Embed Size (px)
Citation preview

d e n t a l m a t e r i a l s 3 0 ( 2 0 1 4 ) 424–432
Available online at www.sciencedirect.com
ScienceDirect
jo ur nal ho me pag e: www.int l .e lsev ierhea l th .com/ journa ls /dema
Mechanical fatigue degradation of ceramics versusresin composites for dental restorations�
Renan Belli ∗, Eva Geinzer, Anna Muschweck, Anselm Petschelt,Ulrich LohbauerLaboratory for Biomaterials Research, Dental Clinic 1 – Operative Dentistry and Periodontology,Friedrich-Alexander University of Erlangen-Nürnberg, Glueckstrasse 11, 91054 Erlangen, Germany
a r t i c l e i n f o
Article history:
Received 25 July 2013
Received in revised form
20 September 2013
Accepted 14 January 2014
Keywords:
Resin composite
Ceramics
Flexural strength
Fatigue
Staircase approach
a b s t r a c t
Objectives. For posterior partial restorations an overlap of indication exists where either
ceramic or resin-based composite materials can be successfully applied. The aim of this
study was to compare the fatigue resistance of modern dental ceramic materials versus
dental resin composites in order to address such conflicts.
Methods. Bar specimens of five ceramic materials and resin composites were produced
according to ISO 4049 and stored for 14 days in distilled water at 37 ◦C. The following
ceramic materials were selected for testing: a high-strength zirconium dioxide (e.max Zir-
CAD, Ivoclar), a machinable lithium disilicate (e.max CAD, Ivoclar), a pressable lithium
disilicate ceramic (e-max Press, Ivoclar), a fluorapatite-based glass-ceramic (e.max Ceram,
Ivoclar), and a machinable color-graded feldspathic porcelain (Trilux Forte, Vita). The com-
posite materials selected were: an indirect machinable composite (Lava Ultimate, 3M ESPE)
and four direct composites with varying filler nature (Clearfil Majesty Posterior, Kuraray;
GrandioSO, Voco; Tetric EvoCeram, Ivoclar-Vivadent; and CeramX Duo, Dentsply). Fifteen
specimens were tested in water for initial strength (�in) in 4-point bending. Using the same
test set-up, the residual flexural fatigue strength (�ff) was determined using the staircase
approach after 104 cycles at 0.5 Hz (n = 25). Weibull parameters �0 and m were calculated for
the �in specimens, whereas the �ff and strength loss in percentage were obtained from the
fatigue experiment.
Results. The zirconium oxide ceramic showed the highest �in and �ff (768 and 440 MPa,
respectively). Although both lithium disilicate ceramics were similar in the static test, the
pressable version showed a significantly higher fatigue resistance after cyclic loading. Both
the fluorapatite-based and the feldspathic porcelain showed equivalent initial and cyclic
fatigue properties. From the composites, the highest filled direct material Clearfil Majesty
Posterior showed superior fatigue performance. From all materials, e.max Press and Clearfil
Majesty Posterior showed the lowest strength loss (29.6% and 32%, respectively), whereas
the other materials lost between 41% and 62% of their flexural strength after cyclic loading.
Conclusions. Dental ceramics and resin composite materials show equivalent fatigue strength
degradation at loads around 0.5�in values. Apart from the zirconium oxide and the lithium
� This study was presented at the 5th International Conference on Mechanics of Biomaterials and Tissues (ICMoBT 2013).∗ Corresponding author. Tel.: +49 9131 854 3741; fax: +49 9131 853 4207.
E-mail address: [email protected] (R. Belli).0109-5641/$ – see front matter © 2014 Academy of Dental Materials. Published by Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.dental.2014.01.003

d e n t a l m a t e r i a l s 3 0 ( 2 0 1 4 ) 424–432 425
disilicate ceramics, resin composites generally showed better �ff after 10,000 cycles than
the fluorapatite glass-ceramic and the feldspathic porcelain. Resin composite restorations
may be used as an equivalent alternative to glass-rich-ceramic inlays regarding mechanical
performance.
emy
1
Tdoadso
tmaTiapdtmterc
ttwtmoimottoftwim
otitataT(
© 2014 Acad
. Introduction
he guidelines for the restoration of small to medium-sizeefects in the posterior region of teeth present an overlapf indications, where both direct or indirect techniques arepplicable. Apart from empirical criteria, little relevant evi-ence is available to the dentist, which could be used as aolid principle for the choice of one treatment option over thether.
The terms “direct” and “indirect” restorations relate mostlyo the in situ placement of resin composites and to the
achined- or laboratory-made ceramics, respectively. Bothlternatives show technical advantages and disadvantages.issue removal during preparation for direct resin compos-
te follows minimally invasive conducts, pleasing patientsnd dentists. Resin composites however contract, and in situolymerization may inflict temporary flexural stresses onamaged cavity walls [1] and prompt premature cracking ofhin enamel borders. Resin composite restorations are also
ore technique sensitive, color unstable and less wear resis-ant than their ceramic restoration counterparts. In turn,conomical aspects are sure to make direct restorations withesin composites an attractive option to costly indirect pro-esses and materials.
This balance of pros and cons contain most of the factorshat are usually taken into account by dentists to deal withhis conflict. However, these are hardly the factors that haveeight in determining the success rate of a type of restora-
ion. Instead, clinical studies show that failure of small toedium-size posterior restorations mostly happens in one
f two ways [2]. The first one is biological and is character-zed by the infiltration of bacteria through the restorations
argins causing tissue degradation (secondary caries). Thether is mechanical and results in partial or complete frac-ure of the restoration. These two factors are not related tohe technique itself, but rather to the materials in use. Sec-ndary caries, for example, may depend on the caries riskactor of the patient [3], but it is ultimately determined byhe bonding effectiveness of the bonding/luting agent. Like-ise, the fracture process depends on the subjected load, but
t is primarily governed by the mechanical properties of theaterial.That supports the study of the mechanical performance
f resin composites and dental ceramics for creating criteriahat are more clinically relevant for determining treatmentndications. Mostly, mechanical properties such as elas-ic modulus, flexural strength and fracture toughness aressessed under static loading conditions for the initial charac-
erization of materials. In this regard, substantial differencesre observed between resin composites and dental ceramics.he latter are stiffer, showing elastic moduli between 65 GPafeldspathic and glass-ceramics) and 250 GPa (alumina- and
of Dental Materials. Published by Elsevier Ltd. All rights reserved.
