Embed Size (px)
Citation preview

Medical Consultant Report (To be completed by medical consultant)
Medical Consultant Name: Ronald E. Goans, PhD, MD, MPH Report Date: 12/4/2007
Licensee Name: Karmanos Cancer Center
License No. 2 1-04 127-06 Event No. 43746 Docket No. 030-09376
Facility Name: Kmanos Cancer Center
Incident Date: 10/24/2007
Date of Notification: 10/25/2007
Individuals’ / Patient Physician Name and Address:
Maria T. Vlachaki, MD Clinical Director, Radiation Oncology Karmanos Cancer Center Wayne State University 4100 John R Detroit, Michigan 4820 1
Individuals Contacted During Investigation:
Maria T. Vlachaki, MD Clinical Director, Radiation Oncology Karmanos Cancer Center Wayne State University 4 100 John R Detroit, Michigan 48201 (3 13) 993-8730
Joe Rakowski, PhD Medical Physicist, RSO Karmanos Cancer Center Wayne State University 4100 John R Detroit, Michigan 48201 (3 13) 996-2260
Issued 11/07 M. Jelich Gsmms K n i i 1

Records Reviewed: (General Description)
1. 2. 3. 4. 5 . 6. 7. 8. 9. 10.
NRC Enclosure - Description of the Medical Event Draft document - Description of the event; NRC fax 10/25/2007 NRC Preliminary Notification of Event (Event # 43746) NRC Medical Event - 15 day report from licensee Karmanos Cancer Center correspondence to the NRC Detailed review of patient records and photographs Karmanos Cancer Center documents on event analysis and remediation efforts Karmanos Cancer Center Gamma Knife planning form Karmanos Cancer Center Gamma Knife Re-procedure checklist Karmanos Cancer Center Time-out draft document
Estimated Dose to Unintended Anatomic Region (see appendix A). By assessment of clinical signs:
18 Gy to left cerebellum (normal brain tissue); no adverse clinical signs or symptoms at this time.
Probable Error Associated with Estimation: < 10 %; the 18 Gy dose was planned but delivered to the wrong side of the cerebellum.
Prescribed Dose (Medical Misadministration Only):
18 Gy to right cerebellar lesion.
Method Used to Calculate Dose: Radiation oncology clinical dose profile and physical dosimetry.
Description of Incident:
On October 24,2007, a medical event occurred at the Leksell Gamma Knife facility at the Wayne State - Karmanos Cancer Center which resulted in the total dose delivered differing from the prescribed dose by more than 20%. The patient is a 64 year old female with a history of small cell lung cancer. She previously underwent chemotherapy and radiation therapy, along with 25 Gy to the whole brain in 10 fractions. The patient subsequently developed a metastatic lesion in the right cerebellum and was prescribed 18 Gy via gamma knife therapy to the nodule at the 50% isodose line.
Due to a left - right reversal of the treatment planning MRI images, the patient's left side was targeted and treated rather than the right side. The patient was treated with one shot of 18 mm at a gamma knife angle of 140 degrees. The error resulted in an 18 mm shift of isocenter across midline of the brain. The collimator diameter selected for the treatment was 18 mm, thus resulting in some overlap of the delivered 50% isodose volume with the correct intended target lesion volume. The event resulted in approximately 7% of the lesion volume receiving the prescribed dose of 18 Gy to the 50% isodose, rather than the preferred 95% of the lesion volume.
During the pre-treatment setup and simulation with MRI imaging, a caudal view was selected by the technician whereas the patient should have had a cranial view selected. This had the effect of reversing the axial images left to right. The standard of practice in gamma knife radiosurgery is to position the patient in the MRI scanner head first, and to use the cranial scan technique. The caudal MRI images were imported into the Gamma Knife treatment planning computer, and
Issued 11/07 M. Jelich Gamma Knife 2
subsequently registered as cranial. This resulted in the wrong side of the patient being targeted and treated, i.e. the left cerebellum was targeted and treated rather than the right cerebellar lesion.
Clinical Details (See Appendix 1 for planned and given dose profiles)
The patient is a 64 year old, right-handed female with a history of small cell lung cancer diagnosed in 2005. The past medical history is pertinent for a 40 pack-year smoking history and bilateral breast cancer diagnosed in 1992. The patient previously underwent chemotherapy and radiation therapy for the small cell tumor, along with 25 Gy to the whole brain in 10 fractions. She subsequently developed a metastatic lesion to the right cerebellum and was prescribed 18 Gy gamma knife stereotactic radiosurgery to the nodule at the SO?! isodose line. The patient currently also has metastatic disease to the liver.
Assessment of Probable Deterministic Effects of the Radiation Exposure on the Individual:
Normal brain tissue is relatively radio-resistant. The tolerance dose with 5% severe complication rate in 5 years is referred to as the TD5,5. For brain with complications of radiation necrosis and infarction, the T D 5 1 5 is approximately 50 Gy. The radiation dose in this case was given to a relatively silent portion of the brain and, therefore, I would not expect any significant deterministic effects.
Briefly describe the current medical condition of the exposed individual:
The patient is a 64 year old female with a history of small cell lung cancer diagnosed in 2005. She subsequently developed a metastatic lesion to the right cerebellum and was prescribed 18 Gy gamma knife stereotactic radiosurgery to the nodule at the 50% isodose line. The patient currently also has metastatic disease to the liver. Her long-term prognosis is not favorable due to her tumor burden.
References
LF Fajardo L-G, M Berthrong, and RE Anderson Radiation Pathology. Oxford Press. 200 1
GH Fletcher. Textbook of Radiotherapy. 3rd edition. Lippincott, Williams & Wilkins. 1980.
FA Mettler Jr, and AC Upton. Medical Effects of Ionizing Radiation. Second Edition. Saunders. 1995.
Was individual or individual's physician informed of DOE Long-term Medical Study Program?
Yes
If yes, would the individual like to be included in tbe program?
No
Issued 11107 M. Jelich Gamma K n i i 3

