Embed Size (px)
Citation preview

MEDICAL BILLING MEDICAL BILLING PROCESSPROCESS

APPOINTMENTAPPOINTMENT
PATIENT CALLS / WALKS TO THE DOCTORS OFFICE TO FIX THE APPOINTMENT

DATE OF SERVICEDATE OF SERVICE
ONCE THE APPOINTMENT IS FIXED, PATIENT COMES TO THE DOCTORS OFFICE AND FILLS THE DEMO FORMS (i.e., his address with contact #, DOB, Gender, SS#, Employer Information, policy name and number, effective date etc.) and signs the Breach of Confidentiality.

CHECK-UPCHECK-UP
DOCTOR CHECKS THE PREVIOUS MEDICAL HISTORY OF THE PATIENT AND CHEKS THE PATIENT AND DOES THE PROCEDURE AS PER THE CURRENT ILLNESS.

MEDICAL TRANSCRIPTIONMEDICAL TRANSCRIPTION
DOCTORS GIVE THE DICTATION TO THE MEDICAL TRANSCRIPTIONIST FOR MEDICAL RECORD KEEPING. (AS IT IS MENDATORY IN USA TO KEEP THE MEDICAL RECORD OF THE PATIENTS AT LEASET FOR 5 YEARS).

MEDICAL CODINGMEDICAL CODING
AFTER THE MEDICAL TRANSCRIPTION IS DONE, THE DOCUMENTS / REPORTS ARE SENT TO THE MEDICAL CODING DIVISION TO GET THE REPORTS CODED AS CPT (CURRENT PROCEDURAL TERMINOLOGY) AND ICD (INTERNATIONAL CLASSIFICATION OF DISEASE) WITH THE HELP OF CODING BOOKS AND MAINTAINING CODING GUIDELINES.

MEDICAL BILLINGMEDICAL BILLING
ONCE THE CODING IS OVER THE CODED REPORTS / SUPERBILLS COME TO THE BILLING DEPARTMENT, WHERE BELOW MENTIONED STEPS ARE FOLLOWED:

DEMO ENTRYDEMO ENTRY
DEMOGRAPHICS OF THE NEW PATIENTS ARE ENTERED INTO THE BILLING SOFTWARE AND UPDATION OF THE OLD ACCOUNS ARE DONE.

CRITICAL FIELDS – DEMO CRITICAL FIELDS – DEMO ENTRYENTRYPATIENTS INFORMATION:
1. NAME
2. DATE OF BIRTH
3. GENDER
4. SOCIAL SECURITY NUMBER (SS#)
5. ADDRESS (INCLUDING ZIP)
6. CONTACT NUMBER
7. RELATIONSHIP TO THE INSURED
8. MARITAL STATUS
INSURED’S INFORMATION:
1. ID Number
2. Name
3. Address )including Zip code)
4. Policy and Group Name
5. Insured’s Plan or Program name
6. Insured’s Date Of Birth

CLAIM GENERATION OR CLAIM GENERATION OR CHARGE ENTRYCHARGE ENTRY
ONCE THE ACCOUNT OF THE PATIENT IS CREATED IN THE BILLING SOFTWARE, CHARGE CAN BE POSTED.

CRITICAL FIELDS – CRITICAL FIELDS – CHARGE ENTRYCHARGE ENTRY
a. Is the Patient’s Condition Related to: Employment, Auto Accident, Other Accident
b. Name of Referring Physician
c. ID Number of Referring Physician
d. Diagnosis Codes
e. Prior Authorization Number (if applicable)
f. Dates of Service & Date of Hospitalization (in case of Inpatient)
g. Place and Type of Service
h. CPT
i. Modifiers (if applicable)
j. Linked Diagnosis Codes to the Procedure Codes
k. Days or Units (if applicable)

CLAIM SUBMISSIONCLAIM SUBMISSIONThere are two ways to submit the claims to the insurance companies:
1. Electronic Media Claims submission (EMC): EMC is an electronic claims processing system that enables a provider to submit his/her claims to the carrier more efficiently than the paper claims, Provider can submit claim by modem, by magnetic computer tape or by floppy diskette.
2. Paper Submission on different forms (such as CMS 1500, CMS 1450 or UB 92, ADA 992000)
Time taken by Medicare to pay a clean claim: Medicare statute provides for claims payment floors and ceilings. A floor is the minimum amount of time a claim must be held before payment. A ceiling is the maximum time allowed for processing a clean claim before Medicare owes interest to the Provider of Services.
Physicians and suppliers who file Paper Claims will not be paid before the 26 th day after the date of recei0pt of their claims. Clean claims filed Electronically will be paid not sooner than 13 days after receipt.