zirconia-based ceramics) [4], whereas the interval 8–15 GPa iscommon for most resin composites [5]. Ceramics may be asstrong as 900 MPa in bending for pure crystalline materials [6],whereas glass-rich ceramics, such as feldspathic- and leucite-based, show flexural strengths similar to resin composites(70–130 MPa) [5,7]. The values of fracture toughness in resincomposites (1–2 MPa
√m) [8], however, surpass those of glass-
rich ceramics (0.7–1.5 MPa√
m) [4,6] used for inlays, onlaysand veneering of infrastructures. For lithium disilicate-basedglass-ceramics an increase in fracture toughness (∼3 MPa
√m)
is observed despite the relatively high amount of glass (30%)due to toughening mechanisms induced by the microstruc-ture [9–11]. A complete elimination of the glass phase leadsto high values of toughness in zirconia and alumina ceramics(5–7 MPa
√m) [4,6].
The above-mentioned parameters are particularly relevantduring overloading events that lead to fast fracture. This sce-nario is however not that representative of clinical failures[2,12,13]. For applications where the loading conditions arerather repetitive and subcritical, such as those experiencedin the mouth, studies that characterize the fatigue behav-ior and strength degradation of restorative materials mightoffer a higher predictive potential [14]. In resin composites, forinstance, properties derived from fast fracture conditions haveshown little association to their fatigue resistance under cyclicloading in vitro [15]. For ceramic restorations, in vitro fatigueexperiments have shown to be good predictors of their in vivosurvivability [16].
Under cyclic loading, the degradation of strength can bedirectly assessed by measuring the crack advance in rela-tion to the range of stress intensity factor (K) applied. Usingthe Paris law relationship during Regimen II, subcritical crackgrowth susceptibility parameters (n) can be derived. Thetracking of crack growth in materials presenting low frac-ture toughness and low R-curve behavior can be problematic,with obtained n values showing a high variation amongstudies. For glass-rich ceramics the literature reports val-ues between 3.7 and 54.6 [17,18], and between 5.2 and 70.5[19–21] for resin composites. A more practical method forceramic materials derives slow crack growth susceptibilityparameters (ndyn, for dynamic loading) indirectly using a rangeof stressing rates. Unfortunately, due to the substantial vis-coelastic response of resin composites at low strain rates, thelatter method is suboptimal for comparing the fatigue resis-tance of resin-based materials against highly brittle dentalceramics.
Aiming a practical comparison of the fatigue resistanceof resin composite and dental ceramic materials, the presentstudy used a phenomenological approach that calculates the
residual flexural fatigue strength for a defined loading chal-lenge. By selecting different compositions among currentlymarketed resin composites and dental ceramics, discussions
l s 3 0 ( 2 0 1 4 ) 424–432
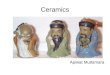
Fig. 1 – (a) Diagram of the test set-up for flexural strength instatic and cyclic loading conditions used in this study; and(b) a random sequence of 4 specimens under cyclic loadingaccording to the staircase approach, where the firstspecimen survives and the subsequent two fail. In (b) “d”
426 d e n t a l m a t e r i a
on the clinical applications of these materials were conductedbased on their mechanical performance.
2. Materials and methods
2.1. Materials
Five currently commercially available resin composite mate-rials for direct (four materials) and indirect (one material)restorations were selected for testing. In Table 1 details abouttheir filler configuration and matrix composition can be found.This selection of composites included mainly Bis-GMA-basedcomposites with a filler content between 55 and 82 vol%, oneof them containing prepolymerized fillers (Tetric EvoCeram,Ivoclar-Vivadent, Liechtenstein) and one machinable indirectcomposite (Lava Ultimate, 3M ESPE, USA).
Five ceramic systems were selected to encompass differ-ent compositions (crystalline structure and glass content) andclinical indications for inlays or onlays (Table 2). Reinforcedsystems that can be used as infrastructures or monolithi-cally included a zirconium dioxide ceramic (IPS e.max ZirCAD,Ivoclar-Vivadent) and a lithium disilicate glass-ceramic in twoforms: a machinable block (IPS e.max CAD, Ivoclar-Vivadent) ora pressable variant (IPS e.max Press, Ivoclar-Vivadent). Glass-rich ceramic systems with restricted indications for use in themonolithic form or as veneers included a fluorapatite glass-ceramic powder for use with the layering technique (IPS e.maxCeram, Ivoclar-Vivadent) and a machinable color-graded felds-pathic porcelain block (Vitablocs Trilux Forte, Vita, Germany).
2.2. Specimen preparation
2.2.1. Resin composite specimensForty bending bars (2 mm × 2 mm × 25 mm) were produced foreach material using a tungsten carbide/glass mold under cali-brated conditions of 23 ◦C and 50% humidity. The specimenfabrication followed the manufacturers’ recommendationsand ISO 4049 standard. The materials were inserted in themold in one previously weighted increment, and light-curedwith five overlapping spots of ∅ = 8 mm on both top and bot-tom with a commercial light-curing unit (Elipar® Trilight, 3MESPE, Germany) with an output intensity of 800 mW/cm2 for20 s at each spot. After removal from the mold, the bottomof the specimens was polished with silicon carbide paperdown to 4000 grit to remove surface flaws that could influencestrength values [10]. For the indirect material Lava Ultimate,bending bars of same dimensions were supplied by the man-ufacturer and further polished following the procedures usedfor the other tested materials. The specimens were stored indistilled water at 37 ◦C for 14 days before mechanical testing.
2.2.2. Ceramic specimensFrom the materials that were supplied in machinable blocks(IPS e.max ZirCAD, IPS e.max CAD and Vitablocs Trilux Forte),bar specimens were cut using a low-speed saw and a diamond-
coated copper disk (Buheler, USA) under water lubrication.Bars of IPS e.max CAD were further crystallized over a crys-tallization tray (Ivoclar-Vivadent) in a furnace (Vita Vacumat4000, Vita) at a maximum temperature of 850 ◦C according torepresents the stress increment.
