Embed Size (px)
Citation preview
Sweitzer et al.
ADHD, smoking withdrawal and inhibitory control: Results of an fMRI study with methylphenidate challenge
Supplementary Information
Supplemental Methods and Materials
Psychiatric Evaluation
Diagnostic criteria for ADHD and other psychiatric disorders were determined by a
comprehensive psychiatric evaluation conducted by a Ph.D.-level psychologist. The evaluation
included administration of a structured, computerized psychiatric screening measure, Conners’
Adult ADHD Rating Scale (CAARS; Conners et al., 1998), Conners’ Adult ADHD Diagnostic
Interview for DSM-IV (CAADID; Epstein et al, 2000), and clinical interview. ADHD
participants met all diagnostic criteria for ADHD and had age- and sex-adjusted T-scores on
relevant CAARS subscales ≥ 65. Control participants reported no history of ADHD and had T-
scores on relevant CAARS subscales ≤ 55.
Exclusion Criteria
Exclusion criteria for both groups were current significant health problems; estimated IQ
scores of < 80 measured using the Kaufman Brief Intelligence Test (K-BIT 2; Kaufman and
Kaufman, 2004), current primary Axis I disorder other than ADHD or nicotine dependence;
current use of psychoactive medications (other than ADHD pharmacotherapies among ADHD
diagnosed participants); use of smokeless tobacco; drug or alcohol abuse within the past year;
positive urine drug screen; current use of nicotine replacement therapy or other smoking
Sweitzer et al.
cessation treatment; presence of conditions contraindicated for MRI or methylphenidate; and
pregnancy among females.
Study Drug and Medication Safety
Methylphenidate (MPH) was administered via 40 mg capsules provided by two
manufacturers over the course of the study (Mallinckrodt and Watson). Placebo capsules
contained Dextrose, USP Anhydrous (provided by Medisca). Over-encapsulation of MPH and
placebo was conducted by Duke Investigational Drug Service, which also provided blinded kits.
All participants completed a 4-hr MPH safety session prior to scanning. In this session,
participants were administered 40 mg MPH and self-reported symptoms and vitals were acquired
every 30 minutes. The study physician (RD) reviewed the results of this session and cleared
participants for participation.
Participants Excluded from Analyses
A total of 633 participants were telephone screened for the study, resulting in 101 in-
person screens. Of these, 67 were enrolled in the study, and 35 were included in analyses. Of
participants not included in the analysis, 9 (n=6 ADHD, n=3 control) were lost to contact or had
scheduling difficulty; 8 exhibited a lack of MPH tolerance at the medication safety session (n=4
ADHD; n=4 control); 10 were noncompliant with study requirements (e.g. did not abstain from
smoking; tested positive for drugs; quit or substantially reduced smoking; n=6 ADHD;
4=control). An additional two ADHD participants were found to have tattoos or metal implants
post enrollment but prior to scanning. Finally, three control participants were excluded from
analysis due to excessive head motion.
Sweitzer et al.
CO and Self-Report Withdrawal
Consistent with abstinence/smoking requirements, CO levels in the SAT+PLAC,
ABS+PLAC, and ABS+MPH conditions were 17.1 (SD=8.2), 2.9 (SD=2.1), and 3.0 (SD=1.8)
ppm, respectively. On the SJWS, main effects of condition were observed for Negative Affect,
F(2,72)=8.62, p<.001, Craving, F(2,72)=87.58, p<.0001, Habit Withdrawal, F(2,72)=40.52,
p<.0001, and Appetite, F(2,72)=4.27, p<.05, with these effects being largely driven by symptoms
that were greater in the ABS as compared to SAT conditions (see Supplementary Figure S1).
MPH did not affect symptom levels differentially between the two groups compared with
ABS+PLAC.

Sweitzer et al.
