Embed Size (px)
Citation preview
Medical Coding and Billing
Governance
Casper Venter HealthMan Director

Medical Coding in South Africa
Current Coding Structures
Dilemma
• Lack of an Authoritative Source Reference for new codes & queries
– Code Manipulations and billing malpractice exist and on the increase
– Certain procedures in the past were described by one or two codes with a few additional codes for the “complicated case”. Now routinely being used and more codes added.
• Guidelines established are not freely available RPL does not exist
• Unilateral decision making process by Schemes and Providers
– Lack of transparency
– Not all providers support the structure in place
• Determination of RVU values
– Lacks transparency and outdated
• Review of existing RVU values- Top 300 review
• New technology/techniques
– Use of existing codes and adding others to make up fee
– Unnecessary motivations required
– No guidance
Agenda for Coding Governance
1. Statistical Overview
2. General Coding Governance
3. American Medical Association Processes for Guidance
4. South African Classification of Healthcare Interventions (“SACHI”) as a unique RSA Solution

Statistical Overview
• Let’s look at some of the statistics that generate medical
services invoices…
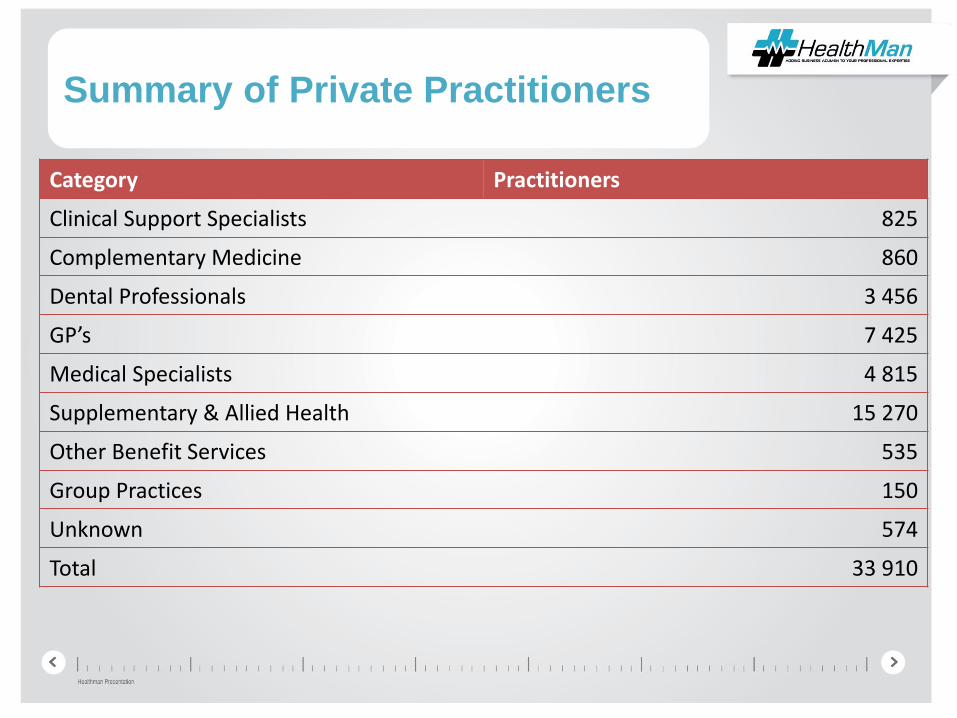
Summary of Private Practitioners
Category Practitioners
Clinical Support Specialists 825
Complementary Medicine 860
Dental Professionals 3 456
GP’s 7 425
Medical Specialists 4 815
Supplementary & Allied Health 15 270
Other Benefit Services 535
Group Practices 150
Unknown 574
Total 33 910
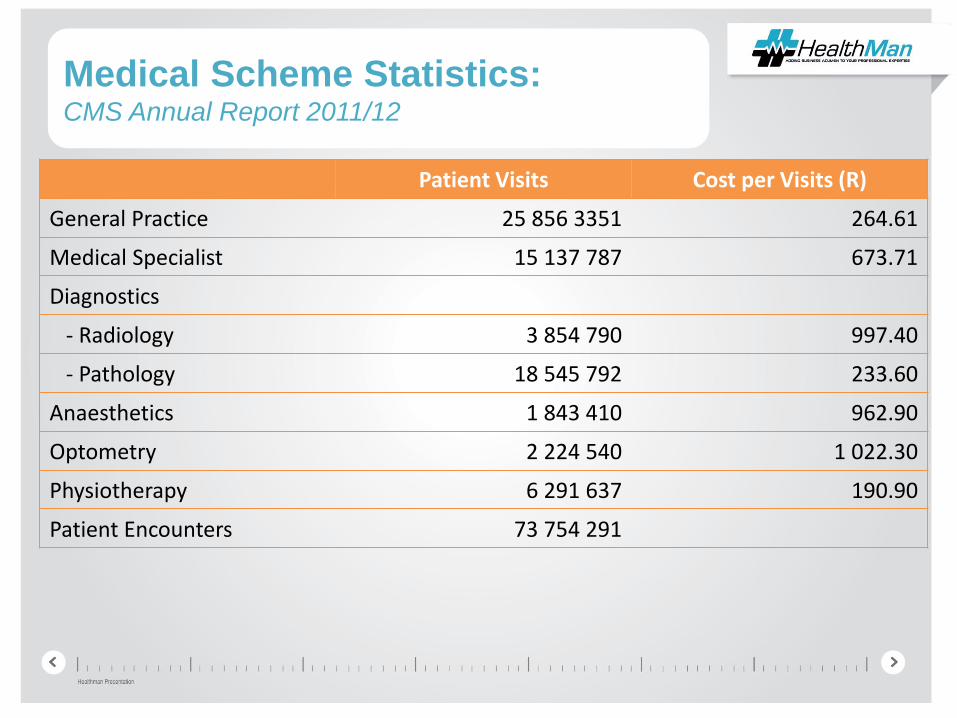
Medical Scheme Statistics: CMS Annual Report 2011/12
Patient Visits Cost per Visits (R)
General Practice 25 856 3351 264.61
