Embed Size (px)
Citation preview
Medical Decision
Making
Michael Nauss MD FACEP
Senior Staff
HFH Dept. of Emergency Medicine
Billing 101:
Down coding
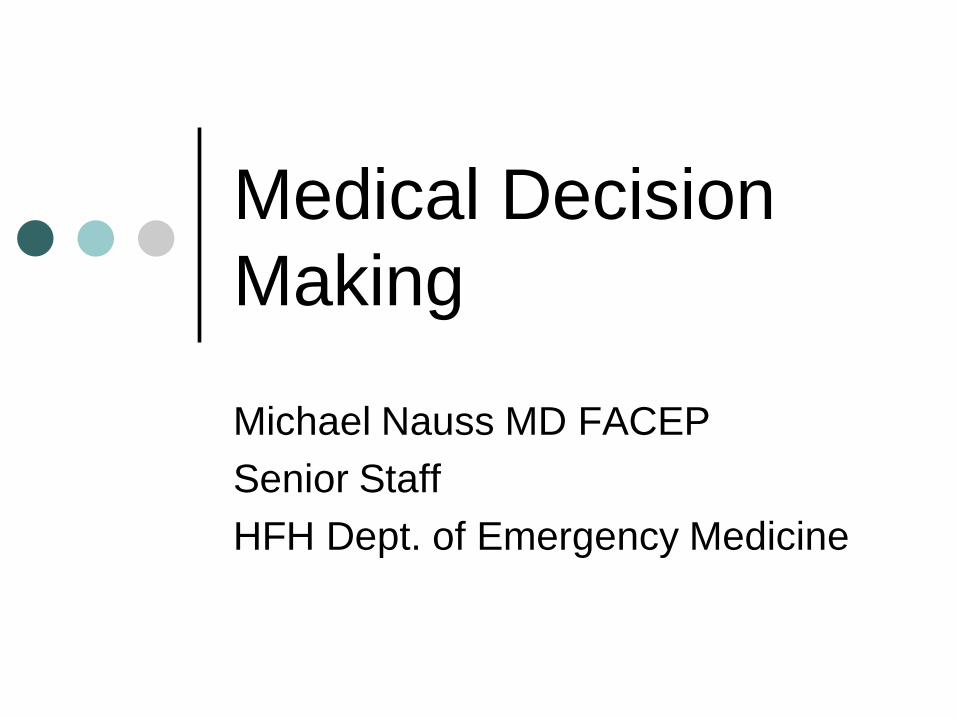
Compared to national benchmark:
• HFH -1% on critical care
• When compared to Level 5 billing:
• Loss of $220 professional charges/pt
• Loss of $765 facility charges/pt
• HFH -9% Level 5 charts
• When compared to Level 4 billing:
• Loss of $215 processional charges/pt
• Loss of $494 facility charges/pt
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
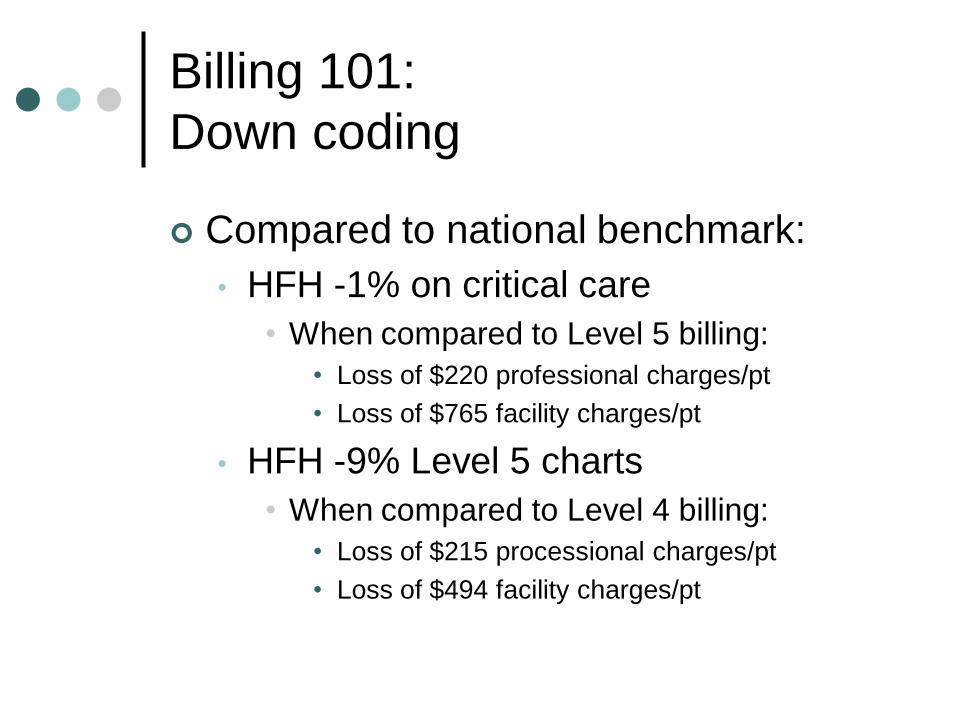
99281 99282 99283 99284 99285 99291 99292 Other
DEM Mean
FSPC Mean
July-Dec 2013
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
99281 99282 99283 99284 99285 99291 99292 Other
DEM Mean
FSPC Mean
Jan-June 2013
Downcoding
Focus on 10% of patients
Can increase charges by 20%
Why do you care ?
