Embed Size (px)
Citation preview

AmericansForSafeAccess.org
Americans for Safe Access 1624 U Street, NW, Suite 200 Washington, DC 20009 Tel: 202.857.4272 AmericansForSafeAccess.org
MED
ICA
L CA
NN
AB
IS A
S A
TOO
L TO C
OM
BAT PA
IN
MEDICAL CANNABIS AS A TOOL TO COMBAT PAIN AND THE OPIOID CRISIS
A BLUEPRINT FOR STATE POLICY2017 Report prepared by Americans for Safe Access

MEDICAL CANNABIS AS A TOOL TO COMBAT PAIN AND THE OPIOID CRISIS A BLUEPRINT FOR STATE POLICY
2017 Report prepared by Americans for Safe Access

2 3
TABLE OF CONTENTS
INTRODUCTION. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
KEY FACTS AND TALKING POINTS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8CASE STUDY: Michigan. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10
OVERVIEW OF CURRENT STATE LAWS: HOW DOES YOUR STATE MEASURE UP?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .36
“ACT NOW” DRAFT EMERGENCY LEGISLATION . . . . . . . . . . . . . . . . . . . . .38
REGULATORY ACTIONS.................................................58
RECOMMENDATIONS........................................................62
SUGGESTED REFERENCES....................................64

4 5
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS
RESEARCH SHOWS
THAT OPIOID DEATHS
HAVE DECREASED IN
STATES WITH MEDICAL
CANNABIS LAWS BY
AS MUCH AS 25%
AND HAS FOUND A
23% REDUCTION IN
HOSPITALIZATIONS
RELATED TO OPIOID
DEPENDENCE OR ABUSE.
Medical cannabis can also reduce healthcare costs. In a study published in the Journal of Health Affairs National, overall reductions in Medicare program and enrollee spending when states implemented medical marijuana laws were estimated to be $165.2 million per year in 2013.8 The availability of medical marijuana has a significant effect on prescribing patterns and spending in Medicare Part D.9 These same researchers, from their results of a similar study, estimated that if all states had enacted a medical cannabis law in 2014, total savings for fee-for-service Medicaid could have been $1.01 billion.10
Using medical cannabis to treat chronic pain is an approach that is supported by research and medical professionals, and has demonstrated positive public health outcomes. Thirty states in the US have passed medical cannabis laws and another sixteen have passed more limited laws. Medical cannabis programs on average are serving 2% of the population despite a potential addressable market of 1/3 of the population that are living with chronic pain.
Americans for Safe Access and our advisors have examined current medical cannabis programs and have identified many barriers for medical professionals, patients, and their caregivers that prevents them from utilizing medical cannabis as a tool to combat pain and opioid use disorder. The following report takes a public health approach to defining enrollment issues and offers a blueprint for legislative and regulatory bodies to resolve these issues. We have concluded that improvements in state medical cannabis legislation and regulations could increase program enrollment and save lives.
8 Vyas, Marianne Beare et al. The use of cannabis in response to the opioid crisis: A review of the literature. Nursing Outlook. September, 2017.
9 Bradford, AC, Bradford, DW. Medical Marijuana Laws Reduce Prescription Medication Use In Medicare Part D. Health Affairs. 2016; 35(7).
10 Bradford, AC, Bradford, DW. Medical Marijuana Laws May Be Associated With A Decline In The Number Of Prescriptions For Medicaid Enrollees. Health Affairs. 2017; 36(5).
INTRODUCTIONAccording to the Institute of Medicine1 (IOM), chronic pain affects approximately one–third of the US adult population with an economic cost of at least $560-635 billion annually2. States across the US are also dealing with an opioid crisis that is claiming between 91-175 American lives a day. State medical cannabis programs have the potential to play a key role in combating the pain epidemic and the opioid crisis if implemented correctly.
Research shows that cannabis is effective in treating chronic pain. In January, the National Academies of Sciences, Engineering, and Medicine released “The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research (2017)”3 which compiled research from over 10,000 studies on cannabis and its components. The report states that “in adults with chronic pain, patients who were treated with cannabis or cannabinoids are more likely to experience a clinically significant reduction in pain symptoms” and “there is substantial evidence that cannabis is an effective treatment for chronic pain in adults.”4
Research shows that opioid deaths have decreased in states with medical cannabis laws by as much as 25%5 and has found a 23% reduction in hospitalizations related to opioid dependence or abuse.6 According to the Center for Disease Control (CDC), there were an estimated 64,000 opioid overdose deaths in 2016.7 Nearly half of all opioid overdose deaths involve a prescription opioid.
1 Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington (DC): National Academies Press (US); 2011. Available from: https://www.ncbi.nlm.nih.gov/books/NBK91497/ doi: 10.17226/131722 Gaskin DJ, Richard P. The Economic Costs of Pain in the United States. In: Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington (DC): National Academies Press (US); 2011. 3 National Academies of Sciences, Engineering, and Medicine. 2017. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington, DC: The National Academies Press. https://doi.org/10.17226/24625.4 National Academies of Sciences, Engineering, Medicine, Nearly 100 Conclusions on the Health Effects of Marijuana and Cannabis-Derived Products Presented in New Report, Press Release,(Jan. 12, 2017), http://www8.nationalacademies.org/onpinews/newsitem.aspx?RecordID=246255 Bachhuber MA, Saloner B, Cunningham CO, Barry CL. Medical Cannabis Laws and Opioid Analgesic Overdose Mortality in the United States, 1999-2010. JAMA Intern Med. 2014;174(10):1668–1673. doi:10.1001/jamainternmed.2014.40056 Shi, Yuyan. Medical marijuana policies and hospitalizations related to marijuana and opioid pain reliever. Drug & Alcohol Dependence. February 2017 (173): 144 - 150.
7 CDC. Wide-ranging online data for epidemiologic research (WONDER). Atlanta, GA: CDC, National Center for Health Statistics; 2016. Available at http://wonder.cdc.gov.

6 7
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS
4. EM ILITATIBUS EAQUE OCCUMEcatempo riasse reptus min nos dem est lamet quid que porit libus. Riberna turion nat. Od ut quis dis velit et ad que voluptis reperat emporeperem ipsam est etur, quia nonsectaspid molorenda quatis sequissunt idi arionseque asit odias se nimporu pienis mollab ipsanihillab id magnis enducipsapis alit ipietur? Quiatio occus non perovid magnis am faccus magnis con coreptatem andem lam eumquis eossinc tiatur? Em et hita siminis velessunt, est es re nobit eost volesti onsendes digenducimo doluptati dolorum harcia nusandis dolessus sam rerovident hitia m quae et et experibus comnimusam alignatquiam int dolore nem volento blandicabor repudae sint verio optatem porumque parchillecae parum reped ut ipsa nihici aspiciati nitium liti aut et porit, ommos moluptatior autem velitatianis im et post illaut apedion comni arum dersperum dolupta musdam que quodio. Ut et odis ea nus.
Derorepel est re, cum aut laut vel is autem cuptat et earibus, am, et quis ea conecul laboribus, offic tempor sed quo maxime prepuda essint ut eic tem hicatur, quat laccum audamusa cor aut est, corem gentureptur simpore corunt re core non non re prae resendero cus ate porro cor sunt, dam, eicto temperum faccusam idesseq uatures aceriaeperum faccus aut et ut officimus eiunt pa qui oditaque quidendus dolut minum qui vent eicit lab intus.
Em ilitatibus eaque occum ut dolor rehent quamentem ad qui totatur recullu ptibus voluptae seque volore rectin pliquid quis mosam utes et arit, ommollores conse essitio nsequae aut ut ea que quam vollupt aerorep ediscipsant volupti nemquia adi quis doluptis esectuuae excera dollicatusam dit excero denture pernam, solestibus nostisciam facee pelest qui raectat ioresti omnihit preium il ipid modiore volupti asitat occum quatiissam, sam, officti as maximusam, a sim ad ut atenihilici doluptur? dolupta nonse a doluptiat.
CHAPTER 1 KEY FACTS AND TALKING POINTS
Even the states with legal medical cannabis, patients often can’t gain access to the programs. The model legislation provided by Americans for Safe Access and detailed in this report would provide wider access to medical cannabis for constituents in your state.
• Legislative and regulatory improvements to medical cannabis programs could decrease opioid overdose deaths by even more than 25 percent.
• Over 80 percent of physicians in the U.S. are over 40 years old and, therefore, most likely have not studied the Endocannabinoid System while in medical school.
• This legislation will encourage doctors and medical professionals to take Continuing Medical Education courses about medical cannabis that are accredited by organizations such as the American Medical Association so doctors can better prescribe the right medication for their patients.
• More residents in your state will gain access to safer treatment for chronic pain, lowering rates of opioid addiction, overdose deaths, and the cost of medical care.
V KEY FACTS AND TALKING POINTS
A third of the U.S. population suffers from chronic pain, but medical care has too long relied on dangerous opioids as the solution.
• We now face a devastating opioid crisis that kills nearly 100 Americans per day.
• Nearly 50 percent of all opioid overdose deaths involve a prescription opioid.
Medical cannabis is a proven and effective alternative to opioids for addressing chronic pain, and also reduces state healthcare costs.
• Sixty-four percent of patients using medical marijuana to control chronic pain reported a reduction in their use of opioids, and opioid deaths have decreased in states with medical cannabis laws by as much as 25 percent.
• Medical cannabis legislation can reduce opioid addiction related hospitalizations by 23 percent, saving the state from the hefty price tag of $1,878 per patient per day.
• Legal medical cannabis programs serve just 2 percent of state populations on average, but 93 percent of chronic pain patients would be more likely to choose cannabis as a treatment if it were more readily available.
• The National Academies of Sciences, Engineering, and Medicine reports that in adults with chronic pain, patients treated with cannabis or cannabinoids are more likely to experience a clinically significant reduction in pain, and researchers have never documented a lethal overdose of cannabis.
KEY FACTS AND TALKING POINTS
Chapter 1 1
2
3

8 9
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS
4. EM ILITATIBUS EAQUE OCCUMEcatempo riasse reptus min nos dem est lamet quid que porit libus. Riberna turion nat. Od ut quis dis velit et ad que voluptis reperat emporeperem ipsam est etur, quia nonsectaspid molorenda quatis sequissunt idi arionseque asit odias se nimporu pienis mollab ipsanihillab id magnis enducipsapis alit ipietur? Quiatio occus non perovid magnis am faccus magnis con coreptatem andem lam eumquis eossinc tiatur? Em et hita siminis velessunt, est es re nobit eost volesti onsendes digenducimo doluptati dolorum harcia nusandis dolessus sam rerovident hitia m quae et et experibus comnimusam alignatquiam int dolore nem volento blandicabor repudae sint verio optatem porumque parchillecae parum reped ut ipsa nihici aspiciati nitium liti aut et porit, ommos moluptatior autem velitatianis im et post illaut apedion comni arum dersperum dolupta musdam que quodio. Ut et odis ea nus.
Derorepel est re, cum aut laut vel is autem cuptat et earibus, am, et quis ea conecul laboribus, offic tempor sed quo maxime prepuda essint ut eic tem hicatur, quat laccum audamusa cor aut est, corem gentureptur simpore corunt re core non non re prae resendero cus ate porro cor sunt, dam, eicto temperum faccusam idesseq uatures aceriaeperum faccus aut et ut officimus eiunt pa qui oditaque quidendus dolut minum qui vent eicit lab intus.
Em ilitatibus eaque occum ut dolor rehent quamentem ad qui totatur recullu ptibus voluptae seque volore rectin pliquid quis mosam utes et arit, ommollores conse essitio nsequae aut ut ea que quam vollupt aerorep ediscipsant volupti nemquia adi quis doluptis esectuuae excera dollicatusam dit excero denture pernam, solestibus nostisciam facee pelest qui raectat ioresti omnihit preium il ipid modiore volupti asitat occum quatiissam, sam, officti as maximusam, a sim ad ut atenihilici doluptur? dolupta nonse a doluptiat.
Making Medical Cannabis an Option for Pain and Opioid Use Disorder
CHAPTER 2 MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
Chapter 2 Forty-six states, the District of Columbia, Guam, and Puerto Rico all have passed some kind of medical cannabis legislation.
However, the passage of these laws does not ensure that medical cannabis is an option for everyone in that state or territory.
In fact, millions of people living with chronic pain and opioid use disorder are not eligible to participate in their medical cannabis programs due to the federal-state legal conflict, inadequacies in state laws, and lack of medical professional and patient education.

10 11
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS CHAPTER 2 MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
Michigan accepted patients into the medical cannabis program in 2009. However, to date millions of patients in Michigan are not able to participate in the program due to several barriers created by legislative and regulatory language. In some cases, these barriers are the result of an oversight but more often they exist because the programs were not created to ensure enrollment. First, let’s examine the landscape with regards to how Michigan is currently addressing the opioid crisis in terms of medical cannabis. Michigan lost 2,126 individuals to opioid overdoses in the last year. If we consider the research which supports an up to 25% decrease in medical cannabis states, an additional 531 individuals could have been victims if it were not for the state’s medical cannabis program.
BARRIER PEOPLE AFFECTED
NOTES
Living in Poverty 1,529,645 Cannot afford medicine
Serving Probation 55,000 Unable to obtain card
Living in Hospice 33,000 Policy prohibits medical cannabis
Residing in Assisted Living Establishment 45,000 Policy prohibits medical cannabis
Patient in Treatment Center 63,578 Policy prohibits medical cannabis
Federal Employee 52,100 Federal policy prohibits federal employees from medical cannabis
Veterans 672,215Due to federal policy, veterans are subject to loss of all VA benefits if found to be using medical cannabis
Elderly or Homebound 91,100 Unable to get to required doctor appointments and/or pick up medical cannabis
Employees Drug Tested 2,645,769 Using medical cannabis would lead to positive test and potential loss of job
On Organ Transplant List 3,342 Policy prohibits cannabis use to be considered for transplant list
TOTAL 5,190,759 Not eligible for medical cannabis program (some of these populations may overlap)
DATA SOURCES FOR THIS CHART ARE AVAILABLE ON PAGE 68
CASE STUDY: MICHIGAN
In the following chart, we can see that the number of lives saved could be significantly higher were Michigan to remove the barriers to access of the patient populations listed.
According to the CDC, approximately 1/3 of Americans are living with chronic pain. Therefore, we can estimate that within Michigan’s population of 9,883,640, approximately 2,569,720 suffer daily from chronic pain.
The state’s federal employees and most Veterans (totaling 724,315) will continue to be excluded until federal laws change. However, if Michigan were to eliminate the other barriers through legislative and regulatory changes to their medical cannabis program, it would be able to potentially serve an additional 4,466,434 patients in their program and further reduce the number of opioid overdose deaths in the state.