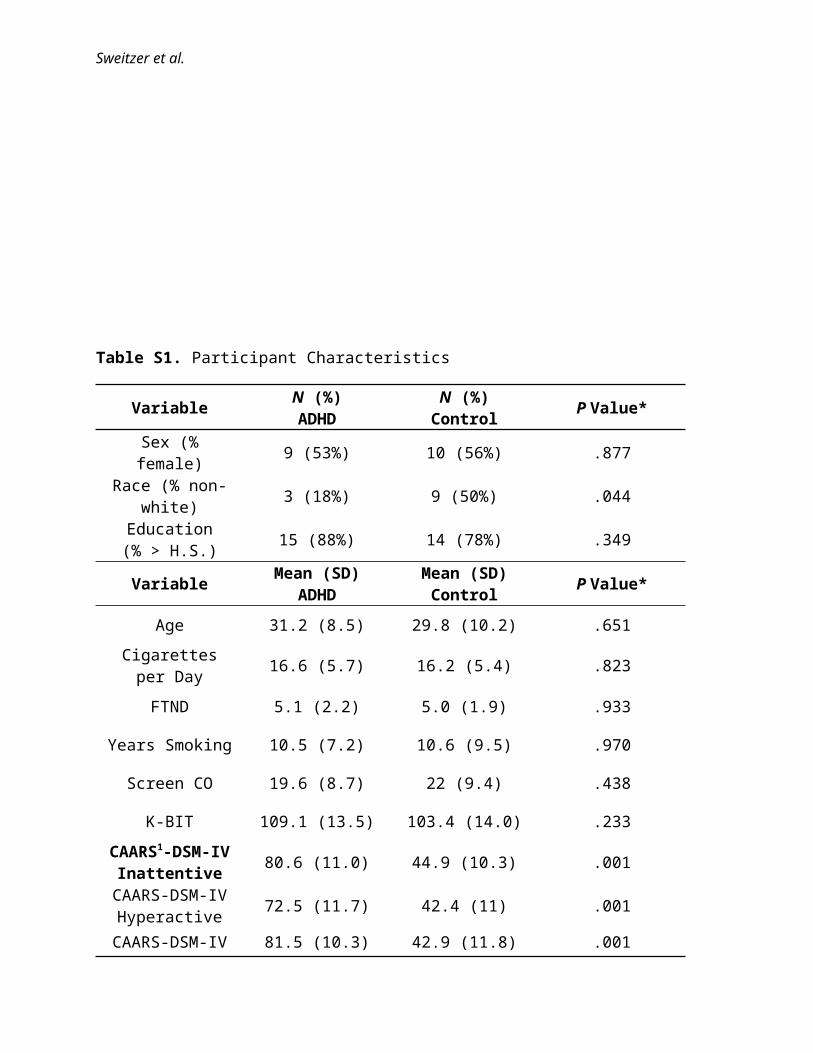
Table S1. Participant Characteristics
Variable N (%) ADHD
N (%) Control P Value*
Sex (% female) 9 (53%) 10 (56%) .877
Race (% non-white) 3 (18%) 9 (50%) .044
Education (% > H.S.) 15 (88%) 14 (78%) .349
Variable Mean (SD)ADHD
Mean (SD)Control P Value*
Age 31.2 (8.5) 29.8 (10.2) .651
Cigarettes per Day 16.6 (5.7) 16.2 (5.4) .823
FTND 5.1 (2.2) 5.0 (1.9) .933
Years Smoking 10.5 (7.2) 10.6 (9.5) .970
Screen CO 19.6 (8.7) 22 (9.4) .438
K-BIT 109.1 (13.5) 103.4 (14.0) .233
CAARS1-DSM-IV Inattentive 80.6 (11.0) 44.9 (10.3) .001
CAARS-DSM-IV Hyperactive 72.5 (11.7) 42.4 (11) .001
CAARS-DSM-IV Total 81.5 (10.3) 42.9 (11.8) .001
*P-value reflects statistical significance of chi-square or t-test as appropriate.
1Conners’ Adult ADHD Rating Scale for DSM-IV, Self-Report Version
Sweitzer et al.