You will…in less than 3 years
What is good for the dept. affects you
Revenue = power
What can you do to help?
Improve documentation
To reflect what we actually see and do
To reflect the complexity of our
patients and our workup’s
To capture the appropriate revenue
“Level 5 Chart”
HPI: Four
location, quality, severity, timing,
associated sx, duration, context,
modifying factors
ROS: Ten
• Constitutional, Eyes, ENMT, CV,
Respiratory, GI, GU, MSK,
Integumentary, Neuro, Psych,
Endocrine/Metabolic,
Hematologic/Immunological
“Level 5 Chart”
ROS
“Do you have any fever, chills,
nausea, vomiting, cough, sore throat,
rashes or bruises, pain in your head,
back, belly, chest, or burning when
you urinate ?”
There is your 10 in once phrase….
“Level 5 Chart”
PMHx, Family Hx, Social:
Three: Epic does this for you (mostly)
PE
8 systems
• Constitutional, Eyes, ENMT, CV, Resp.,
GI, GU, MSK, Skin, Neuro., Psych,
Heme/Immun.
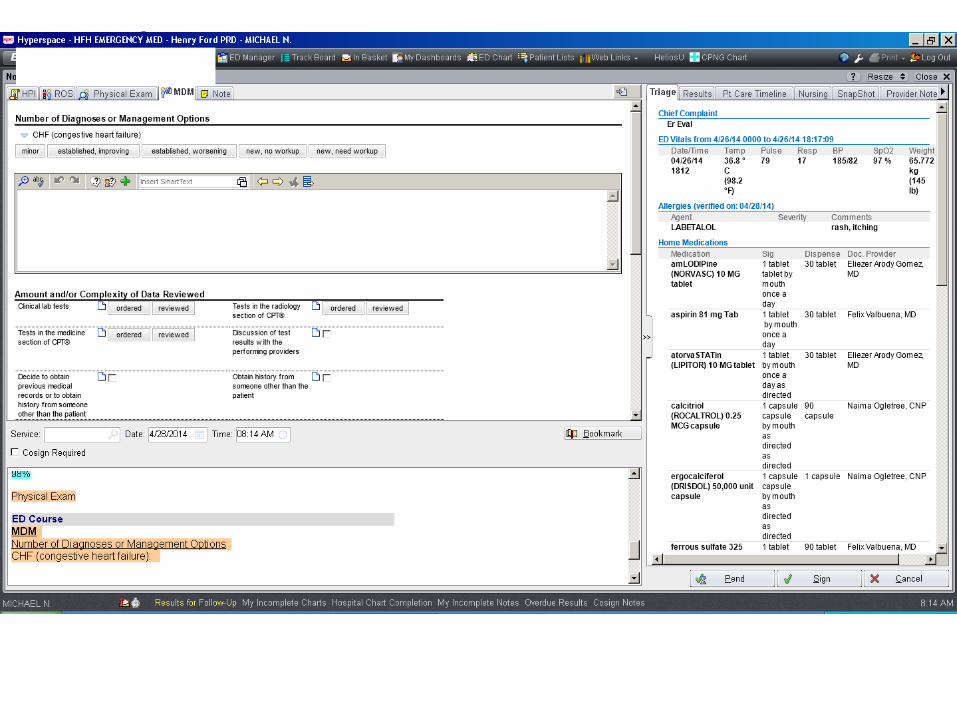
MDM
MDM
In talking with coding…this is our #1
issues….
