Embed Size (px)
Citation preview

Cancer Therapy: Preclinical
Mechanisms of Acquired Drug Resistance to theHDAC6 Selective Inhibitor Ricolinostat RevealsRational Drug-Drug Combination with IbrutinibJennifer E. Amengual1, Sathyen A. Prabhu1, Maximilian Lombardo1, Kelly Zullo1,Paul M. Johannet2, Yulissa Gonzalez1, Luigi Scotto1, Xavier Jirau Serrano1,Ying Wei3, Jimmy Duong3, Renu Nandakumar4, Serge Cremers4,Akanksha Verma5, Olivier Elemento5, and Owen A. O'Connor1
Abstract
Purpose: Pan-class I/II histone deacetylase (HDAC) inhi-bitors are effective treatments for select lymphomas.Isoform-selective HDAC inhibitors are emerging as poten-tially more targeted agents. ACY-1215 (ricolinostat) is afirst-in-class selective HDAC6 inhibitor. To better under-stand the discrete function of HDAC6 and its role in lym-phoma, we developed a lymphoma cell line resistant toACY-1215.
Experimental Design: The diffuse large B-cell lymphoma cellline OCI-Ly10 was exposed to increasing concentrations ofACY-1215 over an extended period of time, leading to thedevelopment of a resistant cell line. Gene expression profiling(GEP) was performed to investigate differentially expressedgenes. Combination studies of ACY-1215 and ibrutinib wereperformed in cell lines, primary human lymphoma tissue, anda xenograft mouse model.
Results: Systematic incremental increases in drug exposureled to the development of distinct resistant cell lines with IC50
values 10- to 20-fold greater than that for parental lines. GEPrevealed upregulation of MAPK10, HELIOS, HDAC9, and FYN,as well as downregulation of SH3BP5 and LCK. Gene-setenrichment analysis (GSEA) revealed modulation of the BTKpathway. Ibrutinib was found to be synergistic with ACY-1215in cell lines as well as in 3 primary patient samples of lym-phoma. In vivo confirmation of antitumor synergy was dem-onstrated with a xenograft of DLBCL.
Conclusions: The development of this ACY-1215–resistantcell line has provided valuable insights into the mechanisticrole of HDAC6 in lymphoma and offered a novel method toidentify rational synergistic drug combinations. Translation ofthese findings to the clinic is underway. Clin Cancer Res; 23(12);3084–96. �2016 AACR.
IntroductionPan-class I/II histone deacetylase (HDAC) inhibitors have
proven to be successful agents for the treatment of lymphoma,though their clinical application has been restricted predom-inantly to the T-cell lymphomas (1–5). While the precise role ofindividual HDAC isoforms in lymphoma has remained an areaof active research, isoform-selective HDAC inhibitors havebegun to emerge. The first example of this is ACY-1215 (rico-linostat), an isoform-selective HDAC6 inhibitor. HDAC6
belongs to the class 2b family of HDACs and differs fromother HDACs in that it resides predominantly in the cytoplasm.It is known to play a role in protein homeostasis and theunfolded protein response (UPR; refs. 6, 7). HDAC6 inhibitionhas demonstrated activity in preclinical models of lymphomaand multiple myeloma and is presently being studied in clinicalstudies both as a single agent and in combination. Althoughvery well tolerated clinically, activity as a single agent has beenlimited and combination strategies have proven more effica-cious thus far. Combinations of ACY-1215 with lenalidomide,pomalidomide, and bortezomib are presently in clinical studyfor patients with multiple myeloma (8–11).
In an effort to gain insights into the role of HDAC6 in lym-phoma and to identify novel pathways that may be synergisticwith ACY-1215, a lymphoma cell line was developed to beresistant to the HDAC6-selective inhibitor ACY-1215. Drug resis-tance can be defined as intrinsic or acquired. Intrinsic drugresistance is often difficult to demonstrate in tissue culture, andis defined as cells that harbor preexisting conditions which renderthem unresponsive to a particular drug or drug combination.Acquired drug resistance typically emerges in stages, and at leasttheoretically is attributed to the emergence of pathways thatbypass the inhibition posed by a particular drug. We reasonedthat if the emergence of compensatory pathways could mitigatesensitivity to exposure of a specific drug, then such pathways
1Center for Lymphoid Malignancies, Columbia University Medical Center, NewYork, New York. 2Stanford University School of Medicine, Stanford, California.3Department of Biostatistics, Mailman School of Public Health, Columbia Uni-versity, New York, New York. 4Division of Clinical Pathology, Department ofPathology andCell Biology, Columbia UniversityMedical Center, NewYork, NewYork. 5Institute for Computational Biomedicine, Weill Cornell Medical College,New York, New York.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: Jennifer E. Amengual, Columbia University, 51 W 51stStreet, Suite 200, NewYork, NY 10019. Phone: 212-326-5720; Fax: 212-326-5725;E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-16-2022
�2016 American Association for Cancer Research.
ClinicalCancerResearch
Clin Cancer Res; 23(12) June 15, 20173084
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

could represent logical targets for rational drug-drug combina-tions, preempting acquired drug resistance, at least in that specificcontext. This paradigm, if validated, could create a logic informingthe development of "rational" upfront combinations that couldimprove the efficacy of new drug combinations.
We employed a strategy of gradual drug acclimation to identifya resistant cell line to try and capture emerging compensatorypathways of resistance to ACY-1215. We conducted gene expres-sion profiling (GEP) of the resistant line which was comparedwith the parental line. The GEP data revealed modulation of theB-cell receptor (BCR) pathway, including downregulation of thenegative regulator of BTK (SH3BP5), increased FYN, and IKZF2.These observations led to systematic evaluation of the combina-tion of ACY-1215 with ibrutinib, a first-in-class BTK inhibitor,which demonstrated strong synergy. This synergy was demon-strated across a large panel of cell lines, including ones represent-ing DLBCL and mantle cell lymphoma (MCL), and primaryhuman samples including chronic lymphocytic lymphoma(CLL), lymphoplasmacytic lymphoma, and marginal zone lym-phoma (MZL). In addition, an in vivomurine xenograft model ofDLBCL (OCI-LY10) confirmed the therapeutic benefits of thecombination over the individual drugs. Interestingly, the UPRhas been shown to be linked to the BCR pathway through IRE-1and XBP-1 (12, 13) in models of CLL. Work conducted in thecurrent manuscript further substantiates this link as a potentialmechanism in models of DLBCL, MCL, and MZL. We believethesefindings add credence to the idea that understandingmecha-nisms of acquired drug resistance could lead to the developmentof rational drug-drug combinations with novel agents nowemerging in the clinic. The findings of these series of experimentslay the foundation for clinical studies of ACY-1215 and ibrutinibin B-cell lymphoid malignancies.
Materials and MethodsDrugs and reagents
ACY-1215 was provided by Acetylon Pharmaceuticals, Inc..Bortezomib, ibrutinib, romidepsin, verapamil, and vorinostatwere obtained from Selleck Chemicals. All drugs were diluted
in DMSO. Deuterated internal standard ibrutinib-d5 waspurchased from TLC Pharmaceutical Standards Ltd. All sol-vents and other chemicals for sample extraction were LC/MSgrade.
Cell lines and cultureHbl-1, OCI-Ly10, and Riva are activated B-cell (ABC) DLBCL
cell lines; OCI-Ly1, OCI-Ly7, Su-DHL-6 are germinal center(GC) DLBCL cell lines; JVM2, MAVER, Hbl-2, Jeko-1, and Rec-1are mantle cell lymphoma (MCL) cell lines; HH and H9 areT-cell lymphoma (TCL) cell lines. Su-DHL-6, HBL-1, Riva,HBL2, Jeko-1, Rec-1, MAVER, HH, and H9 were obtained fromATCC. OCI-Ly1, OCI-Ly7, and OCI-Ly10 were obtained fromDSMZ. Su-DHL-6, Hbl-1, Hbl-2, HH, H9, Jeko-1, Jvm-2,MAVER, and Rec-1 were grown in RPMI (10% FBS). OCI-Ly7,OCI-Ly10, and Riva were grown in IMDM (10% FBS). All celllines were authenticated and screened for mycoplasma usingthe ATCC/Promega STR Authentication Testing Kit and LonzaMycoAlert for mycoplasma testing. Primary patient lymphomasamples were collected on an approved institutional reviewboard (IRB) protocol. Peripheral blood was collected andperipheral blood mononuclear cells were extracted by Ficoll-Paque density gradient media and centrifugation.
Cell viability assaysCells (3� 105 cells/well) were incubatedwith 1:100 dilution of
drug (listed above) alone or in combination. Cell viability wasassessed using the CellTiter-Glo Luminescent Cell Viability Assay(Promega Corporation) and confirmed by Vi-Cell Series CellViability Analyzer (14, 15). The ACY-1215–resistant cell line wasderived from the OCI-Ly10 cell line. OCI-Ly10 was exposed toincreasing concentrations of ACY-1215 over time. Systematicincremental increases in drug concentration exposure led to thedevelopment of distinct cell lines with IC50 values 10- to 20-foldgreater than that for parental lines.
