Embed Size (px)
Citation preview

© 2014 by National Association of Orthopaedic Nurses Orthopaedic Nursing • November/December 2014 • Volume 33 • Number 6 331
Measuring patient outcomes is becoming in-creasingly important as the healthcare sys-tem evolves into one that demands effi cien-cies and quality. The concept of measuring
clinical outcomes is not new. In 2000, the Agency for Healthcare Research and Quality stated that “No longer just the domain of a small cadre of researchers, out-comes research has altered the culture of clinical prac-tice and health care research by changing how we assess the end results of health care services. In doing so, it has provided the foundation for measuring the quality of care. The results of AHRQ outcomes research are be-coming part of the ‘report cards’ that purchasers and consumers can use to assess the quality of care in health plans. For public programs such as Medicaid and Medicare, outcomes research provides policymakers with the tools to monitor and improve quality both in traditional settings and under managed care. Outcomes research is the key to knowing not only what quality of care we can achieve, but how we can achieve it.”
In today’s environment, there is a mandate to im-prove the quality of care and at the same time control cost, which is driving organizations and clinicians to look at ways to monitor the care that they provide and look for ways to improve when necessary. This has raised the question, how can clinical outcomes be effi ciently monitored and then evaluate those data to make change?
What matters most to one entity may matter least to another. For example, length of stay following a total joint replacement is very important to hospitals and payors and is not nearly as important to the patient who is more interested in the clinical outcome of less pain and improved quality of life. Fromme, Eilers, Mori, Hsieh, and Beer (2004) found that the clinician's
Measuring Outcomes in Orthopaedics Implementation of an Outcomes Program in an Outpatient Orthopaedic Practice
Mary F. Rodts ▼ Renée Glanzman ▼ Adam Gray ▼ Randal Johnson ▼ Dennis Viellieu ▼ Fadi Hachem
With increased demand to provide quality care for patients, orthopaedic practices will need to develop ways to effi ciently collect and manage data to support the care that they pro-vide. An outcomes management program must be effi cient and consistent to provide good data. This article describes the implementation of an outcomes program at one large private orthopaedic practice within an academic medical setting.
perceptions often varied greatly from their patients. It, therefore, is important to look at many facets of the pa-tient’s care to develop improved care protocols.
Nurse researchers have valued the patient-reported out-come as an essential element to develop practice change (Bella, Ross, & Cella, 2014). In recent years, regulatory groups and payors have begun to see the value in patient-reported outcomes. The National Institutes of Health sup-ported the development of PROMIS, Patient-Reported Outcomes Measurement Information System, which is available online and has numerous valid tools that measure physical, mental, and social well-being ( PROMIS, 2014 ). The importance of assessing the patient’s thoughts on their care can be evaluated in relation to other traditional clini-cal outcomes measurements, resulting in a more compre-hensive understanding of a particular problem.
The Data Throughout the care continuum, there are many differ-ent opportunities to gather data on the care the patient receives whether that be related to inpatient or outpatient settings. Drawing on each piece of data is
Mary F. Rodts, DNP, CNP, ONC, FAAN , Associate Professor, Rush College of Nursing, Chief Operating Offi cer, Midwest Orthopaedics at Rush, Chicago, IL.
Renée Glanzman, MS-Health Systems Management , Care Transformation Manager and Compliance Offi cer, Midwest Orthopaedics at Rush, Chicago, IL.
Adam Gray, MS-Health Systems Management , Formerly, Application Implementation Specialist, Midwest Orthopaedics at Rush, Currently, Medical Student, Des Moines University, Des Moines, IA.
Randal Johnson, MBA , Chief Financial Offi cer, Midwest Orthopaedics at Rush, Chicago, IL.
Dennis Viellieu, BS, Chief Executive Offi cer, Midwest Orthopaedics at Rush, Chicago, IL.
Fadi Hachem, MS-Health Systems Management , Manager of Patient Experience, Midwest Orthopaedics at Rush, Chicago, IL.