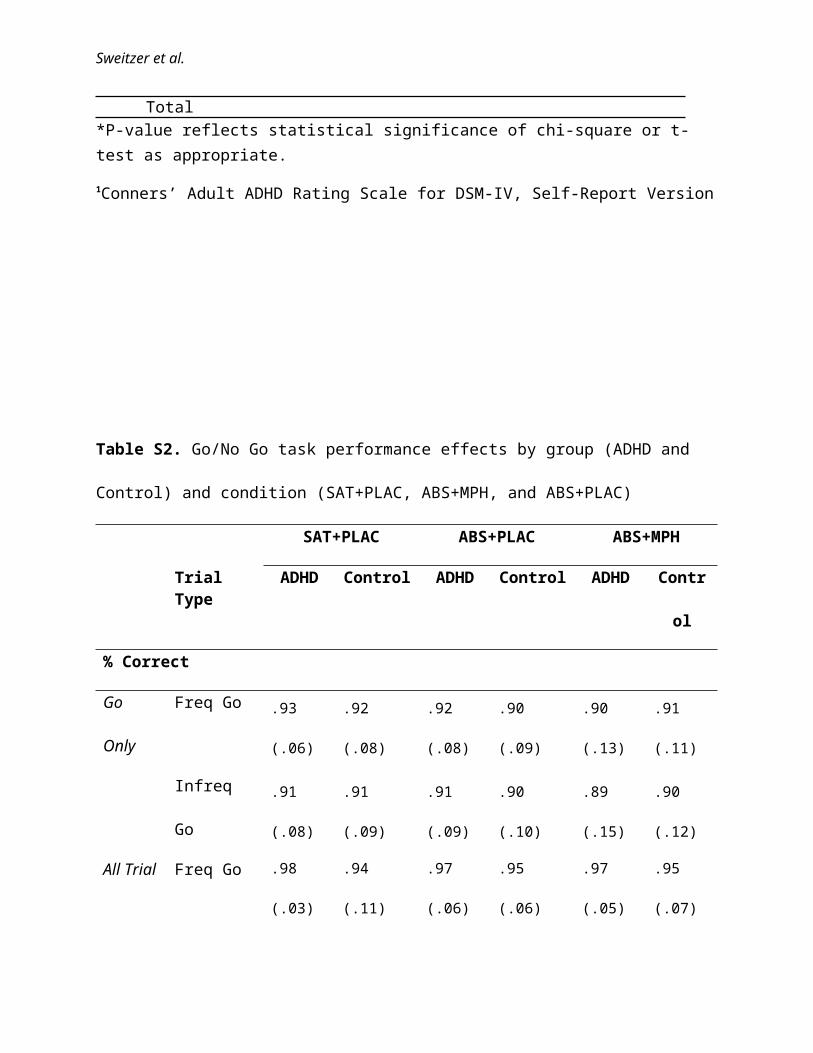
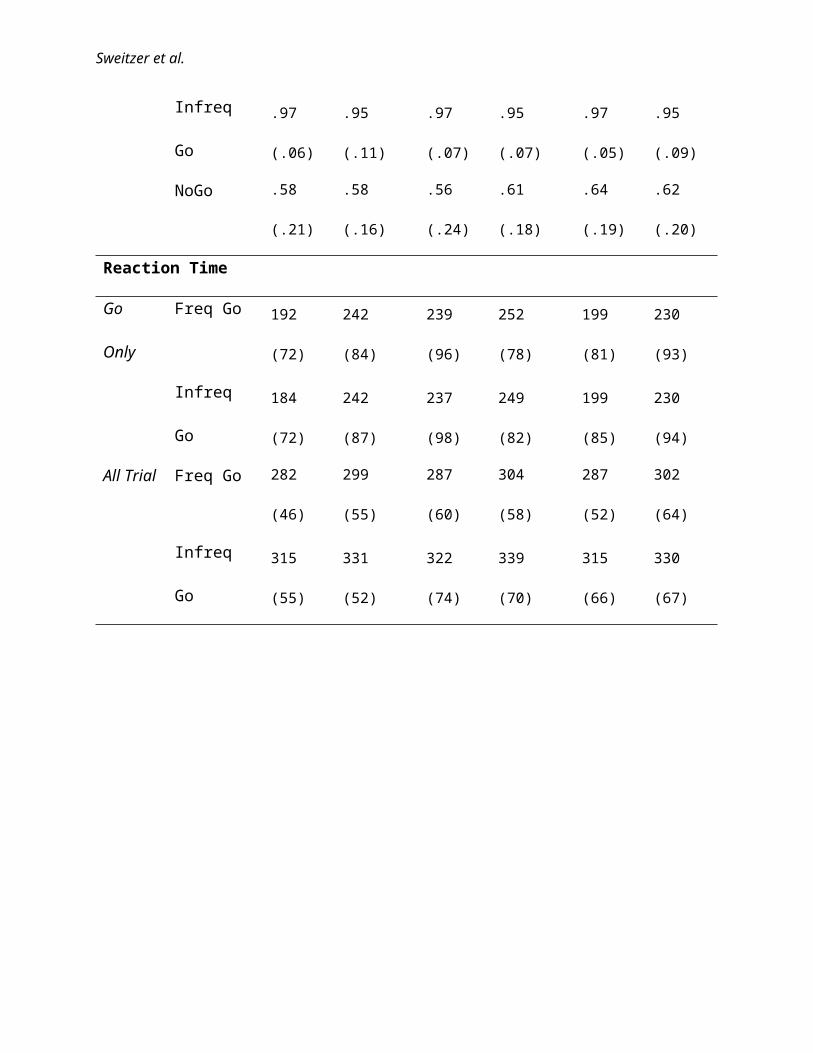
Table S2. Go/No Go task performance effects by group (ADHD and Control) and condition
(SAT+PLAC, ABS+MPH, and ABS+PLAC)
SAT+PLAC ABS+PLAC ABS+MPH
Trial Type ADHD Control ADHD Control ADHD Control
% Correct
Go Only Freq Go .93 (.06) .92 (.08) .92 (.08) .90 (.09) .90 (.13) .91 (.11)
Infreq Go .91 (.08) .91 (.09) .91 (.09) .90 (.10) .89 (.15) .90 (.12)
All Trial Freq Go .98 (.03) .94 (.11) .97 (.06) .95 (.06) .97 (.05) .95 (.07)
Infreq Go .97 (.06) .95 (.11) .97 (.07) .95 (.07) .97 (.05) .95 (.09)