BH3 profilingBH3 profiling was performed as described previously (16).
Briefly, whole cells were permeabilized using the detergentdigitonin which selectively permeabilizes the cell membrane,but not the mitochondrial membrane. BH3 peptides (synthe-sized by the Tufts University Peptide Synthesis Core andGenscript) were administered to the cells in prescribed con-centrations. Depolarization of the mitochondrial membranepotential was assessed by staining the cells with JC-1 dye in384-well, black, flat-bottom, nontreated plates. FollowingJC-1 exposure, the JC-1 emission was read on a GloMax(Promega) plate reader once every 5 minutes for 180 minutesto generate a kinetic trace of mitochondrial membrane poten-tial over time.
Flow cytometry/JC-1FACSCalibur System was used to acquire the fluorescence
signals (�1 � 105 events/sample); data was analyzed usingFlowjo 8.8.6. Cells (3 � 105/mL) were quantitated for apopto-sis using Alex Fluor 488/Annexin V (Dead cell apoptosis kitInvitrogen #V13240) or for the determination of the trans-membrane mitochondrial membrane potential (Dym) viastaining with JC-1 1.3 ug/mL JC-1 dye (Invitrogen) as describedpreviously (14).
Translational Relevance
To better understand the function of HDAC6 and its role inlymphoma, we developed lymphoma cell lines resistant to theselective HDAC6 inhibitor ACY-1215. ACY-1215 has demon-strated activity in preclinical models ofmultiplemyeloma andlymphoma and is currently being studied clinically for both ofthese diseases. Gene expression profiling was performed onthe resistant line and compared with the parental line whichpointed to modulation of the BTK pathway revealing a poten-tial drug partner. Synergywas confirmedwith the combinationof ACY-1215 and ibrutinib in lymphoma cell lines, primaryhuman lymphoma tissue, and a mouse model of lymphoma.The development and characterization of this ACY-1215–resistant cell line has proven to be a valuable tool to advanceour understanding of the functional role of HDAC6 in lym-phoma. This strategy is a practicalmethod to identify potentialrational and synergistic drug-drug combinations. Translationof these findings in lymphoma is now underway.
Selective HDAC6 Inhibitor has Synergy with Ibrutinib
www.aacrjournals.org Clin Cancer Res; 23(12) June 15, 2017 3085
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

Western blottingWestern blotting was performed as described previously (14).
Antibodies used were as follows: anti-acetylated lysine, anti-GRP78/BiP, anti-HDAC6, anti-HDAC9, anti-PERK and p-PERK,anti-p-eif2a, anti-IRE1a,, anti-FYN, anti-eif2a, anti-p-eif2a,anti-BTK, anti-p-BTK, anti-PCL-g2, anti-p-PCL-g2, anti-CARD11,anti-ATF4, anti-AKT, anti-p-AKT, anti-CHOP, anti-Helios, anti-b-actin, anti-BIM (C23C5), anti-Bcl2 (Cell Signaling Technolo-gy); anti-MAPK10, anti-p-IRE1a and anti-SH3BP5 (Abcam);anti-XBP-1 (Santa Cruz Biotechnology). Densitometry analysiswas performed on scanned images using ImageJ software (NIH,Bethesda, MD).
Gene expression profilingRNA was extracted from cells using the RNeasy minikit
(Qiagen). RNA was quantified and assessed for integrity viaBioanalyzer 2100 (Agilent) for an RNA Integrity Number great-er than 8 for RNA sequencing by the Columbia Genome Center.mRNA was enriched from total RNA samples using poly-A pulldown and libraries were prepared using the TruSeq RNA prepkit (Illumina). Sample-derived libraries were then sequencedusing the HiSeq2500 platform (Illumina).
Base callingwas performedusingReal TimeAnalysis (Illumina)and bcl2fastq(v 1.8.4) for converting BCL to fastq format. Readswere then mapped to a reference genome (Human:NCBI/build37.2) using TopHat (v2.0.4). Relative abundance was estimatedusing Cufflinks (version 2.0.2). Differentially expressed geneswere tested for using the R package DESeq2.
Gene set enrichment analysis was performed using a prerankedtool from the Broad Institute's GSEA software (17). The metric of�log10 of the P value�sign of the log fold changewas used to rankthe genes. Pathway analysis on this preranked list of genes wasthen performed using Gene Ontology and Lymphoid biologygene sets from the Staudt lab (18).
Semi-quantitative PCRSemi-quantitative Multiplex RT-PCR was performed as
described previously (19). Reverse transcription (RT) was per-formed in a 20 mL reaction system with a total of 2 mg of RNasefree DNase treated RNA (Omniscript RT kit, Qiagen) and oligo-d(T). Multiplex PCR reactions were run in 30 cycles. Primers(Thermo Fisher Scientific) were designed to span multiple exonsof the target genes. Primer sequences can be found in Table 1.Images were analyzed using the ImageJ software (NIH, Bethesda,MD) and band densities were normalized to GAPDH.
In vivo studiesAnimals were housed and maintained in accordance with an
IUCAC-approved protocol. OCI-Ly10 cells (1 � 107; either resis-
tant or parental) in 50% Matrigel (BD Biosciences) were subcu-taneously injected into the flanks of 5- to 7-week-old beige/SCIDmice (Taconic Farms, Inc). Treatment was initiated when tumorvolumemeasured 80mm3. Tumor volumewas assessed using thetwo largest perpendicular axes (l ¼ length; w ¼ width) andcalculated using the formula v ¼ 0.5(l2 � w). Mice were dividedinto 4 cohorts of 8–10 mice per cohort as follows: (i) untreatedcontrol; (ii) ACY-1215: 50 mg/kg days 1–5, 8–12, 15–19; (iii)ibrutinib: 3mg/kgdays 1–20; (iv)ACY-1215plus ibrutinib.Drugswere diluted in sterile dextrose 5% inwater andwere administeredvia the intraperitoneal (IP) route (20). Mice were assessed forweight loss and tumor volume 3�/week. Animals were sacrificedwhen the tumor volume exceeded 2,000 mm3 or after sustain-ed loss of >10% body weight in accordance with institutionalguidelines.
Pharmacokinetic/pharmacodynamic in vivo studiesMice were studied for pharmacokinetic and pharmacodynamic
effects of ACY-1215 and ibrutinib. Approximately 250 mL ofblood was collected by submandibular vein bleed at 0.5, 1, and2 hours after treatment. Mice were sacrificed at 4, 6, and 8 hoursafter treatment; blood and tumor tissues were collected for mea-surement of drug concentration and Western blot analysis.
LC/MS-MS analysis for quantitation of ACY-1215 and ibrutinibACY1215 and ibrutinib were measured in mouse serum and
tumor tissues using ultra performance LC/MS-MS after liquid–liquid extraction using deuterated ibrutinib as internal stan-dard. Serum samples (100 mL) or aqueous tissue homogenatecontaining 10 mg wet tissue disrupted by a Tissue Tearerhomogenizer were spiked with deuterated internal standard ata level of 50 ng/mL. This was mixed with 100 mL of acetonitrile,vortexed, and incubated for 10 minutes followed by addition of750 mL of methyl tert-butyl ether. The mixture was vortexed for10 minutes, centrifuged and the organic layer was transferredto a LC-MS vial, evaporated under nitrogen stream and resus-pended in 50% methanol. Calibration standards and qualitycontrol (QC) samples for both the compounds were preparedspanning a range of 0.5 ng/mL to 1,000 ng/mL and extractedsame as the samples.
LC/MS-MS analysis was performed on a platform compris-ing Agilent 1290 Infinity UHPLC integrated to Agilent 6410triple quad mass spectrometer controlled by MassHunter v 3.1(Agilent Technologies). Chromatographic separation was per-formed on an Agilent Poroshell C18 column (50 � 2.1 mm,2.7u, 100A) maintained at 40�C. The flow rate was maintainedat 500 mL/minute. The initial flow conditions were 50% solventA (water containing 0.1% formic acid) and 50% solvent B(methanol with 0.1% formic acid). Solvent B was raised to
Table 1. Primers used for semiquantitative RT-PCR
Gene Forward Reverse
MAPK10 5'-CGGACTCCGAGCACAATAAA-3' 5'-GGAGCAGGTAGATGCAAGATAG-3'SH3BP5 5'-ATGAGGGTAGGAGGGACTTATAG-3' 5'-CGTCACCACCTCGTCTTTATC-3'FYN 5'-GGATTGGCCCGATTGATAGA-3' 5'-GGTTTCACTCTCGCGGATAAG-3'HDAC9 5'-GAGGCAAGAACAGGAAGTAGAG-3' 5'-GGATGGAGATGTTCCACTAAGG-3'IKZF2 5'-CACCCAACCACTCCCAAATA-3' 5'-CTGAGCCATATCCACCTCTTTC-3'HDAC6 5'-AGTGGCCGCATTATCCTTATC-3' 5'-GAGGGTCCTTCTCTGTCTTCTA-3'LCK 5'-CTACGGGACATTCACCATCAA-3' 5'-CTCTCTGTGGTCTCAGGAAATG-3'GAPDH 5'- - 3' 5' - - 3'
Amengual et al.