A NO State has operational medical cannabis law
YES
State law includes pain and opioid use disorder as
qualifying conditions
• Patient moves to state with MC law
• Patient utilizes illicit market
• Pass new laws allowing for use
B NO YES
* Patient with existing injury or Illness
Determining if Cannabis is an Option for Pain TreatmentPatient with New Injury or Illness
• Patient moves to state with MC law
• Patient utilizes illicit market
• Add pain as qualifying condition/allow doctor to recommend for any condition
C NO
• Department of Health & Board of Medicine can notify medical professionals about the program and CME courses
• Department of Health can notify patient advocacy organizations about the program and offer patient education about MC
NO The patient can access MC in reasonable time frame
YES
• Patient moves to state with MC Law
• Patient utilizes illicit market
• Pass law or regulations that decrease waiting periods for medication
NO YESThe patient’s treatment contract excludes THC testing*
D
E
• Patient utilizes illicit market • Department of Health & Board of Medicine can
notify medical professionals about CDC guidelines
• Pass state law to prohibit it
NOF
• Patient breaks protocols and risks care• Pass laws and regulations that allow
these facilities to act as caregivers
YES
CONTINUE TO NEXT PAGE
Hospices, hospitals, and/or treatment center allows MC
use*
Americans for Safe Access and our advisors have analyzed current medical cannabis programs and have identified significant barriers for medical professionals, patients, and their caregivers that prohibits them from fully utilizing medical cannabis as a tool to combat pain and opioid use disorder.
The following chart illustrates the considerations patients face when determining if medical cannabis is an option for treating pain. These barriers are keeping enrollment levels low in medical cannabis programs and limiting the tools patients and their medical professionals have to combat pain.
The patient and his/her medical professional know
about medical cannabisYES

G NO Patient qualifies for program YES
Patient can afford ID card• Patient utilizes illicit
market • Pass law that allows
for patients with drug convictions, on probation, or with special job requirements to qualify
• Pass law that allows medical professionals and patients to choose cannabis as front line treatment
H NO
• Patient utilizes illicit market
• Pass laws and regulations that create discounts for Medicaid recipients and/or financial hardship exemption
I NO There is access for patient
YES
• Patient utilizes illicit market • Pass laws and regulations that
include delivery services and sufficient number of access points
NO Access points has products patient needs
YES
• Patient utilizes illicit market
• Pass laws and regulations that require proper testing and labeling of products
• Pass laws and regulations that allow for diverse types of cannabis and delivery methods
• Pass laws and regulations that create tax-free R&D
NO YESPatient can “afford” treatment
J
K
• Patient changes job or moves
• Pass laws that protect employment, housing, and parental rights
• Pass laws and regulations that remove sales tax and excises taxes for medical cannabis cultivation and manufacturing
• Pass laws and regulations that allow for compassion programs and/or hardship discounts
Cannabis is an option!!
* Patient with existing injury or Illness
YES
Determining if Cannabis is an Option for Pain Treatment
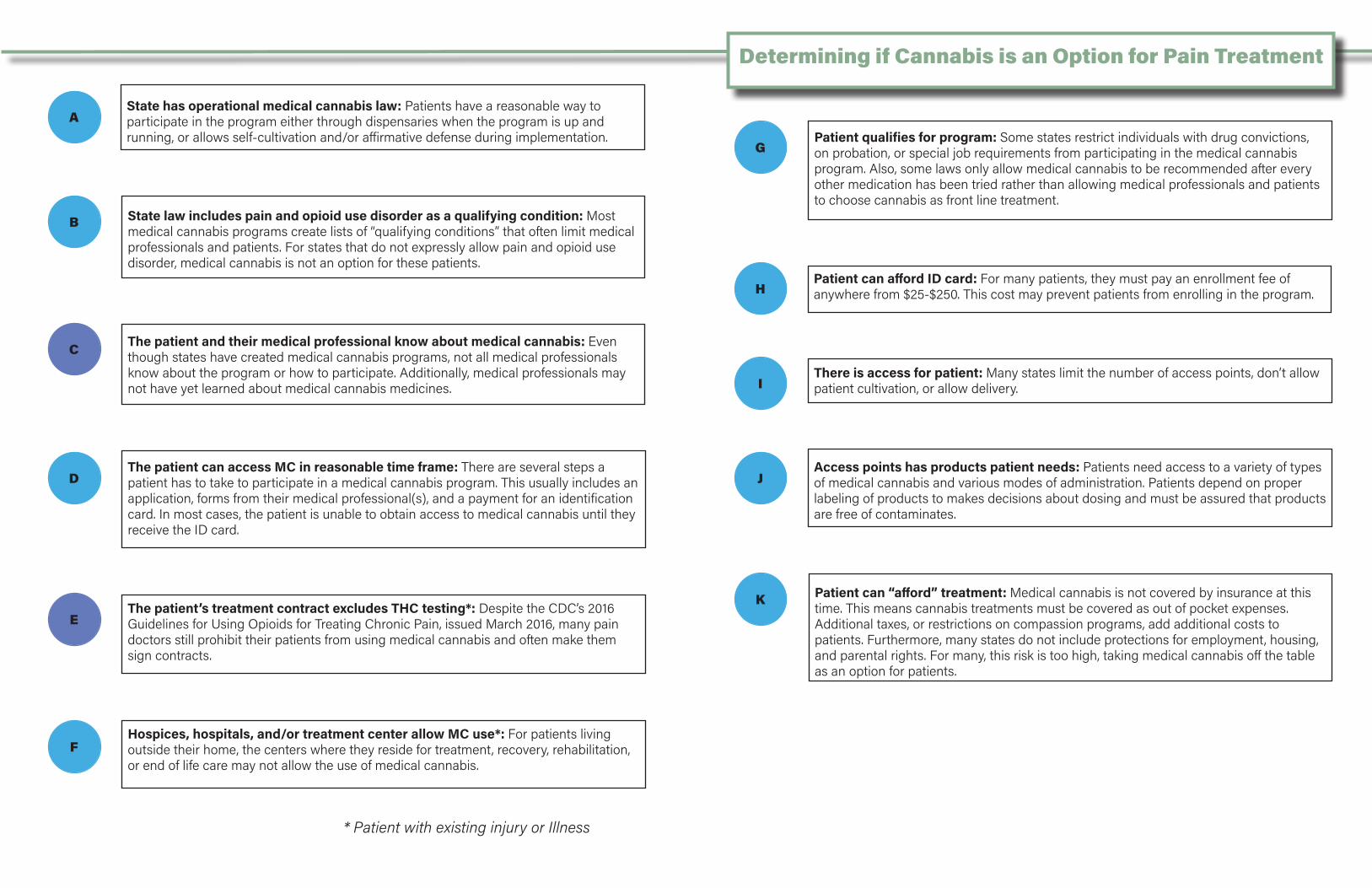
AState has operational medical cannabis law: Patients have a reasonable way to participate in the program either through dispensaries when the program is up and running, or allows self-cultivation and/or affirmative defense during implementation.
State law includes pain and opioid use disorder as a qualifying condition: Most medical cannabis programs create lists of “qualifying conditions” that often limit medical professionals and patients. For states that do not expressly allow pain and opioid use disorder, medical cannabis is not an option for these patients.
B
C The patient and their medical professional know about medical cannabis: Even though states have created medical cannabis programs, not all medical professionals know about the program or how to participate. Additionally, medical professionals may not have yet learned about medical cannabis medicines.
The patient can access MC in reasonable time frame: There are several steps a patient has to take to participate in a medical cannabis program. This usually includes an application, forms from their medical professional(s), and a payment for an identification card. In most cases, the patient is unable to obtain access to medical cannabis until they receive the ID card.
D
The patient’s treatment contract excludes THC testing*: Despite the CDC’s 2016 Guidelines for Using Opioids for Treating Chronic Pain, issued March 2016, many pain doctors still prohibit their patients from using medical cannabis and often make them sign contracts.
E
Hospices, hospitals, and/or treatment center allow MC use*: For patients living outside their home, the centers where they reside for treatment, recovery, rehabilitation, or end of life care may not allow the use of medical cannabis.
F
GPatient qualifies for program: Some states restrict individuals with drug convictions, on probation, or special job requirements from participating in the medical cannabis program. Also, some laws only allow medical cannabis to be recommended after every other medication has been tried rather than allowing medical professionals and patients to choose cannabis as front line treatment.
Patient can afford ID card: For many patients, they must pay an enrollment fee of anywhere from $25-$250. This cost may prevent patients from enrolling in the program.H
IThere is access for patient: Many states limit the number of access points, don’t allow patient cultivation, or allow delivery.
Access points has products patient needs: Patients need access to a variety of types of medical cannabis and various modes of administration. Patients depend on proper labeling of products to makes decisions about dosing and must be assured that products are free of contaminates.
Patient can “afford” treatment: Medical cannabis is not covered by insurance at this time. This means cannabis treatments must be covered as out of pocket expenses. Additional taxes, or restrictions on compassion programs, add additional costs to patients. Furthermore, many states do not include protections for employment, housing, and parental rights. For many, this risk is too high, taking medical cannabis off the table as an option for patients.
J
K
* Patient with existing injury or Illness
Determining if Cannabis is an Option for Pain Treatment

18 19
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS
BARRIERS AND SOLUTIONS
CHAPTER 2 MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
Section 14. Patient Cultivation Registrations
(A) The Department shall issue a cultivation registration to a qualifying patient or their personal caregiver. No more than 10 qualified patients may collectively cultivate, and each participating patient must obtain a cultivation registration. The Department may deny a registration based on the provision of false information by the applicant. Such registration shall allow the qualifying patient or their personal caregiver to cultivate an area of limited square footage of plant canopy, sufficient to maintain a 90-day supply of cannabis, and shall require cultivation and storage only in a restricted access area.
(B) The Department shall issue regulations consistent with this section within 120 days of the effective date of this law. Until the department issues such final regulations, the written recommendation of a qualifying patient’s physician shall constitute a limited cultivation registration.
(C) A qualifying patient or personal caregiver shall not be considered to be in possession of more than a 90-day supply at the location of a restricted access area used collectively by more than one patient, so long as the total amount of cannabis within the restricted access area is not more than a 90-supply for all the participating qualifying patients. A copy of each qualifying patient’s written recommendation shall be retained at the shared cultivation facility.
Figure 2., Section 14 of ACT NOW
Medical Cannabis Program Excludes Pain and Opioid Use Disorder as Qualifying
Conditions.
Most medical cannabis programs create lists of “qualifying conditions” that often limit medical professionals and patients. For states that do not expressly allow pain and opioid use disorder, medical cannabis is not option for these patients. Many states are moving toward removing the qualifying conditions list and leaving this decision to medical professionals and their patients.
Solution: Pass laws allowing medical professionals to choose conditions or expressly allow pain and opioid use disorder to lists of “qualifying conditions. (Figure 3., Section 2 of ACT NOW)
2
Section 2. Definitions
(P) “Opioid use disorder” means any condition that reflects physical or psychological dependence on opioid medicines, including but not limited to prolonged self administration, administration in doses higher than prescribed, or use for non-medical purposes.
(W) “Qualifying medical condition” shall mean any condition for which treatment with medical cannabis would be beneficial, as determined by a patient’s qualified medical professional, including but not limited to cancer, glaucoma, positive status for human immunodeficiency virus, acquired immune deficiency syndrome (AIDS), hepatitis C, amyotrophic lateral sclerosis (ALS), Crohn’s disease, Parkinson’s disease, post-traumatic stress disorder, arthritis, chronic pain, neuropathic and other intractable chronic pain, multiple sclerosis, and opioid use disorder.
Figure 3., Section 2 of ACT NOW
Section 5. Affirmative Defense
An individual may establish an affirmative defense to charges of violations of state law relating to cannabis through proof at trial, by a preponderance of the evidence, that their use was medical if the individual is:
(A) a qualifying patient or a personal caregiver who is not registered with the (STATE) but is in compliance with all other terms and conditions of the state law; or
(B) a qualifying patient or a personal caregiver who is in possession of more than a 90-day supply of cannabis and can demonstrate the amount possessed in excess of the 90-day supply was necessary to provide a consistent and reliable source of medical cannabis to treat the qualifying patient.
(C) a non-resident of [STATE] shall be considered a qualifying patient for this Section if they have or can establish through a preponderance of the evidence that an individual authorized in their state of residence, who is authorized to prescribe medications, has recommended the therapeutic use of cannabis for the non-resident.
Figure 1., Section 5 of ACT NOW
State Medical Cannabis Program is Not Operational.
Thirty states have passed medical cannabis laws and another 16 have passed restricted medical cannabis laws. For some of these states, implementation has taken as long as 4 years, leaving patients waiting. States with new laws can expedite patient enrollment and allow affirmative defenses and self-cultivation (permanent or temporary) while the program is being implemented.
Solution: Pass laws that allows self-cultivation and/or affirmative defense during implementation and beyond. (Figure 1., Section 5 and Figure 2., Section 14 of ACT NOW)
1

20 21
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS CHAPTER 2 MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
The Medical Professional and Patient Do Not Know About Medical Cannabis as an Option.
Even though states have created medical cannabis programs, not all medical professionals know about the programs or how to participate. Additionally, medical professionals may not have yet learned about medical cannabis treatments and protocols. There are now Continuing Medical Education (CME) accredited courses for medical professionals.
Solutions: Department of Health & Board of Medicine notifies medical professionals about the program and CME courses.
Department of Health includes information about medical cannabis in all opioid crisis materials.
Department of Health notifies patient advocacy organizations about the program and offers patient education about medical cannabis.(Figure 4., Section 19 of ACT NOW)
3
Section 19. Implementation of Regulations and Fees
(H) The Department shall issue regulations for continuing education requirements for healthcare practitioners that provide for, at minimum, 2.0 hours concerning dosing methods, preparations and interactions with other substances including opioids.
Figure 4., Section 19 of ACT NOW
The Patient Does Not Have Access in Reasonable Timeframe
There are several steps a patient has to take to participate in a medical cannabis program. This usually includes an application, forms from their medical professional(s), and a payment for an identification card. In most cases, the patient is unable to obtain access to medical cannabis until they receive the ID card. The cards can often take up to 60 days to be processed. For patients setting their course for pain management, or patients entering chemotherapy, this delay means that medical cannabis is not an option.
Solution: Pass laws requiring state-issued ID cards to process in 24 hours, or allow patients to use recommendations from physicians to participate in program until ID card arrives. (Figure 5., Section 15 of ACT NOW)
4
Section 15. Medical cannabis registration cards for qualifying patients and designated caregiver
(D) Upon receiving a medical cannabis recommendation under this section, a patient shall immediately qualify to begin use of medical cannabis and nothing in this chapter shall prohibit a qualifying patient from obtaining medical cannabis on the same date that a recommendation is issued by a health care provider. A healthcare practitioner’s recommendation will remain valid as a method to participate in the medical cannabis program until the application for a registration card is approved or denied by the Department.
Figure 4., Section 15 of ACT NOW
The Patient’s Pain Treatment Contract Requires THC Testing.
In response to the opioid crisis, many medical professionals use pain contracts or treatment contracts1 with their patients who are under care for pain. These contracts often prohibit the use of cannabis even under medical use. If the patient tests positive for THC, they are denied treatment and abruptly cut off all pain medications. In the Guidelines for Using Opioids for Treating Chronic Pain, issued on March 18, 2016, the Centers for Disease Control (CDC) advise clinicians against testing for cannabis, specifically tetrahydrocannabinol (THC), as criteria for eligible care. The guidelines state that a positive test for cannabis is not an effective indication for patient management outcomes and warns clinicians that dismissing a patient from care based solely on a urine drug test result could have adverse consequences for the patient’s safety.
Solution: Department of Health & Board of Medicine notifies medical professionals about CDC guidelines. (Figure 6., Section 7(E) of ACT NOW)
1 https://www.drugabuse.gov/sites/default/files/files/SamplePatientAgreementForms.pdf
5
Section 7. Discrimination Prohibited
E) Health care practitioners shall not disqualify or refuse to provide care for a patient due to positive urinary or blood test results indicating the presence of cannabis or cannabis metabolites including tetrahydrocannabinol, nor shall the presence of compounds of cannabis or cannabis metabolites be a reason for the cessation of care.
Figure 6., Section 7(E) of ACT NOW
Hospices, Hospitals, and/or Treatment Centers Do Not Allow for the Use of Medical Cannabis.
For patients living outside their home, the centers where they reside for treatment, recovery, rehabilitation, or end of life care may not allow the use of medical cannabis.
Solution: Pass laws to allow these facilities to become caregivers and allow medical cannabis use on these premises. (Figure 7., Section 2(S) of ACT NOW)
6
Section 2. Definitions
S) “Personal caregiver” shall mean a person or entity including hospitals, nursing care institutions, hospices, recovery centers, or home health centers, who have agreed to assist with a qualifying patient’s medical use of cannabis.
Figure 7., Section 2(S) of ACT NOW