Supplemental digital content is available for this article. Direct URL citations appearing in the printed text are provided in the HTML and PDF version of this article on the journal’s web site (www.orthopaedicnursing.com).
The authors have disclosed no potential confl icts of interest, fi nancial or otherwise.
DOI: 10.1097/NOR.0000000000000103
2.0ANCCContactHours
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ768_LR 331ONJ768_LR 331 11/11/14 11:51 PM11/11/14 11:51 PM

332 Orthopaedic Nursing • November/December 2014 • Volume 33 • Number 6 © 2014 by National Association of Orthopaedic Nurses
FIGURE 1. Institute for Healthcare Improvement’s Triple Aim.
important when determining the advantages of a spe-cifi c care protocol. Typical data that have historically been used are the Retrospective Hospital Data and Patient Satisfaction scores. More recently, data from the Physician Quality Reporting System have been re-quired. Patient-reported outcomes will be an additional element that will be evaluated in the near future.
• Retrospective hospital data : These are typical in-dicators of quality at the hospital level and are typically centered around a single hospital stay or a 90-day global period for surgeries. These data are also triggered by hospital entry or admission of a patient. Readmission rates and infections rates are two indicators that are being followed.
• Patient surveys : General satisfaction questions provide data regarding both the environment of care and the interactions patients have with staff. Although surveys do not typically ask patients spe-cifi c questions regarding the quality of care re-ceived, studies have found that higher overall sat-isfaction scores are associated with better performance on various clinical quality measures ( Jha, Orav, Zheng, & Epstein, 2008 ; Glickman, 2010). This suggests that patient perceptions can be a good indicator of the quality of care received and adds validity to the idea that improving pa-tient satisfaction scores can also have an impact on clinical quality.
The Clinician and Group Consumer Assessment of Healthcare Providers and Systems (CGCAHPS) survey, which will be required for providers to submit in the near future, gathers information about the individual interaction with the providers and their staff during one offi ce visit. The question domains include the following:
� Getting timely appointments, care, and informa-tion
� How well providers (or doctors) communicate with patients
� Helpful, courteous, and respectful offi ce staff � Patients’ rating of the provider (or doctor) � Individual item: follow-up on test results
The CGCAHPS does not ask questions about how the treatment improved the patient’s quality of life. While the CGCAHPS survey is valuable, it is only one piece of the patient care algorithm.
• Physician Quality Reporting System was instituted by the Centers for Medicare and Medicaid Services in an effort to have providers look at the quality of care that they provide to patients. Multiple quality metrics are available to the clinician to report back to the Centers for Medicare and Medicaid Services to demonstrate the care that is provided which can then be compared with other providers.
• Clinical Outcomes Questionnaires: Historically, clinical outcomes surveys were used for research subjects and were done through paper. A research assistant would then manually enter this informa-tion for analysis. The data sample was often very specifi c and only as large as the overall study pop-ulation. Therefore, clinical outcomes measure-
ment has been utilized only in a minimum number of patients and for certain problems. The importance of evaluating clinical outcomes in all patients who undergo any type of care regimen is to see whether the patients believe the treatment they have received has improved their quality of life. An example in orthopaedics might be the re-view of the perfect postoperative total hip replace-ment radiograph, yet the patient’s reported out-comes demonstrate continued pain and disability.
Changing Healthcare Environment With the passing of the Affordable Care Act, the Institute for Healthcare Improvement's “Triple Aim” to improve the patient experience of care, to improve the overall health of populations, while reducing the cost per capita of healthcare, has become the framework for many of the federal government’s healthcare programs and initiatives ( Berwick, Nolan, & Whittington, 2008 ).
Three elements of the triple aim (see Figure 1 ) are the implementation of the Value Based Modifi er, which is determined by self-reported quality metrics; outcomes measurements to evaluate readmissions, acute preven-tive quality indicators, and chronic preventive quality indicators; and the management of patient populations through care management via Accountable Care Organizations/Medical Homes to obtain desired out-comes and control cost. All of these initiatives will re-quire data capture and reporting and are currently or will impact overall reimbursement.
