Embed Size (px)
Citation preview

Dr. Adelina Vlad, MD PhD
Associate Professor, Physiology Department
UMPh ,Carol Davila’ Bucharest
Mechanical Properties of the Heart

Myocardial Properties
EXCITABILITY/ bathmotropia
AUTOMATICITY/ chronotropia
CONDUCTIBILITY/ dromotropia
CONTRACTILITY/ inotropia
RELAXATION/ lusitropia

Mechanical Properties of the Heart
Contractility inotropia
Relaxation lusitropia

Mechanical properties of
I. The myocardial fiber
II. The heart as a whole

I. Mechanical Events of the
Myocardial Fiber

Types of Muscles

Muscle Properties

Cardiac Muscle vs Skeletal Muscle

The Myocardial Fiber Striated, structurally similar, but not identical with the skeletal
muscle fiber

Skeletal Muscle

Skeletal Muscle

The Sarcomere

The Sarcomere


Structure of Thin and Thick Filaments

The Role of Ca2+ in Triggering
Contraction

Z line
M band
Structural Proteins of the Sarcomere
Actin Myosin

TitinAnchoring part
Elastic segment
Actin
Myosin
Moderate
stretch
Important stretch

The Cross-Bridge Cycle
Each cycle advances the myosin head by two actin monomers

The Cross-Bridge Cycle


Calcium Transport and Storage

The transverse
tubules (T tubules)
are extensions of
the plasma
membrane,
penetrating the
muscle cell at two
points in each
sarcomere:
the junctions of the A and I bands
The Triad

The Tetrade A tetrad of four L-
type Ca2+
channels on the T tubules faces a single Ca2+-release channel of the SR
Each L-type Ca2+
channel interacts with the foot of one of the four subunits of the Ca2+-release channel

Excitation-Contraction Coupling

Cardiac Contraction Requires Ca2+
Entry Through L-type Ca2+ Channels
EC coupling in skeletal muscle does not require Ca2+ influx
through L-type Ca2+ channels - the linkage between activated L-
type Ca2+ channels (Cav1.2, dihydropyridine receptors) in the T-
tubule membrane and the Ca2+ release channels is mechanical
and does not require Ca2+ entry per se
Cardiac contraction has an absolute requirement for Ca2+ influx
through these channels during the action potential.
The increase in [Ca2+]i resulting from Ca2+ influx alone is not
sufficient to initiate contraction is greatly amplified by Ca2+-
induced Ca2+ release from the SR through the Ca2+-release
channels, because the Ca2+-release channels remain open for a
longer period than do L-type Ca2+ channels

Calcium-Induced Calcium Release

Particularities of the Myocardial
EC-Coupling The initiating event
in the skeletal muscle is the arrival of an action potential at the
neuromuscular junction, the release of acetylcholine, and the
initiation of an end-plate potential.
in the ventricular myocyte, action potentials in adjacent
myocytes depolarize the target cell through gap junctions and
generate an action potential
T tubules
unlike skeletal muscle cells, cardiac myocytes also have axial
T tubules that run parallel to the long axis of the cell and
interconnect adjacent radial T tubules

Particularities of Myocardial EC-
Coupling
Cardiac contraction requires Ca2+ entry through L-type Ca2+
channels
Cardiac myocytes have a very high density of mitochondria and
thus are capable of sustaining very high rates of oxidative
phosphorylation (i.e., ATP synthesis, that fuels the cross-bridge
cycling, as well as the termination of contraction)

E-C Coupling in the Skeletal Muscle

E-C Coupling in the Cardiac Muscle

Ca2+ Removal From the Cytoplasm
After you activate your book, you will get

Termination of Contraction The relaxation of the contractile proteins depends on:
(1) extrusion of Ca2+ into the extracellular fluid
(2) re-uptake of Ca2+ from the cytosol by the SR
(3) dissociation of Ca2+ from troponin C

Termination of Contraction (2) and (3) are highly regulated:
Phospholamban (PLN), an integral SR membrane protein, inhibits
SERCA2a.
Phosphorylation of PLN by any of several kinases relieves
phospholamban's inhibition of SERCA2a, allowing Ca2+
resequestration to accelerate
an increase in the rate of cardiac muscle relaxation (e. g. by β1-
adrenergic agonists)
β1-Adrenergic agonists accelerate relaxation by promoting
phosphorylation of troponin I, which in turn enhances the dissociation of Ca2+ from troponin C.

