Embed Size (px)
Citation preview
Measuring Health Workforce Distribution Inequalities in Uganda
Anna Awor, Elaine Byrne and Ruairi Brugha
The ChallengeMany challenges:– Staff shortages – uneven distribution– gaps in skills and competencies– low retention & poor motivation– limited funding for recruitment– constricted career structure– Lack of champions for health– lack of recognition & shortage of role models, – ineffective training materials and methods:
Without overcoming these challenges, attainment of Millennium Development Goals will not be possible in most developing countries.
Objective
• Assess regional distribution and skill mix of health workers at the Regional Referral Hospitals (RRH) in Uganda, in order to illustrate the imbalances in geographical distribution and skills mix
• The analysis was based on the critical HRH levels in the Regional Referral Hospitals
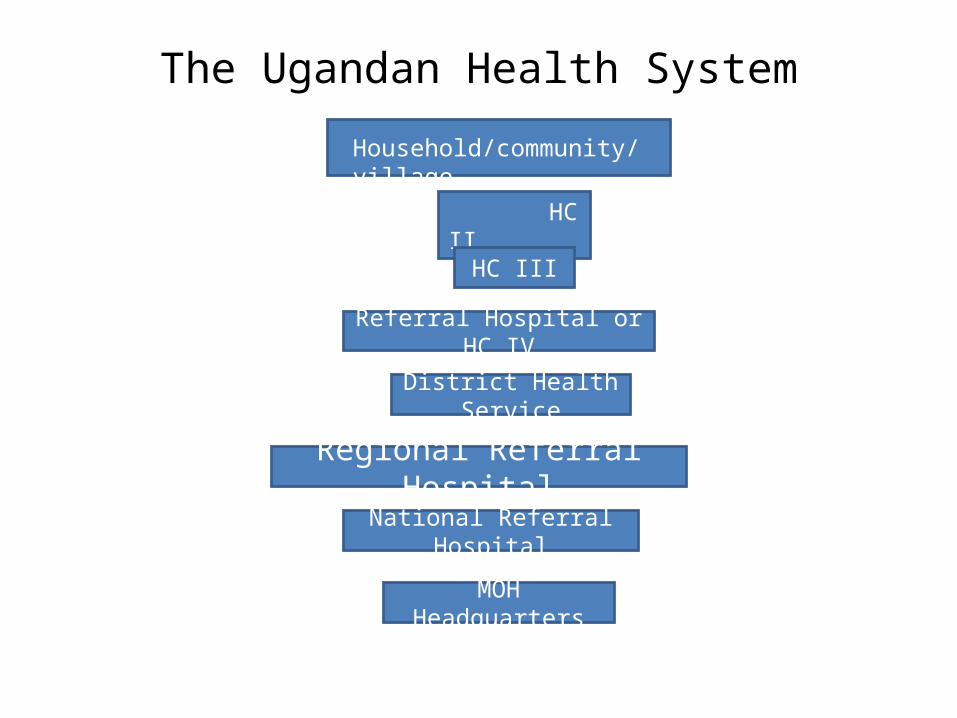
The Ugandan Health System
Household/community/village
HC II
HC III
Regional Referral Hospital
MOH Headquarters
National Referral Hospital
District Health Service
Referral Hospital or HC IV
Functions of the Regional Referral Hospitals• Preventive, promotive, curative, maternity, in-
patient health, and blood transfusion services• Specialist clinical services such as psychiatry,
ENT, ophthalmology, higher level surgical and medical, and clinical support
• In-service training, consultation and operational research in support of the community-based health care programmes
• Teaching and research* each RRH provide services to 2 million people
Methods
Using data from the ministry of health HRH audit report 2010, we:•Analysed the distribution of health workers in the 12 regional referral hospitals in Uganda. •Compared proportions of vacant positions with the set norm for various cadres at the 12 RRH.•Analysed cadre-specific (skill mix) distributions of health workers focusing on the specialised services in the 12 RRH.