CLAIM ADJUDICATIONCLAIM ADJUDICATION
Processing of paper claims starts in the mailroom where the envelops are opened, attachments unstapled, and clipped to the claim. Claims are then scanned into the computer.
Processing of electronic claims begins when a file of transmitted claims is received from the clearinghouse. (The clearinghouse edits the claims before sending to the insurance companies) and is opened in the claims processing computer.

STEPS (CLAIM STEPS (CLAIM ADJUDICATION) -ADJUDICATION) -
1. The computer scans each claim for patient and policy identification and compares them with the master policy file.
Claims will be automatically rejected if the patient and subscriber names do not match exactly with the names on the master policy list. Use of nicknames or typographical errors on claims will cause rejection and return, or delay in reimbursement to the provider because the claim cannot be matched with the names on the master list.
2. Procedure codes on the claim form are matched with the policy’s master benefit list. In the case of managed care claim, both the procedures and the dates of service are checked to ensure that services performed were authorized and performed within the authorized dates of services.

CLAIM ADJUDICATION – CLAIM ADJUDICATION – Cont.Cont.
Any service determined to be a non-covered benefit is marked as an uncovered procedure or non-covered procedure and rejected for payment.
Services provided to a patient without proper authorization or that are not covered by a current authorization are marked as an unauthorized service. Patients may be billed for uncovered for non-covered procedures, but not for unauthorized services.
3. Procedure codes are cross-matched with the diagnosis codes to ensure the medical necessity of all services provided. Any service that is considered not “medically necessary” for the submitted diagnosis code may be rejected.
4. The claim is checked against common data file. The information presented on each claim is checked against the insurer’s common data file, which is an abstract of all recent claims filed on each patient. This step determines whether the patient is receiving concurrent care for the same condition by more than one provider. This function further identifies services that are related to recent surgeries, hospitalizations, or liability coverage's.

CLAIM ADJUDICATION – CLAIM ADJUDICATION – Cont.Cont.
5. A determination is made by “allowed charges”. If no irregularity or inconsistency is found on the claim, the allowed charge for each covered procedure is determined. (The allowed charges is the maximum amount the insurance company will pay for each procedure or service, according to the patient’s policy. The exact amount allowed varies according the the contract and is less than than or equal to the fee charged by the provider, Payment is never greater than the fee submitted by the provider).
6. Determination of patient’s annual deductible obligation is made. (The deductible is the total amount of covered out-of-pocket medical expenses a policyholder must incur each year before to insurance company is obligated to pay any benefits)
7. The co-payment or co-insurance requirement is determined.

CLAIM ADJUDICATION – CLAIM ADJUDICATION – Cont.Cont.
8. The Explanation of Benefits (EOB) is completed. The (EOB) form or report is a statement telling the patient or provider how the insurance company determined its share of the reimbursement. The report includes the following:
a). A list of all procedures and charges submitted on the claim form.
b). A list of any procedure submitted but not considered a benefit of the policy.
c). A list of all the allowed charges for each covered procedures.
d). The amount of the patient deductible, if any, subtracted from the total allowed charges.
e). The patient’s financial responsibility for cost sharing (co-payment for this claim.
f).The total amount payable by the insurance company on this claim.

CLAIM ADJUDICATION – CLAIM ADJUDICATION – Cont.Cont.
9. EOB and benefit check is mailed. If the claim form stated that direct payment should be made to the physician, the reimbursement check and a copy of the EOB will be mailed to the physician. This can be accomplished in one of three ways:
a). The patient signs the Authorization of Benefits Statement, Block 13 on the CMS – 1500 form.
b). The Physician marks “YES” in Block 27 on the CMS – 1500 form.
c). The Physician has signed an agreement with the insurer for direct payment of all claims.
If reimbursement is to be sent to the patient, the policyholder will received a copy of the EOB; explanation is sent to the provider by most carriers, without payment.