Clin Cancer Res; 23(12) June 15, 2017 Clinical Cancer Research3086
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

70% over 1.75 minutes and to 95% by 1.95 minutes, held until3.5 minutes and back to initial conditions by 4 minutes with atotal run time of 6 minutes. The retention time for ACY-1215and ibrutinib was 1.34 and 2.08 minutes, respectively. Themass spectrometer was operated under multiple reaction mon-itoring (MRM) mode with positive electrospray ionization. ForMRM, following transitions were utilized for quantitation:ACY1215 434.2>274.0; ibrutinib 441.2>304.1 and ibruti-nib-d5 446.2>309.1. Mass spectrometer was operated usingthe following parameters: gas temperature, 300�C; gas flow,13 L/minute; nebulizer, 30 psi; capillary 3 Kv; desolvation gasflow, 500 L/hour; cone gas flow, 50 L/hour and collisionenergy, 30 v.
Lower limit of quantification (LLOQ), defined as the lowestconcentration with an accuracy and precision of <20% wasdetermined to be 0.5 ng/mL for ACY1215 and 2.5 ng/mL foribrutinib in serum. In tumor samples, the LLOQ was determinedto be 1 ng/mL for both ACY1215 and 2.5 ng/mL for ibrutinib. Theintra-assay accuracy and precision for ACY1215 was 96.1% and1.32%, respectively, while for ibrutinib, the intra-assay accuracywas 99.6% with a precision of 1.72%. The assay showed an inter-assay precision for ACY1215 0.90% and for ibrutinib 1.52%.
Statistical analysisFor determination of the inhibitory concentration of 50% of
cells (IC50) and synergy, all experiments were run in triplicateand repeated at least twice. IC50 was calculated with Calcusynsoftware (Biosoft). Relative risk ratio (RRR) was used as amodel for establishing synergy between 2 drugs (21). RRR isbased on calculating the ratio between the actual value andexpected value (EV). In the case of two cytotoxic compounds,EV is calculated by the formula: EV ¼ (NA X NB)/100, where NA
represents the percentage of viable cells treated with drug A andNB represents the percentage of viable cells treated with drug B.RRR<1 represents a synergistic effect; values equal to 1 indicatethe mean additive effect; and values>1 represent an antagonis-tic effect. Flow cytometry assays were performed in duplicate,repeated at least twice, and reported as the mean with associ-ated SDs.
In vivo statistical analysis was performed using Prism Graph-Pad's two-way ANOVA Analysis. Overall survival (OS) was esti-mated using the Kaplan–Meier method, and presented as themean OS with 95% confidence intervals. Area under the serumconcentration time curve (AUC) and half-life were determinednoncompartmentally using Phoenix Winnonlin software version6.3 (Certara). All drug concentrations are represented as themeanwith the SD where applicable.
ResultsThe development of an ACY-1215–resistant cell line is stableand not dependent on efflux pumps
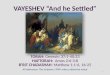
The diffuse large B-cell lymphoma cell line OCI-Ly10 wasexposed to increasing concentrations of ACY-1215 over thecourse of 1 year. Systematic incremental increases in drugexposure led to the development of a distinct cell line withan IC50 value 10- to 20-fold greater than that of the parentalline. The resistant R10-OCI-LY10 (R10) exhibited an IC50 of10 mmol/L as compared with parental IC50 of 0.9 mmol/L after48 hours of exposure (Fig. 1A). Resistance was maintainedafter repeated passages for �1 month in the absence of drug
and was not overcome by inhibition of efflux pumps as deter-mined via verapamil co-exposure (Fig. 1A; ref. 22). Interest-ingly, the resistant line was cross resistant to vorinostat whichstrongly inhibits HDAC6 (R10 IC50 ¼ not reached vs. P IC50 ¼0.6 mmol/L). Treatment of the resistant line with bortezomibdemonstrated intermediate activity underscoring the notionthat although their molecular targets are vastly different (i.e.,proteasome vs. HDAC6), both drug mechanisms converge onthe processing of misfolded proteins (R10 IC50 ¼ 8 nmol/Lvs. P IC50 ¼ 3.3 nmol/L). In contrast, the resistant line wassensitive to romidepsin which is known to predominantly in-hibit HDAC1, 2, and 3 with minimal activity against HDAC6(R10 IC50¼ 3 mmol/L vs. P IC50¼ 2.25 mmol/L; Fig. 1B; ref. 23).
Both the resistant and parental LY10 cell lines were xenograftedinto the flanks of SCID beige mice at 107 cells. Mice were dividedinto 4 cohorts, resistant (R) control, parental (P) control, (R)ACY-1215, (P) ACY-1215. Mice were treated with ACY-1215 50mg/kgdays 1–5, 8–12, 15–19 by intraperitoneal route. The tumorvolume doubling time was calculated for each cohort usingGraphPad Prism software. The resistant cohorts exhibited accel-erated tumor growth and decreased survival demonstrating thatthe resistant line maintains a highly aggressive phenotype overtime in vivo. Treating the resistant mouse with ACY-1215 hadno impact on the tumor doubling time as compared with theuntreated resistant control mice (6.857 vs. 7.004 days). In addi-tion, the rate of growth was greater in the resistant control mousecohort as compared with the parental control cohort (7.004 vs.8.039 days to doubling). The volumetric doubling time of (P)ACY-1215 treated tumors was more than twice as long comparedwith those of the (R) line treated with ACY-1215 (15.62 vs. 6.857days; Fig. 1C). This translated into a shorter survival for both theresistant cohorts as compared with parental cohorts. Mediansurvival in days was as follows for each cohort: resistant control(26.5) < resistant ACY-1215 (38) < parental control (43.5) <parental ACY-1215 (54; Fig. 1D).
The IRE-1/XBP-1 pathway is upregulated in cells resistant toACY-1215
To evaluate for intrinsic drug resistance, basal levels of Bcl2and Bim were correlated with the IC50 of a panel of lymphomacell lines. It has been demonstrated by others that decreasedlevels of Bim and increased levels of Bcl2 correlate with drugresistance (24, 25). The Bcl2-Bim ratio correlated to sensitivityto ACY-1215 and cell lines with relatively high levels of Bcl2and low levels of Bim were relatively resistant to ACY-1215(Fig. 2A). Next we investigated whether resistance to apopto-sis in the resistant cell line was due to alterations in the Bcl2family proteins, which are known to play critical roles inregulating apoptosis. Mitochondrial membrane depolarizationwas evaluated following treatment with ACY-1215 in parentaland resistant cells to in an effort to study changes followingacquired drug resistance. Compared with the parental line, theresistant line did not depolarize the mitochondrial membranefollowing treatment with ACY-1215 2.5 mmol/L, confirmingresistance to induction of apoptosis (Fig. 2B). BH3 profiling is afunctional assay which informs the cellular dependence onantiapoptotic proteins for evasion of cell death (26). Therewas no difference in the BH3 profiles of the resistant andparental cell lines (Fig. 2C). Taken together, these findingsconclude that functional alterations in the Bcl2 family ofproteins do not contribute to resistance to ACY-1215.
Selective HDAC6 Inhibitor has Synergy with Ibrutinib
www.aacrjournals.org Clin Cancer Res; 23(12) June 15, 2017 3087
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

0
20
40
60
80
100
1.510.50Concentra�on (μmol/L)
Vorinostat
0
20
40
60
80
100
151050Concentra�on (nmol/L)
Bortezomib
0
20
40
60
80
100
420Concentra�on (nmol/L)
Romidepsin
0
20
40
60
80
100
20151050
R10 – OCI-LY10
0
20
40
60
80
100
20151050
R10 – OCI-LY10
- R10
- R10 passaged 1 month without drug
A
C
B
***
D
- ACY-1215
- ACY-1215 plus Verapamil
0
20
40
60
80
100
20151050
Cell
viab
ility
(%)
Cell
viab
ility
(%)
Cell
viab
ility
(%)
Concentra�on (mmol/L)
Concentra�on (mmol/L)
Concentra�on (mmol/L)
ACY-1215
OCI-LY-10 Parental vs. resistant OCI-LY-10 Parental vs. resistant2,000
1,500
1,000
500
00 10 20 30 40 0 20 40 60 80
Day Day
Tum
or v
olum
e (m
m3 )
Per
cent
sur
viva
l
100
50
0
(R) Control
(R) Control(R) ACY-1215
(R) ACY-1215(P) Control
(P) Control(P) ACY-1215
(P) ACY-1215
P = 0.0383P = 0.0046
48 h LY10R
48 h LY10R
48 h LY10R
72 h LY10R
48 h LY10P
72 h LY10P
48 h LY10R
72 h LY10R
48 h LY10P
72 h LY10P
72 h LY10R
48 h LY10P
72 h LY10P
72 h LY10R
48 h LY10 RP
72 h LY10P
Figure 1.