Medical Specialist 15 137 787 673.71
Diagnostics
- Radiology 3 854 790 997.40
- Pathology 18 545 792 233.60
Anaesthetics 1 843 410 962.90
Optometry 2 224 540 1 022.30
Physiotherapy 6 291 637 190.90
Patient Encounters 73 754 291
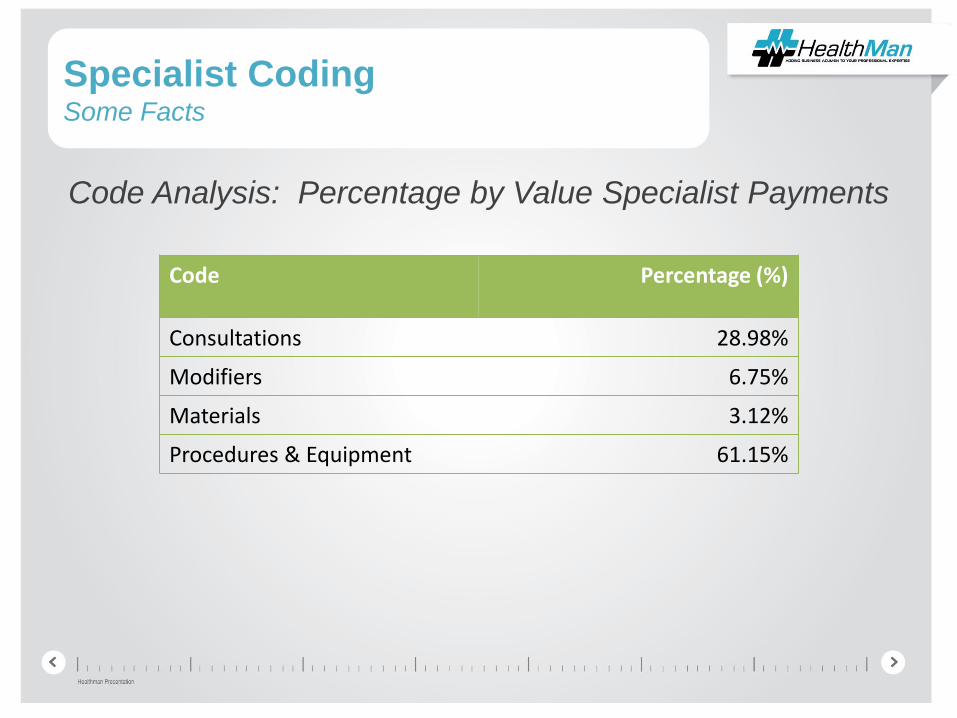
Specialist CodingSome Facts
Code Analysis: Percentage by Value Specialist Payments
Code Percentage (%)
Consultations 28.98%
Modifiers 6.75%
Materials 3.12%
Procedures & Equipment 61.15%
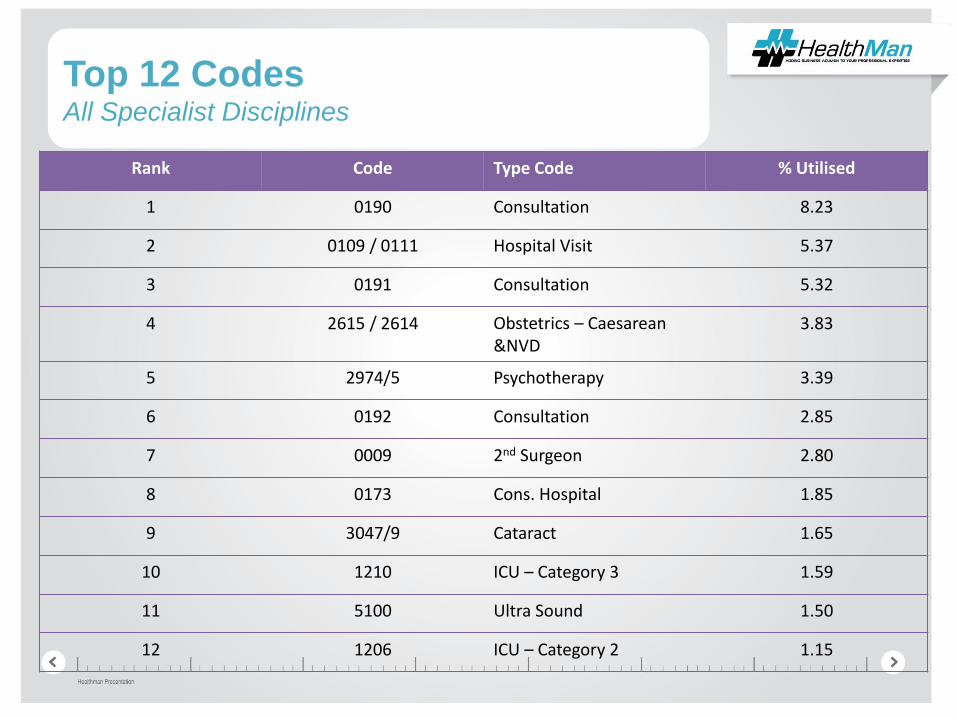
Top 12 CodesAll Specialist Disciplines
Rank Code Type Code % Utilised
1 0190 Consultation 8.23
2 0109 / 0111 Hospital Visit 5.37
3 0191 Consultation 5.32
4 2615 / 2614 Obstetrics – Caesarean &NVD
3.83
5 2974/5 Psychotherapy 3.39
6 0192 Consultation 2.85
7 0009 2nd Surgeon 2.80
8 0173 Cons. Hospital 1.85
9 3047/9 Cataract 1.65
10 1210 ICU – Category 3 1.59
11 5100 Ultra Sound 1.50