The transition to a value-based healthcare environ-ment has arrived. It is now important to determine the factors that make up quality and thus what needs to be measured because if you cannot measure it, you cannot manage it. The inability to manage these factors will be detrimental to a practice in the coming years. According to Andrawis, Chenok, and Bozic (2013), the outcome
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ768_LR 332ONJ768_LR 332 11/11/14 11:51 PM11/11/14 11:51 PM

© 2014 by National Association of Orthopaedic Nurses Orthopaedic Nursing • November/December 2014 • Volume 33 • Number 6 333
FIGURE 2. Important components of the research tool.
measures that are needed to determine “value” have not been typically collected. Outcomes need to be collected to provide the additional data necessary to develop quality, cost-effective, and effi cient care.
What exactly is quality can be divided into two as-pects: clinical and perceived. Patient perception is cap-tured through surveys such as CGCAHPS and will be directly linked to payment incentives in value-based care. What a patient perceives to be part of quality care might be seen as inconsequential to the clinician. For example, a patient may relate quality care to how soon they can get back to work. Return to work/activity is something that is not being captured on CGCAHPS. Perceived and clinical outcomes of quality are very much dependent on one another. A patient’s pain level or quick return to the golf course can reduce the nega-tive feelings of a brief interaction with a provider after a lengthy wait time in the clinic offi ce. It is also important to note that on an individual level both the experience and clinical result are important to quality patient care. Both will also soon have a fi nancial impact on all prac-tices, so development of a system to capture and man-age this information is vital.
With the growing movement of transitioning care to-ward value with quality and cost containment, there is a large need for patient-driven data. The patient’s individual experience in regard to the clinical care re-ceived and the outcomes within their daily lives are nec-essary outcomes to track. Technology needs to be imple-mented and leveraged to reach patients on an individual level and on a consistent basis. This will allow providers to measure the entire episode of care in terms of the patients’ abilities, function, and pain.
The other advantage of leveraging the technology is that the data used for current and future research will be easily utilized in a database to identify trends of much larger samples than previously captured. The ability to automate the process ensures that the ques-tionnaires are presented to the patient on an ongoing basis and not dependent upon the manual push of the survey with the inherent error associated with that manual process.
Case Study
B ACKGROUND Midwest Orthopaedics at Rush is a private orthopaedic practice associated with Rush University Medical Center in Chicago. The forty-one physician members and their staffs of Midwest Orthopaedics at Rush have a long-standing history and commitment to high-level research activities at both the national and international levels. Capturing clinical data had been a manual process re-quiring research assistants to manually enter the data into individual databases. With the need to include more patients in clinical outcomes research, manual entry and following of patient compliance would be onerous.
P ROCESS In 2012, the group began looking at ways to become more effi cient with data collection and data mining.
Several key factors (see Figure 2 ) in the selection of the appropriate research tool were identifi ed: sound re-search methodologies for collection of data; automation of data collection; ease of mining the clinical data; secu-rity of patient data; and the ability to benchmark data with other programs across the country.
The fi rst step in this process was to obtain the institu-tional review board approval for the development of a repository of data. Once this was accomplished, the eval-uation process of available research tools was under-taken by a core group of clinical and administrative staff. The VR 12 was selected as the quality-of-life tool that would be used for all patients being seen in the practice. In addition, each subspecialty came to consensus on what minimum outcomes tools would be collected. Table 1 is the current list of the outcomes tools that are being used by the various subspecialties. Additional tools may be introduced for a specifi c study, as demon-strated by the comprehensive list for study participants (Supplemental Table 2, http://links.lww.com/onj/A6).