COMPLETE FOR MEDICAL MISADMINISTRATION v o be completed by Medical Consultant)
1. Based on your review of the incident, do you agree with the licensee’s written report that was submitted to the NRC pursuant to 10 CFR 3533 in the following areas:
a. Why the event occurred - Yes.
b. Effect on the patient - Yes.
My independent dose estimates generally agree with those provided by the hospital.
c. Licensee’s immediate actions upon discovery - There was immediate reporting of the event to the NRC.
d. Improvements needed to prevent recurrence - Yes.
This is a human factors issue, correctable by education and improved procedures. The issue was also addressed through the hospital Radiation Safety Committee and by physician management in the Karmanos Cancer Center. A time-out protocol is also currently in development to allow medical staff to review all aspects of the medical case prior to gamma knife treatment.
For all fbture gamma knife cases, IeWright alignment of the MRI images will be inspected by the authorized medical physicist (AMP) by using the Leksel anterior face plate with fiducial markers visible in the MRI images. A Gamma Knife MRI protocol will also be written and posted in the MRI department and in the Gamma Knife suite. The protocol will clearly indicate the patient and scan orientation required for Gamma Knife planning and delivery, which are patient on table head first, with head first scanning protocol.
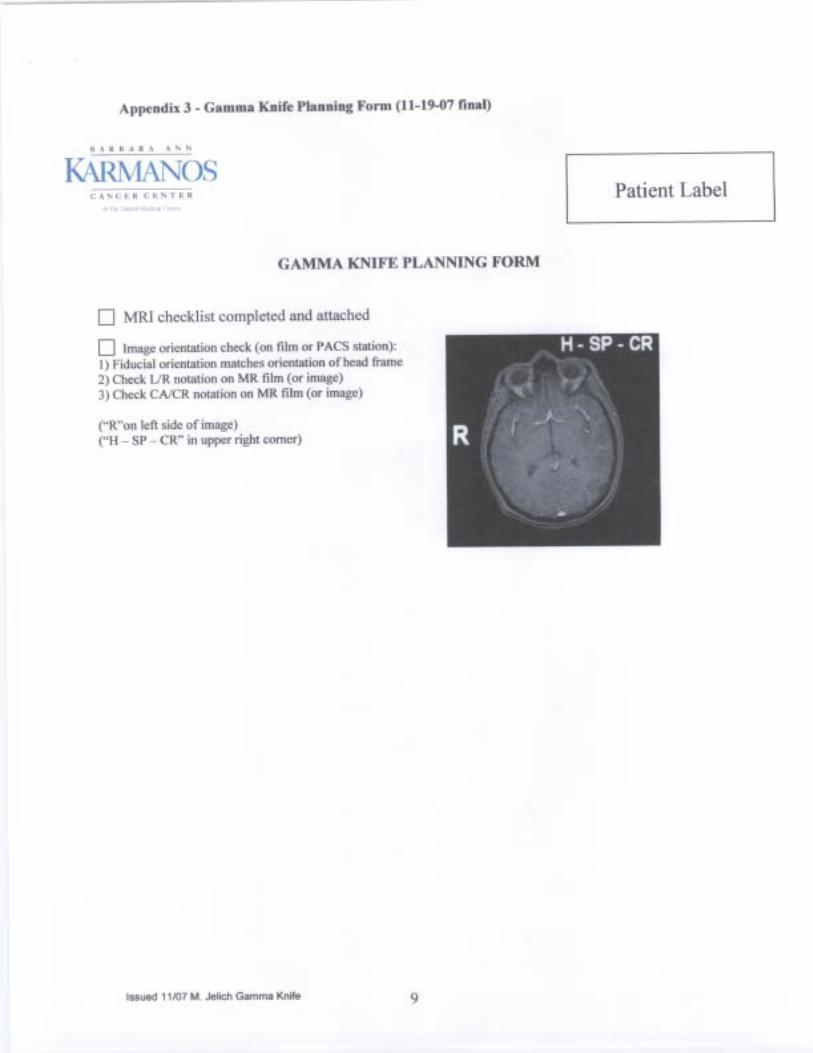
Appendix 2 illustrates the current pre-procedure gamma knife checklist, while appendix 3 presents the current gamma knife planning form. Appendix 4 presents the planned stereotactic imaging planning form. In this accident, prior to the therapy, the medical physicist noted that the stereotactic headset bubble readings did not match those in the pre- treatment planning form, he called the company representative and was told to proceed. This was quite unfortunate.
2. In areas where you do not agree with the licensee’s evaluation (report submitted under 10 CFR 3533, provide the basis for your opinion: N/A
3. Did the licensee notify the referring physician of the misadministration? Yes
Did the licensee noti@ the patient’s or the patient’s responsible relative o r guardian? Yes
If the patient or responsible relative o r guardian was not notified of the incident, did the licensee provide a reason for not providing notification consistent with 10 CFR 3533? NIA
Explain rationale for response.
Issued 11/07 M. J e l i Gamma Knife 4