12 1206 ICU – Category 2 1.15
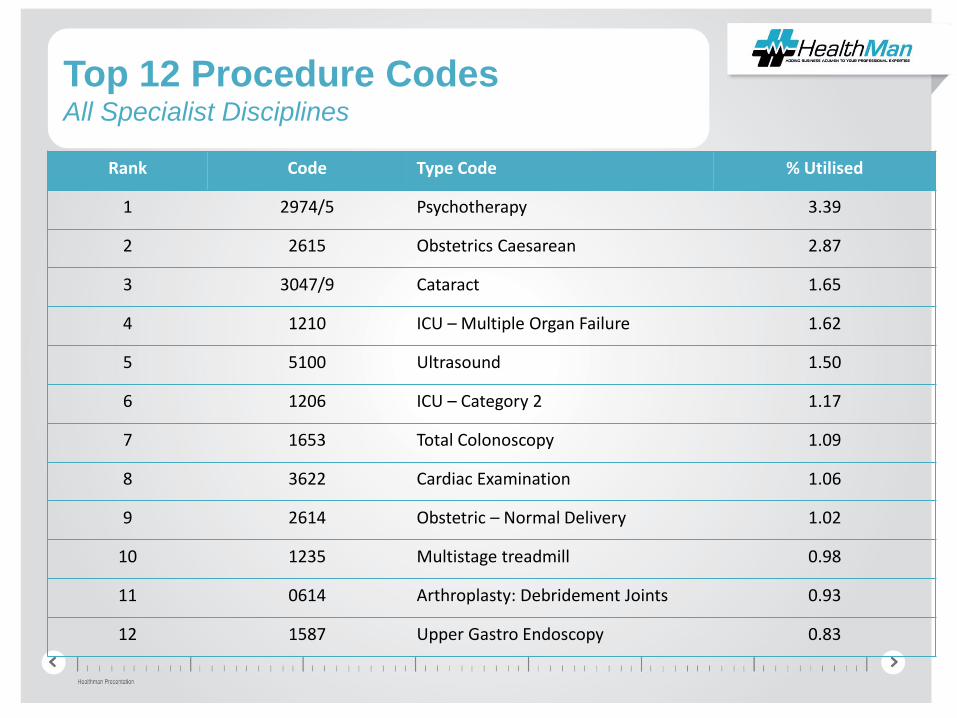
Top 12 Procedure CodesAll Specialist Disciplines
Rank Code Type Code % Utilised
1 2974/5 Psychotherapy 3.39
2 2615 Obstetrics Caesarean 2.87
3 3047/9 Cataract 1.65
4 1210 ICU – Multiple Organ Failure 1.62
5 5100 Ultrasound 1.50
6 1206 ICU – Category 2 1.17
7 1653 Total Colonoscopy 1.09
8 3622 Cardiac Examination 1.06
9 2614 Obstetric – Normal Delivery 1.02
10 1235 Multistage treadmill 0.98
11 0614 Arthroplasty: Debridement Joints 0.93
12 1587 Upper Gastro Endoscopy 0.83
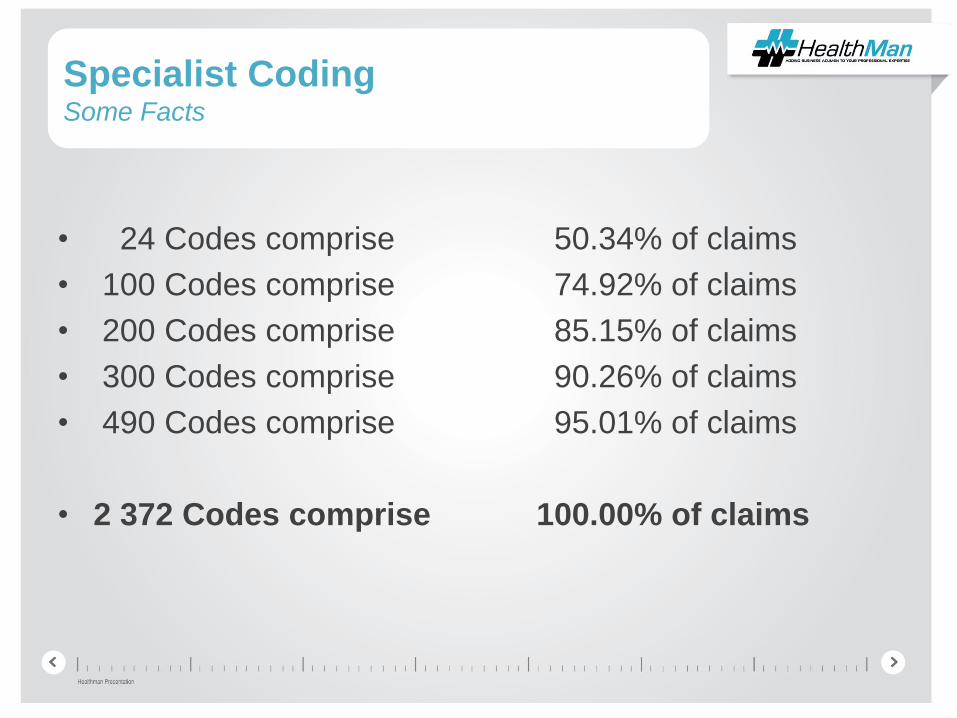
Specialist CodingSome Facts
• 24 Codes comprise 50.34% of claims
• 100 Codes comprise 74.92% of claims
• 200 Codes comprise 85.15% of claims
• 300 Codes comprise 90.26% of claims
• 490 Codes comprise 95.01% of claims
• 2 372 Codes comprise 100.00% of claims
General Coding Governance