To understand the effects of care given, it is crucial to measure various metrics within the care process as well as the overall clinical outcome. Through the collection of these data, practices can begin to understand the ef-fects of different treatment paths and interventions, for both clinical and cost-effectiveness. The downstream impact of this knowledge will lead to enhanced decision making from the provider, thus improving quality and cost of care, leading to stronger negotiating power with payors and an overall better reputation in the commu-nity. There are challenges that exist in being able to col-lect patient-reported outcomes in the offi ce setting; how-ever, the value to bring this information to payors and hospital systems should drive practices to seek a way to manage an outcomes program. If the implementation of a patient-reported outcomes program seems impossible, evaluation of existing registries such as the Functional Outcomes Research and Comparative Effectiveness in Total Joint Replacement (FORCE-TJR), which was funded by the Agency for Healthcare Research and Quality, should be explored ( Ayers & Bozic, 2013 ). The American Joint Replacement Registry (AJRR) is also managing data for total joint replacement patients.
S OLUTION Ayers, Zheng, and Franklin (2013) discussed the need to fi nd a way to collect outcomes in an effi cient manner outside of the offi ce visit. In late 2012, the Outcomes Based Electronic Research Database (OBERD) system was selected as the tool to automate the collection of clinical outcome data for Midwest Orthopaedics at Rush. The system works in conjunction with the elec-tronic practice management/electronic health record system and captures all information electronically, with
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ768_LR 333ONJ768_LR 333 11/11/14 11:51 PM11/11/14 11:51 PM

334 Orthopaedic Nursing • November/December 2014 • Volume 33 • Number 6 © 2014 by National Association of Orthopaedic Nurses
FIGURE 3. Home versus clinic form completion.
TABLE 1. MOR MINIMUM OUTCOMES PER SPECIALTY
MOR Minimum Outcomes By Subspecialty Outcomes
Hand/wrist VR-12/DASH (Disability of Arm, Shoulder and Hand)
Elbow VR-12/DASH (Disability of Arm, Shoulder and Hand)
Spine & PMR
Cervical VR-12/NDI (Neck Disability Index)
Lumbar VR-12/ODI (Oswestry Disability Index)
Deformity VR-12/SRS-22 (Scoliosis Research Society)
Joints
Hip VR-12/HHS (Harris Hip Screening)
Knee VR-12/KSS (Knee Society Score)
Foot & Ankle VR-12/FAAM (Foot and Ankle Ability Measure)
Sports
Shoulder VR-12/ASES (American Shoulder and Elbow Surgeons Outcome)
Elbow VR-12/DASH (Disability of Arm, Shoulder and Hand)
Knee VR-12/IKDC (International Knee Documentation Committee)
Hip VR-12/HOS (Hip Outcome Score)
most aspects entirely automated and integrated into the EHR. Being able to collect the patient reported out-comes prior to the offi ce visit is ideal as it lessens the disruption to the clinic schedule. Operationally, this means when the patient schedules a new patient ap-pointment, all forms are automatically e-mailed to the patient prior to the visit. This new patient set of forms consists of registration forms that include demograph-ics, consents, and the patient history form as well as outcomes forms. The patient is encouraged to complete the forms in the comfort of their homes or offi ces. At this time, there is approximately a 70% completion rate prior to the offi ce visit (see Figure 3 ). The ability to cap-ture this information prior to the offi ce visit has im-proved patient throughput through the offi ce visit.
C OMPLEXITY OF M EASURING O UTCOMES IN O RTHOPAEDICS There are many different patient-reported outcome tools available for the orthopaedic patient population. Being able to effi ciently distribute the appropriate out-
come tool is key to success in an outcomes program. Completion of those forms needs to occur. Schamber, Takemoto, Chenok, and BOzik (2013) reported that when an electronic method was utilized that there was an increased chance that the forms would be completed than those patients who used paper surveys. The effi -ciency that is a direct result of the electronic data cap-ture is also very important. The manual data entry error is eliminated.