Development and characterization of selective HDAC6 inhibitor resistant cell line. The DLBCL cell line, OCI-LY10, was exposed to increasing concentrationsof ACY-1215 over time. A, Concentration–effect relationships were established for resistant and parental Ly10 at 48 and 72 hours following exposureto ACY-1215. Forty-eight–hour concentration–effect relationship of increasing concentrations of ACY-1215 in the resistant line after immediateexposure and after a wash-out period of 1 month. Concentration–effect relationship was determined with ACY-1215 alone or in combination withverapamil 20 mmol/L to inhibit efflux pumps. B, Concentration–effect relationships were established for resistant and parental Ly10 at 48 and 72 hoursfollowing exposure to vorinostat, bortezomib, and romidepsin. C, SCID-beige mice were injected with LY10 107 in their flanks and treated with ACY-121550 mg/kg days 1–5, 8–12, 15–19 via the intraperitoneal route. D, Kaplan–Meier Curve was calculated for the resistant control mice as compared withthe resistant ACY-1215 mice, parental control, and treatment cohorts.
Amengual et al.
Clin Cancer Res; 23(12) June 15, 2017 Clinical Cancer Research3088
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

Given the known influence of ACY-1215 on the unfoldedprotein response (UPR; refs. 6, 7), evaluation of PERK and IRE-1 pathways were evaluated by immunoblot (Fig. 2D). The resis-tant line displayed relatively stableGRP78, themaster regulator ofthe UPR. The GRP78–PERK pathway also remained relativelystable. The IRE-1 pathway, however, was upregulated with con-
comitant activation of XBP-1 and AKT as compared withthe parental line perhaps driving accelerated growth in theseACY-1215–resistant cells. This corresponds to previouslypublished preclinical studies of CLL. Kriss and colleagues dem-onstrated that the Em-TCL1 mouse model was found to haveupregulated levels of the ER stress response pathway, in particular
B
D
(%) P-Untreated
P-Treated
R-Untreated
R-Treated
Live 74 35 69 65
Apopto�c 26 65 28 26
0
100,000
200,000
300,000
Inte
nsity
(RFU
)
Ly10 Parental
0
100,000
200,000
300,000
Inte
nsity
(RFU
)
Ly10 ResistantC
IC50 (mmol/L): 0.9 1.6 4.0 0.9 1.2 2.5 Bc
l2 :
BIM
Ra�
o
A Parental Resistant
HDAC6
Ac-Tubulin
GRP78
PERK
EIF-2α
ATF4
MAPK10
p-EIF-2α
p-IRE-1
IRE-1
XBP-1
p-AKT (S473)
AKT
β-Ac�n
β-Ac�n
PERK
Pat
hway
IRE-
1 Pa
thw
ay
Bim
Bcl2
DLBCL-ABC MCL TCL
OCI
-LY1
0
Hbl1
Jym
2
Mav
er
H9 HH
1,000
100
10
1
0.1
0.01
0.001
Parental Resistance
Untreated
Treated*
Figure 2.
The IRE-1/XBP-1 pathway is upregulated in the cells resistant to ACY-1215. A, Western blot analysis of a panel of lymphoma cell lines for Bcl2 and Bimwas compared with the IC50 in these cell lines. B, Mitochondrial membrane potential was measured following 48-hour exposure of cells to ACY-12152.5 mmol/L via flow cytometry. C, BH3 profiling was performed on the parental and resistant cell lines. D, Baseline characteristics of the resistant line wascompared with the parental line with respect to the unfolded protein response (UPR).
Selective HDAC6 Inhibitor has Synergy with Ibrutinib
www.aacrjournals.org Clin Cancer Res; 23(12) June 15, 2017 3089
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

IRE-1 and XBP-1 (12). In the Em-TCL1 model, the tonic IRE-1/XBP-1 pathway led to a constitutively active B-cell receptor path-way. In addition, in an XBP-1KD/Em-TCL1 mouse model, micewith knocked-downXBP-1had significantly slower progression toB-cell leukemia than XBP-1WT/Em-TCL1 mice (13). Together,these findings suggest a functional link between the IRE-1/XBP-1 and B-cell receptor pathways.
Gene expression profiling reveals distinct modulation of theB-cell receptor pathway in the resistant cell line as comparedwith the parental cell line
Gene expression profiling was performed on both the resistantand parental cell lines. The parental and resistant cell lines haddistinct gene expression signatures as represented by principalcomponent analysis and as can be visualized on the heatmap(Fig. 3A). The gene expression data were analyzed by GSEA andgene cluster analysis. There were 1,363 genes from resistant line 2-log fold upregulated as compared with the parental and 1825genes 2-log fold downregulated as compared with the parental(P < 0.05). GSEA revealed increased expression of pathwaysknown to drive lymphomagenesis of activated B-cell (ABC)lymphoma such as the BTK pathway (Fig. 3b). In addition tochanges in the UPR, differentially expressed genes in the resistantline included upregulation of MAPK10, HELIOS, HDAC9, andFYN, as well as downregulation of SH3BP5 (a negative regulatorof BTK) and LCK. The change in expression was confirmed byPCR (Fig. 3C) and Western blot analysis (Fig. 3D). Given theupregulation of FYN, a tyrosine kinase in the B-cell receptorpathway, and the downregulation of SH3BP5 a negative regulatorof the Bruton tyrosine kinase, as well as findings generated byGSEA, the resistant linewas treatedwith ibrutinib. Cell viability ofthe resistant and parental lines was evaluated over time. Ibrutinib2 mmol/L was able to overcome resistance with a 70% viabilityin the resistant line versus 64% viability in the parental lineat 72 hours (Fig. 3E). These data reveal that cells exposed toACY-1215, a selective HDAC6 inhibitor, rely heavily on the B-cellreceptor pathway for expansion. It also suggests that treatmentwith the combination of ACY-1215 and ibrutinib may lead to asynergistic interaction.
ACY-1215 plus ibrutinib is highly synergistic in lymphoma celllines and primary human lymphoma samples
On the basis of the findings generated from the resistant cellline, a panel of lymphoma cell lines were treated with ACY-1215,ibrutinib, or the combination and viability and synergy weremeasured over 24, 48, and 72 hours (Fig. 4A). Cell lines includedthe GCB-DLBCL OCI-Ly7, the ABC-DLBCL cell lines HBL1, OCI-Ly10, RIVA, mantle cell lymphoma (MCL) lines HBL2, JEKO1,REC1, and the T-cell lymphoma lineH9. As expected, synergy wasmost pronounced in the ABC-DLBCL and MCL cell lines withsynergy coefficients as low as 0.10 (Ly10) and 0.15(JEKO1),respectively (where RRR<1 connotes synergy). Both of thesedisease entities are known to be driven by tonic signaling of theB-cell receptor (BCR) pathway and are highly sensitive to BTKinhibitors. There was little-to-no synergy in GCB-DLBCL andT-cell lymphoma, respectively, as these cell lines do not rely onthe BCR pathway for growth. The heatmaps represent the viabilityor synergy of a panel of cell lines following treatment withACY-1215, ibrutinib or the combination at 24, 48, and 72 hours.Red boxes indicate lower viability and higher synergy, whereasblue boxes represent high viability and no synergy. Synergy was
calculated by the relative risk ration (RRR) where a RRR < 1connotes synergy.
To confirm the clinical relevance of this observation, threeprimary patient samples of leukemic phase lymphoma werecollected under an IRB-approved protocol. The patient samplesspanned three subtypes of lymphoma including chronic lympho-cytic lymphoma (CLL), lymphoplasmacytic B-cell lymphoma(LPL), and marginal zone lymphoma (MZL) harboring a 17pdeletion. These three diseases are known for their sensitivity toBTK inhibitors. Cells were treated with increasing concentrationsof ibrutinib in combination with ACY-1215 and viability andsynergy were measured after 24, 48, 72, and 96 hours. All three ofthe lymphoma subtypes achieved marked synergy with RRR of0.54, 0.43, and 0.22, respectively (Fig. 4B).
The molecular effects of the combination treatment was eval-uated in three lymphoma cell lines, 2 ABC-DLBCL (LY-10 andHBL-1) and one MCL line (JEKO1) as well as the primary humanMZL 17p- patient sample by immunoblot (Fig. 4C). The combi-nation led to a decrease in p-IRE1- a which has been shown tointerplay with the BTK pathway (12, 13). This corresponded toa decrease p-BTK, total BTK, and its downstream targets such asp-PLC2-g and CARD11. There was decreased expression ofSH3BP5, the negative regulator of the BTK in all cell lines. Thisis expected as its function is to inhibit autophosphorylation ofBTK and the cells treated with the combination exhibited com-plete inhibition of p-BTK (27). These findings show that targetingthe IRE1pathway of theUPR and the BTKpathwaywith a selectiveHDAC6 inhibitor and ibrutinib are synergistic at both the cyto-toxic and biologic level.