4. Provide an opinion of the licensee’s plan for patient follow-up. If available.
The patients will be followed clinically by oncology physicians as indicated. I believe that the hospital system and, specifically, the oncology department, will institute an effective program to prevent a recurrence of this event. The information in the preliminary notification has also been reviewed with licensee management. Detailed checklists and policy statements are included in the appendices.
Issued 11107 M. Jelich Gamma Knife 5




0 Qualitative agreement of wire frame (from bubble measurements) with MR image
Largest measured deviation between wire frame contour and MR image surface:
Lesion (1): Name: Treatment
Lesion (2): Name: Treatment Site:
Lesion (3): Name: Treatment Site:
Lesion (4): Name: Treatment Site:
Lesion (5): Name: Treatment
Lesion (6): Name: Treatment Site:
Lesion (7): Name: Treatment Site:
Lesion (8): Name: Treatment
Lesion (9): Name: Treatment Site:
Lesion (10): Name: Treatment Site:
Planning Physicist: Physics Check:
0 Identify number and orientation of lesions (to be checked by neurosurgeon and radiation oncologist)
Neurosurgeon: Radiation Oncologist:
Comments:
10

Appendix 4 - Stereo Imaging Placement Form
Patient Label
Stereotactic Frame Placement and Neuroimaging Form - MENINGIOMA
I NEUROSURGEON:
DATE OF BIRTH:
RADIATION ONCOLOGIST:
1 TUMOR BOARD DATE:
GAMMA KNIFE DATE:
DATE OF LAST MRIICT:
NUMBER OF LESIONS: WHO
HAS FILMSKD:
LOCATION OF LESION(S) [PLEASE INDICATE RIGHTILEFT]:
2- I ’-

4- 5-
6-
OPTIMAL FRAME PLACEMENT [BASED ON LOCATION OF LESION(S)]:
1- 0 RIGHT 0 LEFT 0 NEUTRAL
2- OSUPERIOR 0 INFERIOR 0 N t U I KAL
3- OANTERIOR 0 POSTERIOR NEUTRAL
NEUROIMAGING PROTOCOL REQUIRED:
Comments:
Neurosurgeon (Date)
(Date) Neurosurgery RN (Date) GK Coordinator * Patient Label
12