Because of the many different types of orthopaedic problems, many different outcome tools are required to capture the appropriate data. Currently more than 40 different outcomes tools are in use and assigned on the basis of the particular problem such as the Harris Hip Score, Disabilities of the Arm, Shoulder and Hand (DASH), Neck Disability Index, Oswestry Disability Index, and Foot and Ankle Ability Measure. Upon initial implementation, multiple outcomes forms were assigned to the patient on the basis of the problem the patient was being seen for. The lesson learned from this was that too many forms were sent
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ768_LR 334ONJ768_LR 334 11/11/14 11:51 PM11/11/14 11:51 PM

© 2014 by National Association of Orthopaedic Nurses Orthopaedic Nursing • November/December 2014 • Volume 33 • Number 6 335
to the patient, requiring a signifi cant time commit-ment. Currently, the VR12, a simple quality-of-life survey, is the only one that is sent out to all new pa-tients. Additional surveys are assigned following the initial patient appointment. This allows the clinicians to have a discussion with the patient about the out-comes forms and how this will help manage their healthcare.
For the sports medicine subspecialty, if the patient is scheduled for a rotator cuff surgery, the following forms are assigned: Western Ontario Rotator Cuff Index, Constant, American Shoulder and Elbow Surgeons, and the Single Assessment Numeric Evaluation. The forms are sent to the patient electroni-cally 1 week prior to surgery and then again at 3-month, 6-month, 1-year, and 2-year postoperative intervals.
The baseline measurement can then be compared with the follow-up surveys .
H OW I T W ORKS At the time of the fi rst call to schedule a patient, the scheduling department explains to the patient how he or she will receive their new patient forms to be com-pleted. Our registration and outcomes tool automati-cally assigns questionnaires according to the appoint-ment type selected in the Electronic Health Record when the appointment is scheduled. The patient is sent an e-mail 1 week prior to that appointment, which pro-vides a link to the patient portal where their forms will be found (see Figures 4a and 4b ). The patient is encour-aged to complete the forms prior to his or her visit.
FIGURE 4. (A) Example of the e-mail the patient receives. (B) The patient’s view of the forms that need completion.
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ768_LR 335ONJ768_LR 335 11/11/14 11:51 PM11/11/14 11:51 PM
336 Orthopaedic Nursing • November/December 2014 • Volume 33 • Number 6 © 2014 by National Association of Orthopaedic Nurses
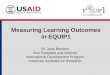
Managing the completion of the surveys is very im-portant. The OBERD dashboard provides the necessary information for the individual physician staff to oversee the process of survey completion (see Figure 5 ). One week prior to the appointment, the secretarial staff be-gins monitoring their patient appointments for the fol-lowing week. If an e-mail address is missing, the secretary is to obtain the e-mail so that the automated process will work. If the forms are not completed, the system is automated to remind the patients every 3 days until completion. The secretaries also have the option to manually remind patients through a remind button. At this time the completion rate prior to the offi ce visit is approximately 70%. We have found that when the indi-vidual physician's secretary engages the patient and fur-ther explains the need for an e-mail, the formerly reti-cent patient agrees.
On the day of the appointment, the patient represent-ative at the front desk reviews the completion data and if the patient has not completed the forms prior to the visit, an iPad is given to the patient to complete the forms in the waiting room. Once the forms are completed, the in-formation is directly integrated into the Electronic Health Record. This occurs real time and is available im-mediately to the clinicians. In an effort to make this in-formation easy to view and utilize in the clinic setting,
the front sheet document was developed. The front sheet is a synthesis and clear presentation of the information that the patient has provided. The front sheet is custom-izable by physician to include or reorder the information in the way that he or she wants to see the information.
From the front sheet, the physician is able to look at the patient’s outcome scores. This information can be shared with the patient to demonstrate improvement following treatment (see Figure 6 ). Improvement can be monitored on both operative and nonoperative patients. Figure 7 demonstrates how outcomes information is presented to the providers. This patient was fi rst seen as a new patient on August 1, 2013. The patient completed the SF 12 and VR 12 quality-of-life questionnaires. The patient had surgery on August 14 and then completed the same forms in 3-month intervals from the original appointment. The VR 12 is a quality-of-life question-naire, which gauges both physical and mental health and will be the required quality-of-life survey to report in the near future. The graph shows the marked im-provement in the patient’s perception of physical health.