22 23
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS CHAPTER 2 MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
The Patient Does Not Qualify.
Some states restrict individuals who have drug convictions, are on probation, or have special job requirements from participating in the state’s medical cannabis program. Also, some laws only allow medical cannabis to be recommended after every other medication has been tried, rather than allowing medical professionals and patients to choose cannabis as front line treatment.
Solution: Pass laws to allow medical professionals and patients to use cannabis as front line treatment, not after all other medications fail. (Figure 8., Section 10 (G), Figure 9., Section 2(A)(1), and Figure 10., Section 3(A) of ACT NOW)
7 Section 2. Definitions
(A) “Bona fide medical professional-patient relationship” means a patient and a licensed health care professional that includes:
1. Referral from a primary care practitioner or a physical examination and review of medical history.
2. An explanation of the benefits and risks of medical use of cannabis, with or without first explaining options other than medical cannabis for treatment.
3. On-going expectation of care.
Figure 9., Section 2(A) of ACT NOW
Section 3. Protection from State Prosecution and Penalties for Qualified Medical Professionals
A qualified medical professional shall not be penalized under [State] law, in any manner, or denied any right or privilege, for:
(A) advising a qualifying patient about the risks and benefits of the medical use of cannabis with or without discussing other treatment options prior to recommending cannabis;
Figure 10., Section 3(A) of ACT NOW
Section 10. Limitations of Law
(G) Nothing in this law prevents an individual who is on probation or parole from participating in this program, including individuals convicted of excluded felony offenses.
Figure 8., Section 10(G) of ACT NOW
Patient Can Not Afford Enrollment.
Many patients must pay an enrollment fee of anywhere from $25-$250. This cost may prevent patients from enrolling in the program.
Solution: Create low-income and hardship waivers for ID costs. (Section 2 (Figure 12.) and 15(F) (Figure 11.) of ACT NOW)
8
Section 15. Medical cannabis registration cards for qualifying patients and designated caregivers
(F) The Department may assess a reasonable fee of no more than twenty-five dollars ($25) to those seeking to obtain a registration card. Notwithstanding, no fee shall be assessed for any patient who is determined by the Department to have a financial hardship.
Figure 11., Section 15 of ACT NOW
Section 2. Definitions
(H) “Financial Hardship” means an individual who is a recipient of public health benefits, or Supplemental Security insurance payments, social security disability benefits, or who otherwise is unable to generate an income that is 300% of the federal poverty level.
Figure 12., Section 2 of ACT NOW
There is No Reasonable Way for Patient to Access Medical Cannabis.
Many states limit the number of access points, don’t allow patient cultivation, or allow delivery. Implementation of these laws can take years. States should consider measures such as self-cultivation, decriminalization, or allowing possession from other states.
Solution: Pass laws that have a high number of access points and create incentives for communities that are licensing them. (Figure 13., Section 12(C) of ACT of NOW).
Pass laws that include delivery services. (Figure 14., Section 12(E) of ACT NOW)
9
Section 12. Registration of Medical Cannabis Establishments
(C) In the first year after the effective date, the Department shall issue registrations for up to [XXX] medical cannabis establishments, provided that at least one dispensing facility shall be located in each county. If a county has more than 1,000 qualifying patients, an additional dispensary shall be established for each additional 1,000 patients residing in the county. In the event the Department determines in a future year that the number of dispensing facilities is insufficient to meet patient needs, the Department shall have the power to increase the number of registered medical cannabis dispensing facilities in the state, or raise the limit of medical cannabis dispensing facilities in a county.
Figure 13., Section 12(C) of ACT NOW
Section 12. Registration of Medical Cannabis Establishments
(E) The Department shall create rules to facilitate the home delivery of medical cannabis and cannabis-derived products from a dispensing facility to a qualifying patient or personal caregiver.
Figure 15., Section 12(E) of ACT NOW

24 25
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS CHAPTER 2 MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
The Access Points Do Not Have the Products the Patient Needs.
Not all medical cannabis products are the same, patients need access to a variety of types of medical cannabis and various modes of administration. Patients depend on proper labeling of products to make decisions about dosing and must be assured that products are free of contaminates.
Solutions: Pass laws that allow for a variety of types of medical cannabis and cannabinoid content and various modes of administration. (Figure 14., Section 2(C) of ACT NOW)
Pass laws and regulations that include product safety protocols. (Figure 15., Section 18 of ACT NOW)
Pass laws and regulations that create tax incentive for R&D. (Figure 16., Section 21 of ACT NOW)
Pass laws and regulations that prevent shortages. (Figure 17., Section 12(C) of ACT NOW)
10Section 2. Definitions
(C) “Cannabis-derived product” means: a product other than whole-plant cannabis which is manufactured from cannabis and is intended for use or consumption by humans through means such as, but not limited to, food stuffs, extracts, oils, tinctures, topicals, and suppositories.
Figure 14., Section 2(C) of ACT NOW
Section 18. Product Safety
(A) The Department will adopt product safety standards for the cultivation, processing, manufacturing, labeling, testing, and distribution of cannabis based on the American Herbal Products Association’s Recommendations to Regulators and determine a comprehensive plan for the inspection, oversight, and enforcement of such guidelines.
Figure 15., Section 18 of ACT NOW
Section 21. Research and Development
(A) The Department shall gather objective scientific research regarding the efficacy of administering cannabis and its components as part of medical treatment.
(B) There is established within the state treasury the Medical Cannabis Research and Development Fund. The fund shall be expanded at the discretion of the director of health:
(1) to develop and investigate new methods of cannabis production, preparation, and delivery methods of medical cannabis and towards observational and clinical trials.(2) the fund shall consist of all monies derived from fees collected pursuant to section 19.
(C) The department shall issue a publicly available annual report detailing the investments and projects of the Medical Cannabis Research and Development Fund and the research gathered.
Figure 16., Section 21(1,2) of ACT NOW
Section 12. Registration of Medical Cannabis Establishments
(C) In the first year after the effective date, the Department shall issue registrations for up to [XXX] medical cannabis establishments, provided that at least one dispensing facility shall be located in each county. If a county has more than 1,000 qualifying patients, an additional dispensary shall be established for each additional 1,000 patients residing in the county. In the event the
Department determines in a future year that the number of dispensing facilities is insufficient to meet patient needs, the Department shall have the power to increase the number of registered medical cannabis dispensing facilities in the state, or raise the limit of medical cannabis dispensing facilities in a county.
Figure 17., Section 12(C) of ACT NOW

26 27
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS CHAPTER 2 MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
Patient Can Not “Afford” Treatment.
Medical cannabis is not covered by insurance at this time. This means cannabis treatments must be covered as out of pocket expenses. Additional taxes, or restrictions on compassionate programs, result in additional costs to patients. Furthermore, many states do not include protections for employment, housing and parental rights. For many patients, this risk is too high, taking medical cannabis off the table as an option.
Solution: Pass laws banning drug testing for THC for employment. (Figure 18., Section 7(A) of ACT NOW)
Pass civil protections for housing, employment, parental rights, and organ transplant lists. (Figure 18., Section 7 of ACT NOW)
Pass laws that removes or greatly lowers sales tax. (Figure 19., Section 20 of ACT NOW)
Pass laws that removes or greatly lowers excise tax for cultivating/manufacturing medical cannabis. (Figure 19., Section 20(A) of ACT NOW)
11
Section 7. Discrimination Prohibited
(A) Unless a failure to do so would cause the employer to lose a monetary or licensing-related benefit under federal law or federal regulations, an employer may not discriminate against a person in hiring, termination, or any term or condition of employment, or otherwise penalize a person, based upon either of the following:
1. The person’s status as a qualifying patient, caregiver, or cardholder; or
2. A qualifying patient, caregiver, or cardholder
tests positive for cannabis components or metabolites, unless the individual was impaired by cannabis on the premises of the place of employment or during the hours of employment.
(B) Unless required by federal law or required to obtain federal funding, no landlord may refuse to rent a dwelling unit to a person or take action against a tenant solely on the basis of an individual’s status of a qualifying patient or cardholder under this act.
(C) For the purposes of medical care, including organ transplants, a qualifying patient’s medical use of cannabis does not constitute the use of an illicit substance or otherwise disqualify a qualifying patient from medical care.
(D) Neither the presence of cannabinoid components or metabolites in a person’s bodily fluids, nor conduct related to the medical use of cannabis by a custodial or noncustodial parent, grandparent, pregnant woman, legal guardian, or other person charged with the well-being of a child, shall form the sole or primary basis for any action or proceeding by a child welfare agency or a family or juvenile court. This subsection shall apply only to conduct in compliance with this chapter.
(E) Health care practitioners shall not disqualify or refuse to provide care for a patient due to positive urinary or blood test results indicating the presence of cannabis or cannabis metabolites including tetrahydrocannabinol, nor shall the presence of compounds of cannabis or cannabis metabolites be a reason for the cessation of care.
Figure 18., Section 21(1,2) of ACT NOW
Section 20. Taxation
(A) Medical cannabis businesses shall pay an excise tax of no greater than 7% on the gross receipts of medical cannabis sold to a qualifying patient or to a personal caregiver, but shall not pay a higher tax than businesses of comparable activity and size.
(1) Medical Facilities that produce cannabis exclusively for medical use shall not be subject to excise tax.
(B) Nothing in this chapter shall prevent a medical cannabis business from implementing a sales tax on medical cannabis, however this tax rate shall not exceed [insert states applicable tax for over the counter medications].
(C) If a state has a non-medical cannabis program, medical patients shall be exempt from any applicable sales tax.
Figure 19., Section 20 (A, B, C) of ACT NOW

28 29
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS
Michigan’s legislation and regulations on medical cannabis have many of the elements of ACT NOW.
However, like any medical cannabis program there is still room for significant improvement. The relevant authorities are the Michigan Medical Marihuana1 Act (codified at Michigan Compiled Laws §§333.26421-.26430) (“MMMA”) , the Medical Marihuana Facilities Licensing Act (codified at Michigan Compiled Laws §§281.1-.8) , the Marihuana Trafficking Act (codified at §§§333.27901-.27904), Michigan Admin. Code R. 333.101-.133 (“MAC”, and advisory opinions from the Bureau of Medical Marihuana Rules.
Where the Michigan Laws or regulations sufficiently address an ACT NOW legislative priority, only the relevant legislative or code section will be cited. Where there is the need for an amendment or legislative improvement needed to meet the goals of ACT NOW, the changes will be marked in green. An asterisk (*) indicates amendments to statutes where technical renumbering or lettinger would have to occur due to the placement of the language.
1. Chronic Pain and Opioid Use Disorder as Qualifying Conditions
Michigan already allows for severe and chronic pain as a qualifying conditions in its program. No medical cannabis program in the country currently allows for opioid use disorder as a qualifying condition. Michigan’s laws can be amended as follows: MMMA 333.26423 Definitions. 3. Definitions. Sec. 3. is amended as follows in this act:
(b) “Debilitating medical condition” means 1 or more of the following:
(1) Cancer, glaucoma, positive status for human immunodeficiency virus, acquired
1 Michigan’s spelling is primarily sourced from the original spelling of the word, which first appears in US law in the Marihuana Tax Act of 1937, drafted by the Harry Anslinger, head of the Bureau of Narcotics under President Franklin D. Roosevelt.
CHAPTER 2 MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
MMMA 333.26423 Definitions3. DefinitionsSec. 3. As used in this act:
(a) “Bona fide physician-patient relationship” means a treatment or counseling relationship between a physician and patient in which all of the following are present:(1)The physician has reviewed the patient’s medical records and completed a full assessment of the patient’s medical history and current medical condition, including a relevant, in person, medical evaluation of the patient(2)The physician has created and maintained records of the patient’s condition in accord with medically accepted standards(3)The physician has a reasonable expectation that he or she will provide follow-up care to the patient to monitor the efficacy of the use of medical marihuana as a treatment of the patient’s debilitating medical condition(4)If the patient has given permission, the physician has notified the patient’s primary care physician of patient’s debilitating medical condition and certification for the medical use of marihuana to treat that debilitating condition.(5) Nothing in this section prevents a physician in a bona fide physician-patient relationship from recommending marihuana before recommending other medications.
3. Provide Same Day Access for Medicine
Michigan has a fairly brief turnaround time in between the time a patient application is submitted and when a registry card is issued. If an application is approved, the Department has five (5) days to issue a card. However, in the interim, a patient should be able to to use a written certification from their physician for all rights and privileges associated with a registry identification card, including being able to access medicine, and receive protection from arrest and discrimination. Michigan’s law and rules could be amended as follows:
MICHIGAN DRAFT LEGISLATION AND REGULATIONS
immune deficiency syndrome, hepatitis C, amyotrophic lateral sclerosis, Crohn’s disease, agitation of Alzheimer’s disease, nail patella, opioid use disorder or the treatment of these conditions. (2) A chronic or debilitating disease or medical condition or its treatment that produces 1 or more of the following: cachexia or wasting syndrome; severe and chronic pain; severe nausea; seizures, including but not limited to those characteristic of epilepsy; or severe and persistent muscle spasms, including but not limited to those characteristic of multiple sclerosis. (3) Any other medical condition or its treatment approved by the department, as provided for in section 6(k). (*) Opioid use disorder is a medical condition characterized by a problematic pattern of opioid use that causes clinically significant psychological or physical impairment or distress included a strong desire to use opioids, increased tolerance to opioids, and withdrawal syndrome when opioids are abruptly discontinued.
Opioid use disorder could also be added through the the Petition to add qualifying medical conditions described in Michigan Admin. Code R. 333.133.
2. Recommend Cannabis as a First Resort Medication
Michigan does not explicitly require doctors to recommend other medications before turning to cannabis but the law could be improved so health care practitioners know they are not limited in the medicines that they can recommend. A clarifying statement in the definition of “Bona fide physician-patient relationship” would help resolve this.
MMMA 333.26423 Definitions3. DefinitionsSec. 3. As used in this act: (q) “Written certification” means a document signed by a physician, stating all of the following:
(1) The patient’s debilitating medical condition(2) The physician has completed a full assessment of the patient’s medical history and current medical condition, including a relevant, in person, medical evaluation(3) In the physician’s professional opinion, the patient is likely to receive therapeutic or palliative benefit from the medical use of marihuana to treat or alleviate the patient’s debilitating medical condition or symptoms associated with the debilitating medical condition. (4) A statement indicating that the written certification has the same effect as a registry identification card until the approval of a patient or primary caregiver’s application by the Department.
MMMA 333.26426 Administration and enforcement of rules by department.6. Administration of the Department’s RulesSec. 6. (c) The department shall verify the information contained in an application or renewal submitted pursuant to this section, and shall approve or deny an application or renewal within 15 business days of receiving it. The department may only deny an application or renewal if the applicant did not provide the information required pursuant to this section, or if the department finds that the information provided was falsified. Rejection of an application is considered a final department action subject to judicial review. A written certification from a physician shall constitute the legal equivalent of a registry identification card, affording a patient all rights and privileges under this chapter, until the application is approved or denied. Jurisdiction and venue for judicial review are vested in the circuit court for the county of Ingham.