NoGo .58 (.21) .58 (.16) .56 (.24) .61 (.18) .64 (.19) .62 (.20)
Reaction Time
Go Only Freq Go 192 (72) 242 (84) 239 (96) 252 (78) 199 (81) 230 (93)
Infreq Go 184 (72) 242 (87) 237 (98) 249 (82) 199 (85) 230 (94)
All Trial Freq Go 282 (46) 299 (55) 287 (60) 304 (58) 287 (52) 302 (64)
Infreq Go 315 (55) 331 (52) 322 (74) 339 (70) 315 (66) 330 (67)
Sweitzer et al.
Figure S1.
SAT+PLAC ABS+PLAC ABS+MPH01234567
ADHDControl
Hab
it W
ithdr
awal
SAT+PLAC ABS+PLAC ABS+MPH01234567
Aro
usal
SAT+PLAC ABS+PLAC ABS+MPH01234567
ADHDControl
Neg
ativ
e A
ffect
SAT+PLAC ABS+PLAC ABS+MPH01234
567
App
etite
SAT+PLAC ABS+PLAC ABS+MPH0
1
2
3
4
5
6
7ADHDControl
Som
atos
enso
ry
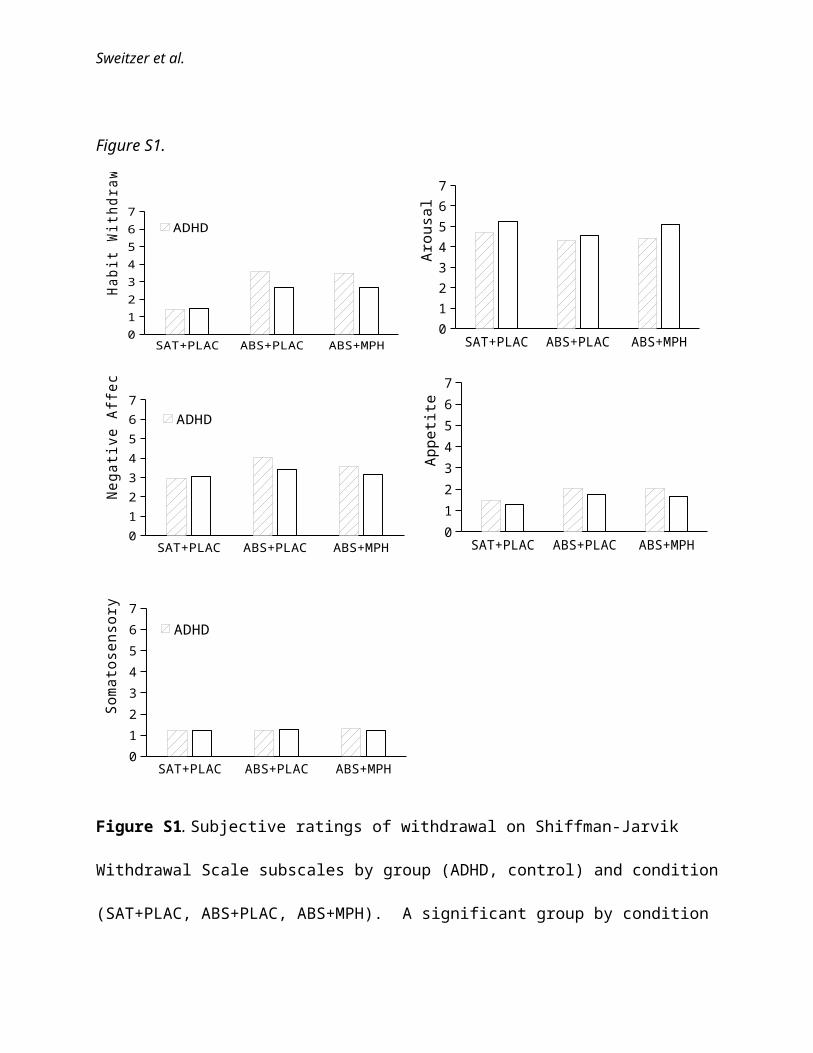
Figure S1. Subjective ratings of withdrawal on Shiffman-Jarvik Withdrawal Scale subscales by
group (ADHD, control) and condition (SAT+PLAC, ABS+PLAC, ABS+MPH). A significant
group by condition interaction was observed for Habit Withdrawal, with SAT+PLAC >
ABS+PLAC for both groups (both p’s < .001); and ADHD > Control during ABS+PLAC, t(72)
= 2.10, p < 0.05. Main effects of condition were observed for Negative Affect (p < 0.05) and
Sweitzer et al.