Phosphorylation of Phospholamban and of Troponin I
Speeds Cardiac Muscle Relaxation

Increasing the Entry of Ca2+ Enhances
the Contractile Force
In skeletal muscle the strength of contractions is regulated by
frequency summation and multiple-fiber summation
In cardiac muscle
frequency summation is precluded the strength of cardiac
muscle contraction is regulated by modulating the
contractile force generated during each individual muscle
twitch
contractile function is regulated by:
modulating the magnitude of the rise in [Ca2+]i
altering the Ca2+ sensitivity of the regulatory proteins

Effects of NE on Contractility
Norepinephrine increase the contractile force of the heart:
acts through the β-type adrenergic receptor
increases the generation of cAMP activates PKA
phosphorylate the L-type Ca2+ channels = increases the
influx of Ca2+ an increase in contractile force.
the cAMP pathway also increases the Ca2+ sensitivity of the
contractile apparatus by phosphorylating one or more of the
regulatory proteins an increase in the force generated for
any given [Ca2+]i.

The Effects of Sympathetic Stimulation
on Contraction and Relaxation

Effects of ACh on Contractility
ACh, acting through muscarinic ACh receptors, raises
intracellular cGMP concentrations
the cGMP-dependent phosphorylation of L-type Ca2+
channels at sites distinct from those phosphorylated by the
cAMP-dependent kinase,
causes a decrease in Ca2+ influx during the cardiac action
potential and thus a decrease in the force of contraction

Cardiac Glycosides (Digitalis)
Digitalis

Antagonists and Agonists of L-type
Ca2+ Channels
After you activate your book, you will get

SKELETAL MUSCLE CARDIAC MUSCLE
Mechanism of
excitation
Neuromuscular transmission Pacemaker potentials.
Electrotonic depolarization
through gap junctions
Electrical activity of
muscle cell
Action potential spikes Action potential plateaus
Ca2+ sensor Troponin Troponin
Excitation-
contraction coupling
L-type Ca2+ channel (DHP receptor)
in T-tubule membrane coupling to
Ca2+-release channel (ryanodine
receptor) in SR
Ca2+ entry through L-type
Ca2+ channel (DHP
receptor) triggers Ca2+-
induced Ca2+ release from
SR
Terminates
contraction
Breakdown of ACh by
Acetylcholinesterase
Action potential
repolarization
Twitch duration 20-200 ms 200-400 ms
Regulation of force Frequency and multifiber
summation
Regulation of calcium entry
Metabolism Oxidative, glycolytic Oxidative

Single Twitch and Tetanus in the
Skeletal Muscle


The Law of Periodic Unexcitability The heart is unexcitable during systole

Muscle Length and Tension


Types of Contraction

II. Mechanical Events of the Whole
Heart

Muscle Layers of the Myocardium
The spiral bundle
contraction wrings the blood
out of the ventricle
The contraction of the apex
before of the bases of the
ventricle propels blood
upward to the Ao and PA
LV
RV
PA
Ao
Tricuspid
Mitral

Geometry of Right Venticular
Contraction
A small movement
of the free wall
ejects a large
volume due to its
large surface area
RV ejects a large
volume at low
pressure

Geometry of Left Venticular
Contraction
The conical shape
of the lumen gives
the LV a smaller
surface-to-volume
ratio than the RV
helps LV to
generate high
pressures
RV
LV
1
2

Comparison of the LV and RV
Contraction
RIGHT VENTRICULAR PRESSURE AND FLOW LEFT VENTRICULAR PRESSURE AND FLOW
RV
LV
Peak systolic:
130 mm Hg
End dyastolic:
10 mm Hg
Peak systolic:
30 mm Hg
End dyastolic:
6 mm Hg

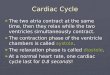
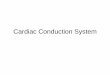
The Cardiac Cycle The sequence of mechanical and electrical events that repeats
with every heartbeat is called the cardiac cycle.
The cardiac cycle consists of a period of relaxation called
diastole, during which the heart fills with blood, followed by a
period of contraction called systole.
The duration of the cardiac cycle is the reciprocal of heart rate:
For a heart rate of 75 beats/min, the cardiac cycle lasts 0.8 s

The Cardiac Cycle
The electrical pacemaker in the sinoatrial node determines the
duration of the cardiac cycle
The electrical properties of the cardiac conduction system and
cardiac myocytes determine the relative duration of contraction
and relaxation

The Closing and Opening of the Cardiac Valves Define
Four Phases of the Cardiac Cycle
Cardiac valves open
passively when upstream
pressure exceeds
downstream pressure.
They close passively when
downstream pressure
exceeds upstream pressure.

