language? Or can we bypass language barriers altogether by
communicating only important numbers and standardized lists of symptoms? Then
different user interfaces can simply translate the common numerical data and display the
information in any language. Of course not all symptoms and categories can be
anticipated so there must be some user-defined flexibility. However by standardizing
most common database fields, we may come close to the universal ideal.
While creating this global standard may seem like a daunting task, the formation
of the internet is proof that global databases are possible. The key requirements include
engaging all stakeholders, and having a versatile platform. Google’s success seems to
indicate that such objectives can be met commercially. However, there is an equally
strong business case for an open source community and openEHR is proof that progress
can be quickly made through non-commercial community efforts.
8.6. Network Availability Whether we consider the world class networks presented in this report or even
smaller deployments such as the Atlantic telei4 Network [49], they all show a disturbing
lack of consideration with regards to network availability.
Network availability is the long-term probability that a system will be operational
at any given instant. Consider two nodes (locations) that are connected by a single
network path. The availability measure is now a function of the reliability metrics of the
one path. We can substantially increase network availability if multiple paths connect the

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 51
two nodes. This is intuitively obvious; if one path breaks down, data can simply be
routed along another path. If multiple paths exist, the outage that the system will
perceive given one failure is the time required to switch data along a different path
(~50ms). On the other hand, if only one path exists, the outage that the system will
perceive given one failure is the time required to send a maintenance crew to repair the
damage (~days).
Many of the network topologies that we have researched for this report have only
one path connecting two nodes. Sjunet in Sweden appears to have the greatest built-in
robustness and redundancy as evidenced by its mesh-like architecture. It is unclear why
others have not followed this example. Either other implementers are unaware of proper
availability design techniques or are unwilling to spend the extra related infrastructure
costs. Both situations are cause for alarm. While sort-term costs may be lower, such
networks will require higher on-going maintenance charges and also result in more
dissatisfied users.
As we indicated earlier, most current deployments seem to be offered with
99.999% availability. These networks appear to be campus networks that integrate
multiple physical buildings into one seamless network. They do not appear to be
dedicated for PACS or EHR. Rather, these networks facilitate all healthcare applications.
Here is the list of current deployments once again:
Facility Beds Core speed Availability Vendor
Central DuPage 394 10-Gbps 99.999% Cisco
Clarian Health 1340 10-Gbps 99.999% Cisco
Austin Radiological Association 1.25-Gbps 99.999% LightPointe
Aurora Health Care 129 1-Gbps N/A Enterasys
Orlando Regional Healthcare 1,640 1-Gbps N/A Nortel
Peninsulas Health Care Corp 305 1-Gbps 99.999% 3Com
Queens Medical Center 526 1-Gbps N/A N/A
San Antonio Community Hospital 330 1-Gbps N/A N/A
North Kansas City Hospital 351 622-Mbps N/A N/A

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 52
As we have noted previously in this report, Cisco appears to be a prominent
player in healthcare networks. Not only have they deployed networks in the United
States, but they are responsible for the infrastructure needs of Canadian projects as well.
In particular, they provided the optical network and routers for the Alberta SuperNet.
This is particularly interesting since Nortel is the incumbent supplier.
Moreover, our research did not uncover regional deployments where the core
bandwidth was greater than 1-Gbps. Certainly there are networks such as CA*Net that
have 10-Gbps cores, but such semi-public networks facilitate many users and are not
dedicated to one site. However, these networks are interesting since they may be
signalling future direction. Recall that Alberta Health and Wellness announced that it
would be using the Alberta SuperNet to facilitate a PACS strategy. Certainly as more
advanced semi-public networks such as SuperNet allow organizations to lease bandwidth,
dedicated deployments may no longer be required. The additional complexity of
designing, sourcing and deploying networks can thus be avoided.
8.7. Legacy Data Converting all the old paper based records and transactions into electronic format,
is a very complex task. In Alberta, old documents are stored in Adobe Portable
Document Files (*.pdf). Though time intensive, scanning documents into such formats is
not very difficult. The problem is that such documents lack the flexible properties of an
original EHR document. Since they are not linked to database fields, searching for
specific data becomes very difficult: a more elaborate mechanism is required.
One strategy is to outsource the task of data entry to the patients themselves.
Since most EHR systems are web-enabled, a patient can access his/her records through
the internet. Then by answering a few guided questions, a user interface can help to fill
in most of the information. One would expect that a patient would be more
knowledgeable and precise about their history than any other party. Once entered, a GP
can simply verify the data and even release the old paper documents to the patient.