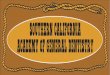
the program provided by the manufacturer. Zirconium dioxidebars of IPS e.max ZirCAD were sintered in a high-temperaturefurnace (Linn EVA-1700, Germany; 200 ◦C/h heating rate) for2 h at the maximum temperature of 1530 ◦C and cooledovernight. The fabrication of IPS e.max Press bar specimensfollowed the “lost-wax” technique, where PMMA bars wereinvested (PressVest, Ivoclar-Vivadent) and molten to create aspace where the pressable material was subsequently injected(EP 500 furnace, Ivoclar-Vivadent). The bars were divestedand sandblasted with 50 �m glass particles at 2 bar pressure(Fig. 2a).
After bar fabrication steps, specimens from all the ceramicmaterials were polished in water with SiC paper 1200 grit onall sides and further down to 4000 grits at the side subjectedto tension. Final dimensions of ceramic specimens were thesame as for the resin composite specimens.
The specimens from IPS e.max Ceram were produced usingthe layering technique, in which a powder-distilled slurrywas poured into a detachable custom-made Plexiglax mold,pressed and dried with absorbent paper. The ceramic pow-der plate was removed from the mold and sintered over arefractory tray in a furnace (Vita Vacumat 4000, Vita) at a max-imum temperature of 750 ◦C following the sintering programprovided by the manufacturer. The resulting sintered ceramicplate presented final dimensions of 27 mm × 21 mm × 3 mm.The plates were subsequently ground with a diamond wheelin a grinding machine (MPS 2 120, G&N, Germany) to obtain2.1 ± 0.1 mm-thick plates with perfect parallel sides. Furtherpolishing steps were undertaken with SiC papers down to1200 on all sides and up to 4000 grits on the side subjected
to tension. The polished plates were then sectioned in multi-ple 2 mm-thick bars using a Micro Water-Jet cutting machine(Womajet F3, Daetwyler, Switzerland) operating at 6000 bar
d e n t a l m a t e r i a l s 3 0 ( 2 0 1 4 ) 424–432 427
Table 1 – Name of the composites tested in this study, their manufacturer, filler content by volume, filler configuration,matrix composition and lot number.
Composite Manufacturer Filler content(vol%)
Filler configuration Matrix composition Lot
Lava Ultimate 3M ESPE, USA 80 20 nm silica particles; 4–11 nmzirconia particles; 0.6–10 �mnanoparticle clusters
Bis-GMA, Bis-EMA, UDMA,TEGDMA
602
Clearfil MajestyPosterior
Kuraray, Japan 82 0.5–10 �m particles; 20 nmparticles
Bis-GMA, TEGDMA, hydrophobicaromatic dimethacrylates
00111B
Grandio SO Voco, Germany 73 0.5–3 �m particles; 20–40 nmnanoparticles
Bis-GMA, Bis-EMA, TEGDMA 1207326
Tetric EvoCeram Ivoclar-Vivadent,Liechtenstein
55 0.5 �m mean particle size; 5–50 �mprepolymerized fillers containing
fillers
Dimethacrylates P67534
glass
paaf
d
2s
FiaG
�
wbsmta
0.4–0.7 �m
CeramX Duo Dentsply, Germany 57 1.1–1.5 �m
particles
ressure and 1000 m/s water jet speed (Fig. 2b). The use of high-pressure abrasive–water mixture cutting procedurellowed for the structural preservation of the material withouturther alterations due to heating.
The specimens from all ceramic materials were stored inistilled water for 14 days at 37 ◦C before mechanical testing.
.3. Initial flexural strength (�in) and flexural fatiguetrength (�ff) testing
or the initial flexural strength (�in) measurements, 15 spec-mens per material were loaded in 4-point bending (Fig. 1a)t 0.75 mm/min in a universal testing machine (Z2.5, Zwick,ermany) using the relation:
in = 3Pd
wb2(1)
here P is the maximum load at failure, d is the distanceetween the midpoint of the lower supports and the upper
upports (5 mm), w the width and b the height of the speci-en. The initial strength data was further analyzed accordingo a two-parameter Weibull distribution in terms of shape (m)nd scale parameters �0 and �−2.97. The m modulus describes
Table 2 – Name of the dental ceramics tested in this study, theirange of clinical indications and lot number.
Ceramic Manufacturer Crystal structure G
IPS e.max ZirCAD Ivoclar-Vivadent,Liechtenstein
Yittrium-stabilizedzirconium dioxidecrystals
IPS e.max CAD Ivoclar-Vivadent,Liechtenstein
0.2–2 �m lithiumdisilicate crystals
IPS e.max Press Ivoclar-Vivadent,Liechtenstein
3–6 �m lithiumdisilicate crystals
IPS e.max Ceram Ivoclar-Vivadent,Liechtenstein
0.1–5 �m fluorapatitecrystals
Vitablocs TriluxForte
Vita Zahnfabrik,Germany
4 �m feldspat crystals
particles; 10 nm Bis-GMA, UDMA, TEGDMA 1211000259
the scatter in stress to failure, and parameters �0 and �−2.97
indicate their magnitude and are given for a failure probabil-ity of 63.2% and 5%, respectively. The Weibull modulus m, thecharacteristic strength �0 and their respective 95% confidenceintervals were corrected by a factor corresponding to the num-ber of specimens (n = 15), according to the European standardEN 843-5 [22].