Pressure Gradients in the Heart


Cardiac Cycle of the Atria Durig diastole atria opperate as passive reservoirs
Atrial contraction enhances ventricular filling and cardiac
output to a small degree.
For a heart rate of 75 (cycle duration = 0,8 s), atrial systole lasts
0,1 s and atrial diastole, 0,7 s

Cardiac Cycle of The Ventricles The cardiac cycle of the ventricles can be divided in four
phases:
1. Inflow phase (VENTRICULAR FILLING)
2. Isovolumetric contraction
3. Outflow phase (EJECTION)
4. Isovolumetric relaxation
Systole includes phases 2 and 3, and diastole includes phases
4 and 1.
For a heart rate of 75 (cycle duration = 0,8 s), ventricular systole
lasts approximately 0,3 s, and ventricular diastole approximately
0,5 s

1. Inflow phase. The inlet valve is open and the outlet valve is
closed.
RAPID VENTRICULAR FILLING (0,11 s)
DIASTASIS (0,19 s)
ATRIAL CONTRACTION (0,11 s)
2. Isovolumetric contraction (0,05 s). Both valves are closed,
with no blood flow.
3. Outflow phase (EJECTION). The outlet valve is open and
the inlet valve is closed.
RAPID EJECTION: 0,09 s; 70% of the stroke volume
ejected
SLOW EJECTION: 0,13 s; 30% of the SV ejected
4. Isovolumetric relaxation (0,08 s). Both valves are closed,
with no blood flow.

Events of the cardiac cycle


Slight Asynchrony Between Left and
Right Ventricle
IC IR
E

Ventricular VolumesSV – stroke volume = the amount of blood ejected by each
ventricle during one systole = EDV – ESV = 70 ml
EDV – end diastolic volume = the maximal ventricular volume =
the amount of blood present in the ventricle at the end of diastole
= 120 ml
ESV – end systolic volume = the minimal ventricular volume = the
amount of blood present in the ventricle at the end of systole =
50 ml

Ventricular VolumesCO - cardiac output = the flow of blood delivered by the heart in
one minute = heart rate x stroke volume
EF – ejection fraction = the stroke volume normalized to the end
diastolic volume:
EF = SV / EDV,
Should exceed 0.55 in a healthy person.

Pressure Values for the Right and Left Heart
Pressures
(mm Hg)
Pressures
(mm Hg)
Right Atrium Left Atrium
Mean 2 Mean 8
Right Ventricle Left Ventricle
Peak systolic
End diastolic
25
6
Peak systolic
End diastolic
130
10
Pulmonary Artery Aorta
Mean
Peak systolic
End diastolic
15
25
8
Mean
Peak systolic
End diastolic
95
130
80
Pulmonary
capillaries
Systemic capillaries
Mean 10 25

Pressure-Volume Loop

Cardiac Performance Is a generic term referring to how efficiently the ventricles are
carrying out their function as a pump
LEFT HEART
CARDIAC
OUTPUT
Performance = Actual CO/ Optimal CO
INPUT OUTPUT
End Diastolic
Volume
Ejection
Fraction
xStroke
Volume
Heart
Rate
•LV relaxation
•LV compliance
•LA function
•Mitral valve
•Pericardium
•Preload
•Afterload
•Contractility
DIASTOLIC
FUNCTION
SYSTOLIC
FUNCTION
=
PRESSURE
IN PULMONARY
VEINS
x

Systolic Function Expresses the ability of the ventricle to empty
It is determined by
Loading conditions
Preload – the load imposed on the ventricle just before
contraction has started, at the end of the diastole (EDV)
Afterload – the systolic load on the ventricle after it has
started to contract (Ao pressure, or more accurate, Ao
impedance)
Contractility – the intrinsic capacity of the myocard to shorten
independent of extrinsic factors (preload, afterload, heart rate)

Preload and the Frank-Starling Law of
the Heart
The intrinsic ability of the heart to adapt the force of ventricular
contraction (SV) to increasing volumes of inflowing blood
(preload, EDV) is called the Frank – Starling law of the heart.