Certainly there will be special situations but these can be handled on a case-by-case basis.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 53
9. Conclusion
In conclusion, despite the great e-healthcare advancements in Scandinavia, it
appears as though other countries face some unique challenges. These include
competitive pressures of a free market economy, decentralized deployments and the
changing roles of established professionals. However, the relative freshness of this
global industry represents some very strong opportunities for both public and private
ventures. It appears that e-healthcare technology is ready for the next step of evolution.
Namely, now that proof of concept is no longer an issue, strong industry standards and
guidelines can be set. Any firm whether public or private that can lead this
standardization effort will likely emerge as a dominant participant. As we have
demonstrated through case studies, some of the major gains can be realized through
standard messaging systems. Moreover, while today there are multiple e-healthcare
applications, this industry will likely see application convergence. In other words,
eventually there will be only one user-friendly interface to PACS, EHR and other related
applications. However, getting to this ideal vision will require great tenacity and
innovation.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 54
10. References
[1] Goldstein, Douglas E. E-Healthcare: Harness the Power of Internet, e-Commerce & e-Care. Jones & Bartlett, 2000. [2] "SPIE—the International Society for Optical Engineering." 9 May 2006 <http://spie.org/>. [3] Fisher, Susan E. "The Facts About PACS." Health IT World. 9 May 2006 <http://www.health-itworld.com/emag/060104/205.html>. [4] "Medical Record." Wikipedia. 17 May 2006 <http://en.wikipedia.org/wiki/Medical_record>. [5] Mazurowski, Jay. "PACS: Planning for ROI." Decisions in Imaging Economics (2005). 10 May 2006 <http://www.imagingeconomics.com/library/200512-02.asp>. [6] Hujsak, Jonathan T. Digital Libraries and Corporate Technology Reuse. Tyrian Corporation. D-Lib Magazine, 1996. 11 May 2006 <http://www.dlib.org/dlib/january96/01hujsak.html>. [7] Ratib, O. "From PACS to the World Wide Web." Health on the Net (1997). 10 May 2006 <http://www.hon.ch/Library/papers/ratib.html>. [8] "One Network. A World of Choice." Advertisement. 11 May 2006 <http://www.nortel.com/solutions/enterprise/collateral/nn101480-0802.pdf>. [9] Nagy, Paul, and Jacob Farmer. Demystifying Data Storage: Archiving Options for PACS. Applied Radiology. 11 May 2006 <http://www.appliedradiology.com/articles/pdf/AR-05-04_nagy.pdf>. [10] Nagy, Paul, and Jacob Farmer. "Demystifying Data Storage: Archiving Options for PACS." Applied Radiology May (2004): 18-22. [11] Rosenfeld, Ken. "Adding Intelligence to Archiving of Data." Health Management Technology (2005). 10 May 2006 <http://www.healthmgttech.com/archives/0505/0505adding_intelligence.htm>. [12] "National Electrical Manufacturers Association." NEMA. 10 May 2006 <http://medical.nema.org/dicom/2004.html>.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 55
[13] Horii, Steven. Interview with National Committee on Vital and Health Statistics. Testimony by Steven Horii. 10 Oct. 2001. 10 May 2006 <http://www.ncvhs.hhs.gov/011010p3.htm>. [14] "Phillips Global PACS Business Unit." 10 May 2006 <http://www.stentor.com/pacs/>. [15] Baldwin, Fred D. "An Action PACS Market." Healthcare Informatics Nov. 2005. 11 May 2006 < http://healthcare-informatics.blacklabs.biz/issues/2005/11_05/cover_baldwin.htm >. [16] Richardson, William C. "To Err is Human." National Academy of Sciences (2000). [17] Walker, Jan. "The Value of Health Care Information Exchange and Interoperability." Health Affairs 24 (2005): 10-19. [18] Romanow, Roy J. The Future of Health Care in Canada. Commission on the Future of Health Care in Canada. National Library of Canada, 2002. [19] Rasmussen, Lars L. National IT Strategy for the Danish Health Care Service. The Ministry of the Interior and Health. National Board of Health, 2003. [20] Martin, Shelley. "Canadians Don’t Appear to Fear Electronic Medical Records." CMAJ 164 (2001): 1739. [21] Baker, M. L. "Patients Willing to Pay for Electronic Medical Records, Surveys Show." EWeek 22 July 2005. 