The flexural fatigue strength (�ff) of the composite andceramic materials was determined for 104 cycles under equiv-alent test conditions at a frequency of 0.5 Hz (n = 25). The“staircase” approach method was used for the fatigue resis-tance evaluation. For each cycle, the stress alternated between1 MPa and maximum applied stress (�app). Tests were con-duced sequentially, with �app in each subsequent specimenbeing increased or decreased by a fixed increment of stress,according to whether the previous 104 cycle runs resultedin failure or survival. The first specimen was tested at�app = 0.5�in. All tests were carried out in distilled water at37 ◦C. The �ff and standard deviation (SD) were determinedusing Eqs. (2) and (3), respectively;
�ff = X0 + d
(∑ini∑ni
± 0.5
)(2)
r manufacturer, crystal structure, glass phase amount,
lass phase(wt%)
Range of indications Lot
0 Single-unit to long-spaninfrastructures or monolithicstructures
L47695
60 Inlays, onlays, veneers, anteriorand premolar crowns, veneering ofinfrastructures
P19972
30 Inlays, onlays, anterior andposterior crowns, 3-elementbridges in the anterior andpre-molar regions, veneering ofinfrastructures
J18904
up to 90 Inlays, laminate veneers,veneering of infrastructures
M04720
80 Inlays, laminate veneers, anteriorcrowns and veneering ofinfrastructures
12500

428 d e n t a l m a t e r i a l s 3
Fig. 2 – (a) Specimens of IPS e.max Press fabricatedaccording to the lost-wax technique, before polishing; and(b) cutting procedure of IPS e.max Ceramic plates using a
residual strength (81.4 MPa) among the composites. Grandio
high-pressure water-jet cutting device.
SD = 1.62d
(∑ni
∑i2ni − (
∑ini)
2
(∑
ni)2
+ 0.029
)(3)
where X0 is the lowest stress level considered in the analy-sis and d is the fixed stress increment. To determine �ff, theanalysis of the data is based on the least frequent event (fail-ures versus survivals). In Eq. (2), the negative sign is used whenthe analysis is based on failures; otherwise the positive signis used. The lowest stress level considered is designated i = 0,the next i = 1, and so on, and ni is the number of failures orsurvivals at the given stress level. A cross-section of the cyclicloading profile for the fatigue experiment used in the staircaseapproach for a given hypothetical sequence of 4 specimens isillustrated in Fig. 1b.
2.4. Statistical analysis
The �in was analyzed using a two-parameter Weibull distribu-tion, in which the 95% confidence intervals for the groups werecomputed and differences were considered significant when
the 95% confidence intervals did not overlap. �in and �ff valueswere analyzed using a one-way ANOVA test and modified posthoc LSD test (p < 0.05).0 ( 2 0 1 4 ) 424–432
3. Results
Table 3 depicts the Weibull distribution parameters for thespecimens tested in 4-point bending. In Table 4 the valuesand standard deviations for �in, �ff and strength degradation(�in − �ff; in MPa and in %) are summarized. Strength degra-dation in percentage was calculated in relation to the �ff after104 cycles and the average value of �in calculated using Eq. (1).
3.1. Strength
The highest characteristic strength was found for the zirco-nium dioxide ceramic, which showed values of 816.97 MPaand 559.35 MPa for a failure probability of 63.2% and 5%,respectively. Following the zirconium dioxide ceramic withsignificantly lower strength values, the two lithium disilicateceramics presented statistically comparable �0, and the lowestm values among all the ceramic materials. The two glass-rich ceramics (IPS e.max Ceram and Vitablocs Trilux Forte)showed equivalent �0, under 70 MPa, statistically lower thanall other ceramic and resin composite materials. Values of �0
for the resin composites ranged from 92 to 145 MPa, with thehighly filled materials (Clearfil Majesty Posterior and GrandioSO) performing slightly better than the machinable indirectcomposite (Lava Ultimate). Regular-filled composites TetricEvoCeram and CeramX Duo showed the lowest strength val-ues from all composites. The highest m values were found forTetric EvoCeram, Lava Ultimate and Vitablocs Trilux Forte.
3.2. Initial strength (�in) vs. residual flexural fatiguestrength (�ff)
All materials showed a significant degradation in strengthafter cyclic loading, revealing different levels of susceptibilityto fatigue. The �ff value represents the residual strength underwhich no failures are to be expected, considering the fatiguedegradation that occurs within 10,000 loading cycles. The �ff
values gains importance in the context of relevant mastica-tion loads to which the materials are subjected. The relativestrength degradation (in %), rather than the global strengthdegradation (in MPa), consists of a more representative valueof the fatigue susceptibility and allows comparisons amongmaterials.
From the values of �ff in Table 4, distinct ranges of residualstrengths can be distinguished. The highest residual strength(440.0 MPa) after cyclic loading was obtained for IPS e.maxZirCAD, which was significantly higher than all other mate-rials. In contrast to the comparable �in values obtained forIPS e.max CAD and IPS e.max Press, a significant differencein �ff values was recorded, with a superior performance ofthe pressable version (202.7 MPa) over the machinable blockversion (120.8 MPa) of the lithium disilicate ceramic. Follow-ing a decreasing �ff value ranking, the direct resin compositeClearfil Majesty Posterior has shown the statistically highest
SO and the indirect composite Lava Ultimate showed compa-rable �ff, with 60.5 MPa and 63.6 MPa, respectively. A lowestrange of �ff was observed for Tetric EvoCeram (42.3 MPa),

d e n t a l m a t e r i a l s 3 0 ( 2 0 1 4 ) 424–432 429
Table 3 – Weibull scale (�0 and �−2.97) and shape (m) parameters for initial strength and 95% confidence intervals (Cl/Cu)and (Dl/Du) for �0 and m, respectively.
Material Weibull �−2.97 (MPa) Weibull �0 (MPa) Cl/Cu �0 Weibull m Dl/Du m
IPS e.max ZirCAD 559.35 816.97a 751.6–887.7 7.11cd 4.5–10.9IPS e.max CAD 172.21 279.68b 251.3–311.1 5.55de 3.5–8.5IPS e.max Press 149.11 325.13b 299.1–353.2 3.45e 2.2–5.3IPS e.max Ceram 49.9 69.98e 64.9–75.3 7.97bcde 5.1–12.2Vitablocs Trilux Forte 60.16 67.82e 66.1–69.6 22.5a 14.3–34.6Lava Ultimate 108.48 126.46c 122.2–130.7 17.57ab 11.1–27.0Clearfil Majesty Posterior* 76.64 129.67c 115.4–145.5 5.12e 3.2–7.8Grandio SO* 113.71 145.11c 137.5–153.0 11.05abcd 7.0–17.0Tetric EvoCeram* 82.61 92.50d 90.2–94.8 23.58a 15.0–36.2CeramX Duo 68.84 96.97d 89.9–104.5 7.86bcd 5.1–12.1
Ce
tdsrma
4
4
Toosotdcrfte
Same letters in columns indicate same statistical subsets at ̨ = 0.05.∗ Results taken from Ref. [15].
eramX Duo (34.4 MPa) and the two glass-rich ceramics IPS.max Ceram (36.0 MPa) and Vitablocs Trilux Forte (38.5 MPa).