30 31
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS CHAPTER 2 MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
MAC Rule 333.113 Registration approval; denialRule 13. (1) Pursuant to section 6(c) of the act, MCL 333.26426(c), the department shall approve or deny an application within 15 business days of receiving the original complete application, required fees and required supporting documentation and information. Until the department issues a final determination on an application, a written certification from a physician shall provide the same rights, privileges, and protections afforded to those who hold a registry identification card.
4. End Discriminatory Testing Through Pain Clinics
Currently, state issued health guidelines for Managing Chronic Non-Terminal Pain used by the University of Michigan hospital system prevent users of cannabis from being prescribed controlled substances. The current guidelines, as written, make no distinction between registered qualifying patients and those using cannabis who are not enrolled in the state program. Page 33 of these regulations described problem results with positive urine screens: “Positive screen. Absolutely no controlled prescription will be prescribed. Controlled substances cannot be safely prescribed in patients taking illicit drugs, including cannabis.” As many medical cannabis patients use opiate therapies in conjunction with their medical cannabis use, these guidelines create a problematic scenario.
While discriminatory testing for tetrahydrocannabinol (THC) and other cannabinoids by pain clinics and pain specialists can not be cleanly fixed legislatively, it could be addressed by the Michigan Department of Health adopting the guidelines issued by the 2016 Centers for Disease Control entitled Prescribing Opioids for Chronic Pain.
This could also be resolved through an advisory opinion from the Bureau of Medical Marihuana Rules adopting the CDC guidelines that recommend against testing for THC and other cannabis compounds in pain patients. Language for this advisory bulletin is below.
of the Michigan Medical Marihuana Act. It only provides a defense from the effective date of the act.
MMMA 333.26428 Defenses
7. Protect the Civil Rights of Patients
Michigan’s program partially protects civil rights of patients including providing protections for parents who are medical cannabis patients, explicit privacy standards, and arrest protections. However, Michigan’s legislation that provides civil protections could be expanded as follows:
MMMA 333.26424 Qualifying patient or primary caregiver; arrest, prosecution, or penalty prohibited; conditions; privilege from arrests; presumption; compensation; physician subject to arrest, prosecution, or penalty prohibited; marihuana paraphernalia; person in presence or vicinity of medical use of marihuana; registry identification card issued outside of department; sale of marihuana as felony; penalty; marihuana-infused product
8. Affirmative Defense and Dismissal for Medical MarihuanaSec 8. (a) except as provided in section 7(b), a patients and a patient’s primary caregiver, if any, may assert the medical purpose of using marihuana as a defense to any prosecution involving marihuana, and this defense shall be presumed valid where the evidence shows that:
(1) A physician has stated that, in the physician’s professional opinion, after having completed a full assessment of the patient’s medical history and current medical condition made in the course of a bona fide physician-patient relationship, the patient is likely to receive therapeutic or palliative benefit from the medical use of marihuana to treat or alleviate the patient’s serious or debilitating medical condition or symptoms of the patient’s serious or debilitating medical condition;(2) The patient and the patient’s primary caregiver, if any, were collectively in
“The purpose of this advisory bulletin is to inform the public of the Bureau of Medical Marihuana Regulation’s intentions regarding testing for tetrahydrocannabinol (THC) at pain management clinics and pain specialists. When conducting urine testing, clinicians should not test for substances for which results would not affect patient management or for which implications for patient management are unclear. There might be uncertainty about the clinical implications of a positive urine drug test for THC. This bulletin is for advisory purposes only and is subject to change.”
5. Allow Hospice, Recovery Centers and Home Health Centers to be Caregivers
Michigan currently only allows individuals, and not entities to serve as caregivers. This change would allows healthcare organizations to serve as caregivers:
MMMA 333.26323 Definitions
(k) “Primary caregiver” or “caregiver” means a (1) Person who is at least 21 years old and who has agreed to assist with a patient’s medical use of marihuana and who has not been convicted of any felony within the past 10 years and has never been convicted of a felony involving illegal drugs or a felony that is an assaultive crime as defined in section 9a of chapter X of the code of criminal procedure, 1927 PA 175, MCL 770.9a.
(2) An entity including hospitals, nursing care institutions, hospices, recovery centers, or home health centers licensed by this state, who have agreed to assist with a qualifying patient’s medical use of marihuana.
6. Drug Conviction Reversal for Certain Offenses
Michigan’s Medical Marihuana Program does not provide retroactive dismissal or expungement of low level drug offenses that occurred before the passage
possession of a quantity of marihuana that was not more than was reasonably necessary to ensure the uninterrupted availability of marihuana for the purpose of treating or alleviating the patient’s serious or debilitating medical condition or symptoms of the patient’s serious or debilitating medical condition; and(3) The patient and the patient’s primary caregiver, if any, were engaged in the acquisition, possession, cultivation, manufacture, use, delivery, transfer, or transportation of marihuana or paraphernalia relating to the use of marihuana to treat or alleviate the patient’s serious or debilitating medical condition or symptoms of the patient’s serious or debilitating medical condition.
(b) A person may assert the medical purpose for using marihuana in a motion to dismiss, and the charges shall be dismissed following an evidentiary hearing where the person shows the elements listed in subsection (a).
(c) If a patient or a patient’s primary caregiver demonstrates the patient’s medical purpose for using marihuana pursuant to this section, the patient and the patient’s primary caregiver shall not be subject to the following for the patient’s medical use of marihuana:
(1) disciplinary action by a business or occupational or professional licensing board or bureau; or(2) forfeiture of any interest in or right to property.
(d) A patient, primary caregiver, or physician, who was convicted of an offense detailed in this section prior to the effective date of this act, shall be able to petition the circuit court of the county in which they reside for expungement proceedings decided consistently with the provisions of this chapter.
780.621 Application for order setting aside conviction; misdemeanor conviction; setting

32 33
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS CHAPTER 2 MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
aside of certain convictions prohibited; victim of human trafficking violation; time and contents of application; submitting application and fingerprints to department of state police; report; application fee; contest of application by attorney general or prosecuting attorney; notice to victim; affidavits and proofs; court order; definitions.Sec 1....(4) A person who is convicted of a violation of section 448, 449, or 450 of the Michigan penal code, 1931 PA 328, MCL 750.448, 750.449, and 750.450, or a local ordinance substantially corresponding to section 448, 449, or 450 of the Michigan penal code, 1931 PA 328, MCL 750.448, 750.449, and 750.450, may apply to have that conviction set aside if he or she committed the offense as a direct result of his or her being a victim of a human trafficking violation.
(*) A person who is convicted of a violation of section 333.7403 of the Michigan Penal code, or a local ordinance substantially corresponding to 333.7403 of the Michigan penal code, may apply to have that conviction set aside if he or she committed the offense as a direct result of his or her being a patient, caregiver, or physician enrolled in the Medical Marihuana Program.
8. Protections for the Medical Use of Marihuana. Sec. 4. (a) A qualifying patient who has been issued and possesses a registry identification card is not subject to arrest, prosecution, or penalty in any manner, or denied any right or privilege, including, but not limited to, civil penalty or disciplinary action by a business or occupational or professional licensing board or bureau, for the medical use of marihuana in accordance with this act, provided that the qualifying patient possesses an amount of marihuana that does not exceed a combined total of 2.5 ounces of usable marihuana and usable marihuana equivalents, and, if the qualifying patient has not specified that a primary caregiver will be allowed under state law to cultivate marihuana for the qualifying patient, 12 marihuana plants kept in an enclosed, locked facility. Any incidental amount of seeds, stalks, and unusable roots shall also be allowed under state law and shall not
product if in a liquid form.(d) A person shall not be denied custody or visitation of a minor for acting in accordance with this act, unless the person’s behavior is such that it creates an unreasonable danger to the minor that can be clearly articulated and substantiated. (*) For the purposes of medical care, including organ transplants, a qualifying patient’s medical use of marihuana does not constitute the use of an illicit substance or otherwise disqualify a qualifying patient from medical care. (*) A school, employer or landlord may not refuse to enroll or employ or lease to or otherwise penalize a person solely for that person’s status as a qualifying patient or a primary caregiver unless failing to do so would put the school, employer or landlord in violation of federal law or cause it to lose a federal contract or funding. (e) There is a presumption that a qualifying patient or primary caregiver is engaged in the medical use of marihuana in accordance with this act if the qualifying patient or primary caregiver complies with both of the following:
(1) Is in possession of a registry identification card.(2) Is in possession of an amount of marihuana that does not exceed the amount allowed under this act. The presumption may be rebutted by evidence that conduct related to marihuana was not for the purpose of alleviating the qualifying patient’s debilitating medical condition or symptoms associated with the debilitating medical condition, in accordance with this act.
(f ) A registered primary caregiver may receive compensation for costs associated with assisting a registered qualifying patient in the medical use of marihuana. Any such compensation does not constitute the sale of controlled substances. (g) A physician shall not be subject to arrest, prosecution, or penalty in any manner, or denied any right or privilege, including but not limited to civil penalty or disciplinary action by the Michigan board
be included in this amount. The privilege from arrest under this subsection applies only if the qualifying patient presents both his or her registry identification card and a valid driver license or government-issued identification card that bears a photographic image of the qualifying patient. (b) A primary caregiver who has been issued and possesses a registry identification card is not subject to arrest, prosecution, or penalty in any manner, or denied any right or privilege, including but not limited to civil penalty or disciplinary action by a business or occupational or professional licensing board or bureau, for assisting a qualifying patient to whom he or she is connected through the department’s registration process with the medical use of marihuana in accordance with this act. The privilege from arrest under this subsection applies only if the primary caregiver presents both his or her registry identification card and a valid driver license or government-issued identification card that bears a photographic image of the primary caregiver. This subsection applies only if the primary caregiver possesses marihuana in forms and amounts that do not exceed any of the following:
(1) For each qualifying patient to whom he or she is connected through the department’s registration process, a combined total of 2.5 ounces of usable marihuana and usable marihuana equivalents.(2) For each registered qualifying patient who has specified that the primary caregiver will be allowed under state law to cultivate marihuana for the qualifying patient, 12 marihuana plants kept in an enclosed, locked facility.(3) Any incidental amount of seeds, stalks, and unusable roots.
(c) For purposes of determining usable marihuana equivalency, the following shall be considered equivalent to 1 ounce of usable marihuana:
(1) 16 ounces of marihuana-infused product if in a solid form.(2) 7 grams of marihuana-infused product if in a gaseous form.(3) 36 fluid ounces of marihuana-infused
of medicine, the Michigan board of osteopathic medicine and surgery, or any other business or occupational or professional licensing board or bureau, solely for providing written certifications, in the course of a bona fide physician-patient relationship and after the physician has completed a full assessment of the qualifying patient’s medical history, or for otherwise stating that, in the physician’s professional opinion, a patient is likely to receive therapeutic or palliative benefit from the medical use of marihuana to treat or alleviate the patient’s serious or debilitating medical condition or symptoms associated with the serious or debilitating medical condition, provided that nothing shall prevent a professional licensing board from sanctioning a physician for failing to properly evaluate a patient’s medical condition or otherwise violating the standard of care for evaluating medical conditions. (h) A person shall not be subject to arrest, prosecution, or penalty in any manner, or denied any right or privilege, including but not limited to civil penalty or disciplinary action by a business or occupational or professional licensing board or bureau, for providing a registered qualifying patient or a registered primary caregiver with marihuana paraphernalia for purposes of a qualifying patient’s medical use of marihuana.
(i) Any marihuana, marihuana paraphernalia, or licit property that is possessed, owned, or used in connection with the medical use of marihuana, as allowed under this act, or acts incidental to such use, shall not be seized or forfeited. ( j) A person shall not be subject to arrest, prosecution, or penalty in any manner, or denied any right or privilege, including but not limited to civil penalty or disciplinary action by a business or occupational or professional licensing board or bureau, solely for being in the presence or vicinity of the medical use of marihuana in accordance with this act, or for assisting a registered qualifying patient with using or administering marihuana. (k) A registry identification card, or its equivalent, that is issued under the laws of another state, district, territory, commonwealth, or insular possession of

34 35
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS CHAPTER 2 MAKING MEDICAL CANNABIS AN OPTION FOR PAIN AND OPIOID USE DISORDER
the United States that allows the medical use of marihuana by a visiting qualifying patient, or to allow a person to assist with a visiting qualifying patient’s medical use of marihuana, shall have the same force and effect as a registry identification card issued by the department. (l) Any registered qualifying patient or registered primary caregiver who sells marihuana to someone who is not allowed the medical use of marihuana under this act shall have his or her registry identification card revoked and is guilty of a felony punishable by imprisonment for not more than 2 years or a fine of not more than $2,000.00, or both, in addition to any other penalties for the distribution of marihuana. (m) A person shall not be subject to arrest, prosecution, or penalty in any manner or denied any right or privilege, including, but not limited to, civil penalty or disciplinary action by a business or occupational or professional licensing board or bureau, for manufacturing a marihuana-infused product if the person is any of the following:
(1) A registered qualifying patient, manufacturing for his or her own personal use.(2) A registered primary caregiver, manufacturing for the use of a patient to whom he or she is connected through the department’s registration process.
(n) A qualifying patient shall not transfer a marihuana-infused product or marihuana to any individual. (o) A primary caregiver shall not transfer a marihuana-infused product to any individual who is not a qualifying patient to whom he or she is connected through the department’s registration process.
9. Establish Rigorous Product Safety Standards
Michigan’s proposed regulations related to Medical Marihuana Facilities and Medical Marihuana Tracking begin to address consumer and product safety standards. The Bureau of Medical Marijuana rules should issue product safety regulations that are the same or substantially similar to those of Maryland
quarterly retail income of the provisioning center and the amount of tax due, and shall submit a copy of the form to the department. If a law authorizing the recreational or nonmedical use of marihuana in this state is enacted, this section does not apply beginning 90 days after the effective date of that law.
(2) The taxes imposed under this section shall be administered by the department of treasury in accordance with 1941 PA 122, MCL 205.1 to 205.31, and this act. In case of conflict between the provisions of 1941 PA 122, MCL 205.1 to 205.31, and this act, the provisions of this act prevail.
If Michigan eventually approves cannabis for adult use, all medical sales should be exempt from sales tax and this section should be amended appropriately.
12. Expanded Research/ Research and Development
Michigan’s state universities have conducted research surrounding medical cannabis, but there is no centralized aspect of Michigan’s program that encourages extended research into the benefits of cannabis. Michigan’s Medical Marihuana Act could be amended as follows:
MMMA 333.26431 (New Section) 11. ResearchSec. 11(A) The Department shall gather objective scientific research regarding the efficacy of administering cannabis and its components as part of medical treatment and issue an annual report of its findings. (B) There is established within the state treasury the Medical Cannabis Research and Development Fund. The fund shall be expanded at the discretion of the director of health:
(1) to develop and investigate new methods of cannabis production, preparation, and delivery of medical cannabis and towards observational and clinical trials. (2) the fund shall consist of all monies derived from fees collected from the
which has some of the robust medical cannabis product safety regulations in the country (Annotated Code of Maryland §§13-3301—13-3303).
10. Create Financial Hardship Exemptions for ID Cards and Licenses
Michigan’s program determines fees for the program through regulations. Currently there is no financial hardship or waiver for veterans to participate in Michigan’s Medical Cannabis Program.
MAC R 333.101 Definitions(*) means an individual who is a recipient of public health benefits, or Supplemental Security insurance payments, social security disability benefits, or who otherwise is unable to generate an income that is 300% of the federal poverty level.
MAC R 333.111 Fees, Patient refunds.Rule 11. (1) a qualifying patient shall pay a $60.00 fee for a renewal or a new application. This fee shall be waived by the department if the patient or primary giver can show proof of financial hardship or military service.
11. Tax Relief
Michigan did not provide for taxation through the Michigan Medical Marihuana Act or its accompanying rules. However, the Medical Marihuana Facilities Licensing Act later provided for the taxation and assessment of medical marihuana. Medical Marihuana is currently taxed at a rate of 3% of the providing center’s gross receipts. Making medical marihuana affordable and accessible to patients greatly increases access.
MMFLA 333.27601Sec. 601(1) A tax is imposed on each provisioning center at the rate of 3% of the provisioning center’s gross retail receipts. By 30 days after the end of the calendar quarter, a provisioning center shall remit the tax for the preceding calendar quarter to the department of treasury accompanied by a form prescribed by the department of treasury that shows the gross
program.(C) The department shall issue a publicly available annual report detailing the investments and projects of the Medical Cannabis Research and Development Fund and the research gathered. 13. Accessibility
Michigan’s Medical Marihuana program allows for delivery of cannabis (MMMA 333.26424a(1)) to homebound patients and allows patients to grow their own medicine (MMMA 333.26424(4a). These features of Michigan’s program make it easier for patients to access medicine.