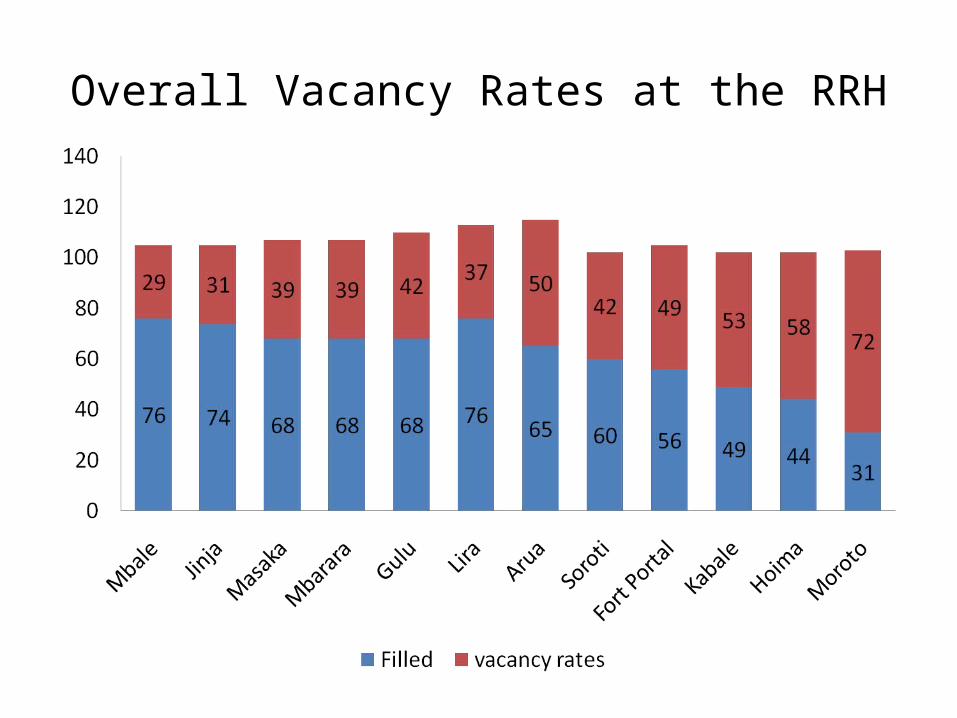
Overall Vacancy Rates at the RRH
Overall Vacancy Rates
The health sector strategic plan (HSSP II, 2006-2010) set a staffing level of 65%, of which 4 RRH are lower than this level:•Soroti at 60%,•Fort Portal at 56%, •Kabale at 49%, •Moroto at 31%.
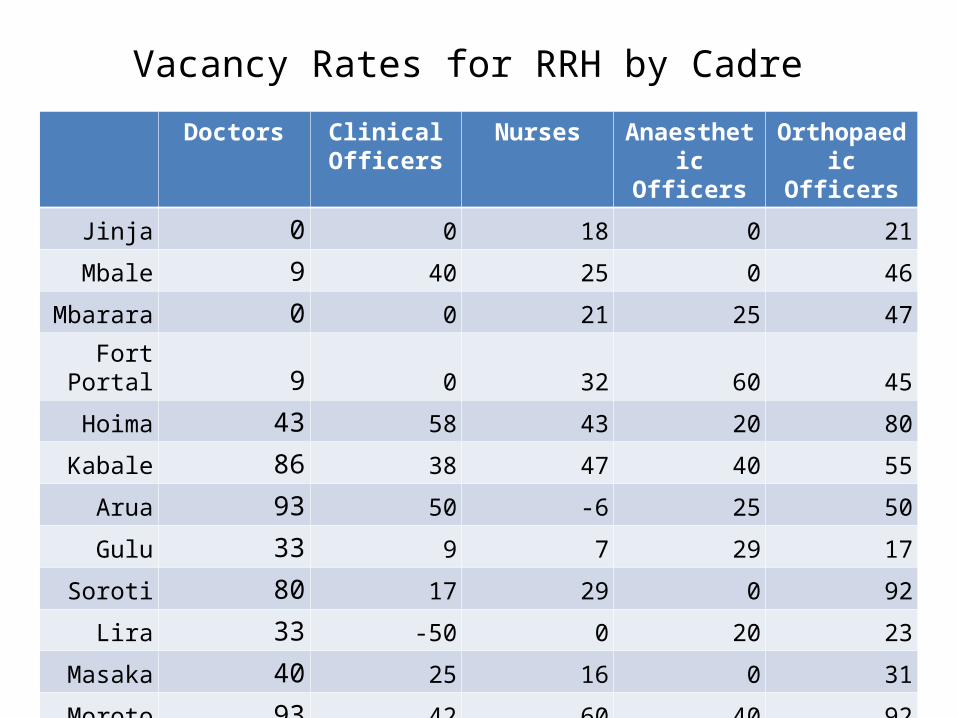
Vacancy Rates for RRH by Cadre
Doctors Clinical Officers
Nurses Anaesthetic Officers
Orthopaedic Officers
Jinja 0 0 18 0 21
Mbale 9 40 25 0 46
Mbarara 0 0 21 25 47
Fort Portal 9 0 32 60 45
Hoima 43 58 43 20 80
Kabale 86 38 47 40 55
Arua 93 50 -6 25 50
Gulu 33 9 7 29 17
Soroti 80 17 29 0 92
Lira 33 -50 0 20 23