Appetite (p < .001); no condition or interaction effects were observed for Arousal or
Somatosensory withdrawal.
Sweitzer et al.
Figure S2.
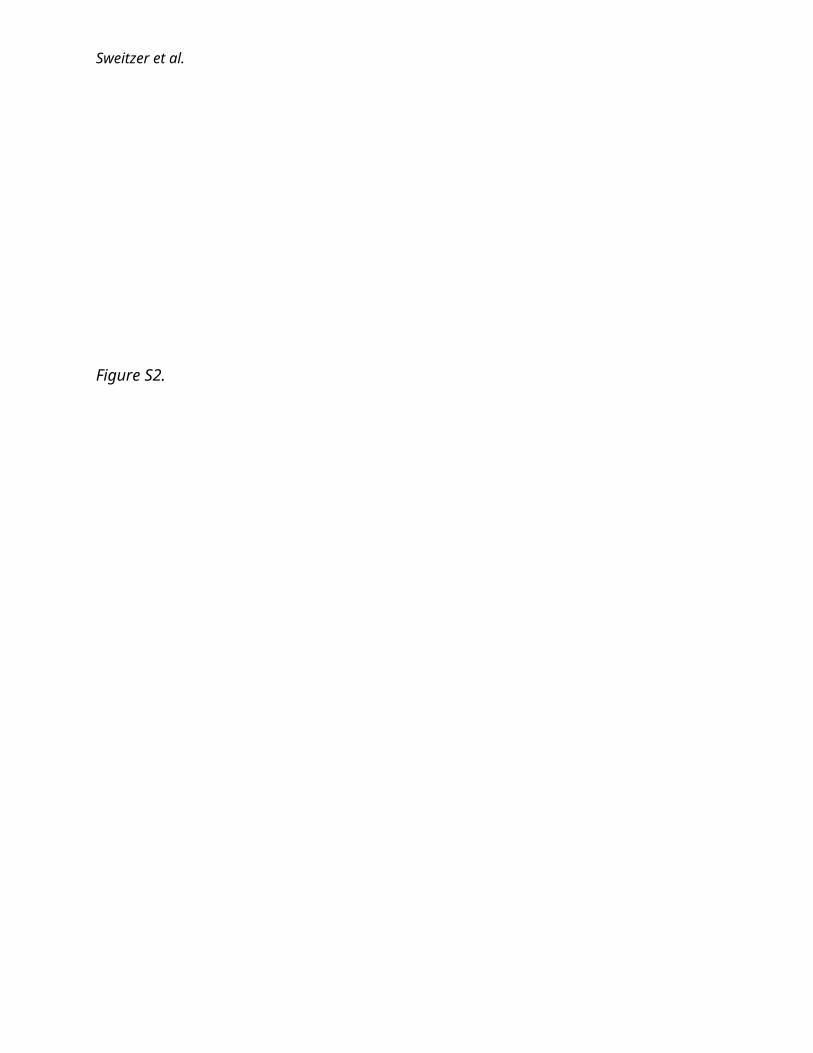
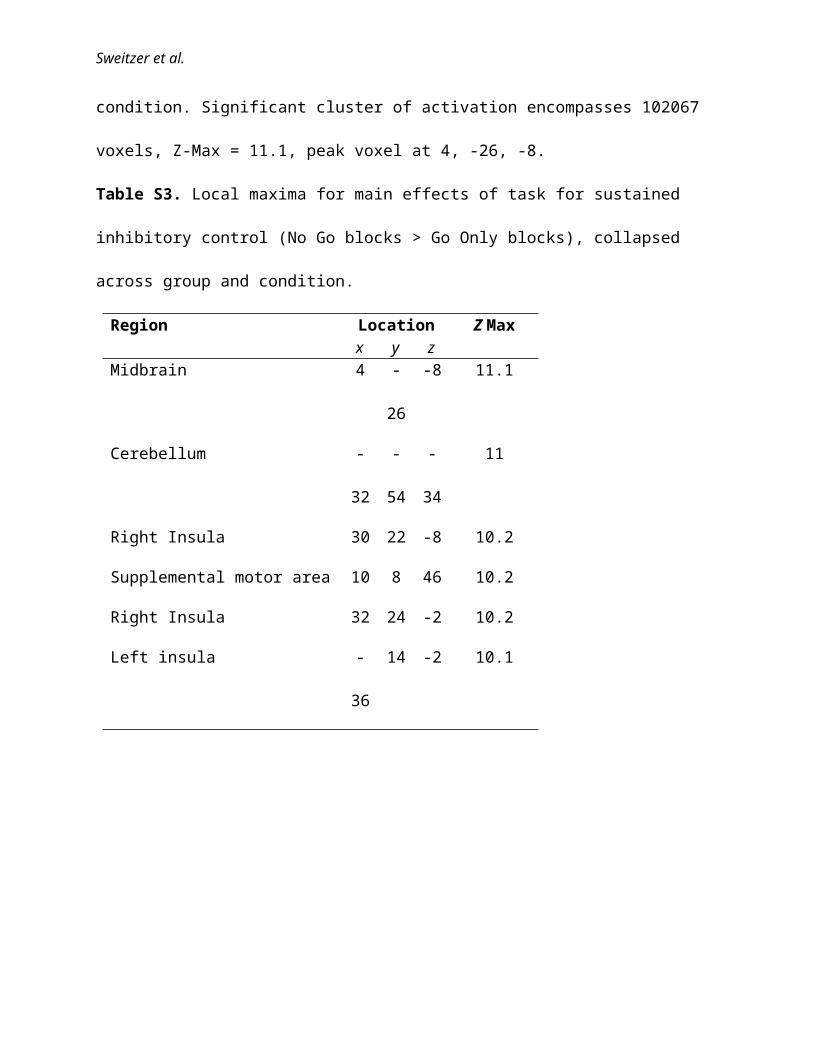
Figure S2. Main effects of task for sustained inhibitory control (No Go blocks > Go Only
blocks), collapsed across group and condition. Significant cluster of activation encompasses
102067 voxels, Z-Max = 11.1, peak voxel at 4, -26, -8.
Sweitzer et al.
Table S3. Local maxima for main effects of task for sustained inhibitory control (No Go blocks
> Go Only blocks), collapsed across group and condition.
Region Location Z Maxx y z
Midbrain 4 -26 -8 11.1
Cerebellum -32 -54 -34 11
Right Insula 30 22 -8 10.2
Supplemental motor area 10 8 46 10.2
Right Insula 32 24 -2 10.2
Left insula -36 14 -2 10.1
Figure S3.
Sweitzer et al.
