Embed Size (px)
Citation preview
932
steady or, in some instances, reducing the intake of medicalstudents.
W. KEITH C. MORGAN.
Department of Medicine,West Virginia University
School of Medicine,Morgantown,
West Virginia 26506, U.S.A.
EFFECT OF ORAL CONTRACEPTIVES ONVITAMIN-B12, METABOLISM
A. MAJID SHOJANIA.
Department of Hematology,St. Boniface General Hospital, and
Department of Pediatrics,University of Manitoba,
Winnipeg, Canada.
SIR,-Low serum folate and vitamin-B12 levels are
common in pregnancy, and are generally attributed to
parasitisation by the fetus. We have reported that women onoral contraceptives have lower serum and red-cell folate 1than controls, which suggests that hormonal factors maybe involved in folate deficiency of pregnancy.To determine whether the fall in serum-B12 during
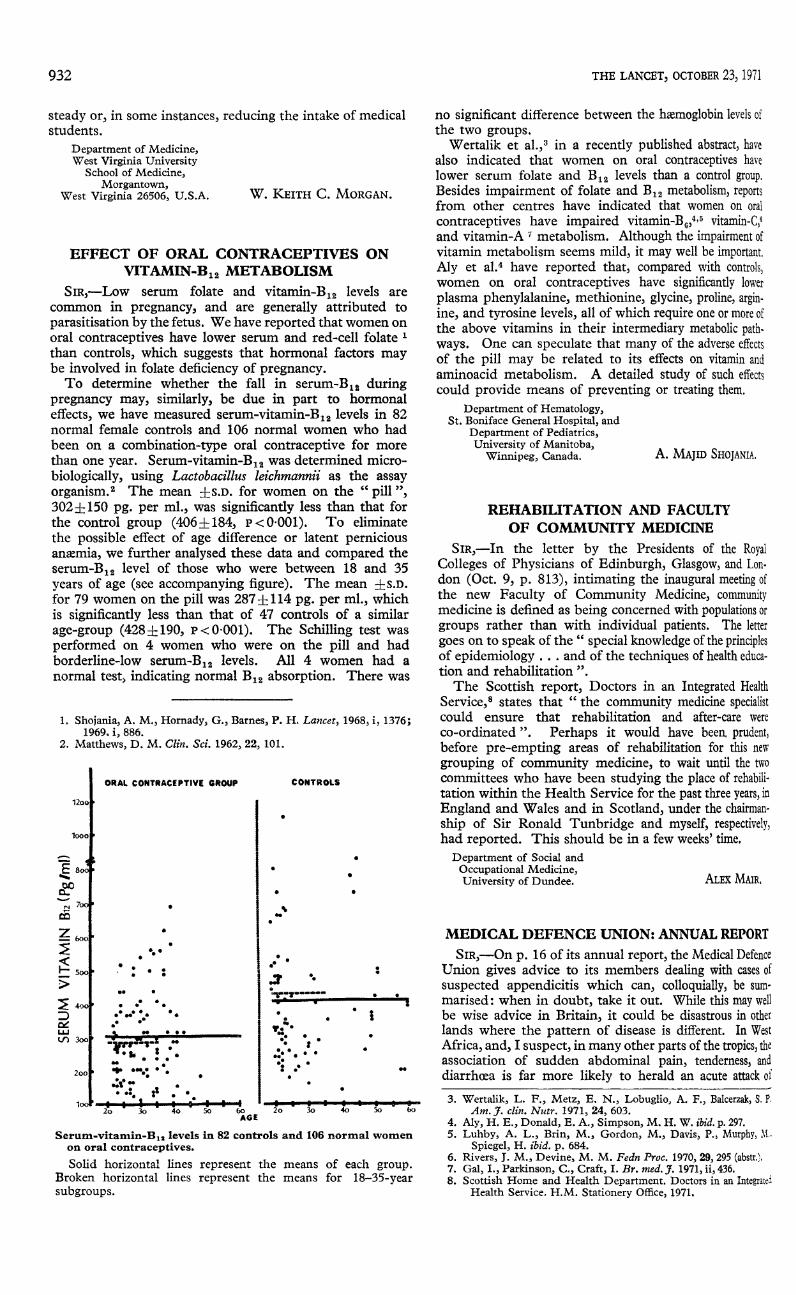
pregnancy may, similarly, be due in part to hormonaleffects, we have measured serum-vitamin-B12 levels in 82normal female controls and 106 normal women who hadbeen on a combination-type oral contraceptive for morethan one year. Serum-vitamin-B12 was determined micro-biologically, using Lactobacillus leichmannii as the assayorganism. 2 The mean ±s.D. for women on the " pill ",302.+50 pg. per ml., was significantly less than that forthe control group (406+184, p< 0-001). To eliminatethe possible effect of age difference or latent perniciousanxmia, we further analysed these data and compared theserum-B12 level of those who were between 18 and 35years of age (see accompanying figure). The mean ::f::S.D.for 79 women on the pill was 287+114 pg. per ml., whichis significantly less than that of 47 controls of a similarage-group (428+190, p< 0-001). The Schilling test wasperformed on 4 women who were on the pill and hadborderline-low serum-B12 levels. All 4 women had anormal test, indicating normal B12 absorption. There was
1. Shojania, A. M., Hornady, G., Barnes, P. H. Lancet, 1968, i, 1376;1969, i, 886.
2. Matthews, D. M. Clin. Sci. 1962, 22, 101.
Serum-vitamin-B.. levels in 82 controls and 106 normal womenon oral contraceptives.Solid horizontal lines represent the means of each group.