Because we often don’t do it
And please….Fill out the boxes….
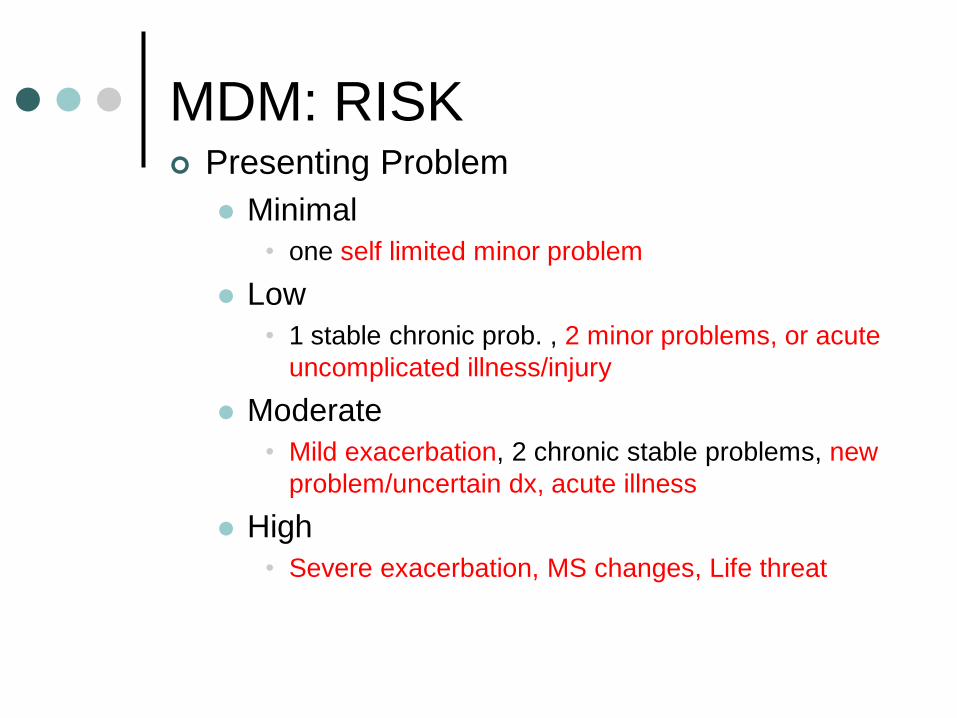
MDM: RISK Presenting Problem
Minimal
• one self limited minor problem
Low
• 1 stable chronic prob. , 2 minor problems, or acute
uncomplicated illness/injury
Moderate
• Mild exacerbation, 2 chronic stable problems, new
problem/uncertain dx, acute illness
High
• Severe exacerbation, MS changes, Life threat
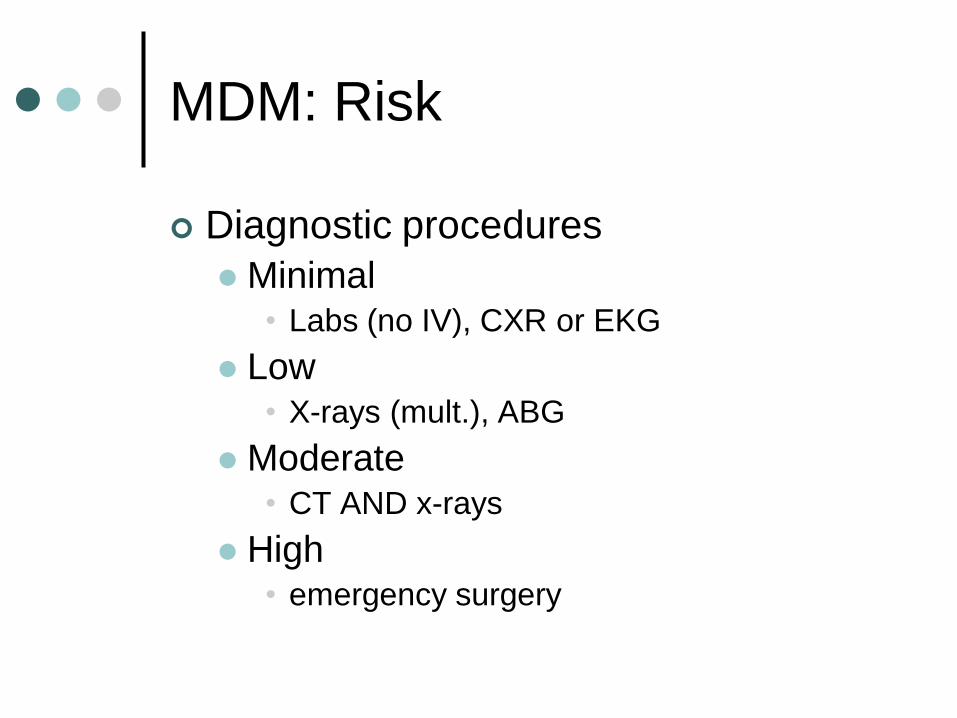
MDM: Risk
Diagnostic procedures
Minimal• Labs (no IV), CXR or EKG
Low• X-rays (mult.), ABG
Moderate• CT AND x-rays
High• emergency surgery
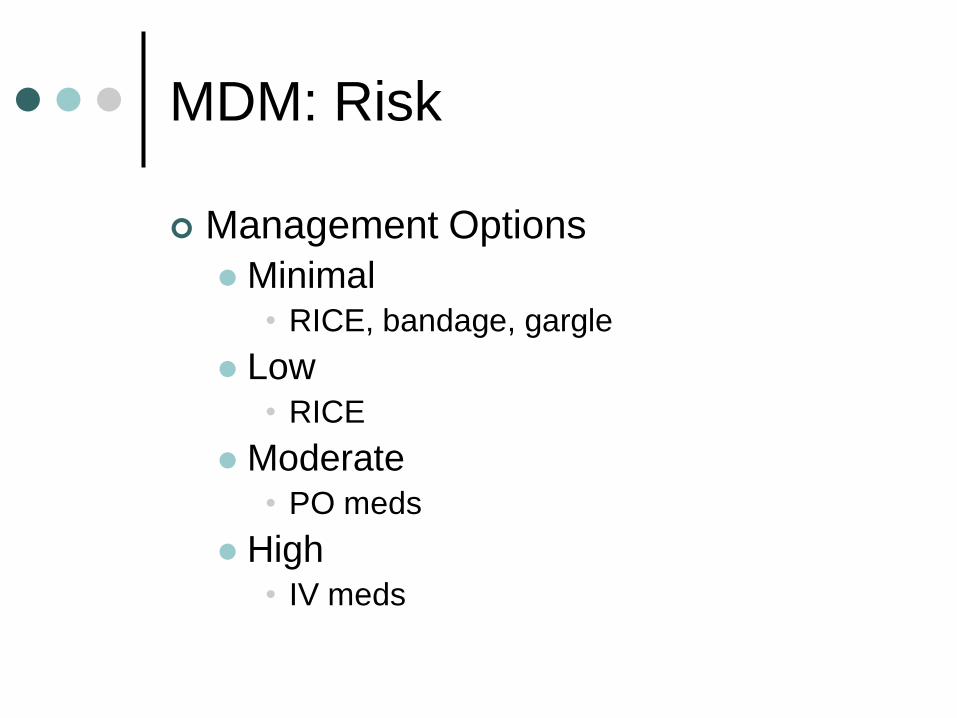
MDM: Risk
Management Options
Minimal• RICE, bandage, gargle
Low• RICE
Moderate• PO meds
High• IV meds
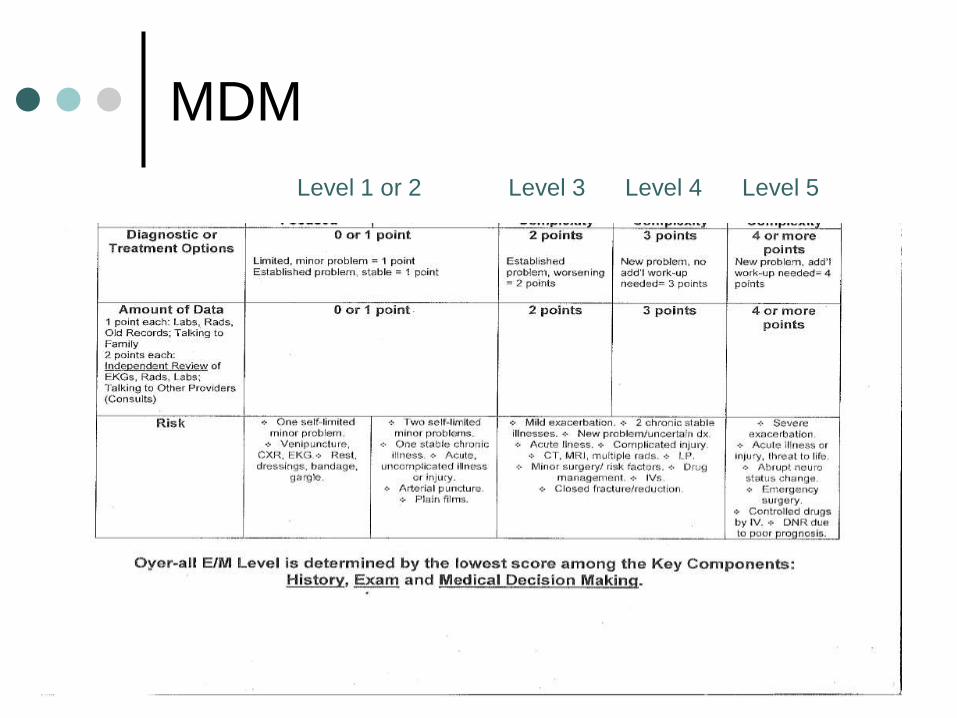
MDM
Level 1 or 2 Level 3 Level 4 Level 5
Critical Care
Can be billed by staff only
Do not click “CC” in your notes
Medical Decision Making
Arguably the most important piece of
the medical chart
HPI “paints a picture”
MDM “plays art critic”
Common Mistakes
Missed information on