The combination of ACY-1215 and ibrutinib led to markedtumor growth delay and prolonged overall survival in axenograft model of lymphoma
The parental LY10 cell line was xenografted into the flanks ofSCID beige mice at 107 cells. Mice were divided into 4 cohorts,control, ACY-1215, ibrutinib, and the combination. Mice weretreated with ACY-1215 50 mg/kg days 1–5, 8–12, 15–19, andibrutinib 3mg/kg once daily on days 1–20. Both drugs were givenby intraperitoneal route (Fig. 5A). The combination of ACY-1215and ibrutinibwaswell toleratedwithweight loss observed in boththe ACY-1215 and combination cohorts that returned to baselineby day 20 (Fig. 5B). This finding is similar to that seen in priormouse studies of single agent and combinations with ACY-1215(6, 7). Mice demonstrated significant tumor growth delay fol-lowing treatment with the combination as compared with eitherACY-1215, ibrutinib, or untreated mice (P¼ 0.0003, P¼ 0.0006,and P < 0.0001, respectively; Fig. 5C). Mice treated with thecombination had a prolonged overall survival compared withthe control (Fig. 5D). Of the mice that completed one cycle oftherapy, the mean survival in days was as follows: combination(66.5) > ibrutinib (57.6) > ACY-1215 (56.6) > control (40.1) >resistant control (26.5).
Pharmacokinetic and pharmacodynamic effects of ACY-1215in combination with ibrutinib
The concentration of ACY-1215 and ibrutinib was measuredat sequential time points in serum and tumor tissue after asingle intraperitoneal injection of ACY-1215 (50 mg/kg) oribrutinib (3 mg/kg) or a combination of both. The concentra-tions achieved for both drugs are similar or greater than theconcentrations found to induce cytotoxicity in the in vitro
Amengual et al.
Clin Cancer Res; 23(12) June 15, 2017 Clinical Cancer Research3090
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

R P B
C D
A
0102030405060708090
100
1 2 3 4 5 6 7
Cell
surv
ival
(% o
f con
trol
)
Drug concentra�on (mmol/L)
LY10 Ibru�nib
48 h Resistant
72 h Resistant
48 h Parental
72 h Parental
Helios
FYN
β-Ac�n
Parental
SH3BP5
P-BTK (Y223)
P-PLCG2(Y759)
Resistant
BTK
PLCG2
FYN
IKZF2
SH3BP5
GAPDH
Parental ResistantHDAC6
HDAC9
LCK
MAPK10
0
0.5
1
1.5
Rela
�ve
to G
APD
H
Parental
Resistant
Parental (FPKM)
Resistant (FPKM)
Log2 fold change
1087 1506 0.5
2 4437 10.8
17 99 2.5
28 9 –1.6
15 1169 6.2
195 831 2
17080 2336 –2.9
56269 63070 0.16
Gene expression values
ParentalResistant
E
1050
–5–10–15
–50 500
PC1
Figure 3.
Resistant cell line has differentially expressed gene profile as compared with parental line and identifies that the BCR pathway is upregulated in resistant cells.A, Resistant (R) cells and parental cells (P) were evaluated by RNA Seq for gene expression. The two cells lines were distinct as demonstrated byprincipal component analysis. The heatmap represents the top 100 genes with significant overall 2-log fold change between the resistant and parental lines.B, Gene set enrichment analysis (GSEA) was performed to compare enrichment of pathways in resistant verses parental lines. C, Differentially expressedgenes of interest were confirmed via PCR for the resistant line as compared with the parental line. D, Protein expression of genes of interest wasconfirmed with immunoblot analysis. E, Concentration–effect relationships of ibrutinib in resistant and parental lines was evaluated at 48 and 72 hours.
Selective HDAC6 Inhibitor has Synergy with Ibrutinib
www.aacrjournals.org Clin Cancer Res; 23(12) June 15, 2017 3091
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

A
C
B
SH3BP5
MAPK10
BTK
p-PLC2-γ
IRE1-α
p-IRE1-α
HBL-1 JEKO-1 Primary Human MZL (17p-)
PLC2-γ
XBP-1s
p-BTK
CARD11
β-Ac�n
24 HOCI-LY-10
C A I AI
XBP-1u
C A I AI C A I AI C A I AI
1 5 10 1 5 10 1 5 10
24 Hours 48 Hours 72 Hours
Viab
ility
(per
cent
of c
ontr
ol)
DLB
CL
(GC) OCI-
LY7
0 84.9 63.2 39.6 86.0 52.3 17.4 96.6 76.2 17.51 83.1 63.8 40.3 91.2 50.4 13.9 101.1 73.0 11.7
1.5 76.4 62.0 42.3 85.6 48.8 9.4 88.0 62.2 11.1
DLB
CL (A
BC)
HBL10 99.0 91.6 84.1 72.5 74.0 58.5 67.2 64.4 40.51 90.5 85.2 63.7 52.8 47.9 28.9 46.5 34.9 19.9
1.5 83.3 68.3 53.6 48.2 38.5 14.4 32.4 23.8 9.2
OCI-LY10
0 75.1 63.0 37.6 43.8 24.7 10.8 25.9 9.6 2.71 56.7 40.1 13.9 16.4 5.8 1.7 4.8 0.9 0.9
1.5 34.8 22.4 6.0 5.4 1.3 0.7 0.8 0.5 0.6
RIVA0 88.6 87.9 72.8 78.7 76.3 68.1 72.3 67.5 59.21 82.5 70.4 25.1 69.9 63.0 23.7 62.9 54.0 19.1
1.5 71.5 56.1 17.1 66.3 49.7 15.7 56.0 41.0 11.8
MAN
TLE
CELL
HBL20 107.0 103.3 56.5 108.1 93.9 49.4 94.0 79.8 43.81 105.5 100.2 50.1 99.2 91.9 41.9 98.8 81.0 38.9
1.5 108.0 100.3 72.9 101.3 96.4 62.4 91.8 88.5 62.2
JEKO10 99.6 110.5 69.6 84.0 58.0 20.1 142.5 75.2 0.91 85.4 65.4 24.1 57.8 38.1 4.2 98.0 26.3 0.2
1.5 57.8 49.3 23.5 35.8 19.2 2.0 56.6 9.2 0.1
REC10 108.8 102.5 63.1 85.8 68.0 38.8 110.0 91.6 31.31 121.2 94.7 52.4 77.1 53.4 18.4 104.3 61.3 12.4
1.5 108.3 72.5 46.6 67.4 35.5 9.5 89.3 31.4 6.7
T-CE
LL
H90 100.7 99.5 92.3 100.2 99.1 85.1 105.2 95.1 85.31 100.5 101.0 72.2 101.8 96.8 85.3 101.7 101.6 80.7
1.5 99.0 101.1 93.3 99.2 99.8 83.3 100.1 94.2 82.9
1 5 10 1 5 10 1 5 10
24 Hours 48 Hours 72 Hours
RRR
DLB
CL
(GC) OCI-
LY7
1 1.03 1.09 1.04 1.06 0.99 0.96 1.07 0.82 0.67
1.5 0.96 1.03 1.08 1.05 0.96 0.97 1.14 0.56 0.75
DLB
CL (A
BC)
HBL11 0.91 0.91 0.73 0.93 0.80 0.57 0.76 0.61 0.52
1.5 0.87 0.87 0.62 0.77 0.68 0.48 0.66 0.32 0.29
OCI-LY10
0.5 0.94 0.79 0.46 0.49 0.31 0.21 0.21 0.11 0.39
1 1.01 0.77 0.35 0.43 0.18 0.24 0.10 0.16 0.68
RIVA1 1.00 1.07 1.06 0.86 0.99 0.98 0.37 0.42 0.39
1.5 0.89 1.05 1.05 0.71 0.81 0.82 0.26 0.29 0.27
MAN
TLE
CELL
HBL21 1.06 1.00 1.09 1.27 1.17 0.99 0.66 1.14 0.93
1.5 1.01 0.92 1.04 1.18 0.87 0.91 0.68 0.85 0.77
JEKO1
1 0.81 0.86 0.94 0.62 0.67 0.29 0.29 0.22 0.18
1.5 0.77 0.69 0.44 0.67 0.50 0.06 0.43 0.16 0.15
REC11 1.06 0.97 1.00 0.89 0.80 0.76 0.64 0.57 0.47
1.5 0.96 0.88 1.00 0.73 0.69 0.37 0.57 0.34 0.23
T-CE
LL
H91 1.00 1.05 0.96 1.02 1.01 1.06 0.79 1.04 0.94
1.5 1.02 1.02 1.10 1.05 1.04 1.15 1.04 1.01 1.12
Ibru�nib (mmol/L)
Ibru�nib (mmol/L) Ibru�nib (mmol/L)
Ibru�nib (mmol/L)
0 2 4 8 0 2 4 8 0 2 4 8 0 2 4 8ACY-1215 (μmol/L) 24 Hours 48 Hours 72 Hours 96 Hours
Viab
ility
(per
cent
of
con
trol
) CLL 0 100.0 99.1 95.2 83.5 100.0 75.9 68.9 52.8 100.0 58.1 59.1 38.1 100.0 60.0 48.8 27.02 98.2 90.4 87.9 69.1 83.8 57.0 49.6 32.2 81.9 43.4 37.0 18.7 83.8 36.8 29.4 12.1
LPL 0 100.0 145.9 152.2 114.3 100.0 125.9 118.5 126.6 100.0 133.9 142.0 97.1 100.0 117.5 116.6 81.52 107.5 118.8 111.1 94.9 88.7 88.5 80.9 48.1 94.7 94.3 81.2 71.9 75.8 51.3 59.8 31.9
MZL (17p-)
0 100.00 52.29 62.56 81.49 100.00 87.58 76.89 65.84 100.00 103.64 94.49 66.85 100.00 96.74 88.38 50.590.5 84.60 94.55 73.24 89.62 60.86 82.47 42.02 66.38 64.64 49.40 13.84 51.28 40.08 35.89 7.81 35.47
0.0 10.0 20.0 30.0 40.0 50.0 60.0 70.0 80.0 90.0 100.0
2 4 8 2 4 8 2 4 8 2 4 8
ACY-1215 (μmol/L) 24 Hours 48 Hours 72 Hours 96 Hours
RRR
CLL 2 0.93 0.94 0.84 0.9 0.86 0.73 0.91 0.77 0.6 0.73 0.72 0.54LPL 2 0.76 0.68 0.77 0.79 0.77 0.43 0.74 0.6 0.78 0.58 0.68 0.52
MZL (17p-) 0.5 2.14 1.38 1.3 1.55 0.9 1.66 0.76 0.23 0.53 0.93 0.22 1.75
0 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1% Viability RRR
ACY-1215
(μmol/L)
ACY-1215
(μmol/L)
Figure 4.