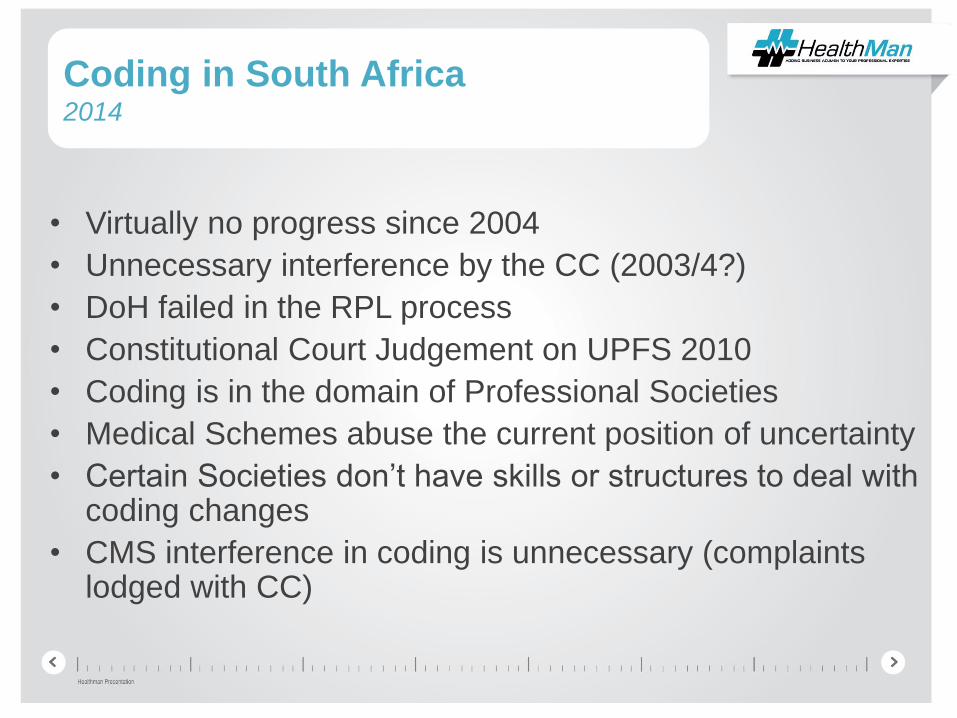
Coding in South Africa 2014
• Virtually no progress since 2004
• Unnecessary interference by the CC (2003/4?)
• DoH failed in the RPL process
• Constitutional Court Judgement on UPFS 2010
• Coding is in the domain of Professional Societies
• Medical Schemes abuse the current position of uncertainty
• Certain Societies don’t have skills or structures to deal with coding changes
• CMS interference in coding is unnecessary (complaints lodged with CC)
Objective of a Comprehensive
Coding System
To provide a uniform language that accurately describes
medical, surgical and diagnostic services, and thereby
serves as an effective means for reliable national private
and public sector communication amongst all healthcare
professionals, patients, funders and administrators, and
other stakeholders – SACHI
What is required in South Africa?