The highest relative strength degradation was recorded forhe resin composite CeramX Duo (62.3%), whereas the lithiumisilicate ceramic IPS e.max Press showed the lowest fatigueusceptibility (29.6% of strength degradation), along with theesin composite Clearfil Majesty Posterior (32.0%). All other
aterials have shown strength degradations between 41.8%nd 56.5%.
. Discussion
.1. Ceramics
he values of �ff are illustrative of the residual values of �in
btained statically, and reveal significant strength degradationf all tested ceramic materials after 104 loading cycles. Theeverity of strength degradation, following the usual behaviorf ceramic materials, showed a high dependency on composi-ion and microstructure, indicating the operation of distinctegradation mechanisms. Common to all glass-containingeramics, stress corrosion acts as the dominant mechanism
educing their fracture resistance and clinical lifetime. Lowerailure stresses at decreasing stressing rates characterize theime-dependency of these mechanisms in dynamic fatiguexperiments [23,24], rendering parameters that describe theTable 4 – Mean and standard deviations (in parentheses) of initafter 104 cycles, relative strength degradation (�in − �ff), and glo
Material �in (MPa) �ff (MPa)
IPS e.max ZirCAD 768.13 (109.4)a 440.01 (51.5)IPS e.max CAD 259.53 (47.13)b 120.87 (15.21IPS e.max Press 288.38 (68.95)b 202.78 (47.09IPS e.max Ceram 66.25 (9.01)f 36.07 (1.69)Vitablocs Trilux Forte 66.39 (3.19)f 38.58 (2.39)Lava Ultimate 123.08 (7.46)d 63.66 (5.63)Clearfil Majesty Posterior* 119.78 (24.20)d 81.40 (8.01)Grandio SO* 139.23 (13.63)c 60.50 (3.17)Tetric EvoCeram* 90.63 (4.19)e 42.30 (2.45)CeramX Duo 91.74 (12.37)e 34.59 (8.50)
Same letters in columns indicate same statistical subsets at ̨ = 0.05.∗ Results taken from Ref. [15].
susceptibility to subcritical crack growth (ndyn). For dentalceramics, several studies report ndyn values dependent on theamount of glass phase. For low glass-content alumina–glassand alumina–zirconia–glass composites, where the glassymatrix still consists of the main crack path [25], ndyn values aregenerally orders of magnitude higher than in glass-rich felds-pathic porcelains and silicate-based glass-ceramics [7,26,27].The degradation of �in observed for e.max CAD, e.max Press,e-max Ceram and Vitablocs Trilux Forte are expected to havebeen governed by typical stress corrosion mechanisms, withstrength degradation severity being linked to their glass phaseamount.
In the lithium disilicate e.max Press ceramic, cracks alsopropagate preferentially through the glass phase, but contraryto glass-ceramics containing leucite and fluorapatite crystalphases, lithium disilicate crystals are efficient in promotingcrack deflection and crack branching [9–11,28]. These extrinsictoughening mechanisms are mainly dictated by interactionsof the crack front with the crystal microstructure, thus res-tricting the strength degradation due to glass-driven corrosionmechanisms and accounting for the low global strength degra-dation values observed herein (29.6%). Differences betweene.max Press and e.max CAD are probably related to the higheramount of glass, reduced crystal phase and small crystal size
of the latter.Dynamic fatigue experiments have also shown a highercrack velocity and lower ndyn (12.9) for a fluorapatite-based
ial strength (�in), residual flexural fatigue strength (�ff)bal strength degradation (in %).
�in − �ff (MPa) Strength degradation (%)a 328.12 42.7)c 138.66 53.4)b 85.60 29.6
g 30.18 45.5fg 27.81 41.8e 59.42 48.2d 38.38 32.0e 78.73 56.5fg 48.33 53.3g 57.15 62.3

l s 3
430 d e n t a l m a t e r i aveneer (Eris, Ivoclar-Vivadent, similar to e.max Ceram) incomparison to a lithium disilicate ceramic (Empress 2,Ivoclar-Vivadent, now e.max Press; ndyn = 28.07) [11]. Undercyclic bending fatigue experiments performed by Studartet al. [29], Empress 2 has also shown a superior resistanceto subcritical crack growth than a zirconium oxide ceramic(ncyc = 33.1 vs. 24.9, respectively), supporting the results foundin the present study. Their threshold values for KI (Kth), belowwhich no stable crack propagation occurs, was reported to1.8 MPa
√m for the lithium disilicate ceramic, 32% lower than
its critical value for K (Kc). For our e.max Press fatigue spec-imens, we calculated critical crack size values of 4.66 �musing Studart’s value for Kth and our values of �ff (202.7 MPa)through Griffith’s relation KI = �appYa1/2, (where Y = 1.3 for sur-face cracks). Below that crack size, no crack growth shouldoccur before 104 cycles. Since the �app levels in our fatiguetest for e.max Press reached values higher than 0.68�in (upto 0.87�in), subcritical cyclic crack growth occurred for cracks>3.06 �m, leading to fracture of some specimens. Such dimen-sions of crack size are comparable to the length of thecrystalline phase in e.max Press, and large in comparison tothe mean surface roughness obtained after polishing with4000 grits SiC paper (0.15 �m [10]). The low m value and thehigh standard deviation of �ff measured for e.max Press mightreflect an inhomogeneous distribution of large processingflaws.