PAYMENTSPAYMENTS
PAYMENTS: Amount paid to the physicians against the services rendered by them to the patient.
THE SERVICES THAT ARE PROVIDED TO THE PATIENTS ARE SENT OUT TO THE INSURANCE COMPANIES IN THE FORM OF CLAIMS. THESE CLAIMS GET PAID BY THE INSURANCE COMPANIES. THE PAYMENTS ARE RECEIVED AT THE PROVIDER’S MAILING ADDRESSES AND / OR AT THE BILLING COMPANIES’ ADDRESSES. IN CASES WHEN THEY ARE RECEIVED AT THE PROFIDERS’ ADDRESSES THEN THEY ARE IN TURN FORWARDED TO THE BILLING COMPANY TO THE PAYMENT IN THEIR SYSTEM. SUCH PAYMENTS COME IN THE THE FORM OF BATCHES AND MAY HAVE BANK’S DEPOSIT SLIP OR PAYMENT LISTING WITH THEM. PAYMENTS THAT ARE RECEIVED DIRECTLY AT THE BILLING COMPANIES’ ADDRESS DO NOT HAVE THE BANK’S DEPOSIT SLIP.
SOMETIMES, IN THE CASE OF NON-PARTICIPATING PROVIDER’S, PAYMENTS ARE RECEIVED BY THE INSURED PARTIES ADDRESS AND THEY FORWARD THE PAYMENT TO THE PHYSICIAN’S ADDRESS.

DENIALSDENIALS
Claim that do not get paid, come back as Denials from the Insurance carriers. This can be due to posting errors, incorrect procedure / diagnosis codes, lack of information (medical records) while filing the claims, or missing / incomplete patient details.
Denials are broken down into two categories: In-House and Patient Responsibility.
In-House denials are the ones that require some type of correction from our part and can be resubmitted. We do not bill patient.
Patient Responsibilities are those denials that we can’t do anything to get the claim paid by the insurance company. Al we can do is, transfer the charge to the patient with the correct message code.

A/R MANAGEMENTA/R MANAGEMENT
The following guidelines are intended to assist staff who are engaged in Third Party or self follow-up. The guidelines are consistent with the Fair Debt Collection Practices Act. It is important for the billing service, as a third party involved in the billing and collection of our client’s accounts, to confirm our guidelines to the Act to the assure the protection of the billing service and it’s clients.
CAUTIONARY GUIDELINESBefore placing a follow-up call:
1. Review Insurance A/R aging report.
2. First focus on accounts with aging 120+ days and large balances, You’re your way down up to 45 days of balance outstanding.
3. For Self-Pay patients, after one statement has gone out, F/U should be done after 30 Days from the date statement was mailed.
4. Review account notes and transaction history. Make sure that the billing service is not at fault.
5. Plan what you want to say before making a call.

A/R MANAGEMENT – cont.A/R MANAGEMENT – cont.
When making Call:
1. Call between 8:00 am. and 9:00 pm. (US Time)
2. Know whom you are speaking to.
3. Identify yourself properly – do not represent yourself as calling from the Doctor’s office. You are a third party billing service (e.g. Hello, my name is ___________. I am calling from ___________ (billing service name). We are the billing service for Dr. ___________.)
4. Do not leave messages on voice mail or on answering machines that imply a problem with an account or any confidential information – you do not know who will retrieve the message. General messages to return your call is permissible.
5. When need arises to threaten a guarantor with the collection, you should always say : “We may refer your account to a collection agency or to an attorney for further collection action.” It is important to remember that any threatened collection action must be taken if there is no change in account circumstances. Not all clients will transfer account to collection, please refer to client profile before threatening with taking such action.
6. If the debtor states that an attorney is handling his debts – refrain from any future contact with the debtor and direct all communications to the attorney.

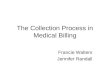
MEDICAL BILLING FLOW MEDICAL BILLING FLOW CHARTCHART

THE END