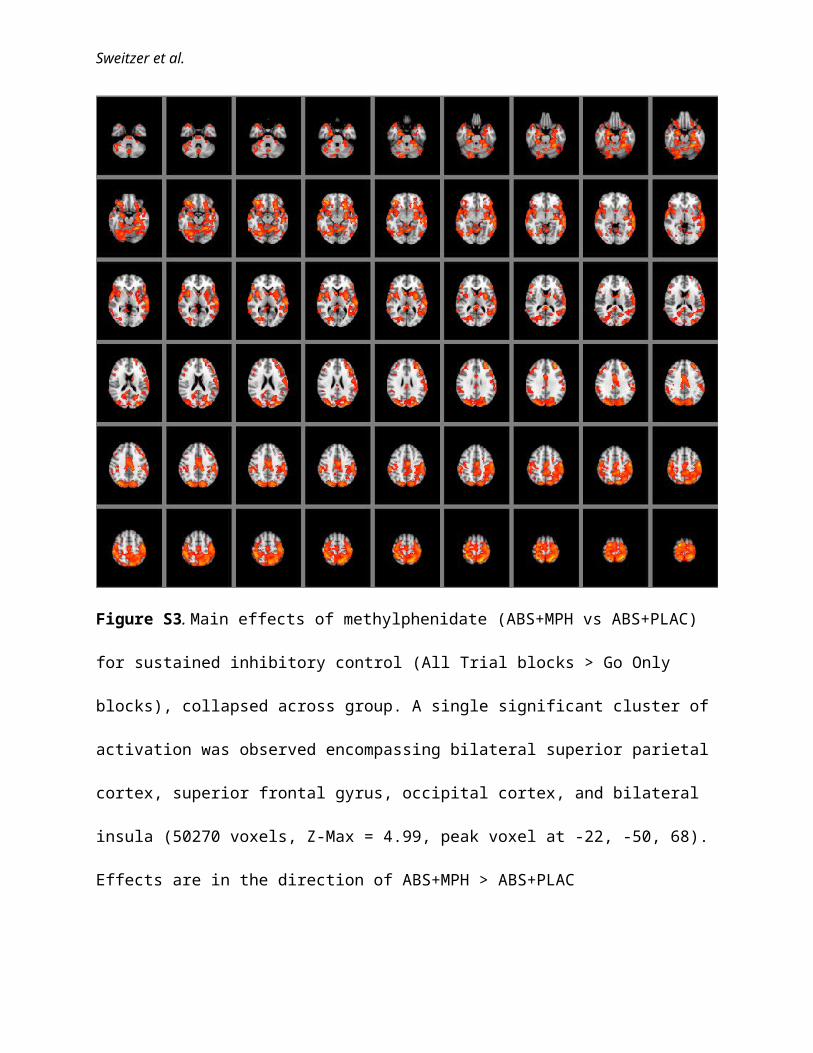
Figure S3. Main effects of methylphenidate (ABS+MPH vs ABS+PLAC) for sustained
inhibitory control (All Trial blocks > Go Only blocks), collapsed across group. A single
significant cluster of activation was observed encompassing bilateral superior parietal cortex,
superior frontal gyrus, occipital cortex, and bilateral insula (50270 voxels, Z-Max = 4.99, peak
voxel at -22, -50, 68). Effects are in the direction of ABS+MPH > ABS+PLAC
Sweitzer et al.
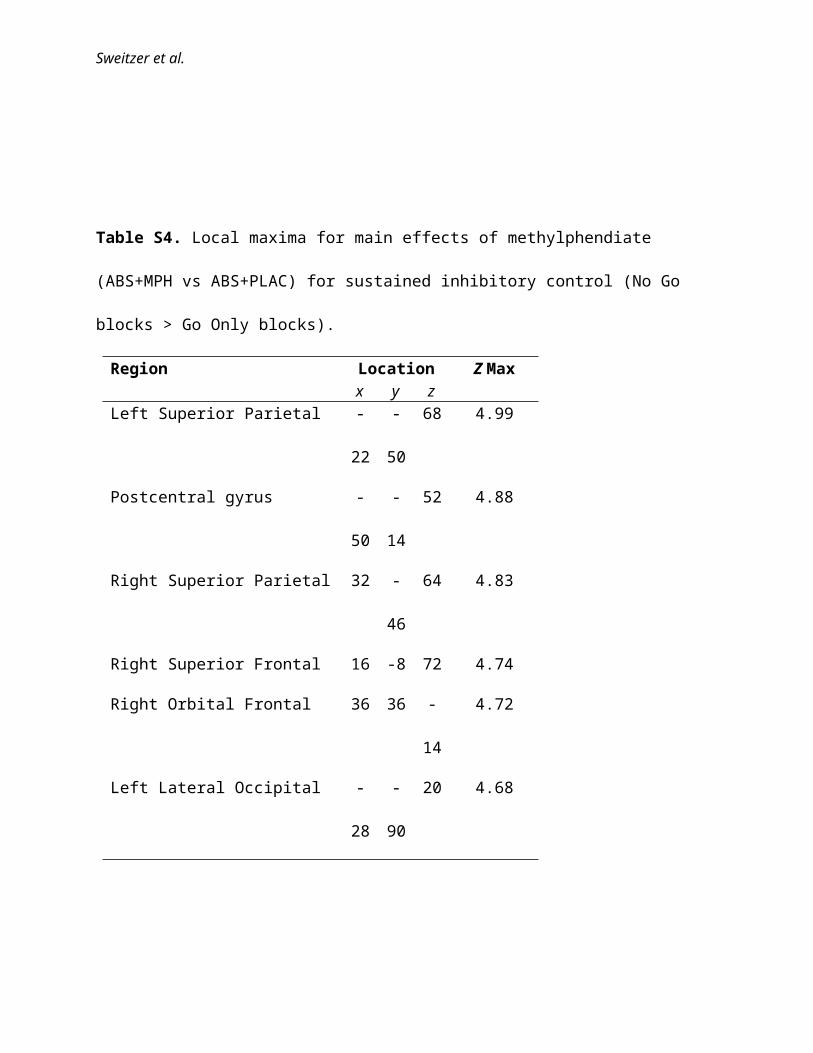
Table S4. Local maxima for main effects of methylphendiate (ABS+MPH vs ABS+PLAC) for
sustained inhibitory control (No Go blocks > Go Only blocks).