• To establish an independent multi-stakeholder NPO
entity that will manage governance processes.
• It will not own codes, but will assist with and manage
processes related to implementation and management of
coding systems.
What is required in South Africa?
• Seek guidance from International experience – American Medical Association (“AMA”)
• Establish a Corporate Governance Structure within a Company registered ito Companies Act 2008
• Not-for-profit organisation
• South African Classification for HealthCare Interventions “SACHI”
AMA Processes
1. Developing Descriptors
2. Relative Value Scale Update Process
3. Practice Expense Review
4. Review and Introduce new Technology
Coding Advisory Committee
• Advises on procedure coding and specialist nomenclature;
• Documents appropriateness of medical and surgical procedures
being considered for inclusion in Coding Manual;
• Suggests revisions to Coding. Committee meets 2-3 times p.ato discuss items of mutual concern and to keep abreast of current
issues in coding and nomenclature;
• Assists in the review and further development of relevant coding
issues and in the preparation of technical education material and
articles pertaining to Coding; and
• Promotes and educates its membership on the use and benefits
of accurate Coding.
Application and Adjudication
• Editorial Panel meets 4 times a year to discuss– New and emerging technologies
– Difficulties with procedures and services (esp. relating to codes)
• Interested parties may submit applications for changes to CPT.
• Either applicants advised of panel’s recommendations if issue has previously been dealt with; or application is referred to the Advisory Committee if a new issue or offering significant new information
• If no Advisory Panel support, can be withdrawn, otherwise becomes an Agenda item for Editorial Panel discussion at next meeting.
Editorial Panel Meetings
• Schedule allows 3 months for preparation and processing before
issues are ready for Panel review.
• Agenda material prepared for Panel at least 30 days in advance
(incl. original application, commentary by Advisory Committee
members, ballot for decision)
• 4 possible outcomes:– Addition or revision (will reflect in forthcoming volume of Coding Manual),
– referral to workgroup for further study,
– postponement to a future meeting; or
– rejection.
“A multi-step process naturally means that deadlines are very
important.”
Category 1 Code Status
• Category 1 codes (5-digit code & descriptor
nomenclature) provide a detailed description of a
medical procedure or service
• Panel requires evidence that the service/procedure:
– has FDA or EUapproval (for devices and drugs)
– is distinct and performed by many practitioners nationwide
– [’s] clinical efficacy is well established and documented in U.S. peer review literature
– doesn’t have an existing code, nor fragments one that does
– doesn’t report extraordinary circumstances related to an existing code
AMA Governance Processes
• Relative Value Scale Update Process
“Suggestions from physicians, medical specialty societies,
state medical associations, and those who deal regularly with
health care information are the only way to ensure that
CPT reflects current practice.”
Resource-Based Relative Value
Scale and Update Committee
• AMA advocates for fair and accurate valuation for all physician
services, hence Resource-Based Relative Value Scale (“RBRVS”)
• CPT has 8,000 defined procedure codes, with relative values in the
RBRVS corresponding to the procedure definitions
• AMA/Specialty Society Relative Value Scale Update Committee
(“RUC”) ensures physician services across all specialities are well-
represented
– Acts as an expert panel to make annual recommendations re. new and revised services to CMS
– Performs a broad review of the RBRVS every 5 years
Five-Year Reviews of RVUs
• Updating and maintaining the RVU is a clinical & scientific activitythat must remain in the hands of the medical profession
• Each review is an opportunity to improve the accuracy of the physician work component (1 of 3) of the RVUs
• physician work (52%),
• practice expense (44%), and
• malpractice expense (4%)
• All of the codes on the Scheme Payment Schedules must be open for public comment
• In addition, the Relativity Assessment Workgroup (5-Year Review Identification Workgroup) identifies potentially misvalued services using objective mechanisms for re-evaluation during the upcoming Review 300 Services as a Benchmark.

