Embed Size (px)
Citation preview
0022-5347/98/1603-0831$03.00/0 THE JOURNAL OF UROLOGY Copyright 0 1998 by A M E R I C A N UROLOCICAL ASSOCIATION, I N C .
Vol. 160,831-832, September 1998 Printed in U.S.A.
MECKEL'S DIVERTICULUM AS A CONTINENCE MECHANISM
DAVID GOTSADZE AND GEORGI PIRTSKHALAISHVILI From the Department of Urology, Oncological Research Center, Lisi Lake, Tbilisi, Republic of Georgia
KEY WORDS: urinary reservoirs, continent; Meckel's diverticulum; ileum
Construction of abdominal urinary reservoirs became rou- tine for supravesical urinary diversion during the last de- cade. Fashioning a continence mechanism that is reliable and easy for catheterization is principally important for the successful functioning of intestinal reservoirs. We report a case of construction of an ileal reservoir with Meckel's diver- ticulum as a continence mechanism, which to our knowledge has not been described previously.
CASE REPORT
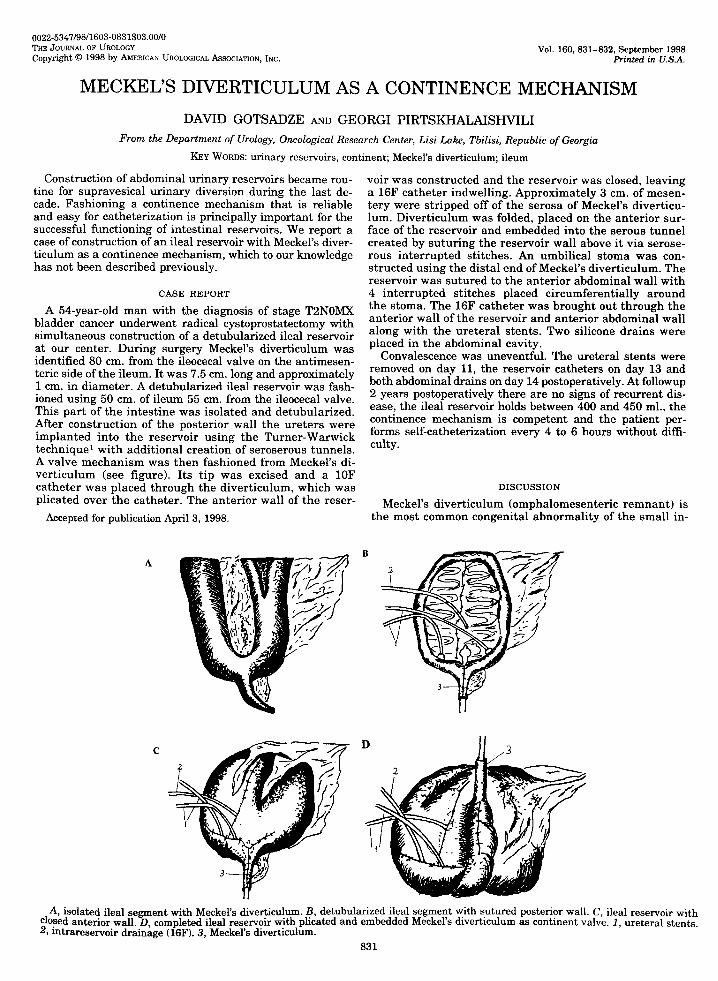
A 54-year-old man with the diagnosis of stage TBNOMX bladder cancer underwent radical cystoprostatectomy with simultaneous construction of a detubularized ileal reservoir at our center. During surgery Meckel's diverticulum was identified 80 cm. from the ileocecal valve on the antimesen- teric side of the ileum. It was 7.5 cm. long and approximately 1 cm. in diameter. A detubularized ileal reservoir was fash- ioned using 50 cm. of ileum 55 cm. from the ileocecal valve. This part of the intestine was isolated and detubularized. After construction of the posterior wall the ureters were implanted into the reservoir using the Turner-Warwick technique1 with additional creation of seroserous tunnels. A valve mechanism was then fashioned from Meckel's di- verticulum (see figure). Its tip was excised and a 10F catheter was placed through the diverticulum, which was plicated over the catheter. The anterior wall of the reser-
Accepted for publication April 3, 1998.
voir was constructed and the reservoir was closed, leaving a 16F catheter indwelling. Approximately 3 cm. of mesen- tery were stripped off of the serosa of Meckel's diverticu- lum. Diverticulum was folded, placed on the anterior sur- face of the reservoir and embedded into the serous tunnel created by suturing the reservoir wall above it via serose- rous interrupted stitches. An umbilical stoma was con- structed using the distal end of Meckel's diverticulum. The reservoir was sutured to the anterior abdominal wall with 4 interrupted stitches placed circumferentially around the stoma. The 16F catheter was brought out through the anterior wall of the reservoir and anterior abdominal wall along with the ureteral stents. Two silicone drains were placed in the abdominal cavity.
Convalescence was uneventful. The ureteral stents were removed on day 11, the reservoir catheters on day 13 and both abdominal drains on day 14 postoperatively. At followup 2 years postoperatively there are no signs of recurrent dis- ease, the ileal reservoir holds between 400 and 450 ml., the continence mechanism is competent and the patient per- forms self-catheterization every 4 to 6 hours without diffi- culty.
DISCUSSION
Meckel's diverticulum (omphalomesenteric remnant) is the most common congenital abnormality of the small in-
B A
C
A, isolated ileal segment with Meckel's diverticulum. B, detubularized ileal segment with sutured posterior wall. C, ileal reservoir with closed anterior wall. D, completed ileal reservoir with plicated and embedded Meckel's diverticulum as continent valve. 1 , ureteral stents. 2, htrareservoir drainage (16F). 3, Meckel's diverticulum.
831

832 MECKEL'S DIVERTICULUM AS
testine and can be seen in 1 to 3% of the population, and its presence may be accompanied by complications.2,3 Therefore, some authors advocate prophylactic excision of Meckel's diverticulum in the absence of contraindications.3 However, Meckel's diverticulum may be useful as an arti- ficial valve during construction of an intestinal reservoir. The continence mechanism may be fashioned by creating a serous tunnel as we described or by formation of a submu- cosal tunnel when feasible, as has been performed with appendix.
CONTINENCE MECHANISM
REFERENCES 1. Warwick, R. T. and Ashen, M. H.: The functional results of
partial subtotal and total cystoplasty with special reference to ureterocalcocryptoplasty, selective sphincterotomy and cysto- cystoplasty. Brit. J. Urol., 39 3, 1967.
2. Leijonmarck, C. E., Bonman-Sandelin, K., Frisell, J. and Raf, L.: Meckel's diverticulum in the adult. Brit. J. Surg., 73: 146, 1986.
3. Liidtke, F. E., Mende, V., Kohler, H. and Lepsier, G.: Incidence and frequency of complications and management of Meckel's diverticulum. Surg. Gynec. & Obst., 169 537, 1989.


![Laparoscopic approach to Meckel's diverticulum · 2017. 4. 25. · The advances in laparoscopy have significantly aided the diagnosis and surgical treatment[3,5,6,9-12] of this disease,](https://img.pdfslide.us/doc/110x75/6052e45efaf23930c8470fe7/laparoscopic-approach-to-meckels-diverticulum-2017-4-25-the-advances-in-laparoscopy.jpg)