Region Location Z Maxx y z
Left Superior Parietal -22 -50 68 4.99
Postcentral gyrus -50 -14 52 4.88
Right Superior Parietal 32 -46 64 4.83
Right Superior Frontal 16 -8 72 4.74
Right Orbital Frontal 36 36 -14 4.72
Left Lateral Occipital -28 -90 20 4.68
Sweitzer et al.
Table S5. Whole-brain correlations between abstinence-induced changes (ABS+PLAC –
SAT+PLAC) in No Go trial accuracy (NoGo percent correct) and sustained inhibitory control
(All Trial > Go Only block effects). Table presents overall activation clusters and local maxima.
Region (and Local Maxima) Location Z Max Voxelsx y Z
Left Lateral Occipital -18 -84 40 4.65 13980
Left Lateral Occipital -18 -84 40 4.65
Right Lateral Occipital 24 -80 44 4.41
Right Superior Parietal 34 -48 58 4.34
Precuneus -4 -44 56 4.16
Postcentral gyrus 0 -36 58 3.97
Precentral gyrus -34 -8 52 3.96
Left planum polare/central opercular cortex
-56 -8 4 3.85 2541
Precentral gyrus -34 -8 52 3.96
Left Insula -40 6 -8 3.56
Left Superior Temporal -56 -24 -2 3.51
Left Middle Temporal -52 -22 -12 3.42
Left Insula -38 2 -6 3.42
Left Planum Polare -46 -2 -2 3.42
Right Insula 32 12 2 4.83 1269
Right Putamen 32 0 8 3.47
Right Pallidum 22 -6 6 2.97
Right Orbital Frontal 12 26 -22 2.5
Right Orbital Frontal 12 24 -18 2.46
Sweitzer et al.
Figure S4.
Figure S4. Main effects of task for transient inhibitory control (No Go trials > Rare Go trials),
collapsed across group and condition. Significant clusters of activation encompass 83743 voxels
including parietal lobe, frontal lobe, and basal ganglia (Z-Max = 9.29, peak voxel at 52, -40, 48)
and 1935 voxels including cerebellum and temporal lobe (Z-Max = 6.08, peak voxel at -40, -60, -
38).
Sweitzer et al.
Table S6. Regions of activation and local maxima for main effects of task for transient inhibitory
control (No Go trials > Rare Go trials), collapsed across group and condition.
Region Location Z Max Voxels x y Z
Parietal 52 -40 48 9.29 83743
Intraparietal 38 -44 42 9.25
Inferior parietal 46 -40 42 9.12
Superior temporal sulcus 52 -34 -4 8.97
Putamen 24 14 -6 8.69
Putamen 20 6 10 8.47
Cerebellum -40 -60 -38 6.08 1935
Cerebellum -28 -62 -36 5.61
Cerebellum -28 -40 -42 3.31
Temporal lobe -26 -12 -36 2.88
Temporal lobe -28 -16 -34 2.88
Cerebellum -24 -28 -34 2.84
Sweitzer et al.
Figure S5.
Figure S5. Main effects of methylphenidate (ABS+MPH vs ABS+PLAC) for transient
inhibitory control (No-Go trials > Rare-Go trials), collapsed across group. Significant clusters of
activation encompass 11546 voxels, including medial PFC, orbitofrontal cortex, subgenual ACC
and left hippocampus (Z-Max = 4.08, peak voxel at 14, 34, -6), and 1286 voxels including
precuneus/posterior cingulate cortex (Zmax=3.76, peak voxel at -20, -50, 22). Effect is in the
direction of ABS+MPH > ABS+PLAC.
x=-8 z=6x = -12x = -6