10 May 2006 <http://www.eweek.com>. [22] "Medcom - Det Danske Sundhedsdatanet." 10 May 2006 <http://www.medcom.dk/> [23] Case Study: MedCom - the Danish Healthcare Data and Information Network. Empirica GmbH. Bonn, Germany, 2005. [24] Reding, Viviane. The Cost Benefit of Electronic Patient Referrals in Denmark. European Commission Information Society Directorate. Danish Center for Health Telematics. [25] "Silicon Valley's San Jose is the World's Most Knowledge Competitive Economy." Robert Huggins Associates 13 Dec. 2005. 10 May 2006 <http://www.hugginsassociates.com/latest_news.php>. [26] Sjunet - the Swedish Healthcare Network. Carelink. 2003. 10 May 2006 <http://www.itsweden.com/docfile/31930_Sjunet_the_swedish_healthcare_network.pdf>.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 56
[27] Health and Social Sectors with an "e": a Study of the Nordic Countries. Nordic Council of Ministers. Copenhagen: TemaNord, 2005. [28] Current European Practices in Ehealth: Survey of CARElink. European Commission. Sweden: RIDE Consortium, 2006. 17 May 2006 <http://www.srdc.metu.edu.tr/webpage/projects/ride/deliverables/RIDED.2.1.1 - CurrentPracticesSweden.pdf>. [29] Ehealth in the Context of Rural Broadband. a-bard. 2005. 10 May 2006 <http://www.abard.org/Repository/A-Bard_e-Health_topic.pdf>. [30] "Baltic E-Health." Danish Centre for Health Telematics. 10 May 2006 <http://www.baltic-ehealth.org/>. [31] Reding, Viviane. "Introduction to the Ministerial Round Table." E-Health 2005 Conference. Tromso, Norway. 23 May 2005. 10 May 2006 <http://europa.eu.int/comm/commission_barroso/reding/docs/speeches/ehealth-2005-round-table-intro.doc>. [32] Pedersen, Claus D. "An [sic] Baltic Healthcare Network and Interoperability Challenges." Cisco E-Health Think Tank Meeting. Brussels. 25 Jan. 2005. 10 May 2006 <http://www.baltic-ehealth.org/news/Ehealth-thinktank_25_01_05.ppt>. [33] Baldwin, Fred D. "An Action-PACS Market." Healthcare Informatics Online Nov. 2005. 10 May 2006 <http://www.healthcare-informatics.com/issues/2005/11_05/cover_baldwin.htm>. [34] "EHRVA." 10 May 2006 <http://www.himssehrva.org/>. [35] "OpenEHR." 10 May 2006 <http://www.openehr.org/>. [36] "IBM Federated Records Management." IBM. 10 May 2006 <http://www-306.ibm.com/software/data/cm/cmgr/rm/federated.html>. [37] "Canada Health Infoway." Government of Canada. 10 May 2006 <http://www.infoway-inforoute.ca/>. [38] "Alberta Supernet." 10 May 2006 <http://www.albertasupernet.ca/>. [39] Beaton, Mary. "Village Broadband in Hungary – Fantasy or Feasible?" BUTE-UNESCO Information Society Research Institute (2005). 10 June 2006 <http://istri.hu/english/docs/village_boradband_beaton.pdf>. [40] "NORTH Network." 10 May 2006 <http://www.northnetwork.com/>.

Prabhat Kulshreshtha – Medical Grade Telecom Networks Page 57
[41] "MBTelehealth - Linking Care Providers and Patients." 10 May 2006 <http://www.mbtelehealth.ca/>. [42] Irving, Richard. 2002 Report on Information Technology in Canadian Hospitals. Canadian Healthcare Technology. Thornhill Ontario, 2002. [43] Porter, Michael E. "Clusters and the New Economics of Competition." Harvard Business Review (1999): 77-90. [44] "Alberta Netcare." Alberta Government. 18 May 2006 <http://www.albertanetcare.ca/>. [45] "Momentum Healthware." 10 May 2006 <http://www.momentum.ca/>. [46] Rosmus, Lori. "Electronic Health Records: Benefits and Drawbacks." Faculty of Medicine and Dentistry (2005). 11 May 2006 <http://www.uahsj.ualberta.ca/files/Issues/2-1/html/38.htm> [47] "The Rosetta Project." 10 May 2006 <http://www.rosettaproject.org/>. [48] Languages of the World. Summer Institute for Linguistics. 1999. 10 May 2006 <http://www2.ignatius.edu/faculty/turner/worldlang.htm>. [49] "Health Infostructure Atlantic." Provincial Government of Nova Scotia. 10 May 2006 <http://www.gov.ns.ca/health/hia/>.