C HALLENGES There are multiple challenges associated with imple-menting clinical outcomes collection in the outpatient
FIGURE 5. OBERD (Outcomes Based Electronic Research Database) dashboard demonstrating patients with assigned forms. (A, in box) New patients receive the complete set of forms; H = History, R = Registration, C = Consents, I = PQRS, and O = Outcomes. (B, in box) Forms in the process of being completed in real time.
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ768_LR 336ONJ768_LR 336 11/11/14 11:51 PM11/11/14 11:51 PM

© 2014 by National Association of Orthopaedic Nurses Orthopaedic Nursing • November/December 2014 • Volume 33 • Number 6 337
FIGURE 6. Example of the clinician front sheet where access to the outcome trends is easily retrievable to allow sharing of this information with the patient.
FIGURE 7. Outcomes data for a postoperative patient.
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ768_LR 337ONJ768_LR 337 11/11/14 11:51 PM11/11/14 11:51 PM

338 Orthopaedic Nursing • November/December 2014 • Volume 33 • Number 6 © 2014 by National Association of Orthopaedic Nurses
setting. Automation of the process is critical to be sure that outcomes are collected at the scheduled intervals. A strong research tool is necessary but works well only when the information to correctly trigger the dissemi-nation of tools works. The practice e-mail capture rate was identifi ed early on in this process as being a key factor to make the electronic distribution of forms suc-cessful. Education of staff to the importance of this in-formation is an ongoing part of this program.
One of the biggest challenges has been the time re-quirement for the complete set of questionnaires. The registration form takes approximately 20 minutes to complete. Add that with averages of 30 minutes for our health history, 4 minutes for a VR 12, 2 minutes for the study consent, and 2 minutes for a PQRS questionnaire, and the total time is approximately 1 hour. Engaging all staff to make it a priority to obtain e-mail addresses if one is not in the patient record has improved the preof-fice visit completion rate to greater than 75%. Completing the forms on an iPad in the waiting room is always the last resort for our patients, especially the new patients who have multiple questionnaires to com-plete. Because the workload of the patient representa-tive has now lessened, the patient representative is now available to assist the patients who have been unable to complete the forms prior to the visit. The patient is told to come to the offi ce earlier to be sure that this is accom-plished.
An initial concern by the implementation team was how different age groups would respond to the surveys and if there would be differences noted by age groups. Figure 8 demonstrates the completion of the registra-tion forms by age group. While there was increased time noted in the patients older than 65 years, there have been few complaints across all age groups in regard to electronic survey completion.
Another challenge was to evaluate the cost of the out-comes system. Because of the commitment to research by the organization and in an effort to increase outcomes data capture with the potential for managing care protocols, the decision was made to implement the OBERD tool.
With any new program, evaluation of the process and ongoing management was necessary. The ongoing train-ing of staff, research protocol development, and patient
support were seen as necessary to the success of the out-comes program. A Manager of Patient Experience was hired who is dedicated to the maintenance of the sys-tem, the training of the staff, troubleshooting clinician and staff problems, and the patient interaction with the system. Additional responsibilities of this position are to oversee the patient satisfaction program and the edu-cational modules that the patients receive.
W HAT ’ S N EXT ? Data, data, data. There is plenty of data to work with as we begin to evaluate every aspect of the patient care that is provided by the organization. It is critical that patient compliance be monitored and increased. E-mail cap-ture, as well as providing easy access for patients to uti-lize the patient portal, is necessary. The focus will be on increasing the patient engagement and participation with their clinicians via the patient portal.
It is now time to evaluate the data that have been col-lected, and understand how the patient populations can be grouped to better understand and improve clinical pathways. Comparing the patient reported outcomes with functional outcomes will be necessary to deter-mine if care protocols are successful. In addition, com-parison of patient-reported outcomes with patient satis-faction questionnaires will be evaluated.
Finally, the integration of the accurate health history information that is being collected via the research tool into the EHR will provide a great opportunity to look very carefully at other aspects of the patient history that may impact outcomes. This information will be not only a benefi t for this practice but also invaluable, as sharing of clinical data advances via the Health Information Exchanges.