36 37
OVERVIEW OF CURRENT STATE LAWS
HOW DOES YOUR STATE MEASURE UP?
CHAPTER 3 OVERVIEW OF CURRENT STATE LAWS
Chapter 3 Overview of Current State Laws
States
Chr
onic
Pai
n an
d O
pioi
d U
se D
isor
der
as Q
ualif
ying
C
ondi
tions
Reco
mm
end
Can
nabi
s as
a
Firs
t Res
ort
Prov
ide
for S
ame
Day
Acc
ess
to
Med
icin
e
End
Dis
crim
inat
ory
Test
ing
at P
ain
Clin
ics
Hos
pice
, Re
cove
ry
Cen
ters
and
H
ome
Hea
lth
Cen
ters
to b
e C
areg
iver
s
Dru
g C
onvi
ctio
n Re
vers
al fo
r C
erta
in O
ffens
es
Prot
ect t
he
Civ
il Ri
ghts
of
Patie
nts
Rigo
rous
Pr
oduc
t Saf
ety
Stan
dard
s
Fina
ncia
l H
ards
hip
Exem
ptio
ns fo
r ID
Car
ds a
nd
Lice
nces
Tax
Relie
f
Rese
arch
and
D
evel
opm
ent
for M
edic
al
Can
nabi
s Pr
ogra
m
Supp
ort
Rese
arch
Alaska ✓ ✓ ✓
Arizona ✓ ✓ Case by case ✓ ✓
Arkansas ✓ ✓ ✓ ✓ ✓
California ✓ ✓ ✓ ✓ ✓ Partial ✓ ✓ Partial ✓ ✓
Colorado ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓
Connecticut ✓ ✓ ✓ Partial ✓ ✓
Delaware ✓ ✓ ✓ ✓ ✓ ✓
District of Columbia ✓ ✓ ✓
Florida ✓ ✓ ✓ ✓ ✓ ✓
Hawai'i ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓
Illinois ✓ ✓ ✓ ✓ ✓ ✓
Louisiana ✓
Maine ✓ ✓ ✓ Partial ✓ ✓
Maryland ✓ ✓ ✓ Partial ✓ ✓
Massachusetts ✓ ✓ ✓ Pending ✓ Partial ✓ ✓
Michigan ✓ ✓ Partial ✓
Minnesota ✓ Partial ✓ ✓ ✓ ✓
Montana ✓ ✓ Limited ✓ ✓ ✓
Nevada ✓ ✓ ✓ Partial ✓ ✓
New Hampshire ✓
New Jersey Limited
New Mexico ✓ ✓
New York ✓ Limited
North Dakota ✓
Ohio ✓
Oregon ✓ ✓ ✓
Pennsylvania ✓ Limited
Rhode Island ✓ ✓
Vermont ✓ ✓ ✓
Washington ✓ ✓ ✓
West Virginia
The below chart shows the strengths and weaknesses of how states use their medical cannabis programs in fighting the opioid epidemic. It is worth noting that while many states have included chronic pain as a qualifying condition for their program, there is no state in the country that currently recognizes opioid use disorder as an enumerated qualifying condition. The states were assessed on twelve categories relating to patient access and treatment options. The results show that even the most comprehensive programs need improvement when it comes to using medical cannabis as a tool to combat the opioid epidemic.

38 39
“ACT NOW” Draft Emergency Legislation
CHAPTER 4 “ACT NOW” DRAFT EMERGENCY LEGISLATION
“ACT NOW”
DRAFT EMERGENCY LEGISLATION
Chapter 4 WHEREAS: cannabis (marijuana) has been used as a medicine for at least 5,000 years and can be effective for serious medical conditions for which conventional medications fail to provide relief;
WHEREAS: modern medical research has shown that cannabis can slow the progression of such serious diseases as Alzheimer’s and Parkinson’s and stop HIV and cancer cells from spreading; has both anti-inflammatory and pain-relieving properties; can alleviate the symptoms of epilepsy, PTSD and multiple sclerosis; is useful in the treatment of depression, anxiety and other mental disorders; and can help reverse neurological damage from brain injuries and stroke;
WHEREAS: the World Health Organization has acknowledged the therapeutic effects of cannabinoids, the primary active compounds found in cannabis, including as an anti-depressant, appetite stimulant, anticonvulsant and anti-spasmodic, and identified cannabinoids as beneficial in the treatment of asthma, glaucoma, and nausea and vomiting related to illnesses such as cancer and AIDS;
WHEREAS: the American Medical Association has called for the review of the classification of cannabis as a Schedule I controlled substance to allow for clinical research and the development of cannabinoid-based medicines;
WHEREAS: the National Cancer Institute has concluded that cannabis has antiemetic effects and is beneficial for appetite stimulation, pain relief, and improved sleep among cancer patients;
WHEREAS: the American Herbal Pharmacopoeia and the American Herbal Products Association have developed qualitative standards for the use of cannabis as a botanical medicine;
WHEREAS: the U.S. Supreme Court has long noted that states may operate as “laboratories of democracy” in the development of innovative public policies;
WHEREAS: thirty states and the District of Columbia have enacted laws that allow for the medical use of cannabis;
WHEREAS: sixteen additional states have enacted laws authorizing the medical use of therapeutic compounds extracted from the cannabis plant;
WHEREAS THE U.S.
SUPREME COURT HAS
LONG NOTED THAT
STATES MAY OPERATE
AS “LABORATORIES
OF DEMOCRACY” IN
THE DEVELOPMENT OF
INNOVATIVE PUBLIC
POLICIES;

40 41
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS
WHEREAS: more than 20 years of state-level experimentation provides a guide for state and federal law and policy related to the medical use of cannabis;WHEREAS: accredited educational curricula concerning the medical use of cannabis have been established that meets Continuing Medical Education requirements for practicing physicians;
WHEREAS: Congress has historically prohibited the federal Department of Justice from using funds to interfere with and prosecute those acting in compliance with their state medical cannabis laws, and the Department of Justice has issued guidance to U.S. Attorneys indicating that enforcement of the Controlled Substances Act is not a priority when individual patients and their care providers are in compliance with state law, and that federal prosecutors should defer to state and local enforcement so long as a viable state regulatory scheme is in place;
The state of XXXXX introduces “Allow Medical Cannabis Treatment for New Opioid Wisdom” ACT NOW Act of 2017.
Be it enacted by the People of (State) and by their authority:
CHAPTER 4 “ACT NOW” DRAFT EMERGENCY LEGISLATION
As used in this Law, the following words shall, unless the context clearly requires otherwise, have the following meanings:
(A) “Bona fide medical professional-patient relationship” means a patient and a licensed health care professional that includes:
1. Referral from a primary care practitioner or a physical examination and review of medical history;2. An explanation of the benefits and risks of medical use of cannabis, with or without first explaining options other than medical cannabis for treatment; and3. On-going expectation of care.
B) “Cannabis” has the meaning given “marijuana” in [insert state-relevant code citation) of the General Laws.
(C) “Cannabis-derived product” means: a product other than whole-plant cannabis which is manufactured from cannabis and is intended for use or consumption by humans through means such as, but not limited to, food stuffs, extracts, oils, tinctures, topicals, and suppositories.
(D) “Cardholder” shall mean a qualifying patient, a personal caregiver, or a medical cannabis agent who possesses a valid registration card issued by the Department.
(E) ”Cultivation facility” means a business that:
1. Is registered with the Department of Agriculture; and
2. Acquires, possesses, cultivates, harvests, dries, cures, trims, and packages cannabis and other related supplies for the purpose of delivery, transfer, transport, supply, or sales to:
(a) dispensing facilities;(b) processing facilities;(c) manufacturing facilities;(d) other cultivation facilities;(e) research facilities; and/or(f ) independent testing laboratories.
(F) “Department” shall mean the Department of Public Health of (STATE), or its successor agency.
(G) “Dispensing facility” shall mean a business that:
1. is registered with the Department; and
SECTION 2.
Definitions
SECTION 1.
Purpose and Intent
The citizens of (State) intend that there should be no criminal or civil penalty under state law for qualifying patients who use cannabis as a medical treatment or for the personal caregivers who may assist those patients, the physicians and healthcare professionals who certify patients as qualifying for medical use, or the individuals who provide medical cannabis to qualified patients or otherwise participate in accordance with state law and regulations in the medical cannabis program, as defined herein.
The purpose of this act is to:
(A) provide legal and civil protections to persons with medical conditions, including chronic pain and opioid use disorder, who engage in the use of cannabis to alleviate the symptoms of a medical condition under the supervision of a medical professional; and
(B) allow for the regulated cultivation, processing, manufacture, delivery, distribution and possession of cannabis as permitted by this chapter;

42 43
MEDICAL MARIJUANA ACCESS IN THE UNITED STATES CHAPTER 4 “ACT NOW” DRAFT EMERGENCY LEGISLATION
(L) “Medical cannabis agent” shall mean an employee, staff volunteer, officer, or board member of a “medical cannabis establishment.”
(M) “Medical cannabis establishment” shall mean an entity, as defined by State law, registered under this law including medical cannabis:
1. Cultivation facilities;
2. Processing facilities;
3. Manufacturing facilities;
4. Independent testing laboratories;
5. Dispensing facilities; and
6. A business that is authorized to operate more than one of the types of businesses listed in (K)(1)-(5).
(N) “Medical cannabis establishment registration certificate” means a registration certificate that is issued by the Department pursuant to authorize the operation of a medical cannabis establishment pursuant to this statute.
(O) “Medical use of cannabis” shall mean the acquisition, cultivation, possession, processing, manufacturing, transfer, transportation, sale, distribution, dispensing, administration, or home delivery of cannabis and/or cannabis derived products for the benefit of qualifying patients.
(P) “Opioid use disorder” means any condition that reflects physical or psychological dependence on opioid medicines, including but not limited to prolonged self administration, administration in doses higher than prescribed, or use for non-medical purposes.
(Q) “Ninety-day supply” means the amount of cannabis that a qualifying patient or his/her personal caregiver may presumptively possess for the qualifying patient’s personal medical use.
(R) “Nonresident card” means a card or other identification that:1. Is issued by a state or jurisdiction other than [State]; and2. Is the functional equivalent of a registration card.
2. acquires and possesses cannabis and cannabis-derived products for the purpose of sales, delivery transport, transfer, and distribution to:
(a) card holding qualifying patients;(b) card holding personal caregivers;(c) other dispensing facilities; and/or(d) independent testing laboratories.
(H) “Financial Hardship” means an individual who is a recipient of public health benefits, or Supplemental Security insurance payments, social security disability benefits, or who otherwise is unable to generate an income that is 300% of the federal poverty level.
(I) “Excluded felony offense” means:
1. A criminal offense for which the sentence, including any term of probation, incarceration or supervised release, was completed more than 10 years before the date of application to participate in the state medical cannabis program described herein; or
2. An offense involving conduct that would be immune from arrest, prosecution or penalty pursuant to this law.
(J) “Independent testing laboratory” shall mean a private and independent testing facility that tests cannabis and/or cannabis-derived products that are to be sold by a licensed medical cannabis establishment to identify the content of the cannabis or cannabis-derived products, including but not limited to such constitutive elements as cannabinoids, to detect the presence of any pesticides, bacteria, or other contaminants, and/or for other purposes determined by the Department.
(K) ”Manufacturing facility” means a business that:
1. Is registered with the Department; and
2. Acquires, possesses, manufactures, and packages cannabis-derived products for the purpose of delivery, transfer, transport, supply, or sale to:
a) dispensing facilities;b) other manufacturing facilities;c) processing facilities; and/ord) independent testing laboratories.
44 45
MEDICAL MARIJUANA ACCESS IN THE UNITED STATES CHAPTER 4 “ACT NOW” DRAFT EMERGENCY LEGISLATION
individuals who are exempt from State criminal and civil penalties for conduct pursuant to this Chapter.
(Z) “Restricted access area” shall mean a location where cannabis is cultivated, including open air, greenhouse, row cover, or other structure that secures the cultivating cannabis from non-cardholders or individuals authorized by the Department while obscuring the view of cannabis from any public right of way.
(AA) “Written recommendation” means a document authorizing a patient’s medical use of cannabis that is written on tamper-resistant paper and signed by a qualified medical professional. Such recommendation shall be made only in the course of a bona fide medical professional-patient relationship and shall specify the qualifying patient’s qualifying medical condition(s).
SECTION 3.
Protection from State Prosecution and Penalties for Qualified Medical Professionals
A qualified medical professional shall not be penalized under [State] law, in any manner, or denied any right or privilege, for:
(A) Advising a qualifying patient about the risks and benefits of the medical use of cannabis with or without discussing other treatment options prior to recommending cannabis; or
(B) Providing a qualifying patient with a written recommendation, based upon a full assessment of the qualifying patient’s medical history and condition, that the use of cannabis may prove beneficial for the patient’s condition(s).
(S) “Paraphernalia” means accessories, devices and other equipment that is necessary or used to assist (or facilitate) in the consumption of medical cannabis.
(T) “Personal caregiver” shall mean a person or entity including hospitals, nursing care institutions, hospices, recovery centers, or home health centers, who have agreed to assist with a qualifying patient’s medical use of cannabis.
(U) “Processing facility” means a business that:
1. Is registered with the Department; and
2. Acquires, possesses, trims, inspects, or grades cannabis or places cannabis in bulk storage or retail containers for the purpose of delivery transfer, transport, supply or sales to:
(a) dispensing facilities;(b) manufacturing facilities;(c) other processing facilities;(d) independent testing laboratory.
(V) “Qualified medical professional” is any individual authorized in the STATE to prescribe medications or any other medical professional authorized by the Department to recommend cannabis pursuant to this statute.
(W) “Qualifying medical condition” shall mean any condition for which treatment with medical cannabis would be beneficial, as determined by a patient’s qualified medical professional, including but not limited to cancer, glaucoma, positive status for human immunodeficiency virus, acquired immune deficiency syndrome (AIDS), hepatitis C, amyotrophic lateral sclerosis (ALS), Crohn’s disease, Parkinson’s disease, post-traumatic stress disorder, arthritis, chronic pain, neuropathic and other intractable chronic pain, multiple sclerosis, and opioid use disorder.
(X) “Qualifying patient” shall mean a person who has a written recommendation from a qualified medical professional for the medical use of cannabis.
(Y) “Registration card” shall mean a personal identification card issued by the Department to authorize participation in [STATE]’s medical cannabis program of a qualifying patient, personal caregiver, or medical cannabis agent. The registration card shall identify for the Department and law enforcement those
SECTION 4.
Protection From State Prosecution and Penalties for Cardholders
A cardholder shall not be subject to arrest, prosecution, or civil penalty, under (STATE) law, provided the cardholder:
(A) is in possession of his or her registration card or can produce their registration card within twenty-four hours of demand by law enforcement;
(B) if the cardholder is a patient, has no more than a 90-day supply of cannabis;
(C) if the cardholder is a personal caregiver, has no more than a 90-day supply for each qualifying patient who has designated the cardholder as a personal caregiver under this Chapter; and
(D) is acting in accordance with all the requirements of this law.
46 47
MEDICAL MARIJUANA ACCESS IN THE UNITED STATES CHAPTER 4 “ACT NOW” DRAFT EMERGENCY LEGISLATION
SECTION 7.
Discrimination Prohibited
(A) Unless a failure to do so would cause the employer to lose a monetary or licensing-related benefit under federal law or federal regulations, an employer may not discriminate against a person in hiring, termination, or any term or condition of employment, or otherwise penalize a person, based upon either of the following:
1. The person’s status as a qualifying patient, caregiver, or cardholder; or2. A qualifying patient, caregiver, or cardholder tests positive for cannabis components or metabolites,
SECTION 8.
Driving Protections
(A) A qualifying patient shall not operate, navigate, or be in actual physical control of any motor vehicle, aircraft, or motorboat while under the influence of cannabis. A qualifying patient shall not be considered to be under the influence of cannabis solely because of the detectable presence of cannabis components or metabolites.
(B) A person’s status as a qualified patient is not a sufficient basis for conducting roadside sobriety tests or the suspension of a driver’s license. The officer must have an independent, factual basis giving reasonable suspicion that the person is driving under the influence of cannabis to conduct standardized field sobriety tests.
SECTION 5.
Affirmative Defense
An individual may establish an affirmative defense to charges of violations of state law relating to cannabis through proof at trial, by a preponderance of the evidence, that their use was medical if the individual is:
(A) a qualifying patient or a personal caregiver who is not registered with the (STATE) but is in compliance with all other terms and conditions of the state law; or
(B) a qualifying patient or a personal caregiver who is in possession of more than a 90-day supply of cannabis and can demonstrate the amount possessed in excess of the 90-day supply was necessary to provide a consistent and reliable source of medical cannabis to treat the qualifying patient.
(C) a non-resident of [STATE] shall be considered a qualifying patient for this Section if they have can establish through a preponderance of the evidence that an individual authorized in their state of residence who is authorized to prescribe medications has recommended the therapeutic use of cannabis for the non-resident.
SECTION 6.
Protection Against Forfeiture and Arrest
(A) The lawful possession, cultivation, processing, transfer, transport, delivery, distribution, or manufacture of medical cannabis and/or cannabis-derived products as authorized by this law shall not result in the forfeiture or seizure of any property.
(B) No person shall be arrested or prosecuted for any criminal or civil offense solely for being in the presence of medical cannabis or its use as authorized by this law.
(C) No person shall be subject to arrest or prosecution for a marijuana offense if that person is in possession of a valid registry identification card and is in compliance with this law.
unless the individual was impaired by cannabis on the premises of the place of employment or during the hours of employment.
(B) Unless required by federal law or required to obtain federal funding, no landlord may refuse to rent a dwelling unit to a person or take action against a tenant solely on the basis of an individual’s status of a qualifying patient or cardholder under this act.
(C) For the purposes of medical care, including organ transplants, a qualifying patient’s medical use of cannabis does not constitute the use of an illicit substance or otherwise disqualify a qualifying patient from medical care.
(D) Neither the presence of cannabinoid components or metabolites in a person’s bodily fluids, nor conduct related to the medical use of cannabis by a custodial or noncustodial parent, grandparent, pregnant woman, legal guardian, or other person charged with the well-being of a child, shall form the sole or primary basis for any action or proceeding by a child welfare agency or a family or juvenile court. This subsection shall apply only to conduct in compliance with this chapter.
(E) Health care practitioners shall not disqualify or refuse to provide care for a patient due to positive urinary or blood test results indicating the presence of cannabis or cannabis metabolites including tetrahydrocannabinol, nor shall the presence of compounds of cannabis or cannabis metabolites be a reason for the cessation of care.