Broken horizontal lines represent the means for 18-35-yearsubgroups.
no significant difference between the hxmoglobin levels ofthe two groups.
Wertalik et all in a recently published abstract, havealso indicated that women on oral contraceptives havelower serum folate and B12 levels than a control group.Besides impairment of folate and B12 metabolism, reportsfrom other centres have indicated that women on oral
contraceptives have impaired vitamin-B6,4,5 vitamin-C,6and vitamin-A ’ metabolism. Although the impairment ofvitamin metabolism seems mild, it may well be important.Aly et al.4 have reported that, compared with controls,women on oral contraceptives have significantly lowerplasma phenylalanine, methionine, glycine, proline, argin-ine, and tyrosine levels, all of which require one or more ofthe above vitamins in their intermediary metabolic path.ways. One can speculate that many of the adverse effectsof the pill may be related to its effects on vitamin andaminoacid metabolism. A detailed study of such effectscould provide means of preventing or treating them.
REHABILITATION AND FACULTY
OF COMMUNITY MEDICINE
ALEX MAIR.
Department of Social andOccupational Medicine,University of Dundee.
SIR,- In the letter by the Presidents of the RoyalColleges of Physicians of Edinburgh, Glasgow, and Lon-don (Oct. 9, p. 813), intimating the inaugural meeting ofthe new Faculty of Community Medicine, communitymedicine is defined as being concerned with populations orgroups rather than with individual patients. The letter
goes on to speak of the " special knowledge of the principlesof epidemiology ... and of the techniques of health educa-tion and rehabilitation ".The Scottish report, Doctors in an Integrated Health
Service states that " the community medicine specialistcould ensure that rehabilitation and after-care were
co-ordinated ". Perhaps it would have been prudent,before pre-empting areas of rehabilitation for this newgrouping of community medicine, to wait until the twocommittees who have been studying the place of rehabili-tation within the Health Service for the past three years, in
England and Wales and in Scotland, under the chairman-ship of Sir Ronald Tunbridge and myself, respectively,had reported. This should be in a few weeks’ time.
MEDICAL DEFENCE UNION: ANNUAL REPORT
SIR,-On p. 16 of its annual report, the Medical DefenceUnion gives advice to its members dealing with cases ofsuspected appendicitis which can, colloquially, be sum-marised : when in doubt, take it out. While this may wellbe wise advice in Britain, it could be disastrous in otherlands where the pattern of disease is different. In WestAfrica, and, I suspect, in many other parts of the tropics, theassociation of sudden abdominal pain, tenderness, anddiarrhoea is far more likely to herald an acute attack of
3. Wertalik, L. F., Metz, E. N., Lobuglio, A. F., Balcerzak, S. P.Am. J. clin. Nutr. 1971, 24, 603.
4. Aly, H. E., Donald, E. A., Simpson, M. H. W. ibid. p. 297.5. Luhby, A. L., Brin, M., Gordon, M., Davis, P., Murphy, M.,
Spiegel, H. ibid. p. 684.6. Rivers, J. M., Devine, M. M. Fedn Proc. 1970, 29, 295 (abstr.).7. Gal, I., Parkinson, C., Craft, I. Br. med. J. 1971, ii, 436.8. Scottish Home and Health Department. Doctors in an Integrated
Health Service. H.M. Stationery Office, 1971.

933
dysentery than one of appendicitis. This is a well-known
pitfall for the surgeon newly arrived in the tropics, whereappendicitis is relatively rare. Laparotomy under suchcircumstances is the worst possible treatment and may welllead to a fatal result.
H. MILNES WALKER.
Newfield,Bickerton,Cheshire.
DIFFERENCES IN THE TWO RED-CELL
POPULATIONS IN ERYTHROLEUKÆMIA
AXEL KAHNMILIA VROCLANS
JACQUES HAKIMPIERRE BOIVIN.
Department of Hæmatology,Hôpital Beaujon-92,
Clichy, France.
SiR,-In a patient with erythroleukasmia, we haveobserved two erythrocytic populations differing in the
antigenic features of their ABO systems, the activity ofsome of their enzymes, and the level of hxmoglobin A2.The patient’s blood-group, as determined before the
disease was discovered, was Ai. After the onset of thedisease, 50% of the red blood-cells (R.B.C.) were entirelynon-agglutinable by anti-A and anti-A1 sera, but their rateof agglutinability was higher than normal, with anti-I,anti-i, and anti-H sera. These two populations wereseparated with anti-A serum. Enzyme activities were verydifferent in the two populations (table I). The activity of other
TABLE I-ENZYME ACTIVITIES IN THE TWO ERYTHROCYTE
POPULATIONS
enzymes was only studied in the abnormal population.It was higher than normal for all except phosphofructokin-ase, which was normal, and glutathione reductase and thephosphohexose isomerase, which were 35% lower thannormal.