Conclusion Midwest Orthopaedics at Rush identifi ed the need to be-come proactive in developing the necessary platform to be able to easily collect patient-reported outcomes and registration information. By the identifi cation of an effi -cient research platform, the practice is now able to col-lect patient-reported outcomes on all patients. This is the fi rst step in having data to support future care initiatives.
FIGURE 8. Time to complete forms by age group.
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ768_LR 338ONJ768_LR 338 11/11/14 11:51 PM11/11/14 11:51 PM
© 2014 by National Association of Orthopaedic Nurses Orthopaedic Nursing • November/December 2014 • Volume 33 • Number 6 339
R EFERENCES Agency for Healthcare Quality and Research . ( 2000 ).
Clinical outcomes . Retrieved from http://www.ahrq.gov/research/findings/factsheets/outcomes/outfact/index.html
Agency for Healthcare Quality and Research . ( 2014a ). Selecting health outcome measures for clinical quality measurement . Retrieved September 21, 2014, from http://www.qualitymeasures.ahrq.gov/tutorial/HealthOutcomeMeasure.aspx
Agency for Healthcare Quality and Research . ( 2014b ). CAHPS clinician & group visit survey . Retrieved from https://cahps.ahrq.gov/surveys-guidance/cg/visit/index.html
Andrawis , J. , Chenok , K. , & Bozic , K. ( 2013 ). Health policy implications of outcomes measurement in orthopae-dics . Clinical Orthopaedics and Related Research , 471 , 3475 – 3481 .
Ayers , D. , & Bozic , K. ( 2013 ). The importance of outcome measurement in orthopaedics . Clinical Orthopaedics and Related Research , 471 , 3409 – 3411 .
Ayers , C. , Zheng , H. , & Franklin , P. ( 2013 ). Integrating pa-tient-reported outcomes into orthopaedic clinical practice . Clinical Orthopaedics and Related Research , 471 , 3419 – 3425 .
Berwick , D. , Nolan , T. , & Whittington , J. ( 2008 ). The triple aim: Care, health, and cost. Health Affairs , 27 ( 3 ), 759 – 769.
Bevans , M. , Ross , A. , & Cella , D. ( 2014 ). Patient-Reported Outcomes Measurement Information System (PROMIS): Effi cient, standardized tools to measure self-reported health and quality of life . Nursing Outlook , 61 ( 5 ), 339 – 345 .
Fromme , E. , Eilers , K. , Mori , M. , Hsieh , Y. , & Beer , T. ( 2004 ). How accurate is clinical reporting of chemotherapy adverse effects? A comparison with patient-reported symptoms and Quality-of-Life Questionnaire C30 . Journal of Clinical Quality , 22 , 3495 – 3490 .
Glickman , S. , Boulding , W. , Manary , M. , et al. ( 2010 ). Patient satisfaction and its relationship with clinical quality and inpatient mortality in acute myocardial infarction . Clinical Cardiovascular Quality Outcomes , 3 ( 2 ), 188 – 195 .
Jha , K. , Orav , J. , Zheng , J. , & Epstein , A. ( 2008 ). Patients’ perception of hospital care in the United States . The New England Journal of Medicine , 359 ( 18 ), 1921 – 1931 .
PROMIS. (Patient-Reported Outcomes Measurement Information System) . ( 2014 ). Retrieved from http://www.nihpromis.org/about/overview
Schamber , E. , Takemoto , S. , Chenok , K. , & BOzik , K. ( 2013 ). Barriers to completion of patient reported outcome measures . The Journal of Arthroplasty , 28 , 1449 – 1453 .
For 13 additional continuing nursing education articles on sports injuries, go to nursingcenter.com/ce.
Copyright © 2014 by National Association of Orthopaedic Nurses. Unauthorized reproduction of this article is prohibited.
ONJ768_LR 339ONJ768_LR 339 11/11/14 11:51 PM11/11/14 11:51 PM