For a zirconium oxide ceramic in water, cyclic stable crackgrowth was reported in another study from Studart et al.[30] to begin already at 54% of the critical stress at failureat Kth = 2.5 MPa
√m. This may reflect the low gain in strength
from 0.5 �in to �ff in the present study for e.max ZirCAD, andthe plateau in �app level that was reached after just a few spec-imens. Here, important to determine the survival for a definednumber of cycles are the size of initial flaws and how fast theygrow. These cracks are accelerated by corrosion of Zr O bondsin the presence of moisture [31], which also seems to act byprompting spontaneous transformation of crystals that loosethe potential for toughening [32]. In cyclic fatigue, friction ofthe fractured surfaces consists of an additional degradationmechanism leading to higher crack growth susceptibility thanunder static fatigue loading conditions (ncyc < nsta) [33]. For sta-bilized zirconium dioxide, the susceptibility to cyclic fatigueeffects seems to be directly associated to the potential fortransformation toughening [34].
4.2. Resin composites
Strength degradation in resin composites also varied amongmaterials, which allows us to hypothesize on the causes ofdegradation based on the differences between compositionsand microstructures. Lower strength degradations were asso-ciated with composites having higher filler contents, reflectingthe susceptibility of the resin phase to strain challenges [14]and environmental degradation [35]. An improvement in resinquality and mechanical fatigue resistance can be achievedthrough post-cure treatments [36,37], employed in indirect
composites like Lava Ultimate. Although a better polymerizedresin matrix also improves the resistance for crack propaga-tion within a fatigued material [38], limited improvements tothe R-curve behavior is provided by additional heat curing,0 ( 2 0 1 4 ) 424–432
according to Shah et al. [39]. In fact, superior K developmentsduring crack growth are expected for composites with largerparticles in contrast to nanofilled composites [40]. To that maybe accredited the superior performance of Clearfil MajestyPosterior over Lava Ultimate, which also indicates an impor-tant role of the microstructure in the mechanical stabilityagainst cyclic fatigue. This is supported by Takeshige et al.[21] and Ornaghi et al. [41], who found superior ncyc and ndyn
for composites with large fillers and larger filler size distribu-tions, respectively. Tetric EvoCeram, although regular-filled,presented superior fatigue resistance than Grandio SO dueto its large pre-polymerized filler phase, which resist fractureunder low energy crack growth during cyclic loading [15].
4.3. Ceramics vs. resin composites
At first glance, Table 4 shows a comparable fatigue resistancefor resin composites and dental ceramics. This comparisonincludes direct and indirect resin composites, as well as glass-rich and fully crystalline materials. A judicious perspective ofthese values, however, must consider the stress dependencyof the subcritical crack growth phenomenon, and ultimatelyof strength degradation. The staircase approach used in thisstudy advocates the use of stress levels for the cyclic load-ing relative to �in values. The initial �app was set empiricallyto �app = 0.5�in, from which the final �ff values can increaseor decrease depending on the frequency of failure or sur-vival within a set of specimens. This means that materialsthat obtained higher �in values were tested under higherloads in the fatigue experiment. These values reached, forinstance, 485 MPa for e.max ZirCAD, 250 MPa for e.max Pressand 180 MPa for e.max CAD, values far over normal chew-ing loads. For these materials, high-load fatigue challengesare interesting to evaluate their performance under extendedapplications, i.e., crowns, short- and/or long-span reconstruct-ions, where they are subjected to higher loads clinically. Forapplications as partial restorations in the posterior segment,in which a comparison to resin composites in meaningful, cor-respondingly lower mastication loads and mechanical fatiguedegradation resulting therefrom should be more relevant.Considering these aspects and the global strength degradationin % observed, a much lower fatigue degradation and longerclinical lifespan would be expected for the zirconium diox-ide and the lithium disilicate ceramic materials under normalchewing loads. The same rationale is valid when comparingresin composites to the two glass-rich ceramics, as for their�app range difference.
4.4. Direct vs. indirect restorations
When based solely on the mechanical performance of therestorative material for choosing between an indirect and adirect technique, our results suggest as follows.
Resin composites may be preferred over glass-rich den-tal ceramic systems due to the low initial strength and highsusceptibility to cyclic fatigue degradation of the latter. Advan-
tages of resin composites are also their higher initial fracturetoughness and superior R-curve behavior, important proper-ties defining the fracture resistance of a material. In low-loadbaring areas where the aforementioned glass-ceramics might
3 0
brthccyacccfto[Irroaiec
bapiafCtpy
miEtld
5
WmcfrcZsmatila
r
d e n t a l m a t e r i a l s
e applicable, a direct technique using resin composites couldender similar or better survival rates. Clinical data seemso support this statement: long-term evaluations (≥10 years)ave shown annual failure rates solely due to fracture foreramic inlays of 0.11% over 10 years for a leucite-basederamic (IPS Empress, Ivoclar-Vivadent) [42], 0.65% over 10ears for a feldspathic porcelain (Vitablocs MK I, Vita) [43],nd 1.04% after 12 years also for IPS Empress [44]. In a singlelinical evaluation of 4.7 years, a comparison between glass-eramic inlays (Evopress, Wegold, Germany) and direct resinomposite restorations (Filtek Z250, 3M ESPE) found annualracture rates of 0.25% for the indirect material and 0.15% forhe direct restorative [45]. Other long-term clinical evaluationsf direct restorations with resin composites have shown 0.64%
46], 0.15% [47], and 0.061% [48] annual fracture rates. In Class cavities, van Dijken [49] found only 1 chip fracture for a directesin composite after 12 years. Further data can be found inecent reviews [2,50,51]. Factors that have shown an influencen fracture rates of glass-ceramic inlays are luting materialnd operator experience [44,52]. The latter was linked to thencreased surface roughness after contact adjustment, whichventually leads to early fractures of the low-toughness glass-eramic restorative material.
Indirect resin composites, according to our study, may alsoe eligible as potential substitutes of glass-rich ceramics inreas of low chewing loads, where they might present com-arable clinical performance to resin composites polymerized
n situ, but hardly better results. In a clinical study of 4 years, 1.1% annual fracture rate was found for Class I and II inlaysor two resin composite materials used indirectly (Artglass andharisma, both Heraeus-Kulzer, Germany) [53]. Others showed
hat when the same materials were used for direct or indirectlacement, an equivalent fracture rate was observed after 11ears [54].