Ibrutinib plus ACY-1215 is synergistic in cell lines and primary human lymphoma samples. A, Heatmap represents the viability of a panel of cell lines followingtreatment with ACY-1215, ibrutinib, or the combination at 24, 48, and 72 hours. Red boxes indicate lower viability. Synergy was calculated by the relativerisk ratio (RRR). RRR < 1 connotes synergy and is represented by red boxes. B, Primary human lymphoma samples, chronic lymphocytic leukemia (CLL),lymphoplasmacytic lymphoma (LPL), and 17p deleted marginal zone lymphoma (MZL), were treated with ACY-1215, ibrutinib, or the combination over 24 to96 hours. Viability was measured and synergy was calculated by RRR and represented in the heatmaps. C, The IRE-1 and BTK pathways were evaluatedfollowing treatment with the combination of ibrutinib and ACY-1215 by immunoblot analysis.
Amengual et al.
Clin Cancer Res; 23(12) June 15, 2017 Clinical Cancer Research3092
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

experiments. In addition, these concentrations also recapitulatewhat has been described in human pharmacokinetic studies.There was no difference in the concentrations of either drug inresistant or parental mice therefore these data were pooled foranalysis (Fig. 6A and B).
The average ACY-1215 serum concentration reached at 0.5and 1 hour after administration was 438 (�85) and 327 (�133)ng/mL, respectively. The average serum concentration ofACY-1215 at 6 and 8 hours was 182 (�80) and 200 (�89)ng/mL, resulting in an average half-life of 5.3 hours and anaverage AUC0-6h, AUC0-8h, and AUC0-inf of 1,425, 2,013, and3,262 hour/ng/mL, respectively, for both single administrationof ACY-1215 and in combination with ibrutinib in both paren-tal and resistant groups. There was no substantial difference inserum pharmacokinetics of ACY-1215 between groups andtreatments, which was also observed for tumor concentrationsof the drug. Mean (þSD) tumor concentrations for singleadministration of ACY1215 and the combination with ibruti-nib in the parental and resistant group at 4, 6, and 8 hours afterinjection were 94 (�47), 80 (�38), and 45 (�18) ng/mL,respectively (Fig. 6C).
The serum pharmacokinetics of ibrutinib exhibited no sub-stantial differences when the drug was administered alone or incombination with ACY-1215. The average ibrutinib serum con-centration reached at 0.5 and 1 hour after administration was778 (�85) and 224 (�183) ng/mL, respectively. The average
serum concentration of ibrutinib at 6 and 8 hours was13 (�22) and 6 (�6) ng/mL, resulting in an average half-lifeof 1.1 hours and an average AUC0-8h and AUC0-inf of 752, and757 h/ng/mL, respectively, for both single administration ofibrutinib and in combination with ACY-1215 in both parentaland resistant groups. Ibrutinib tumor concentrations were belowthe lowest limit of quantification in most samples (Fig. 6B).
Immunoblot analysis of mouse tumor tissue was evaluatedfor modulation of the IRE1 and BTK pathways following6 hours of exposure to ACY-1215, ibrutinib, or the combi-nation. Following the short, single exposure to the drugs therewas reduction of p-BTK and corresponding reduction ofthe downstream targets p-PLC2-g and CARD11 (Fig. 6D)which is most pronounced in the combination. These resultsconfirm those demonstrated in the cell lines treated with thecombination.
DiscussionThe development of this ACY-1215–resistant cell line has
proven to be a powerful tool to identify rational drug partners.As treatment strategies for malignancies evolve, targetedapproaches have become exceedingly specific. Although newhighly selective drugs have efficacy against singular targets, whatcollateral effects these new agents have on other pathways is notimmediately apparent. Utilizing gene expression profiling and
A
D
* *****
* P = 0.0003** P = 0.0006***P < 0.0001
B
C
5 10 15 20
ACY-1215 (50 mg/kg)
Ibrutinib (3 mg/kg)
23
22.5
22
21.5
21
20.5
20
19.50 5 10 15 20 25
Wei
gh
t (g
)
Day
Control
ACY-1215
Ibrutinib
Combo
2,000
1,500
1,000
500
00 20 40 60
Tum
or
volu
me
(mm
3 )
Per
cen
t su
rviv
al
Day Day
Control
ACY-1215
Ibrutinib
Combo
(R) Control(P) Control(P) ACY-1215(P) Ibrutinib(P) Combo
100
50
00 20 40 60 80 100
OCI-LY10 Parental engrafted mice Kaplan–Meier plot
Figure 5.
The combination of ACY-1215 and ibrutinib leads to statistically significant tumor growth delay compared with single-agent treatment in a xenograftmouse model of lymphoma. A, SCID-beige mice were injected with LY10 107 in their flanks and treated with ACY-1215 50 mg/kg days 1–5, 8–12, 15–19, ibrutinib3 mg/kg days 1–20, or the combination via the intraperitoneal route. B, Mice were weighed every 3 to 4 days as a measurement for toxicity. C, Tumorvolume was measured over time as a function of treatment group. D, Kaplan–Meier curve was calculated for the resistant control mice as compared with theparental control and treatment cohorts.
Selective HDAC6 Inhibitor has Synergy with Ibrutinib
www.aacrjournals.org Clin Cancer Res; 23(12) June 15, 2017 3093
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

gene set enrichment analysis we identified that the BTK pathwaycircumnavigated resistance to tonic HDAC6 inhibition.
The resistant line displayed upregulation of the IRE1 pathwayof the UPR as compared with the parental line. This is in keepingwith observations made in models of CLL where inhibition ofIRE1 led to impaired growth through XBP-1 mediated down-regulation of the BTK pathway. In Em-TCL1 mice knocked downfor XBP-1 mice displayed decreased signaling through the B-cellreceptor pathway as revealed by decreased p-BTK. This corre-sponded to slower progression to leukemia relative to age-matched controls (13). By inhibiting IRE1, similar findings werereplicated establishing a link between the unfolded proteinresponse and the B-cell receptor pathway. Recent publicationshave established other links withHDACs and signaling of the BTK
pathway. HDAC inhibition has been shown to restore the expres-sion of BTK-targeting miRNA, leading to decreased signaling ofthe BTK pathway and ultimately apoptosis (28). Combinationsof panobinostat or abexinostat with ibrutinib were synergisticand overcame BTK mutations known to induce ibrutinib resis-tance. In addition, HDAC6 has been linked to the deacetylationand activation of MYD88, a toll-like receptor kinase known tointerplay with the BTK pathway. HDAC6 inhibition with tubacinor vorinostat acetylated and abrogated the effects of MYD88leading to cell-cycle arrest and cell death (29). These three exam-ples point to the interconnectedness of HDAC modulation andBTK signaling.
Our findings reveal that tonic inhibition of HDAC6 leads toupregulation of the IRE1 pathway of the UPR. This in turn was
A B
C D C A I AI
SH3BP5
MAPK10
BTK
p-PLC2-γ
IRE1-αp-IRE1-α
PLC2-γ
XBP-1s
p-BTK
CARD11
β-Ac�n
XBP-1u
ACY-1215 Ibru�nib
SERUM
(ng/mL)0.5 h1.0 h
438 (±83)327 (±133)
778 (±85)224 (±183)
T1/2 (h) 5.3 1.1
AUC (h*ng/mL)0−6 h0−8 h0−inf h
1,4242,0133,262
- - -752757
TUMOR
(ng/mL)4 h6 h8 h
94 (±47)80 (±38)45 (±18)
Below the limit
of detec�on
500
400
300
200
100
00 2 4 6 8 10 0 2 4 6 8 10
AC
Y-1
215
(ng
/mL
)
Ibru
tin
ib (
ng
/mL
)
Time (hr) Time (hr)
ACY alone (serum)ACY in combo (serum)ACY alone (tumor)ACY in combo (tumor)
Ibrutinib alone (serum)Ibrutinib in combo (serum)
Ibrutinib alone (tumor)Ibrutinib in combo (tumor)
1,000
800
600
400
200
0
Figure 6.
