Embed Size (px)
Citation preview
n ew s
If you hand George Whitesides and colleagues of Harvard University some paper, a camera phone, and a few other odds and ends, they’ll give you back a complete biomedical diagnostic kit. In a recent article in AC (2008, 80, 3699–3707), the investigators describe a pack-age that captures data from paper-based microfluidic assays on a camera phone or digital camera and transmits the data to an off-site expert for analysis and interpretation. The do-it-yourself diagnostic kit can be used in developing countries or in remote locations where it is costly and difficult to place specially trained personnel.
Several reasons prompted the White-sides group’s interest in developing low-cost diagnostic devices. First, Whitesides says that the scientific and medical communities have to find a way to distribute health care benefits from the more developed nations to the less developed ones.
The second reason involves innova-tive developing countries (IDCs), such as India, China, and Brazil. IDCs have skilled workforces and resources but re-quire technology to grapple with issues of environmental monitoring, homeland security and border control, and medi-cine. Because the scale of poverty is vast in these countries, diagnostics must be inexpensive. “Obviously, you never get to zero costs,” says Whitesides. But if the goal is to make the cost of the anal-ysis close to zero, then “it turns out to be immensely interesting both techno-logically and scientifically.”
Another reason to develop the de-vices is that the U.S. has to rethink the way in which it handles and implements its own medical care. “We’re absolutely focused on end-of-life, expensive, high-technology medicine. There isn’t a lot of indication that’s the best and most cost-effective way of providing improved health care to the citizens of the coun-try,” states Whitesides.
Diagnostics are only a small part of the problem, he concedes, “but a focus
on them is not a bad one because of the old business school adage, ‘You can’t manage it if you can’t measure it.’”
The investigators patterned What-man paper with a photoresist to create a microfluidic device with a central channel and four side channels leading to wells for different colorimetric assays. Whatman paper wicks fluids well, so it can soak them up without an external pumping source, and it filters out par-ticulate material.
The investigators embedded the reagents for glucose and protein assays within the wells. Glucose detection was based on two enzymatic reactions: glu-cose oxidase catalyzes the oxidation of glucose to gluconic acid and hydrogen peroxide, and horseradish peroxidase
catalyzes the reduction of hydrogen per-oxide to produce the visible oxidation of iodide to iodine (colorless to brown). The protein assay was based on the bind-ing of tetrabromophenol blue (TBPB) to proteins. TBPB’s phenol deprotonates when bound by protein, and the dye changes from yellow to blue. Artificial urine was used as the diagnostic fluid to test the proof of concept.
The investigators tested data capture on two types of camera phones, a por-table scanner, a desktop scanner, and a digital camera. The rationale for using camera phones is their ubiquity (in In-dia, 6 million people register new cell phones each month). Whitesides and colleagues downloaded the images to a computer, converted the colors to a gray scale for the glucose assay and to the CMYK (four-color) scale for the protein assay, and quantified the data.
The package has worked well in the lab, but Whitesides says they haven’t rushed to test it in the field. He says, “Lots of people want to try new tech-nology—there’s no problem in that at all. But you get one shot. If you come up with a neat device and it just fails hopelessly, you don’t get a second chance.” The investigators are still deal-ing with some issues. For instance, the assays are now shelf-stable for 30 days, but the investigators are figuring out how to make them last longer.
Although the project has a well-defined real-world application, it’s also proving to be scientifically rich. “You can look at this and say this is just an en-gineering project. You are taking lateral flow assays and making them smaller. It turns out not to be the case at all,” says Whitesides. “A whole series of problems has come up when you begin to think of paper as a porous material—the phys-ics of fluid flow, evaporation, and heat flow. . . . Everywhere we look, it turns out there are very fundamental scientific questions that go along with the clear application objective.” a
—Rajendrani Mukhopadhyay
Medical diagnostics with paper and camera phones
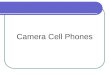
The entrance to the microfluidic deviceis dipped into urine.
An imaging devicedigitizes the resultsand transmits themto an expert.
An expert interpretsthe results and recommends a treatment.
Urine wicks into the assay zones.
Urine
Inexpensive bioassays are performed in paper-based microfluidic devices in a remote location. The test results are sent for interpretation via a camera phone or a por-table scanner to experts who are off-site.
J u n e 1 , 2 0 0 8 / A n A ly t i c A l c h e m i s t r y 3 9 4 9
![JT-60U diagnostics. Infra-red Camera for Divertor Plate [Objectives] Surface temperature of the divertor tiles are measured by Infrared camera system](https://img.pdfslide.us/doc/110x75/56649e175503460f94b02c2b/jt-60u-diagnostics-infra-red-camera-for-divertor-plate-objectives-surface.jpg)