In areas of high mechanical demands, indirect techniquesight be preferred to allow the use of high-strength ceram-
cs, like zirconium oxide and lithium disilicate glass-ceramics.ven at low load challenge areas of the mouth, the use ofhese ceramics are expected to result in longer restorationifetimes than other glass-rich ceramics and restorations pro-uced using the direct technique.
. Conclusions
ithin the limits of our methodology and the selection ofaterials tested here, we could conclude as follows. Resin
omposite materials used for direct restorations are moreatigue resistant than glass-rich ceramics used for indirectestorations in cyclic flexural loading. Direct and indirect resinomposites have shown comparable fatigue performances.irconium dioxide and lithium disilicate-based ceramicshowed the highest initial and residual fatigue strength, anday yield the best clinical performance than resin composites
nd glass-rich ceramics. For the lithium disilicate ceramics,
he amount of glass phase (therefore the amount of crystals)s determinant in their fatigue behavior. Under the same stressevels relative to the initial flexural strength, resin compositesnd dental ceramics present similar fatigue degradation.( 2 0 1 4 ) 424–432 431
Acknowledgements
The authors declare no conflicts of interest related to thematerials tested in the present study. The present workwas performed in partial fulfillment of the requirements forobtaining the degree “Dr. med. dent”.
e f e r e n c e s
[1] Versluis A, Tantbirojn D, Lee S, Tu LS, DeLong R. Canhygroscopic expansion compensate for the polymerizationshrinkage? Part I. Deformation of restored teeth. DentalMaterials 2011;27:126–33.
[2] Demarco FF, Correa MB, Cenci MS, Moraes RR, Opdam NJ.Longevity of posterior composite restorations: not only amatter of materials. Dental Materials 2012;28:87–101.
[3] van de Sande FH, Opdam NJ, Da Rosa Rodolpho PA, CorreaMB, Demarco FF, Cenci MS. Patient risk factors’ influence onsurvival of posterior composites. Journal of Dental Research2013;92:S78–83.
[4] Quinn JB, Sundar V, Lloyd IK. Influence of microstructureand chemistry on the fracture toughness of dental ceramics.Dental Materials 2003;19:603–11.
[5] Ferracane JL. Resin composite – state of the art. DentalMaterials 2011;27:29–38.
[6] Borba M, de Araújo MD, Fukushima KA, Yoshimura HN,Cesar PF, Griggs JA, et al. Effect of microstructure on thelifetime of dental ceramics. Dental Materials 2011;27:710–21.
[7] Gonzaga CC, Cesar PF, Miranda Jr WG, Yoshimura HN. Slowcrack growth and reliability of dental ceramics. DentalMaterials 2011;27:394–406.
[8] Ferracane JL. Resin-based composite performance: Are theresome things we can’t predict. Dental Materials 2013;29:51–8.
[9] Della Bona A, Mecholsky Jr JJ, Anusavice KJ. Fracturebehavior of lithia disilicate- and leucite-based ceramics.Dental Materials 2004;20:956–62.
[10] Lohbauer U, Müller FA, Petschelt A. Influence of surfaceroughness on mechanical strength of resin composite versusglass ceramic materials. Dental Materials 2008;24:250–6.
[11] Mitov G, Lohbauer U, Rabbo MA, Petschelt A, Pospiech P.Investigations of subcritical crack propagation of theEmpress 2 all-ceramic system. Dental Materials2008;24:267–73.
[12] Anusavice KJ. Standardizing failure, success, and survivaldecisions in clinical studies of ceramic and metal–ceramicfixed dental prostheses. Dental Materials 2012;28:102–11.
[13] Bayne SC. Correlation of clinical performance with ‘in vitrotests’ of restorative dental materials that use polymer-basedmatrices. Dental Materials 2012;28:52–71.
[14] Lohbauer U, Belli R, Ferracane JL. Factors involved in thefatigue degradation of dental resin composites. Journal ofDental Research 2013;92:584–91.
[15] Belli R, Lohbauer U, Petschelt A. Are linear elastic materialproperties relevant predictors of the fatigue resistance ofdental resin composites? Dental Materials 2014 [in press].
[16] Lohbauer U, Krämer N, Petschelt A, Frankenberger R.Correlation of in vitro fatigue data and in vivo clinicalperformance of a glass ceramic material. Dental Materials2008;24:39–44.
[17] Kawakami Y, Takeshige F, Hayashi M, Ebisu S. Fatigue of
tooth-colored restoratives in aqueous environment. DentalMaterials Journal 2007;26:1–6.[18] White SN. Mechanical fatigue of a feldspathic dentalporcelain. Dental Materials 1993;9:260–4.

l s 3
after 4 years. Journal of Dentistry 2011;39:478–88.
432 d e n t a l m a t e r i a
[19] Shah MB, Ferracane JL, Kruzic JJ. R-curve behavior andmicromechanisms of fracture in resin based dentalrestorative composites. Journal of the Mechanical Behaviorof Biomedical Materials 2009;2:502–11.
[20] Soappman MJ, Nazari A, Porter JA, Arola D. A comparison offatigue crack growth in resin composite, dentin and theinterface. Dental Materials 2007;23:608–14.
[21] Takeshige F, Kawakami Y, Hayashi M, Ebisu S. Fatiguebehavior of resin composites in aqueous environments.Dental Materials 2007;23:893–9.
[22] European Standard EN-843/5. Mechanical testing ofmonolithic ceramics at room temperature. Part 5: statisticaltreatment; 1997.
[23] Michalske TA, Smith WL, Bunker BC. Fatigue mechanisms inhigh-strength silica-glass fibers. Journal of the AmericanCeramic Society 1991;74:1993–6.
[24] Ritter JE. Engineering design and fatigue failure of brittlematerials. In: Lange FF, editor. Fracture mechanics ofceramics. New York, NY: Plenum Press; 1978. p. 613–46.
[25] Guazzato M, Albakry M, Ringer SP, Swain MV. Strength,fracture toughness and microstructure of a selection ofall-ceramic materials. Part II. Zirconia-based dentalceramics. Dental Materials 2004;20:449–56.
[26] Lohbauer U, Petschelt A, Greil P. Lifetime prediction ofCAD/CAM dental ceramics. Journal of Biomedical MaterialsResearch 2002;63:780–5.