Within physiologic limits, the heart pumps all the blood that
returns to it by the way of the veins.
The greater the heart muscle is stretched during ventricular
filling by an increased EDV, the greater is the force of
contraction and the greater the stroke volume pumped into the
aorta.
Right atrial dilation following an increased venous return
increases the heart rate as well by mechanical stimulation of the
SAN an increased venous return increases the cardiac output
by rising both SV and HR.

Starling Effect on Pressure-Volume
Loop

Force – Length Relationship An increased stretch of the cardiac muscle causes a stronger
contraction.
Why? In skeletal muscle, increased stretch provides a better
interaction between actin and myosin; the amount of tension
developed corresponds to the degree of overlap between the
actin and the myosin filaments
2 mm
2.2 mm
1.4 - 2 mm
> 2.2 mm

In cardiac muscle, as
the sarcomere length
decreases from 2.4 to 1.8
mm, active tension falls
steeply
Since the sarcomere has
the same length in both
types of muscle, the fall in
tension at lower
sarcomere length cannot
be due to the decrease in
the overlap of actin and
myosin

The greater force (f, red curve) developed at higher sarcomere
length (SL) (2.15 mm versus 1.65 mm) in cardiac muscle is
probably due to a length – induced calcium sensitisation; short
sarcomere length somehow reduces the calcium affinity for
TnC
Ca++ transients (c, green curve) are not significantly affected by
sarcomere length

Pressure – Volume Diagram
Shows the limits of ventricular
stretch and the effects of
stretching on systolic and
diastolic pressures
Systolic pressure curve proves
the Frank-Starling law of the
heart: at increasing loading
volumes the force of contraction
increases

Influence of Increased Contractility on
Performance Curves
A ventricular performance
curve
it is a length – tension diagram
that expresses the functional
ability of the ventricles to
pump blood
plots stroke work (P x V) as an
estimate of tension, against
left atrial pressure, as an
estimate of EDV; can be
obtained on a patient
Positive inotropic agents shift the performance curve upward
and to the left Starling’s law is not a fixed relationship

Afterload and the Anrep Effect A healthy heart can overcome any physiological acute increase
in afterload; after an initial decrease, the SV comes back to
normal whithin a couple of heart beats

How?
The Anrep effect (homeometric autoregulation):
– when Ao pressure increases abruptly, a positive inotropic effect
follows within 1-2 minutes
- mechanism: increased wall tension stimulates stretch receptors
a rise of [Ca++]i
The ”garden-hose” effect:
- increased Ao pressure rises the coronary perfusion; an
increase in the coronary artery pressure is distending the heart
from within its walls (stretch), inducing a better shortening of the
myocardial fibers

Preload is related to the degree to which the myocardial fibers
are stretched at the end of the diastole
Afterload is related to the wall stress generated by the
myocardial fibers during systole

Heart Rate and the Force of Ventricular
Contraction
An increase in heart rate progressively enhances the force of
ventricular contraction (Bowditch staircase or treppe
phenomenon)
Why? – During rapid stimulation more Ca++ enter the cell than
can be handled by the mechanisms for Ca++ exit
Time
Tension

Contractility Contractility is the inherent capacity of the myocardium to
shorten independent of changes in load or heart rate
Increased contractility
Means a greater rate of contraction to reach a higher peak of
force
It is explained at a molecular level by increased interaction
between Ca++ and the contractile proteins
Contractility or inotropism (ino, fiber; tropos, to move) is an
important regulator of the myocardial oxygen uptake

Clinical Assessment of Contractility
Ejection fraction, EDV – ESV / EDV, but depends also on
preload and afterload
The rate of pressure development during ejection, DP/Dt, and
the velocity of ejection; are influenced by preload; they
correlate well with inotropic interventions
Pressure-volume loop

LV pressure
The Rate of Pressure Development
During Ejection
Isoprenaline Effort

Pressure – Volume Loops Are among the best of the current methods for estimating the
contractility of the intact heart
The maximal pressure that can be developed by the ventricle at
the ESV is defined by the end-systolic pressure-volume
relationship (ESPVR), which represents the inotropic state of
the ventricle.