48 49
MEDICAL MARIJUANA ACCESS IN THE UNITED STATES CHAPTER 4 “ACT NOW” DRAFT EMERGENCY LEGISLATION
SECTION 9.
Recognition of Nonresident Cards
(A) The (STATE) and the medical cannabis dispensing facilities in this State which hold valid medical cannabis establishment registration certificates will recognize a medical cannabis registry identification card issued by another state or the District of Columbia only under the following circumstances:
1. The state or jurisdiction from which the holder or bearer obtained the nonresident card grants an exemption from criminal prosecution for the medical use of cannabis;2. The nonresident card has an expiration date and has not yet expired;3. The holder or bearer of the nonresident card signs an affidavit in a form prescribed by the Department which sets forth that the holder or bearer is entitled to engage in the medical use of cannabis in his or her state or jurisdiction of residence; and4. The holder or bearer of the nonresident card is in possession of no more than a 90-day supply of cannabis.
(B) For the purposes of the reciprocity described in this section:
1. The amount of medical cannabis that the holder or bearer of a nonresident card is entitled to possess in his or her state or jurisdiction of residence is not relevant; and2. Under no circumstances, while in this State, may the holder or bearer of a nonresident card possess cannabis for medical purposes in excess of a 90-day supply of cannabis.
SECTION 10.
Limitations of Law
(A) Nothing in this law requires any physician to recommend the use of medical cannabis for a patient.
(B) Nothing in this law requires any accommodation of on-site medical use of cannabis in a place of employment, school bus or on school grounds or in any youth center, or in any correctional facility.
(C) Nothing in this law supersedes (STATE) law prohibiting the possession, cultivation, processing, manufacture, transport, distribution, or sale of cannabis for nonmedical purposes.
(D) Nothing in this law prohibits any place of employment from creating accommodations for use of medical cannabis.
(E) Nothing in this law authorizes personal caregivers to
consume medical cannabis acquired for a qualifying patient that they serve.
(F) Nothing in this law shall prohibit a private or public healthcare insurance provider from offering policies that cover the medical use of cannabis under this chapter.
(G) Nothing in this law prevents an individual who is on probation or parole from participating in this program, including individuals convicted of excluded felony offense
SECTION 11.
Department to Define Presumptive 90-Day Supply for Qualifying Patients
A) Within 120 days of the effective date of this law, the Department shall issue regulations defining the quantity of cannabis that may reasonably be presumed to be a ninety-day supply for qualifying patients, based on the best available medical evidence.
(B) This amount shall determine that amount of medical cannabis a qualifying patient or their personal caregiver may possess.
SECTION 12.
Registration of Medical Cannabis Establishments
(A) Within 120 days of the effective date of this law, the Department shall establish a method for licensing medical cannabis establishments and begin accepting applications for medical cannabis establishments to register with the Department. Medical cannabis establishments must register with the Department pursuant to this method.
(B) Not later than ninety days after receiving an application for a medical cannabis establishment, the department shall license the medical cannabis establishment if:
1. The prospective medical cannabis establishment has submitted:
(a) An application fee in an amount to be determined by the Department or Department of Agriculture consistent with Section 19 of this law.(b) An application, including:
(i) the legal name and physical address of the establishment; and(ii) the name, address and date of birth of each principal officer and board member.

50 51
MEDICAL MARIJUANA ACCESS IN THE UNITED STATES CHAPTER 4 “ACT NOW” DRAFT EMERGENCY LEGISLATION
SECTION 13.
Registration of Medical Cannabis Agents
(c) Operating procedures consistent with Department rules for oversight.
2. None of the principal officers or board members has served as a principal officer or board member for a medical cannabis establishment that has had its registration certificate or license revoked.
(C) In the first year after the effective date, the Department shall issue registrations for up to [XXX] medical cannabis establishments, provided that at least one dispensing facility shall be located in each county. If a county has more than 1,000 qualifying patients, an additional dispensary shall be established for each additional 1,000 patients residing in the county. In the event the Department determines in a future year that the number of dispensing facilities is insufficient to meet patient needs, the Department shall have the power to increase the number of registered medical cannabis dispensing facilities in the state, or raise the limit of medical cannabis dispensing facilities in a county.
(D) A medical cannabis establishment registered under this section shall not be penalized, and its registered medical cannabis agents shall not be penalized or arrested under [STATE] law for acquiring, possessing, cultivating, processing, transferring, transporting, selling, distributing, or dispensing cannabis and cannabis derived products to qualifying patients who are cardholders or their personal caregivers who are cardholders.
(E) The Department shall create rules to facilitate the home delivery of medical cannabis and cannabis-derived products from a dispensing facility to a qualifying patient or personal caregiver.
(A) A medical cannabis agent shall be registered with the Department before volunteering or working at a medical cannabis establishment.
(B) A medical cannabis establishment must apply to the Department for a registration card for each affiliated medical cannabis agent by submitting the name, address, and date of birth of the agent.
(C) A registered medical cannabis establishment shall notify the department within one business day if a medical cannabis agent ceases to be associated with the facility, and the agent’s registration card shall be immediately revoked.
SECTION 14.
Patient Cultivation Registrations
(A) The Department shall issue a cultivation registration to a qualifying patient or their personal caregiver. No more than 10 qualified patients may collectively cultivate, and each participating patient must obtain a cultivation registration. The Department may deny a registration based on the provision of false information by the applicant. Such registration shall allow the qualifying patient or their personal caregiver to cultivate an area of limited square footage of plant canopy, sufficient to maintain a 90-day supply of cannabis, and shall require cultivation and storage only in a restricted access area.
(B) The Department shall issue regulations consistent with this section within 120 days of the effective date of this law. Until the department issues such final regulations, the written recommendation of a qualifying patient’s physician shall constitute a limited cultivation registration.
(C) A qualifying patient or personal caregiver shall not be considered to be in possession of more than a 90-day supply at the location of a restricted access area used collectively by more than one patient, so long as the total amount of cannabis within the restricted access area is not more than a 90-supply for all the participating qualifying patients. A copy of each qualifying patient’s written recommendation shall be retained at the shared cultivation facility.
SECTION 15.
Medical Cannabis Registration Cards for Qualifying Patients and Designated Caregivers
(A) A qualifying patient may apply to the Department for a single or multiple-year medical cannabis registration card by submitting:
1. Written certification from a physician; and2. An application, including:
(a) Name, address unless homeless, and date of birth; and(b) Name, address, and date of birth of the qualifying patient’s personal caregiver, if any.
(B) A physician may deem a card valid for one year or two years.
(C) Until the Department begins to issue registration ID cards, a licensed physician’s written recommendation shall provide a qualifying patient the same legal status as a cardholder.
(D) Upon receiving a medical cannabis recommendation under this section, a patient shall immediately qualify to begin use of medical cannabis and nothing in this chapter shall prohibit a qualifying patient from obtaining medical cannabis on the same date that a recommendation is issued by a health care provider.
52 53
MEDICAL MARIJUANA ACCESS IN THE UNITED STATES CHAPTER 4 “ACT NOW” DRAFT EMERGENCY LEGISLATION
SECTION 16.
Registration of Independent Testing Laboratories
(A) The Department shall establish analytic standards based on the American Herbal Pharmacopeia’s Cannabis Monograph, operational standards based on the American Herbal Products Association’s Cannabis Laboratory Operations, and certify private and independent testing laboratories to test medical cannabis and cannabis-derived products that are to be sold by a licensed medical cannabis establishment.
(B) Such a laboratory must be able disclose method used to determine test results and must be able to accurately determine the following for all medical cannabis and cannabis-derived products sold by medical cannabis:
1. Active ingredient identification2. Contaminants3. Potency.
(C) Such a laboratory must be certified/accredited by a third-party, nonprofit, impartial organization.
(D) The Department shall establish within 120 days of the effective date of this law an application process for the registration of independent testing laboratories.
SECTION 17.
Creation of an Advisory Committee on Medical Cannabis
(A) Within 120 days of the effective date of this law, the Director of the Department shall create the Advisory Committee on Medical Cannabis (Committee), consisting of 11 members to be appointed by the Director.
(B) The Director shall appoint as members of the Committee: at least one person who possesses a qualifying patient registry identification card, at least one person who is a designated
A healthcare practitioner’s recommendation will remain valid as a method to participate in the medical cannabis program until the application for a registration card is approved or denied by the Department.
(E) The Department shall issue any rules necessary for how an employee of a hospice provider, nursing, or medical facility providing care to a qualifying patient may serve as a personal caregiver for the purposes of administering medical cannabis to a qualifying patient.
(F) The Department may assess a reasonable fee of no more than twenty-five dollars ($25) to those seeking to obtain a registration card. Notwithstanding, no fee shall be assessed for any patient who is determined by the Department to have a financial hardship.
primary caregiver of one or more qualifying patients, at least one person who is an officer, board member, or other responsible party for a licensed medical cannabis dispensing facility, and at least one person who is a licensed medical professional with knowledge of and experience with treating patients with medical cannabis; provided that the Director shall appoint of an officer, board member, or other responsible party for a licensed medical cannabis dispensing facility within 270 days of the effective date of the this law. The Director shall appoint nine members of the Committee within 120 days of the effective date of this law, and shall appoint an additional 2 members to the Committee within 270 days of the effective date of this law
(C) The Committee shall advise the director on the administrative aspects of the [STATE] Medical Cannabis Program, review current and proposed administrative rules of the program, and provide annual input on the fee structure of the program.
(D) The Committee shall meet at least four times per year, at times and places specified by the Director.
(E) The Department shall provide staff support to the committee.
(F) All agencies of state government are directed to assist the Committee in the performance of its duties and, to the extent permitted by laws relating to confidentiality, to furnish information and advice that the members of the committee consider necessary to perform their duties.
(G) Committee members shall serve a term of four years; provided that in order to maintain five of the members initially appointed to the Committee, as determined by the Director at the time of appointment, shall serve terms of two years. Appointments to fill vacancies shall be appointed by the Director no later than 30 days prior to the end of a term of a current Director, or within 30 days of a resignation or vote of removal of a Committee member by a three-quarters majority vote of the other members of the Committee.
SECTION 18.
Product Safety
(A) The Department will adopt product safety standards for the cultivation, processing, manufacturing, labeling, testing, and distribution of cannabis based on the American Herbal Products Association’s Recommendations to Regulators and determine a comprehensive plan for the inspection, oversight, and enforcement of such guidelines.