triage/EMS/nursing notes (general ED
notes)
“worse HA of life”
“slurred speech”
Common Mistakes
Unanswered abnormal VS
Unanswered abnormal VS
Unanswered abnormal VS
Unanswered abnormal VS
Unanswered abnormal VS
Unanswered abnormal VS
Unanswered abnormal VS
Common Mistakes
Lack of patient reassessment
VS
Pain
Symptom relief
• CP
• Abd. Pain
• Vomiting
• Wheezing
Common Mistakes
Poor consult documentation
Who did you talk to and when
• Make consultant aware of charting
“curb-siding”
Common Mistakes
Discharge Instructions
Ambiguous
No information on what to watch for or
why to come back
Lack of follow up instructions (and
time course to do so)
Common Mistakes
Non Documentation
Procedures and failed attempts etc.
• Also hurts from a billing standpoint
Information from old chart/OSH
Repeat EKG’s (order and document)
Adverse events
• Itching after med. etc.
Community Experience
Regional Group
Risk Management Audit
• Abdominal Pain
• Chest Pain
• HA
• Fever in Child
CC’s represent 75% of dollars lost in
ED suits
Community Experience
How this is done
12 charts (3 per CC)
3-4 months after hire
Sit down evaluation with Risk
Management physician
HFH Experience
Charting metric
Twice a year for PGY-2 and above
Yearly for PGY-1’s
Building a Chart
EMR dependent
Typing is not ideal (…job seekers)
Be aware of templates/macros
• LE Amputees with +2 DP/PT pulses
bilaterally are unusual and hard to find
• preformatted discharge instructions…
How to Put it Together
Just put it somewhere
MDM section
• Reassessment (.now phrase)
• Diff Dx.
How to Put it Together
Summarize
Presentation• This is a patient who presented with
cough and SOB
ED Course• Pt. was given nebs/steroids and labs/cxr
were obtained
Studies • Labs unremarkable (.edlabs)
• CXR showed no pna
How to Put it Together
Summarize
Patient Response to Tx:
• Pt states she felt better after tx
• Eating/Up and ambulatory in ED
• Asking for to go home
How to Put it Together
Evaluate the Differential Dx.
Based on…. I doubt ….
• EKG unchanged, no exertional
component to symptoms I doubt ACS
• No leg swelling/pain, no travel or recent
surgery I doubt PE
Given …. I favor ….