Slope of end-systolic pressure-volume relationship (ESPVR
or Es) – almost insensitive to preload, afterload, and heart rate
most reliable index for assessing myocardial contractility

Inotropic agentsModifiers of contractility can affect the dynamics of cardiac muscle
contraction, independent of preload or afterload
Positive inotropic agents increase [Ca++]i by
- opening Ca++ channels
- inhibiting Na-Ca exchanger
- inhibiting the Ca++ pump, all at the plasma membrane
Examples: Adrenergic agonists
Cardiac glycosides (digitalis derivatives)
High extracellular [Ca++]
Low extracellular [Na+]
Increased heart rate

Influence of Increased Contractility on
Performance Curves
A ventricular performance
curve
it is a length – tension diagram
that expresses the functional
ability of the ventricles to
pump blood
plots stroke work (P x V) as an
estimate of tension, against
left atrial pressure, as an
estimate of EDV; can be
obtained on a patient
Positive inotropic agents shift the performance curve upward
and to the left Starling’s law is not a fixed relationship

Negative inotropic agents decrease [Ca++]i
Examples:
Ca++-channel blockers (verapamil, diltiazem)
Low extracellular [Ca++]
High extracellular [Na+]

Diastolic Function
Expresses the filling capacity of the ventricle
It is influenced by several factors:
o Ventricular relaxation (lusitropia)
o Ventricular compliance
o Atrial function
o AV valve
o Pericardium
o Heart rate

Pressure – Volume Diagram Shows the limits of ventricular
stretch and the effects of
ventricular volumes on systolic
and diastolic pressures
Diastolic pressure curve is an
expression of ventricular
compliance:
C = DV / DP

Assessment of Diastolic Function Izovolumic relaxation
Parameters: duration of izovolumic relaxation (from Ao closure
until Mi opening), time constant of isovolumic pressure decay (t,
ms)
Methods: echocardiography, Doppler echography,
mechanograms

Assessment of Diastolic Function Ventricular filling
Parameter: pressure-volume relationship during ventricular
filling; the slope of the pressure – volume curve dP/dV plotted
from the minimal diastolic pressure to the end-diastolic pressure
represents ventricular stiffness
Methods: Doppler echocardiography

Work of the Heart The stroke work output of the heart is the amount of energy
that the heart converts to work during each heartbeat while
pumping blood into the arteries
The general expression of external work done when a mass is
lifted a certain distance is W = force x distance
For pressure moving a volume, the external work is:
W = P · DV

The pressure-volume area
is used for calculating the net external work
is an index of myocardial O2 uptake

The pressure-volume area requires invasive monitoring for
accurate determination
In clinics the pressure work can be approximated by the
product of stroke volume and peak systolic blood pressure
(SBP):
SBP x SV
Minute work output is the total amount of energy
converted to work in 1 minute:
Minute work = SBP x SV x HR

The total external work is the sum of the pressure-volume work
(= area of the PV loop) and the kinetic energy
W = P · DV + ½ mv2
Kinetic energy
½ mv2, where m is the mass of blood ejected and v is the
velocity of ejection - represents the energy spent for the
acceleration imparted by the heart to the blood during the
cardiac cycle;
accounts for less than 1% of the total external work in healthy
hearts, but increases steeply in aortic stenosis.

Tension Heat Is the potential energy generated by each contraction that is not
converted to external work but maintains active tension
= the energy cost for isometric contraction
the muscle breaks down ATP and the energy ends up as heat
The pressure against which the ventricle must pump (pressure in
the Ao or the PA) is a major determinant of tension heat
Formula: k · T · Dt , where T is the tension of the ventricular wall,
Dt is the time interval that the ventricle maintains this tension,
and k is a proportionality constant

Total Energy Required for Cardiac
Contraction
The total energy transformed in one cardiac cycle is the sum of
the total external work done on the blood and the tension
heat:
E = P · DV + ½ mv2 + k · T · Dt
E is derived mainly from oxidative metabolism of fatty acids,
lactate or glucose the rate of oxygen consumption by the
heart is a measure of E

Mechanical Efficiency of the Heart Or efficiency of work, is the ratio between the external work
performed and the total energy expenditure during systole, W/E
Can be defined also as the relation between the work
performed and the myocardial oxygen uptake
Maximum efficiency of the normal heart is between 20 and 25
per cent; in heart failure, this can decrease to as low as 5 to10
per cent
! Has nothing to do with how effective the ventricle is expelling the
blood, which is expressed by the ejection fraction (EF =
SV/EDV).