Starch-gel electrophoresis, by the method of Fildes andHarris,2 showed that the phenotype of adenylate kinasewas AK1-l in both populations, and that the enzyme wasdeficient in the abnormal population. In isolated granu-locytes, the enzyme activities were either normal or
increased, except in the case of pyruvate kinase and thephosphohexose isomerase, which were just below normal.
Study of glycolytic intermediates of red blood-cellsperformed on the complete erythrocytic population showedonly a low level of A.T.P. (65% of normal). Finally, theresults of haemoglobin electrophoresis and assay of thefraction resistant to alkaline denaturation, in both popu-lations, are shown in table II.These results prompt the following comments:
1. Enzyme abnormalities, sometimes with an increasein hemoglobin F, and blood-group antigenic abnormali-ties are frequently found in acute leukxn-lia 3 or refrac-tory anasmia 1; our patient’s condition is very closeto both diseases.
2. The association of a major weakening of groupantigenic substances in the ABO system togetherwith a very important deficiency of adenylate kinase inthe same erythrocyte population is particularly interesting,
1. Boivin, P., Galand, C., Dreyfus, B. Nouv. Rev. fr. Hémat.1969, 9, 105.
2. Fildes, R. A., Harris, H. Nature, 1966, 209, 261.3. Stratton, F., Renton, P., Hancock, J. A. ibid. 1958, 181, 62.
TABLE HŁHEMOGLOBIN ELECTROPHORESIS IN THE TWO
POPULATIONS
in view of the genetic link between these two systems.4 4It suggests a chromosome lesion in the part holdingboth loci-structural genes of adenylate kinase and ofthe specific transferase of substance A.
3. The increase of almost all enzyme activities in theabnormal population could be due to the youth of thepopulation, and to early hxmolysis; this agrees withthe finding of a reticulocytosis of about 250,000 perc.mm., which still does not compensate his anaemia.
SEA-BLUE HISTIOCYTES IN A RABBIT
ARTHUR SAWITSKYFRED ROSNER.
Long Island Jewish Medical Center,New Hyde Park, N.Y. 11040, U.S.A.
SIR9 The sea-blue-histiocyte syndrome in man is nowa well-established entity, although the specific biochemicaldefect remains to be elucidated. 5 An animal model forthe study of this disorder may have been found in ourserendipitous discovery of classic sea-blue histiocytes in thebone-marrow aspirate of a " healthy " rabbit. Unfortunately,no other anatomical material from this rabbit was madeavailable to us for study. We have since examined 14additional rabbits, none of which was found to haveabnormal cells in their bone-marrow aspirates. We are
continuing our search, and solicit frozen spleen tissueshould any investigator find another such animal. Histio-cytosis resembling lipid-storage disorders in man hasrecentlv been described in two pies and a cow.6
S.O.S.
SIR,-We were interested by Dr. G. H. Robb’s paper,Understanding Prescriptions (Sept. 25, p. 700). Thisarticle should also prove interesting to medical historianssince, as long ago as 1958, the Aitken Report on control ofdangerous drugs and poisons in hospitals recommendedthat the Latin abbreviations s.o.s. and p.r.n. should not beused. There has always been confusion in the interpre-tation of these two abbreviations, and Dr. Robb himselfseems to be at variance with many standard texts 11-14 in hisdefinition of s.o.s. We wish to endorse Dr. Robb’s con-clusion that prescription sheets should be modified so that
4. Rapley, S., Robson, E. B., Harris, H., Smith, S. M. Ann. hum.Genet. 1967, 31, 237.
5. Karayalcin, G., Rosner, F., Sawitsky, A. Lancet, Aug. 7, 1971, p. 318.6. Sandison, A. T., Anderson, L. J. J. Path. 1970, 100, 207.7. Report of the Joint Sub-Committee on the control of Dangerous
Drugs and Poisons in Hospitals. H.M. Stationery Office, 1958.8. Jones, B. R. in Pharmacology for Student and Pupil Nurses and
Student Pharmacy Technicians. London, 1971.9. Trounce, J. R. in Pharmacology for Nurses. London, 1970.
10. Tonkin, R. D., Gibberd, F. B. in Nurses Handbook of CurrentDrugs. London, 1967.
11. Lewis, J. G. in Therapeutics. Oxford, 1968.12. Sears, W. E. in Materia Medica for Nurses. London, 1959.13. Pearce, E. in Medical and Nursing Dictionary and Encyclopædia.
London, 1966.14. Spencer, M., Tait, K. M. in Introduction to Nursing. Oxford, 1970.