[27] Taskonak B, Griggs JA, Mecholsky Jr JJ, Yan J-H. Analysis ofsubcritical crack growth in dental ceramics using fracturemechanics and fractography. Dental Materials 2008;24:700–7.
[28] Apel E, Deubener J, Bernard A, Höland M, Müller R, KappertH, et al. Phenomena and mechanics of crack propagation inglass-ceramics. Journal of the Mechanical Behavior ofBiomedical Materials 2008;1:313–25.
[29] Studart AR, Filser F, Kocher P, Gaucker LJ. In vitro lifetime ofdental ceramics under cyclic loading in water. Biomaterials2007;28:2695–705.
[30] Studart AR, Filser F, Kocher P, Gaucker LJ. Fatigue of zirconiaunder cyclic loading in water and its implications for thedesign of dental bridges. Dental Materials 2007;23:106–14.
[31] De Aza AH, Chevalier J, Fantozzi G, Schehl M, Torrecillas R.Crack growth resistance of alumina, zirconia and zirconiatoughened alumina ceramics for joint prostheses.Biomaterials 2002;23:937–45.
[32] Chevalier J, Gremillard L. The tetragonal-monoclinic inzirconia; lessons learned and future trends. Journal of theAmerican Ceramic Society 2009;92:1901–20.
[33] Chevalier J, Olagnon C, Fantozzi G, Cales B. Subcritical crackgrowth and thresholds in a 3Y-TZP ceramic under static andcyclic loading conditions. Ceramics International1997;23:263–6.
[34] El Attaoui H, Saadaoui M, Chevalier J, Fantozzi G. Static andcyclic crack propagation in Ce-TZP ceramics with differentamounts of transformation toughening. Journal of theEuropean Ceramic Society 2007;27:483–6.
[35] Ferracane JL. Hygroscopic and hydrolytic effects in dentalpolymer networks. Dental Materials 2006;22:211–22.
[36] Drummond JL, Lin L, Al-Turki LA, Hurley RK. Fatiguebehaviour of dental composite materials. Journal of
Dentistry 2009;37:321–30.[37] Lin L, Drummond JL. Cyclic loading of notched dentalcomposite specimens. Dental Materials 2010;26:207–14.
0 ( 2 0 1 4 ) 424–432
[38] Ravindranath V, Gosz M, De Santiago E, Drummond JL,Mostovoy S. Effect of cyclic loading and environmental agingon the fracture toughness of dental resin composite. Journalof Biomedical Materials Research Part B: AppliedBiomaterials 2007;80B:226–35.
[39] Shah MB, Ferracane JL, Kruzic JJ. R-curve behavior andtoughening mechanisms of resin-based dental composites:effects of hydration and post-cure heat treatment. DentalMaterials 2009;25:760–70.
[40] De Souza JA, Goutianos S, Skovgaard M, Sorensen BF.Fracture resistance curves and toughening mechanisms inpolymer based dental composites. Journal of the MechanicalBehavior of Biomedical Materials 2011;4:558–71.
[41] Ornaghi BP. Subcritical crack growth and in vivo lifetimeprediction of resin composites with different fillerdistribution. Dental Materials 2012;28:985–95.
[42] Stoll R, Cappel I, Jablonski-Momeni A, Pieper K, Stachniss V.Survival of inlays and partial crowns made of IPS Empressafter a 10-year observation period and in relation to varioustreatment parameters. Operative Dentistry 2007;32:556–63.
[43] Otto T, De Nisco S. Computer-aided direct ceramicrestorations: a 10-years prospective clinical study of CerecCAD/CAM inlays and onlays. International Journal ofProsthodontics 2002;15:122–8.
[44] Frankenberger R, Taschner M, Garcia-Godoy F, Petschelt A,Krämer N. Leucita-reinforced glass ceramic inlays andonlays after 12 years. Journal of Adhesive Dentistry2008;5:393–8.
[45] Lange RT, Pfeiffer P. Clinical evaluation of ceramic inlayscompared to composite restorations. Operative Dentistry2009;34:263–72.
[46] Da Rosa Rodolpho PA, Donassollo TA, Cenci MS, LoguercioAD, Moraes RR, Bronkhorst EM, et al. 22-Year clinicalevaluation of the performance of two posterior compositeswith different filler characteristics. Dental Materials2011;27:955–63.
[47] Gaengler P, Hoyer I, Montag R. Clinical evaluation ofposterior composite restorations: the 10-year report. Journalof Adhesive Dentistry 2001;3:185–94.
[48] Opdam NJM, Bronkhorst EM, Roeters JM, Loomans BAC. Aretrospective clinical study on longevity of posteriorcomposite and amalgam restorations. Dental Materials2007;23:2–8.
[49] van Dijken JWV. Durability of resin composite restorations inhigh C-factor cavities: a 12-year follow-up. Journal ofDentistry 2010;38:469–74.
[50] Della Bona A, Kelly RJ. The clinical success of all-ceramicrestorations. Journal of the American Dental Association2008;139(9 Suppl.):8S–13S.
[51] Kubo S. Longevity of resin composite restorations. JapaneseDental Science Review 2011;47:43–55.
[52] Frankenberger R, Reinelt C, Petschelt A, Krämer N. Operatorvs. material influence on clinical outcome of bondedceramic inlays. Dental Materials 2009;25:960–8.
[53] Huth KC, Chen HY, Mehl A, Hickel R, Manhart J. Clinicalstudy of indirect composite resin inlays in posteriorstress-bearing cavities placed by dental students: Results
[54] Pallesen U, Qvist V. Composite resin fillings and inlays. An11-year evaluation. Clinical Oral Investigations 2003;7:71–9.





















![Enhanced photocatalytic degradation of RO16 dye using Ag ... 35 05.pdf · Processing and Applicationof Ceramics 11 [1] (2017)27–38 DOI: 10.2298/PAC1701027S Enhanced photocatalytic](https://img.pdfslide.us/doc/110x75/5f7c7b02f0b85826e57ddcbb/enhanced-photocatalytic-degradation-of-ro16-dye-using-ag-35-05pdf-processing.jpg)