Stereotactic Frame Placement and Neuroimaging Form - GLIOBLASTOMA
PATIENT NAME:
1 NEUROSURGEON:
DATE OF BIRTH:
RADIATION ONCOLOGIST:
TUMOR BOARD DATE:
GAMMA KNIFE DATE:
DATE OF LAST MRI/CT:
NUMBER OF LESIONS: WHO
HAS FILMS/CD:
LOCATION OF LESION(S) [PLEASE INDICATE RIGHT/LEFTJ:
2- I ’- L 3-
4- 5-
6-
OPTIMAL FRAME PLACEMENT [BASED ON LOCATION OF LESION(S)]:
L 13

1- 0 RIGHT
2- OSUPERIOR
LEFT 0 NEUTRAL
0 0 INFERIOR
NEUTRAL
3- OANTERIOR 0 POSTERIOR 0 NEUTRAL
NEUROIMAGING PROTOCOL REQUIRED:
Comments:
Neu row rgeon (Date)
(Date) Neurosurgery RN (Date) GK Coordinator
Patient Label r____ Stereotactic Frame Placement and Neuroimaging Form - LOW GRADE
GLIOMA
A 1

PATIENT NAME:
NEUROSURGEON:
DATE OF BIRTH:
RADIATION ONCOLOGIST:
TUMOR BOARD DATE:
GAMMA KNIFE DATE:
DATE OF LAST MRVCT:
I F* n F-
NUMBER OF LESIONS: WHO
HAS FILMSICD:
LOCATION OF LESION(S) [PLEASE INDICATE RIGHT/LEFT]:
2- I I- 5- 4-
6-
OPTIMAL FRAME PLACEMENT [BASED ON LOCATION OF LESION(S)]:
1- 0 RIGHT LEFT 0 NEUTRAL
2- OSUPERIOR 0 INFERIOR 0 NEUTRAL
15

3- OANTERIOR c] POSTERIOR [7 NEUTRAL
NEUROIMAGING PROTOCOL REQUIRED:
Comments:
Neurosurgeon (Date)
(Date) Neurosurgery RN (Date) GK Coordinator
16

Y Patient Label
Stereotactic Frame Placement and Neuroimaging Form - BRAIN METASTASES
PATIENT NAME:
NEUROSURGEON:
DATE OF BIRTH:
RADIATION ONCOLOGIST:
GAMMA KNIFE DATE:
DATE OF LAST MRI/CT:
FW n c n ncdc u -
NUMBER OF LESIONS: WHO
HAS FILMSICD:
LOCATION OF LESION(S) [PLEASE INDICATE RIGHTILEFT]:
1- 2-
4- 5-
6-
17

OPTIMAL FRAME PLACEMENT [BASED ON LOCATION OF LESION(S)]:
1- RIGHT 0 LEFT 0 NEUTRAL
2- 0 SUPERIOR 0 INFERIOR 0
3- OANTERIOR 0 POSTERIOR 0 NEUTRAL
NEUROIMAGING PROTOCOL REQUIRED:
Comments:
Neurosurgeon (Date)
(Date) Neurosurgery RN (Date) GK Coordinator
18

Patient Label v Stereotactic Frame Placement and Neuroimaging Form - ACOUTIC NEUROMA
PATIENT NAME:
NEUROSURGEON:
DATE OF BIRTH:
RAD lATl0 N ONCOLOGIST:
GAMMA KNIFE DATE:
DATE OF LAST MRI/CT:
F- nFw! n c n n c l s
NUMBER OF LESIONS: WHO
HAS FILMS/CD:
LOCATION OF LESION(S) [PLEASE INDICATE RIGHTILEFT]:
2- I '- I
J'
4- 5-
6-
19
OPTIMAL FRAME PLACEMENT [BASED ON LOCATION OF LESION(S)]:
1- 0 RIGHT LEFT c] NEUTRAL
2- OSUPERIOR 0 INFERIOR 0 NEUTRAL
3- UANTERlOR 0 POSTERIOR 0 NEUTRAL
NEUROIMAGING PROTOCOL REQUIRED:
Comments:
Neurosurgeon (Date)
(Date) Neurosurgery RN (Date) GK Coordinator
. A " . * . * A N N
KARMANOS Patient Label
20