Pharmacokinetic and pharmacodynamic effects of ACY-1215 in combination with ibrutinib in mice. Serum and tumor tissue was collected from mice atsequential time points and analyzed for concentration of ACY-1215 and ibrutinib by LC/MS-MS. Mice were treated with ACY-1215 at 50 mg/kg aloneand ACY-1215 50 mg/kg with ibrutinib 3 mg/kg. Drug concentrations are represented as mean values. A, Graphical representation of ACY-1215concentration over time. Mice received one dose of ACY-1215 50 mg/kg or ACY-1215 50 mg/kg plus ibrutinib 3 mg/kg for analysis of serum concentrationof ACY-1215. For analysis of drug concentration in tumor tissue, ACY-1215 was administered at 50 mg/kg with or without ibrutinib. B, Graphicalrepresentation of ibrutinib concentration over time analyzed in serum and tumor tissue. Mice received one dose of ibrutinib 3 mg/kg via intraperitonealroute. C, Summary of pharmacokinetic data for ACY-1215 and ibrutinib. D, Immunoblot analysis of the IRE1 pathway of the UPR and the BTK pathwayfrom whole-cell lysates of mouse tumor tissue treated with ACY-1215, ibrutinib or the combination. Mice were treated with a single intraperitoneal injection andanalyzed at 6 hours.
Amengual et al.
Clin Cancer Res; 23(12) June 15, 2017 Clinical Cancer Research3094
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

associated with upregulation of the B-cell receptor pathway asevidenced by RNA sequencing, GSEA, and immunoblot analysis.Confirmation of the interplay between the UPR and the BCRpathway were further established by demonstrating synergybetween ACY-1215, a selective HDAC6 inhibitor, and ibrutinibacross a panel of cell lines (ABC-DLBCL and MCL) known to besensitive to BTK inhibitors. Furthermore, this synergy was alsoestablished in three primary human lymphoma samples of sub-types also known to be sensitive to BTK inhibitors: CLL, LPL, andMZL. The combinationwas highly synergistic in a rapidly growing17p- deleted MZL demonstrating a novel approach to thesechallenging diseases.
The combination of ACY-1215 and ibrutinib led to markedinhibition of p-IRE1 and p-BTK compared with either of thedrugs alone and this corresponded to inhibition of downstreamtargets of the BCR such as p-PLC-g and CARD11. These findingswere observed in cell lines, primary human lymphoma samplesand xenograft models of lymphoma. In addition, the combi-nation was well-tolerated in mice. Ly10-xenografted mice trea-ted with the combination had statistically significant tumorgrowth delay compared with those treated with either drugalone.
Although it is well established that ibrutinib is effective forpatients with 17p- CLL and MCL, clinical experience hasinformed us that these responses though durable often arenot permanent (30, 31). It has been observed that patientsrelapsing off of ibrutinib have highly aggressive and oftenexplosive disease. Our findings demonstrate that combiningibrutinib with ACY-1215 has potent synergy and that thiscombination is effective at inhibiting the most aggressivesubtypes of lymphoma.
The gene expression data derived from the resistant cell linealso revealed other potential druggable targets. FYN, a Srckinase which plays a crucial role in signaling in the T-cell andB-cell receptor pathways, was also found to be upregulated inthe resistant cell line (32, 33). This kinase is known to beinhibited by dasatinib and combination therapy of dasatinibplus ACY-1215 is being explored. Helios was also upregulatedin the resistant line. Helios is a member of the Ikaros family ofDNA-binding protiens and is found to be mainly expressed inprecursor cells of T-cell lineage. Little is known about Helios'effects in B lymphocytes but ectopic overexpression has led tolymphomagenesis in transgenic mice (34). Most of Helios isfound to be bound to Ikaros, the effects of which are unknown.In models of myeloma, Ikaros in known to be selectivelyubiquitinated and degraded by lenalidomide via cereblonubiquitin ligase (35). Studies evaluating the combination oflenalidomide and ACY-1215 are currently underway in mye-loma and how these findings may be translated to B-celllymphoma are presently under study. Finally, HDAC9 wasfound to be upregulated in the resistant cell line. HDAC9 isa member of the class IIa family and resides in both the nucleusand cytoplasm. Although the function of HDAC9 is not wellstudied, it is likely that its targets may overlap with HDAC6.Upregulation of HDAC9 may have been induced in resistant
line as a collateral effect to overcome tonic HDAC6 inhibition.Pan-class HDAC inhibition with romidepsin was able to over-come this effect as the resistant line was sensitive to treatmentwith romidepsin.
Developing a drug-resistant cell line is an under-utilized strat-egy to identify rational and synergistic drug-drug combinations.This strategy could be applied broadly and may proactivelyidentify pathways co-opted by malignant cells upon inhibitionby highly selective targeted agents. Thefindings of thismanuscriptidentified the synergistic interaction of ACY-1215, a selectiveHDAC6 inhibitor, and ibrutinib the first-in-class BTK inhibitorvia this technique. Translationof thesefindings to the clinic is nowunderway.
Disclosure of Potential Conflicts of InterestJ.E. Amengual reports receiving a commercial research grant from Acetylon
Pharmaceuticals, Inc. No potential conflicts of interest were disclosed by theother authors.
Authors' ContributionsConception and design: J.E. Amengual, S.A. Prabhu, P.M. Johannet, S. Cremers,O.A. O'ConnorDevelopment of methodology: J.E. Amengual, S.A. Prabhu, M. Lombardo,P.M. Johannet, Y. Wei, R. Nandakumar, S. Cremers, O.A. O'ConnorAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): J.E. Amengual, S.A. Prabhu,K.M. Zullo, P.M. Johannet,Y. Gonzalez, X. Jirau-Serrano, R. Nandakumar, S. CremersAnalysis and interpretation of data (e.g., statistical analysis, biostati-stics, computational analysis): J.E. Amengual, S.A. Prabhu, M. Lombardo,K.M. Zullo, Y. We, J.K. Duong, R. Nandakumar, S. Cremers, A. Verma,O. Elemento, O.A. O'ConnorWriting, review, and/or revision of the manuscript: J.E. Amengual, M. Lom-bardo, P.M. Johannet, L. Scotto, R. Nandakumar, S. Cremers, O.A. O'ConnorAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): J.E. Amengual, S.A. Prabhu, M. Lombardo,K.M. Zullo, Y. Gonzalez, O.A. O'ConnorStudy supervision: J.E. Amengual, L. Scotto, X. Jirau-Serrano, O.A. O'Connor
AcknowledgmentsWe would like to kindly thank Anthony Letai, MD, PhD, for providing
technical support for BH3 profiling functional assays.
Grant SupportThis work was supported by the Amos Medical Faculty Development
Program of the American Society of Hematology and Robert Wood JohnsonFoundations and the Columbia University Provost Award for Junior Faculty,research funding from Acetylon Pharmaceuticals, Inc (J.E. Amengual), theAmerican Society of Hematology HONORS Award Program (P.M. Johannet)and the National Center for Advancing Translational Sciences, NIH, (UL1TR00004; S.Cremers), and (R01 CA194547; O. Elemento). We would also liketo acknowledge the Lymphoma Research Fund of Columbia University for itsgenerous support.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received August 11, 2016; revised November 22, 2016; accepted November23, 2016; published OnlineFirst December 19, 2016.
References1. Duvic M, Talpur R, Ni X, Zhang C, Hazarika P, Kelly C, et al. Phase 2 trial of
oral vorinostat (suberoylanilide hydroxamic acid, SAHA) for refractorycutaneous T-cell lymphoma (CTCL). Blood 2007;109:31–9.
2. Piekarz RL, Frye R, PrinceHM, KirschbaumMH,Zain J, Allen SL, et al. Phase2 trial of romidepsin in patients with peripheral T-cell lymphoma. Blood2011;117:5827–34.
Selective HDAC6 Inhibitor has Synergy with Ibrutinib
www.aacrjournals.org Clin Cancer Res; 23(12) June 15, 2017 3095
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

3. O'Connor OA, Horwitz S, Masszi T, Van Hoof A, Brown P, Doorduijn J,et al. Belinostat in patients with relapsed or refractory peripheral T-celllymphoma: results of the pivotal phase II BELIEF (CLN-19) Study. J ClinOncol 2015;33:2492–9.
4. Ning ZQ, Li ZB, Newman MJ, Shan S, Wang XH, Pan DS, et al. Chidamide(CS055/HBI-8000): a new histone deacetylase inhibitor of the benzamideclass with antitumor activity and the ability to enhance immune cell-mediated tumor cell cytotoxicity. Cancer Chemother Pharmacol 2012;69:901–9.