54 55
MEDICAL MARIJUANA ACCESS IN THE UNITED STATES CHAPTER 4 “ACT NOW” DRAFT EMERGENCY LEGISLATION
SECTION 21.
Research and Development
(A) The Department shall gather objective scientific research regarding the efficacy of administering cannabis and its components as part of medical treatment.
(B) There is established within the state treasury the Medical Cannabis Research and Development Fund. The fund shall be expanded at the discretion of the director of health:
1. To develop and investigate new methods of cannabis production, preparation, and delivery methods of medical cannabis and towards observational and clinical trials; and2. The fund shall consist of all monies derived from fees collected pursuant to section 19.
(C) The department shall issue a publicly available annual report detailing the investments and projects of the Medical Cannabis Research and Development Fund and the research gathered.
(A) Medical cannabis businesses shall pay an excise tax of no greater than 7% on the gross receipts of medical cannabis sold to a qualifying patient or to a personal caregiver, but shall not pay a higher tax than businesses of comparable activity and size.
1. Medical facilities that produce cannabis exclusively for medical use shall not be subject to excise tax.
(B) Nothing in this chapter shall prevent a medical cannabis business from implementing a sales tax on medical cannabis, however this tax rate shall not exceed [insert states applicable tax for over the counter medications].
(C) If a state has a non-medical cannabis program, medical patients shall be exempt from any applicable sales tax.
SECTION 20.
TaxationSECTION 19.
Implementation of Regulations and Fees
(A) Within 120 days of the effective date of this law, the Department, with the Department of Agriculture, shall issue regulations for the implementation of Sections 15 through 22 of this Law.
(B) The Department shall create a Merit Based Approval Process, to solicit the best applications for Medical Cannabis Establishments that include solutions to foreseeable environmental, product safety, public safety, and labor & employment issues.
(C) The Department shall set application fees for medical cannabis establishments so as to defray the administrative costs of the medical cannabis program and thereby make this law revenue neutral.
(D) The Department shall establish different categories of medical cannabis establishment agent registration cards, including, without limitation, criteria for mandatory training and certification for each of the different types of medical cannabis establishments at which such an agent may be employed or volunteer.
(E) Licensing fees shall be on a sliding scale based on the projected and/or annual gross of the medical cannabis establishment.
(F) Until the approval of final regulations, written certification by a physician shall constitute a registry identification card for a qualifying patient.
(G) Until the approval of final regulations, a certified mail return receipt showing compliance with Section 12 (A) (2) (b) above by a qualifying patient, and a photocopy of the application, shall constitute a registry identification card for that patient’s personal caregiver.
(H) The Department shall issue regulations for continuing education requirements for healthcare practitioners that at provide for at minimum 2.0 hours concerning dosing methods, preparations and interactions with other substances including opioids.
SECTION 22.
Confidentiality
(A) The Department shall maintain a confidential list of the persons issued medical cannabis registry identification cards. Individual names and other identifying information on the list shall be exempt from the provisions of (STATE) Public Records Law, and not be subject to disclosure, except to employees of the department in the course of their official duties.
(B) It shall be a crime, punishable by up to one hundred eighty (180) days in jail and a one thousand dollar ($1,000) fine, for any person, including an employee or official of the department or another state agency or local government, to breach the

56 57
MEDICAL MARIJUANA ACCESS IN THE UNITED STATES CHAPTER 4 “ACT NOW” DRAFT EMERGENCY LEGISLATION
SECTION 23.
Effective Date
(A) This law shall be effective [MONTH DAY, YEAR].
(A) The provisions of this law are severable, and if any clause, sentence, paragraph, or section of this measure, or an application thereof, shall be adjudged by any court of competent jurisdiction to be invalid, such judgment shall not affect, impair, or invalidate the remainder thereof but shall be confined in its operation to the clause, sentence, paragraph, section, or application adjudged invalid.
SECTION 24.
Severability
confidentiality of information obtained pursuant to this chapter. Notwithstanding this provision, the Department employees may notify law enforcement about falsified or fraudulent information submitted to the department.
(C) Non-public data maintained by the Department may not be used for any purpose not provided for in this Act, and may not be combined or linked in any manner with any other list, dataset, or database.

58
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS
4. EM ILITATIBUS EAQUE OCCUMEcatempo riasse reptus min nos dem est lamet quid que porit libus. Riberna turion nat. Od ut quis dis velit et ad que voluptis reperat emporeperem ipsam est etur, quia nonsectaspid molorenda quatis sequissunt idi arionseque asit odias se nimporu pienis mollab ipsanihillab id magnis enducipsapis alit ipietur? Quiatio occus non perovid magnis am faccus magnis con coreptatem andem lam eumquis eossinc tiatur? Em et hita siminis velessunt, est es re nobit eost volesti onsendes digenducimo doluptati dolorum harcia nusandis dolessus sam rerovident hitia m quae et et experibus comnimusam alignatquiam int dolore nem volento blandicabor repudae sint verio optatem porumque parchillecae parum reped ut ipsa nihici aspiciati nitium liti aut et porit, ommos moluptatior autem velitatianis im et post illaut apedion comni arum dersperum dolupta musdam que quodio. Ut et odis ea nus.
Derorepel est re, cum aut laut vel is autem cuptat et earibus, am, et quis ea conecul laboribus, offic tempor sed quo maxime prepuda essint ut eic tem hicatur, quat laccum audamusa cor aut est, corem gentureptur simpore corunt re core non non re prae resendero cus ate porro cor sunt, dam, eicto temperum faccusam idesseq uatures aceriaeperum faccus aut et ut officimus eiunt pa qui oditaque quidendus dolut minum qui vent eicit lab intus.
Em ilitatibus eaque occum ut dolor rehent quamentem ad qui totatur recullu ptibus voluptae seque volore rectin pliquid quis mosam utes et arit, ommollores conse essitio nsequae aut ut ea que quam vollupt aerorep ediscipsant volupti nemquia adi quis doluptis esectuuae excera dollicatusam dit excero denture pernam, solestibus nostisciam facee pelest qui raectat ioresti omnihit preium il ipid modiore volupti asitat occum quatiissam, sam, officti as maximusam, a sim ad ut atenihilici doluptur? dolupta nonse a doluptiat.
It eos enis di dipsum ipsam eum iurAximin comniet 5 12 85 45 33Tio blaborendi 12 4 3 2,5 0,8Aximin comniet 5 12 85 45 33Blaborendi 7 4 12 2,5 0,8Atio blaborendi 12 6 3 0,5 7
Popiska k obrázkům, tabulkám a grafům
aut lam nusam rature rem aut fugia cum simintis quodigentore mos assero ex es quam facerferum que eiumet ex etus, sitio to omniae restibus atatur, audam adi cuptas utemqui corro dolorehend molupta quiamus si omnime peligendae pro eumque con cuptasp idundhil exceria vitem rem.
RITAT ET MAXIMAG NIHITAE NE NIMET INCTEM SEQUI TEM REPELIG ENITIA DITIA VOLESEQUAM EOST LANDAM QUODIGENT VOLUTEMQUUNT FUGITATUM VOLOREPELIA QUAMUS AUT AUT RE PELIT AUT HARIO ESSITISINUM HARUM VIT
59
REGULATORY ACTIONS
Chapter 5CHAPTER 5 REGULATORY ACTIONS
Regulatory Actions
PROCLAMATION OF A STATE OF EMERGENCY
WHEREAS: between April 2016 and April 2017 over 65,000 individuals lost their lives to drug overdose, with [STATE NUMBER OF DEATHS] occurring in [STATE];
WHEREAS: one in three Americans suffer from some form of pain including an estimated 25.3 million adults who experience chronic pain that has lasted for at least three months and nearly 40 million adults who suffer from severe pain;
WHEREAS: the primary course of pain management involves the prescription of opiate based therapies which has resulted in 259 million annual prescriptions written for opioids, which is more than enough to give each adult American their own bottle of pills;
WHEREAS: the opioid epidemic continues to affect communities, devastate families, and overwhelm law enforcement, healthcare, and social service providers;
WHEREAS: chronic pain and opioid use disorders are devastating life threatening chronic medical conditions and our state needs to improve access to treatments, including medical cannabis, that support recovery and save lives;
WHEREAS: there is a growing body of domestic and international evidence that indicates that medical cannabis can be effective in managing the symptoms of chronic pain, including studies that have appeared in the Journal of the American Medical Association and the National Academies of Sciences, Engineering and Medicines;
WHEREAS: in states with medical cannabis programs, data has shown a 25% reduction in the rate of opioid-related deaths;
WHEREAS: access to safe and effective medicines can help alleviate the opioid crisis;
WHEREAS: the severity and magnitude of this epidemic make it a condition of public health importance that is beyond the timely and effective response and recovery capability of local resources, and emergency assistance is needed; and
THE OPIOID EPIDEMIC
CONTINUES TO AFFECT
COMMUNITIES,
DEVASTATE FAMILIES,
AND OVERWHELM
LAW ENFORCEMENT,
HEALTHCARE, AND
SOCIAL SERVICE
PROVIDERS;

60 61
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS CHAPTER 5 REGULATORY ACTIONS
WHEREAS: a statewide response under [Cite to State’s Public Health Funding Code], coordinated by the Department of Health is need to fully address this condition of public health importances.
NOW, THEREFORE, on this ______ Day of ______, [Insert Governor’s Name], Governor of the State [STATE NAME], in accordance with the authority vested in me by the [STATE] Constitution and statutes, HEREBY PROCLAIM A STATE OF EMERGENCY.
IT IS HEREBY ORDERED THAT:
1. The Department of Health coordinate a statewide response to the opioid crisis that includes the medical use of cannabis to manage chronic pain and opioid use disorder.
2. [STATE] Department of Health shall adopt the 2016 guidelines of the Centers for Disease Control entitled “Prescribing Opioids for Chronic Pain” which recommends against discriminatory testing for tetrahydrocannabinol in pain patients and inform all medical professionals registered in the state of this action.
3. The Department of Health through its website shall make available a minimum of 4.0 hours of continuing education materials to health care practitioners that relate to the prescribing of opioids, opioids interaction with cannabis, the medical use of cannabis, cannabis and cannabinoids as a treatment option for chronic pain and opioid use disorder, and the endocannabinoid system.
4. The Department of Health will educate all medical professionals with the ability to recommend medical cannabis according to State law about their rights to do so and the required documentation to enroll their patients in the State program.
5. The State legislative bodies pass legislation to remove barriers to patient enrollment in the medical cannabis program.
I FURTHER DIRECT that as soon as hereafter possible, this proclamation be filed in the Office of the Secretary of State and that widespread publicity and notice be given of this proclamation.
IN WITNESS WHEREOF I have hereunto set my hand and caused the Great Seal of the State of [STATE] to be affixed this _____ day of [MONTH] 201_.
_____________Governor[STATE]
THE DEPARTMENT
OF HEALTH WILL
EDUCATE ALL MEDICAL
PROFESSIONALS
WITH THE ABILITY TO
RECOMMEND MEDICAL
CANNABIS ACCORDING
TO STATE LAW ABOUT
THEIR RIGHTS TO DO
SO AND THE REQUIRED
DOCUMENTATION TO
ENROLL THEIR PATIENTS
IN THE STATE PROGRAM.

62
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS
4. EM ILITATIBUS EAQUE OCCUMEcatempo riasse reptus min nos dem est lamet quid que porit libus. Riberna turion nat. Od ut quis dis velit et ad que voluptis reperat emporeperem ipsam est etur, quia nonsectaspid molorenda quatis sequissunt idi arionseque asit odias se nimporu pienis mollab ipsanihillab id magnis enducipsapis alit ipietur? Quiatio occus non perovid magnis am faccus magnis con coreptatem andem lam eumquis eossinc tiatur? Em et hita siminis velessunt, est es re nobit eost volesti onsendes digenducimo doluptati dolorum harcia nusandis dolessus sam rerovident hitia m quae et et experibus comnimusam alignatquiam int dolore nem volento blandicabor repudae sint verio optatem porumque parchillecae parum reped ut ipsa nihici aspiciati nitium liti aut et porit, ommos moluptatior autem velitatianis im et post illaut apedion comni arum dersperum dolupta musdam que quodio. Ut et odis ea nus.
Derorepel est re, cum aut laut vel is autem cuptat et earibus, am, et quis ea conecul laboribus, offic tempor sed quo maxime prepuda essint ut eic tem hicatur, quat laccum audamusa cor aut est, corem gentureptur simpore corunt re core non non re prae resendero cus ate porro cor sunt, dam, eicto temperum faccusam idesseq uatures aceriaeperum faccus aut et ut officimus eiunt pa qui oditaque quidendus dolut minum qui vent eicit lab intus.
Em ilitatibus eaque occum ut dolor rehent quamentem ad qui totatur recullu ptibus voluptae seque volore rectin pliquid quis mosam utes et arit, ommollores conse essitio nsequae aut ut ea que quam vollupt aerorep ediscipsant volupti nemquia adi quis doluptis esectuuae excera dollicatusam dit excero denture pernam, solestibus nostisciam facee pelest qui raectat ioresti omnihit preium il ipid modiore volupti asitat occum quatiissam, sam, officti as maximusam, a sim ad ut atenihilici doluptur? dolupta nonse a doluptiat.
It eos enis di dipsum ipsam eum iurAximin comniet 5 12 85 45 33Tio blaborendi 12 4 3 2,5 0,8Aximin comniet 5 12 85 45 33Blaborendi 7 4 12 2,5 0,8Atio blaborendi 12 6 3 0,5 7
Popiska k obrázkům, tabulkám a grafům
aut lam nusam rature rem aut fugia cum simintis quodigentore mos assero ex es quam facerferum que eiumet ex etus, sitio to omniae restibus atatur, audam adi cuptas utemqui corro dolorehend molupta quiamus si omnime peligendae pro eumque con cuptasp idundhil exceria vitem rem.
RITAT ET MAXIMAG NIHITAE NE NIMET INCTEM SEQUI TEM REPELIG ENITIA DITIA VOLESEQUAM EOST LANDAM QUODIGENT VOLUTEMQUUNT FUGITATUM VOLOREPELIA QUAMUS AUT AUT RE PELIT AUT HARIO ESSITISINUM HARUM VIT
63
RECOMMENDATIONS
Chapter 6CHAPTER 6 RECOMMENDATIONS
Recommendations
While the Trump administration has declared the opioid epidemic a “national health crisis,” the President stopped short of taking measures that would provide federal funding, leaving states to face it on their own. Furthermore, all solutions coming from his Administration and advisors ignore a core element of the crisis —the third of Americans living with chronic pain— and instead are focused on law enforcement issues and downstream measures for dealing with addiction.
It is clear that opioids alone are an inefficient way to treat the millions of Americans that suffer from chronic pain. While additional funding into treatment programs and other harm reduction measures are crucial , it is also important to make sure that new, less harmful, treatment options are available. The use of cannabis as an effective treatment for chronic pain has been documented for over 170 years, with over 9,000 patient/years of data from modern clinical studies in existence.1
In order for a state to effectively utilize medical cannabis to help mitigate the opioid crisis, existing barriers to patient access must be minimized. For 20 states, this means passing comprehensive medical cannabis laws. The ACT NOW legislation (page 38) is designed as model legislation that can be introduced in its entirety. For the 30 states, the District of Columbia, Guam, and Puerto Rico, this will mean passing portions of the ACT NOW legislation to remove barriers. In the chart in Section 3: OVERVIEW OF CURRENT STATE LAWS, Americans for Safe Access has identified the gaps in each state’s medical cannabis program.
By combining legislative and regulatory actions, states can make these changes quickly and effectively. It is our hope that legislators and regulators utilize this blueprint to evaluate and improve existing medical cannabis programs or to create them. The research is clear: increased medical cannabis program enrollment can save lives.
Our staff at Americans for Safe Access are here to help with any questions.
1 Russo, E. B., & Hohmann, A. G. (2012). Role of Cannabinoids in Pain Management. In Comprehensive Treatment of Chronic Pain by Medical, Interventional, and Integrative Approaches (pp. 181–197). New York, NY: Springer New York. http://doi.org/10.1007/978-1-4614-1560-2_18
WE HAVE A LONG WAY
TO GO TO END THE
OPIOID EPIDEMIC, BUT
ALL PARTS OF THIS
TOOLKIT CAN HELP
SAVE LIVES UPON
IMPLEMENTATION.
64
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIOID CRISIS
4. EM ILITATIBUS EAQUE OCCUMEcatempo riasse reptus min nos dem est lamet quid que porit libus. Riberna turion nat. Od ut quis dis velit et ad que voluptis reperat emporeperem ipsam est etur, quia nonsectaspid molorenda quatis sequissunt idi arionseque asit odias se nimporu pienis mollab ipsanihillab id magnis enducipsapis alit ipietur? Quiatio occus non perovid magnis am faccus magnis con coreptatem andem lam eumquis eossinc tiatur? Em et hita siminis velessunt, est es re nobit eost volesti onsendes digenducimo doluptati dolorum harcia nusandis dolessus sam rerovident hitia m quae et et experibus comnimusam alignatquiam int dolore nem volento blandicabor repudae sint verio optatem porumque parchillecae parum reped ut ipsa nihici aspiciati nitium liti aut et porit, ommos moluptatior autem velitatianis im et post illaut apedion comni arum dersperum dolupta musdam que quodio. Ut et odis ea nus.
Derorepel est re, cum aut laut vel is autem cuptat et earibus, am, et quis ea conecul laboribus, offic tempor sed quo maxime prepuda essint ut eic tem hicatur, quat laccum audamusa cor aut est, corem gentureptur simpore corunt re core non non re prae resendero cus ate porro cor sunt, dam, eicto temperum faccusam idesseq uatures aceriaeperum faccus aut et ut officimus eiunt pa qui oditaque quidendus dolut minum qui vent eicit lab intus.
Em ilitatibus eaque occum ut dolor rehent quamentem ad qui totatur recullu ptibus voluptae seque volore rectin pliquid quis mosam utes et arit, ommollores conse essitio nsequae aut ut ea que quam vollupt aerorep ediscipsant volupti nemquia adi quis doluptis esectuuae excera dollicatusam dit excero denture pernam, solestibus nostisciam facee pelest qui raectat ioresti omnihit preium il ipid modiore volupti asitat occum quatiissam, sam, officti as maximusam, a sim ad ut atenihilici doluptur? dolupta nonse a doluptiat.
It eos enis di dipsum ipsam eum iurAximin comniet 5 12 85 45 33Tio blaborendi 12 4 3 2,5 0,8Aximin comniet 5 12 85 45 33Blaborendi 7 4 12 2,5 0,8Atio blaborendi 12 6 3 0,5 7
Popiska k obrázkům, tabulkám a grafům
aut lam nusam rature rem aut fugia cum simintis quodigentore mos assero ex es quam facerferum que eiumet ex etus, sitio to omniae restibus atatur, audam adi cuptas utemqui corro dolorehend molupta quiamus si omnime peligendae pro eumque con cuptasp idundhil exceria vitem rem.
RITAT ET MAXIMAG NIHITAE NE NIMET INCTEM SEQUI TEM REPELIG ENITIA DITIA VOLESEQUAM EOST LANDAM QUODIGENT VOLUTEMQUUNT FUGITATUM VOLOREPELIA QUAMUS AUT AUT RE PELIT AUT HARIO ESSITISINUM HARUM VIT
65
SUGGESTED REFERENCES
Chapter 7CHAPTER 7 SUGGESTED REFERENCES
Suggested References
1. Abrams, D. I., Couey, P., Shade, S. B., Kelly, M. E., & Benowitz, N. L. (2011). Cannabinoid–Opioid Inter-action in Chronic Pain. Clinical Pharmacology & Therapeutics, 90(6), 844–851. http://doi.org/10.1038/clpt.2011.188
2. Abrams, D. I., Jay, C. A., Shade, S. B., Vizoso, H., Reda, H., Press, S., et al. (2007). Cannabis in painful HIV-associated sensory neuropathy: a randomized placebo-controlled trial. Neurology, 68(7), 515–521. http://doi.org/10.1212/01.wnl.0000253187.66183.9
3. Bachhuber, M. A., Saloner, B., Cunningham, C. O., & Barry, C. L. (2014). Medical cannabis laws and opi-oid analgesic overdose mortality in the United States, 1999-2010. JAMA Internal Medicine, 174(10), 1668–1673. http://doi.org/10.1001/jamainternmed.2014.4005
4. Bradford, A.C., Bradford, W. D. (2016) Medical Marijuana Laws Reduce Prescription Medication Use In Medicare Part D. Health Afairs, 35(7), 1230-1236. http://content.healthaffairs.org/content/35/7/1230
5. Bradford, AC, Bradford, W.D. (2017) Medical Marijuana Laws May Be Associated With A Decline In The Number Of Prescriptions For Medicaid Enrollees. Health Affairs. 36(5).
6. CDC. Wide-ranging online data for epidemiologic research (WONDER). Atlanta, GA: CDC, National Center for Health Statistics; 2016. Available at http://wonder.cdc.gov
7. Chou, R. (2015). Long-Term Opioid Therapy for Chronic Pain. In Response. Annals of Internal Medicine, 163(2), 148–148. http://doi.org/10.7326/L15-5109-3
8. Cottler LB, Abdallah AB, Cummings SM, Barr J, Banks R, Forchheimer R. (2011) Injury, pain and prescrip-tion opioid use among former NFL football players, Drug and Alcohol Dependence, vol. 113(3).
9. Desroches, J., & Beaulieu, P. (2010). Opioids and cannabinoids interactions: involvement in pain man-agement. Current Drug Targets, 11(4), 462–473.
10. Dowell, D., Haegerich, T., Chou, R. (2016). Center for Disease Prevention and Control. CDC Guideline for Prescribing Opioids for Chronic Pain — United States. Recommendations and Reports / March 18, 2016 / 65(1);1–49. http://www.cdc.gov/mmwr/volumes/65/rr/rr6501e1.htm
11. Federation of State Medical Boards. (2016). Model Guidelines for the Recommendation of Marijuana in Patient Care. https://www.fsmb.org/Media/Default/PDF/BRD_RPT_16-2_Marijuana_Model_Guidelines.pdf
12. Gaskin DJ, Richard P. The Economic Costs of Pain in the United States. In: Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington (DC): National Academies Press (US); 2011.