Stereotactic Frame Placement and Neuroimaging Form - PITUITARY
ADENOMA
OPTIMAL FRAME PLACEMENT [BASED ON LOCATION OF LESlON(S)]:
21 -
~~ ~
PATIENT NAME:
NEUROSURGEON:
DATE OF BIRTH:
RADIATION ONCOLOGIST:
I TUMOR BOARD DATE:
GAMMA KNIFE DATE:
DATE OF LAST MRVCT:
n F I U ~ n rrn n CIS
NUMBER OF LESIONS: WHO
HAS FILMSICD:
LOCATION OF LESION(S) [PLEASE INDICATE RIGHT/LEFTJ:
1- 2-
4- 5-
6-

I- 0 RIGHT
2- OSUPERIOR
NEUTRAL
3- OANTERIOR
0 LEFT 0 NEUTRAL
INFERIOR 0
0 POSTERIOR 0 NEUTRAL
NEUROIMAGING PROTOCOL REQUIRED:
Comments:
Neurosurgeon (Date)
(Date) Neurosurgery RN (Date) GK Coordinator
Patient Label
Stereotactic Frame Placement and Neuroimaging Form - TRIGEMINAL
NEURALGIA

NAME: PATIENT
DATE OF
NEUROSURGEON:
BIRTH:
RADIATION ONCOLOGIST:
GAMMA KNIFE DATE:
DATE OF LAST MRVCT:
CTA- F- ! F w E c n E m s
NUMBER OF LESIONS: WHO
HAS FILMSKD:
LOCATION OF LESION(S) [PLEASE INDICATE RIGHT/LEFT]:
1- 2-
J-
4- 5-
6-
OPTIMAL FRAME PLACEMENT [BASED ON LOCATION OF LESION(S)]:
I- [7 RIGHT [7 LEFT NEUTRAL
2- OSUPERIOR 0 INFERIOR cl
23

3- OANTERIOR 0 POSTERIOR 0 NEUTRAL
NEUROIMAGING PROTOCOL REQUIRED:
Comments:
Neurosurgeon (Date)
(Date) Neurosurgery RN (Date) GK Coordinator
C A N C E R I N S T I T U T E
Patient Label
Stereotactic Frame Placement and Neuroimaging Form - CAVERNOUS
ANGIOMA
PATIENT NAME:
NEUROSURGEON:
24

DATE OF BIRTH:
RADIATION ONCOLOGIST:
GAMMA KNIFE DATE:
DATE OF LAST MRVCT:
NUMBER OF LESIONS: WHO
HAS FILMS/CD:
LOCATION OF LESION(S) [PLEASE INDICATE RIGHTILEFT]:
2- I I- I *
3-
4- 5-
6-
1 OPTIMAL FRAME PLACEMENT [BASED ON LOCATION OF LESlON(S)]:
1- 0 RIGHT 0 LEFT 0 NEUTRAL
2- OSUPERIOR 0 INFERIOR 0 NEUTRAL
3- UANTERIOR 0 POSTERIOR 0 NEUTRAL
25

NEUROIMAGING PROTOCOL REQUIRED:
Comments:
Neurosurgeon (Date)
~~
(Date) Neurosurgery RN (Date) GK Coordinator
26
Patient Label
Stereotactic Frame Placement and Neuroimaging Form - AVM
PATIENT NAME:
NEUROSURGEON:
DATE OF BIRTH:
RADIATION ONCOLOGIST:
GAMMA KNIFE DATE:
DATE OF LAST MRI/CT:
n FIUQ n cn n CIS
NUMBER OF LESIONS: WHO
HAS FILMSKD:
LOCATION OF LESION(S) [PLEASE INDICATE RIGHT/LEFTI:
1- 2-
I rl J-
4- 5-
27

OPTIMAL FRAME PLACEMENT [BASED ON LOCATION OF LESION(S)]:
1- RIGHT 0 LEFT 0 NEUTRAL
2- USUPERIOR 0 INFERIOR 0
3- OANTERIOR 0 POSTERIOR 0 NEUTRAL
NEUROIMAGING PROTOCOL REQUIRED:
Comments:
Neurosurgeon (Date)
(Date) Neurosurgery RN (Date) GK Coordinator
28





