5. San-Miguel JF, Hungria VT, Yoon SS, Beksac M, Dimopoulos MA, Elghan-dour A, et al. Panobinostat plus bortezomib and dexamethasone versusplacebo plus bortezomib and dexamethasone in patients with relapsed orrelapsed and refractory multiple myeloma: a multicentre, randomised,double-blind phase 3 trial. Lancet Oncol 2014;15:1195–206.
6. Amengual JE, Johannet P, LombardoM, Zullo K, HoehnD, Bhagat G, et al.Dual targeting of protein degradation pathways with the selective HDAC6inhibitor ACY-1215 and bortezomib is synergistic in lymphoma. ClinCancer Res 2015;21:4663–75.
7. Santo L, Hideshima T, Kung AL, Tseng JC, Tamang D, Yang M, et al.Preclinical activity, pharmacodynamic, and pharmacokinetic properties ofa selective HDAC6 inhibitor, ACY-1215, in combination with bortezomibin multiple myeloma. Blood 2012;119:2579–89.
8. Yee AJ, BensingerW, Voorhees PM, Berdeja JG, Richardson PJ, Supko J, et al.Ricolinostat (ACY-1215), a selective HDAC6 inhibitor, in combinationwith lenalidomide and dexamethasone: results of a phase 1b trial inrelapsed and relapsed refractory multiple myeloma. Blood 2014;124:4772–4772.
9. Niesvizky R, Richardson PG, Gabrail NY,Madan S, Yee AJ, Quayle SN, et al.ACY-241, a novel, HDAC6 selective inhibitor: synergy with immunomod-ulatory (IMiD�) drugs in multiple myeloma (MM) cells and early clinicalresults (ACE-MM-200 Study). Blood 2015;126:3040–3040.
10. Vogl DT, Raje N, Hari P, Jones SS, Supko JG, LeoneG, et al. Phase 1B resultsof ricolinostat (ACY-1215) combination therapy with bortezomib anddexamethasone in patients with relapsed or relapsed and refractory mul-tiple myeloma (MM). Blood 2014;124:4764–4764.
11. Raje NS, Bensinger W, Cole CE, Lonial S, Jagannath S, Arce-Lara CE, et al.Ricolinostat (ACY-1215), the first selective HDAC6 inhibitor, combinessafely with pomalidomide and dexamethasone and shows promising earlyresults in relapsed-and-refractory myeloma (ACE-MM-102 Study). Blood2015;126:4228–4228.
12. Kriss CL, Pinilla-Ibarz JA,MaillouxAW, Powers JJ, TangCH, KangCW, et al.Overexpression of TCL1 activates the endoplasmic reticulum stressresponse: a novel mechanism of leukemic progression in mice. Blood2012;120:1027–1038.
13. Tang C-HA, Ranatunga S, Kriss CL, Cubitt CL, Tao J, Pinilla-Ibarz JA, et al.Inhibition of ER stress–associated IRE-1/XBP-1 pathway reduces leukemiccell survival. J Clin Invest 2014;124:2585–2598.
14. Paoluzzi L, Gonen M, Gardner JR, Mastrella J, Yang D, Holmlund J, et al.Targeting Bcl-2 family members with the BH3 mimetic AT-101 markedlyenhances the therapeutic effects of chemotherapeutic agents in in vitro andinvivo models of B-cell lymphoma. Blood 2008;111:5350–5358.
15. Marchi E, Paoluzzi L, Scotto L, Seshan VE, Zain JM, Zinzani PL, et al.Pralatrexate is synergistic with the proteasome inhibitor bortezomib ininvitro and invivomodels of T-cell lymphoid malignancies. Clin Cancer Res2010;16:3648–58.
16. Ryan J, Letai A. BH3 profiling in whole cells by fluorimeter or FACS.Methods 2013;61:156–164.
17. SubramanianA, TamayoP,Mootha VK,Mukherjee S, Ebert BL,GilletteMA,et al. Gene set enrichment analysis: a knowledge-based approach for
interpreting genome-wide expression profiles. ProcNat Acad Sci 2005;102:15545–15550.
18. Shaffer AL,WrightG, Yang L, Powell J, NgoV, Lamy L, et al. A library of geneexpression signatures to illuminate normal and pathological lymphoidbiology. Immunol Rev 2006;210:67–85.
19. Kalac M, Scotto L, Marchi E, Amengual J, Seshan VE, Bhagat G, et al. HDACinhibitors and decitabine are highly synergistic and associated with uniquegene-expression and epigenetic profiles in models of DLBCL. Blood2011;118:5506–5516.
20. Yang Y, Shaffer AL III, Emre NC, Ceribelli M, Zhang M, Wright G, et al.Exploiting synthetic lethality for the therapy of ABC diffuse large B celllymphoma. Cancer Cell 2012;21:723–737.
21. Zhao L, Wientjes MG, Au JL. Evaluation of combination chemotherapyintegration of nonlinear regression, curve shift, isobologram, and combi-nation index analyses. Clin Cancer Res 2004;10:7994–8004.
22. Gottesman MM, Fojo T, Bates SE. Multidrug resistance in cancer: role ofATP-dependent transporters. Nat Rev Cancer 2002;2:48–58.
23. Bradner JE, West N, Grachan ML, Greenberg EF, Haggarty SJ, Warnow T,et al. Chemical phylogenetics of histone deacetylases. Nat Chem Biol2010;6:238–243.
24. Chen S, Zhang Y, Zhou L, Leng Y, Lin H, Kmieciak M, et al. A Bim-targetingstrategy overcomes adaptive bortezomib resistance in myeloma through anovel link between autophagy and apoptosis. Blood 2014;124:2687–97.
25. Thomas A, El Rouby S, Reed JC, Krajewski S, Silber R, Potmesil M, et al.Drug-induced apoptosis in B-cell chronic lymphocytic leukemia: relation-ship between p53 genemutation and bcl-2/bax proteins in drug resistance.Oncogene 1996;12:1055–62.
26. Moore VDG, Letai A. BH3 profiling–measuring integrated function of themitochondrial apoptotic pathway to predict cell fate decisions. Cancer Lett2013;332:202–205.
27. Yamadori T, Baba Y, Matsushita M, Hashimoto S, Kurosaki M, KurosakiT, et al. Bruton's tyrosine kinase activity is negatively regulated by Sab,the Btk-SH3 domain-binding protein. Proc Natl Acad Sci U S A 1999;96:6341–6346.
28. Bottoni A, Rizzotto L, Lai TH, LiuC, Smith LL,Mantel R, et al. Targeting BTKthroughmicroRNA in chronic lymphocytic leukemia. Blood. 2016 Oct 17.[Epub ahead of print].
29. NewM, Sheikh S, Bekheet M, Olzscha H, Thezenas ML, Care MA, et al. TLRadaptor protein MYD88 mediates sensitivity to HDAC inhibitors via acytokine-dependent mechanism. Cancer Res 2016;79:6975–87.
30. Woyach JA, Furman RR, Liu T-M, Ozer HG, Zapatka M, Ruppert AS, et al.Resistancemechanisms for the Bruton's tyrosine kinase inhibitor ibrutinib.N Engl J Med 2014;370:2286–2294.
31. Landau D, Landau DA, Wu CJ. Clonal evolution in patients with chroniclymphocytic leukemia (CLL) developing resistance to BTK inhibition.Blood 2013;122:866–866.
32. Gauld SB, Cambier JC. Src-family kinases in B-cell development andsignaling. Oncogene 2004;23:8001–6.
33. Palomero T, Couronn�e L, Khiabanian H, KimM-Y, Ambesi-ImpiombatoA, Perez-Garcia A, et al. Recurrent mutations in epigenetic regulators,RHOA and FYN kinase in peripheral T cell lymphomas. Nat Genet2014;46:166–70.
34. Dovat S, Montecino-Rodriguez E, Schuman V, Teitell MA, Dorshkind K,Smale ST. Transgenic expression of Helios in B lineage cells alters B cellproperties and promotes lymphomagenesis. J Immunol 2005;175:3508–15.
35. Kronke J, Udeshi ND, Narla A, Grauman P, Hurst SN, McConkey M, et al.Lenalidomide causes selective degradation of IKZF1 and IKZF3 inmultiplemyeloma cells. Science 2014;343:301–5.
Clin Cancer Res; 23(12) June 15, 2017 Clinical Cancer Research3096
Amengual et al.
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022

2017;23:3084-3096. Published OnlineFirst December 19, 2016.Clin Cancer Res Jennifer E. Amengual, Sathyen A. Prabhu, Maximilian Lombardo, et al. Ibrutinib
withInhibitor Ricolinostat Reveals Rational Drug-Drug Combination Mechanisms of Acquired Drug Resistance to the HDAC6 Selective
Updated version
10.1158/1078-0432.CCR-16-2022doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2016/12/17/1078-0432.CCR-16-2022.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/23/12/3084.full#ref-list-1
This article cites 34 articles, 15 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/23/12/3084.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/23/12/3084To request permission to re-use all or part of this article, use this link
on July 5, 2020. © 2017 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 19, 2016; DOI: 10.1158/1078-0432.CCR-16-2022