• Pt. has hx of COPD, improved with nebs
and steroids I favor COPD exacerbation
How to Put it Together Case for Discharge/Treatment Plan
Why is this COPD exacerbation going home?
• Given pt. does not desat. during ambulation, is afebrile, feels improved, I feel they can be d/c with oral steroids and abx as well and increase home neb. use
Follow up
Phone call Ability to obtain timely f/u
• iPhone etc.
• Document the call/attempt
How to Put it Together
Discharge Info.
Spell out exactly what to watch for and
reasons to seek further care
Follow up (did you talk with PMD)
“…return if worse or if concerned”
Incidental findings: document in chart
and on d/c Instructions
• Need for repeat cxr in 6 months etc.
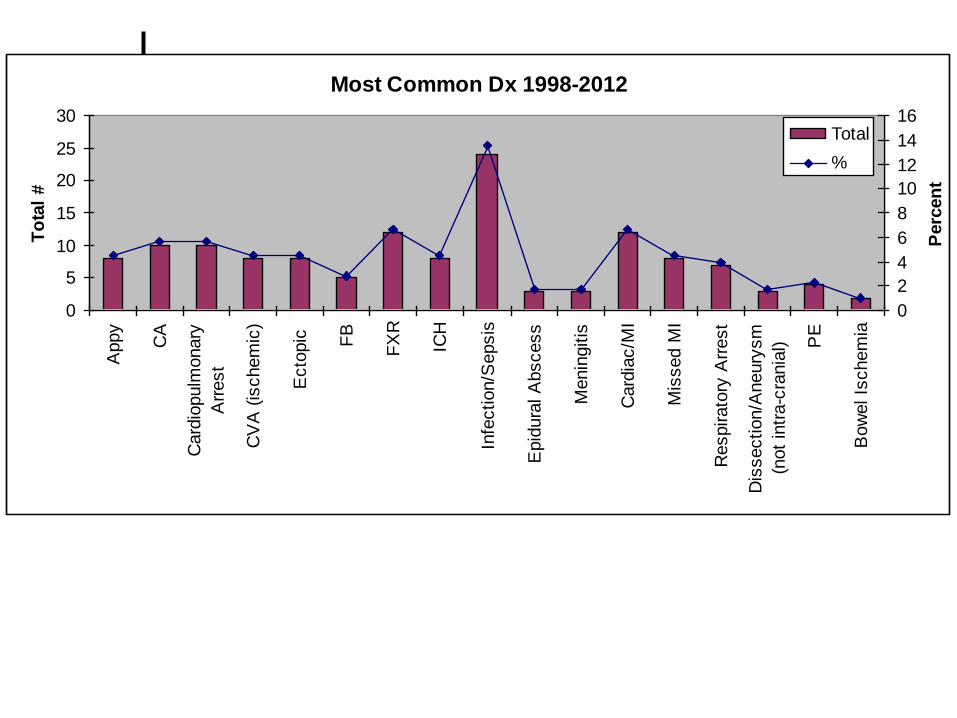
Most Common Dx 1998-2012
0
5
10
15
20
25
30A
ppy
CA
Card
iopulm
onary
Arr
est
CV
A (
ischem
ic)
Ecto
pic
FB
FX
R
ICH
Infe
ction/S
epsis
Epid
ura
l A
bscess
Menin
gitis
Card
iac/M
I
Mis
sed M
I
Respirato
ry A
rrest
Dis
section/A
neury
sm
(not
intr
a-c
rania
l) PE
Bow
el Is
chem
ia
To
tal
#
0
2
4
6
8
10
12
14
16
Perc
en
t
Total
%
How to Put it Together
(finally)
Case for Admission
Medical Necessity
Important for billing (ATMO/IPAS too)
Why is this COPD exacerbation being
admitted ?
• Increased O2 requirement
• Abnormal CXR
• Need for serial cardiac markers etc.
Coding Queries
As of 7/31
$ 55,000 waiting on resident charting
(queries only) to be billed
Finish carts same day/next day
Respond to queries ASAP (even off
service)
Ask me if ?’s
Coming to a ED near you:
Summary MDM
Needs to play a larger role in
documentation
Should reflect disposition thought
processes and data
Must include commonly missed items
• Abnormal VS, reassessments etc.
Follow up and discharge instructions
ought to be viewed with increased
importance