Embed Size (px)
Citation preview

3I Med Genet 1992; 29: 346-348
Brachydactyly type C associated with shorteningof the hallux
J M Rowe-Jones, A L H Moss, M A Patton
AbstractA four generation autosomal dominantpedigree of brachydactyly type C is pre-sented with its radiological features. Thehands and feet were similarly affected.All the subjects showing these changeshad shorter.ing of the big toes and, inaddition, had cupped ears.
the base of the proximal phalanx in the indexand middle fingers. This typically producesulnar deflection of the index finger.
Associated abnormalities of the feet haveonly rarely been described before and no pre-vious cases also having bilateral cup shapedears have been reported.
Department of Plasticand ReconstructiveSurgery, St George'sHospital MedicalSchool, LondonSW17 OQT.J M Rowe-JonesA L H Moss
South West ThamesRegional GeneticService, St George'sHospital MedicalSchool, LondonSW17 OQT.M A Patton
Correspondence to DrRowe-Jones, Department ofOtolaryngology, St George'sHospital, Blackshaw Road,London SW17 OQT.Received 10 June 1991.Revised version accepted23 August 1991.
Brachydactyly was classified into five main typesby Bell' in 1951. Type C involves shorten-ing of the index, middle, and little fingerswith deformity of the proximal and middlephalanges. Characteristically hypersegmenta-tion produces an extra, wedge shaped bone at
11
III
IV
Case reportsThe male index patient (case B, fig 1) pre-sented at 50 years of age. He was of normalintelligence and height. The index and middlefingers of both hands were shortened withulnar deviation of the index fingers (fig 2A,B).No functional deficit was apparent. Both rightand left halluces were shortened, the formermore than the latter (fig 2C,D). He had small,cup shaped ears resulting primarily from adeficiency in the length of the helical rim andscapha in the upper part of the auricle (fig 3).There was also some unfurling of the antiheli-cal fold. He remembered his mother havingsimilar deformities.He stated that his sister's younger son's
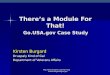
hands (case E) were similarly affected (fig 4E)
Figure I Pedigree offamily with brachydactyly typeC. Subject B is the index case.
Figure 2 Hands and feet of index patient case B.
I Figure 3 Small, cup shaped ear of the index case.Unfurling and shortening, in particular of theantihelical fold, is shown.
346
I
on 6 June 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.29.5.346 on 1 M
ay 1992. Dow
nloaded from
347Brachydactyly type C associated with shortening of the hallux
- __
Figure 4 Radiographs of hands and feet of cases C, D, and E. Case D has had attempted corrective surgery to his right index finger.
while his sister (fig 4A) and older nephew (fig4C) had shortening of both index fingers only.The younger nephew's son, 7 months old atthe time of investigation, also had brachydac-tyly of the right and left index and middlefingers.The big toes were deformed in cases C, D,
E, and F as well (fig 4B,D,F). These familymembers all had similar shaped ears butrefused facial photographs.
DiscussionBell's grouping of 1951 is considered the stan-dard reference for shortening of the digits.'Wood2 in his case report described brachydac-tyly type C under the title hyperphalangism,drawing attention to the occurrence of extraphalanges. He also commented that a range offeatures is usually found in this form of bra-chydactyly as is the case in our reported pedi-gree. The spectrum of changes illustratesclearly the variable expression of this autoso-mal dominant condition.The extra bone is seen to be wedge shaped,
occurring at the base of the proximal phalanx.Its C shaped epiphysis is consistent with thepathology of 'longitudinally bracketed diaphy-sis' as described by Theander and Carstam.3These supernumerary ossicles are usually de-scribed as fusing with the proximal phalangesbut, most interestingly, in case E (fig 4E) it isthe middle two phalanges of the middle fingersthat appear joined.The appearance of the thumbs is also
worthy of note. While brachyphalangism isusually seen as affecting the middle phalanx ofthe index, middle, and little fingers, cases C,D, and E show marked shortening and irregu-lar outline of the proximal phalanges of thethumb (fig 4A,C,E). Involvement of this digitis rare and more commonly presents withhypoplasia of the first metacarpal. The epiphy-sis of this bone may be absent causing shorten-ing, and it may develop a triangular shape.
The anatomy of the big toes in all thesubjects is also abnormal. Shortening of thehallux is contributed to by reduction andirregularity of both the metatarsal bone andproximal phalanx. Most interestingly in case Can extra wedge shaped phalanx has appeared inthe feet as well as in the hands (figs 4A,B).
Foot deformities such as talipes valgus havebeen described in association with brachydac-tyly type C in the hand before,4 though Bell'noted that in most published cases no footanomalies were reported. Our examples allclearly show a similar spectrum of foot invol-vement. Of note, malformation of the big toeassociated with shortening of the fingers hasalso been described in fibrodysplasia ossificansprogressiva.5The transmission of ear changes in our sub-
jects is very unusual. Dysmorphic facialfeatures occurring with such hand abnormalit-ies is extremely rare. Manzke6 reported thecase of an 8 year old boy with the Robinsequence and type C changes but this was anisolated case. The association with ear abnor-malities suggests that the bone shortening intype C brachydactyly may result primarilyfrom a defect in chondrification, as has beenshown in diastrophic dysplasia. Cartilaginousabnormality of the pinna, leading to calcifica-tion, has been seen with brachydactyly in theKeutel syndrome.8
In conclusion our pedigree presents a clearexample of the digital manifestations found intype C brachydactyly. The similar changes inthe big toes of all the subjects are of particularnote and show an affinity with the changes inthe fingers. The presence of cupped ears mayprovide evidence for the condition resultingfrom abnormal chondrification rather thanbone matrix changes.
1 Bell J. On hereditary digital anomalies. Part 1. On brachy-dactyly and symphalangism. In: Penrose LS, ed. Thetreasury of human inheritance. Vol 5. London: CambridgeUniversity Press, 1951:1-31.
2 Wood VE. Different manifestations of hyperphalangism. JHand Surg (Am) 1988;13:883-7.
on 6 June 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.29.5.346 on 1 M
ay 1992. Dow
nloaded from

Rowe-Jones, Moss, Patton
3 Theander G, Carstam N. Longitudinally bracketed diaphy-sis. Ann Radiol (Paris) 1974;17:355-60.
4 Haws DV. Inherited brachydactyly and hypoplasia of thebones of the extremities. Ann Hum Genet 1963;26:201.
5 Connor JM, Evans DAP. Fibrodysplasia ossificans progres-siva. The clinical features and natural history of 34patients. Bone joint Surg (Br) 1982;64:76-83.
6 Manzke H. Symmetrische Hyperphalangie der zwietenFingers durch ein akzessorischen Metacarpale. FortschrRoentgenstr 1966;105:425-7.
7 Stanescu V, Sci DM, Stanescu R, Maroteaux P. Pathogenicmechanisms in osteochondrodysplasias. I Bone Joint Surg(Am) 1984;66:817-36.
8 Fryns JP, van Fleteren A, Mattelaer P, van den Berghe H.Calcification of cartilages, brachytelephalangy and peri-pheral pulmonary stenosis. Confirmation of the Keutelsyndrome. EurI Pediatr 1984;142:201-3.
348
on 6 June 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.29.5.346 on 1 M
ay 1992. Dow
nloaded from