6766
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIATE CRISIS
66
CHAPTER 7 SUGGESTED REFERENCES
13. Glass, M., Dragunow, M., & Faull, R. L. (1997). Cannabinoid receptors in the human brain: a detailed anatomical and quantitative autoradiographic study in the fetal, neonatal and adult human brain. Nsc, 77(2), 299–318.
14. Herkenham, M., Lynn, A. B., Little, M. D., Johnson, M. R., Melvin, L. S., de Costa, B. R., & Rice, K. C. (1990). Cannabinoid receptor localization in brain. Proceedings of the National Academy of Sciences of the United States of America, 87(5), 1932–1936.
15. Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington (DC): National Academies Press (US); 2011. Available from: https://www.ncbi.nlm.nih.gov/books/NBK91497/ doi: 10.17226/13172
16. Johannes et al. The prevalence of chronic pain in United States adults: results of an Internet-based survey. J Pain. 11(11):1230-9. (2010); Gallup-Healthways Well-Being Index.
17. Karst, M., Salim, K., Burstein, S., Conrad, I., Hoy, L., & Schneider, U. (2003). Analgesic efect of the syn-thetic cannabinoid CT-3 on chronic neuropathic pain: a randomized controlled trial. Jama, 290(13), 1757–1762. http://doi.org/10.1001/jama.290.13.1757
18. Lichtenberg, F. R., & Sun, S. X. (2007). The Impact Of Medicare Part D On Prescription Drug Use By The Elderly. Health Afairs, 26(6), 1735-1744 doi: 10.1377/hlthaf.26.6.1735
19. Lucas, P. (2012). Cannabis as an adjunct to or substitute for opioids in the treatment of chronic pain. Journal of Psychoactive Drugs, 44(2), 125–133. http://doi.org/10.1080/02791072.2012.684624
20. Manchikanti, L., & Singh, A. (2008). Therapeutic opioids: a ten-year perspective on the complexities and complications of the escalating use, abuse, and nonmedical use of opioids. Pain Physician, 11(2 Suppl), S63–88.
21. Morel, L. J., Giros, B., & eacute, V. E. R. D. (2009). Adolescent Exposure to Chronic Delta-9-Tetrahydrocannabinol Blocks Opioid Dependence in Maternally Deprived Rats, 1–8. http://doi.org/10.1038/npp.2009.70
22. National Academies of Sciences, Engineering, and Medicine. 2017. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington, DC: The National Academies Press. https://doi.org/10.17226/24625
23. National Academies of Sciences, Engineering, Medicine, Nearly 100 Conclusions on the Health Effects of Marijuana and Cannabis-Derived Products Presented in New Report, Press Release,(Jan. 12, 2017), http://www8.nationalacademies.org/onpinews/newsitem.aspx?RecordID=24625
24. Presidential briefng (Feb 2, 2016) FACT SHEET: President Obama Proposes $1.1 Billion in New Funding to Address the Prescription Opioid Abuse and Heroin Use Epidemic. https://www.whitehouse.gov/the-press-ofce/2016/02/02/president-obama-proposes-11-billion-new-funding-address-prescription
25. Researching the Potential Medical Benefts and Risks of Marijuana, hearing before the Judiciary Subcommittee on Crime and Terrorism, Senate, 114th Cong. (2016) (Testimony of Senator Cory Booker), available at 38:29 and 41:45. http://www.judiciary.senate.gov/meetings/researching-the-potential-medi-cal-benefts-and-risks-of-marijuana
26. Reiman, A. (2009). Cannabis as a substitute for alcohol and other drugs. Harm Reduction Journal, 6, 35–35. http://doi.org/10.1186/1477-7517-6-35
27. Richard, D. J. G. P., & Richard, P. (2012). The Economic Costs of Pain in the United States. Journal of Pain, 13(8), 715–724. http://doi.org/10.1016/j.jpain.2012.03.009
28. Rudd, R., Aleshire, N, Zibbell, & J. E.,Gladden, R.M. (2015). Increases in Drug and Opioid Overdose Deaths — United States, 2000–2014. Atlanta, GA: CDC, National Center for Health Statistics. Available at http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6450a3.htm
29. Russo, E. B., & Hohmann, A. G. (2012). Role of Cannabinoids in Pain Management. In Comprehensive Treatment of Chronic Pain by Medical, Interventional, and Integrative Approaches (pp. 181–197). New York, NY: Springer New York. http://doi.org/10.1007/978-1-4614-1560-2_18
30. Shi, Yuyan. Medical marijuana policies and hospitalizations related to marijuana and opioid pain reliever. Drug & Alcohol Dependence. February 2017 (173): 144 - 150.
31. Sulak, D. (2016). Medical Cannabis As A Solution to the Opioid Epidemic. Presented at http://healer.com/live-event/
32. The White House (2016). FACT SHEET: President Obama Proposes $1.1 Billion in New Funding to Address the Prescription Opioid Abuse and Heroin Use Epidemic. https://www.whitehouse.gov/the-press-of-fce/2016/02/02/president-obama-proposes-11-billion-new-funding-address-prescription
33. Vyas, Marianne Beare et al. The use of cannabis in response to the opioid crisis: A review of the literature. Nursing Outlook. September, 2017.
34. Wallace, M., Schulteis, G., Atkinson, J. H., Wolfson, T., Lazzaretto, D., Bentley, H., et al. (2007). Dose-de-pendent efects of smoked cannabis on capsaicin-induced pain and hyperalgesia in healthy volunteers. Anesthesiology, 107(5), 785–796. http://doi.org/10.1097/01.anes.0000286986.92475.b7
35. Warren, E (2016). Letter to CDC head, Dr. Thomas Frieden. http://www.warren.senate.gov/fles/docu-ments/2016-2-8_Letter_to_CDC_re_opioid_epidemic%20research.pdf
36. Welch, S. P., & Eads, M. (1999). Synergistic interactions of endogenous opioids and cannabinoid sys-tems. Brain Research, 848(1-2), 183–190

6968
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIATE CRISIS
68
CHAPTER 7 SUGGESTED REFERENCES
DATA SOURCES FOR MICHIGAN CASE STUDY IN BARRIERS TO ACCESS
1. Ahmad FB, Rossen LM, Spencer MR, Warner M, Sutton P. Provisional drug overdose death counts. National Center for Health Statistics. 2017.
2. Association of American Medical Colleges. (2013). Michigan Physician Workforce Profile. Retrieved from http://www.aamc.org/download/152142/data/michigan.pdf
3. Bachhuber, M.A..,Saloner, B., Cunningham, C.O.., & Barry, C.L.. (2014). Medical Cannabis Laws and Opioid Analgesic Overdose Mortality in the United States. JAMA Internal Medicine, 1668-1673. doi:10.1001/jamainternmed.2014.4005
4. Gift of Life Michigan. (2017, November 1). The Waiting List. Retrieved from http://www.giftoflifemichigan.org/about-donation/waiting-list
5. Governing. (2016, December). Federal Employees By State. Retrieved from http://www.governing.com/gov-data/federal-employees-workforce-numbers-by-state.html
6. Hartwell, T.D., Steele, P.D., French, M.T., & Rodman, N.F. (1996). Prevalence of drug testing in the workplace. Monthly Labor Review, 35-48. Retrieved from Http://Www.bls.gov/mlr/1996/11/art4full.pdf
7. Thomas, L. (2016, Medical marijuana reduces use of opioid pain meds, decreases risk for some with chronic pain). University of Michigan. 22 March Retrieved from http://ns.umich.edu/new/releases/23622-medical-marijuana-reduces-use-of-opioid-pain-meds-decreases-risk-for-some-with-chronic-pain
8. Mack, J. (2017, See number of medical marijuana cardholders in your Michigan county). MLive. 24 July Retrieved from http://www.mlive.com/news/index.ssf/2017/07/see_number_of_medical_marijuan.html
9. Michigan Assisted Living Association. (2014). Getting Started as a Provider. Retrieved from http://www.miassistedliving.org/getting-started.html
10. Michigan Department of Community Health. (2007, November). Hospice and Palliative Care. Retrieved from http://www.michigan.gov/documents/Hospice_Fact_Sheet_108440_7.pdf
11. Michigan Department of Community Health. (2014). 2014: The “State” of Pain in Michigan:. Retrieved from http://www.michigan.gov/documents/lara/ACPSM_State_of_Pain_Report_to_Directors_Sept._2014_469555_7.pdf
12. Michigan Department of Corrections. (2017). Probation Supervision. Retrieved from http://www.michigan.gov/corrections/0,4551,7-119-1435_1463---,00.html
13. Ornstein, K. A., Leff, B., Covinsky, K., Ritchie, C., Federman, A. D., Roberts, L., … Szanton, S. L. (2015). The Epidemiology of the Homebound in the United States. JAMA Internal Medicine, 175(7), 1180–1186. http://doi.org/10.1001/jamainternmed.2015.1849
14. Substance Abuse and Mental Health Services Administration. (2007). Highlights for 2007 Treatment Episode Data Set (TEDS). Retrieved from http://oas.samhsa.gov/TEDS2k7highlights/TEDSHighl2k7Tbl6a.htm.
15. Talk Poverty - Center for American Progress. (2017, July 24). See number of medical marijuana cardholders in your Michigan county. Retrieved from http://www.mlive.com/news/index.ssf/2017/07/see_number_of_medical_marijuan.html.
16. U.S. Bureau of Labor Statistics. (2017, November 30). Economy at a Glance - Michigan. Retrieved from http://www.bls.gov/eag/eag.mi.htm#eag_mi.f.p.
17. United States Census Bureau. (2014). Veteran Statistics - Michigan. Retrieved from http://www2.census.gov/library/infographics/2015/comm/vets/mi-vets.pdf.

7170
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIATE CRISIS
70
UTILIZING MEDICAL CANNABIS AS TOOL TO COMBAT PAIN AND THE OPIATE CRISIS END PAIN NOT LIVES CAMPAIGN

Americans for Safe Access 1624 U Street, NW, Suite 200 Washington, DC 20009 Tel: 202.857.4272 AmericansForSafeAccess.org
Design & Layout Inspiration: Missing Element, Prague





