South African Classification of Healthcare
Interventions (“SACHI”)
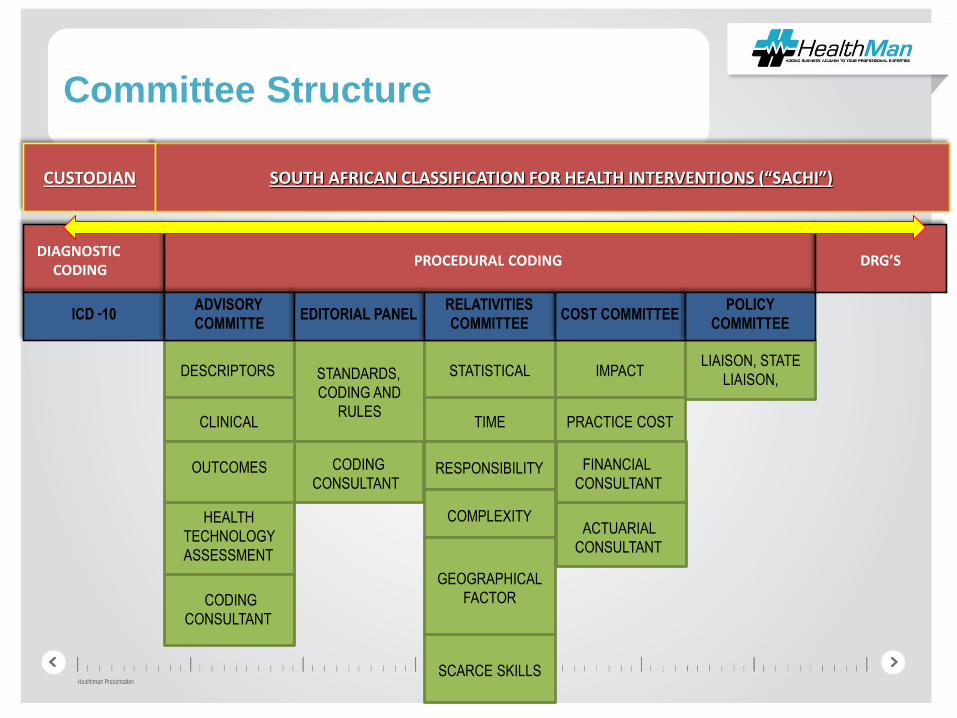
Committee Structure
DIAGNOSTIC CODING
PROCEDURAL CODING DRG’S
ICD -10ADVISORY
COMMITTE EDITORIAL PANEL
RELATIVITIES
COMMITTEE COST COMMITTEE
POLICY
COMMITTEE
DESCRIPTORS STANDARDS,
CODING AND
RULES
STATISTICAL IMPACTLIAISON, STATE
LIAISON,
CLINICAL TIME PRACTICE COST
OUTCOMES RESPONSIBILITY
COMPLEXITYHEALTH
TECHNOLOGY
ASSESSMENT
GEOGRAPHICAL
FACTOR
SCARCE SKILLS
SOUTH AFRICAN CLASSIFICATION FOR HEALTH INTERVENTIONS (“SACHI”)CUSTODIAN
CODING
CONSULTANT
CODING
CONSULTANT
FINANCIAL
CONSULTANT
ACTUARIAL
CONSULTANT
The Way Forward
• Maintenance of current coding structures lacks a governance structure
• Involve all Professions and Stakeholders
• Set up a Section 21 Company – SACHI– Take control of the governance process
– Maintain custody of coding structures within professional societies
• Urgency!





























![BILLING AND CODING - newriver.edu€¦ · BILLING AND CODING MEDICAL INSURANCE BILLING AND CODING CERTIFICATE OF APPLIED SCIENCE (CAS) [PROGRAM HOURS: 30] Train to meet the demand](https://img.pdfslide.us/doc/110x75/600601335678f93023309bea/billing-and-coding-billing-and-coding-medical-insurance-billing-and-coding-certificate.jpg)