Masaka 40 25 16 0 31
Moroto 93 42 60 40 92
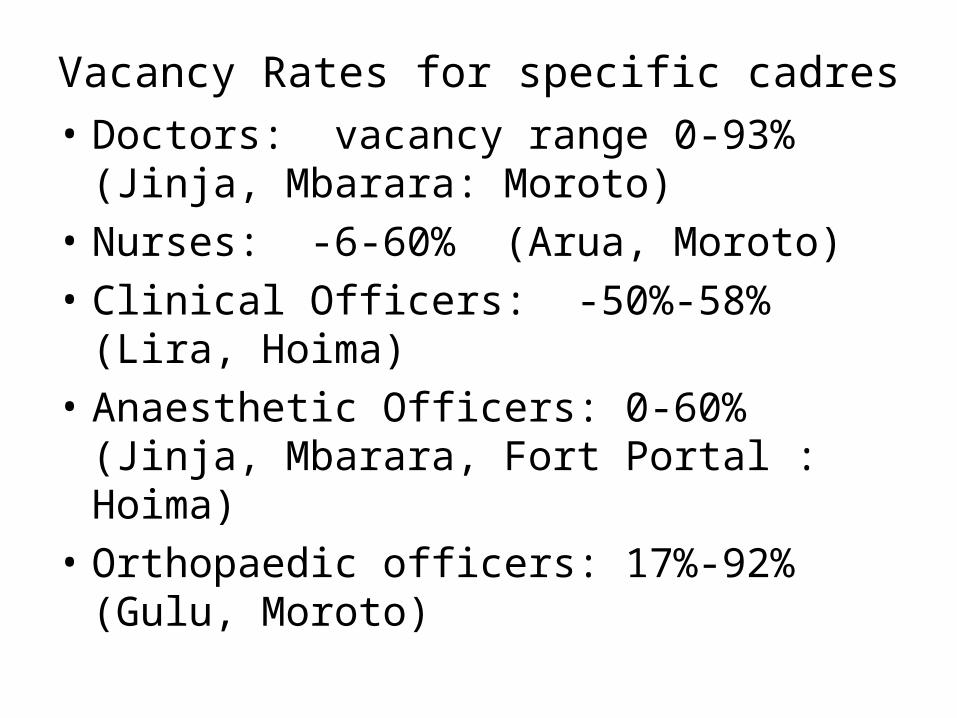
Vacancy Rates for specific cadres• Doctors: vacancy range 0-93% (Jinja,
Mbarara: Moroto)• Nurses: -6-60% (Arua, Moroto)• Clinical Officers: -50%-58% (Lira, Hoima)• Anaesthetic Officers: 0-60% (Jinja, Mbarara,
Fort Portal : Hoima)• Orthopaedic officers: 17%-92% (Gulu, Moroto)
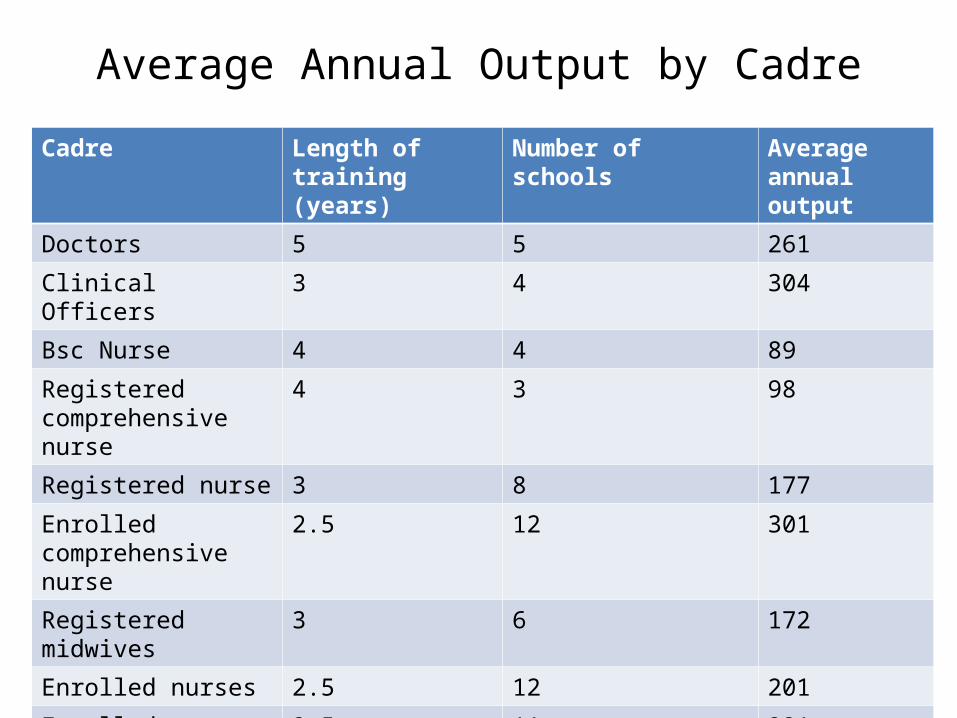
Average Annual Output by Cadre
Cadre Length of training (years)
Number of schools Average annual output
Doctors 5 5 261
Clinical Officers 3 4 304
Bsc Nurse 4 4 89
Registered comprehensive nurse
4 3 98
Registered nurse 3 8 177
Enrolled comprehensive nurse
2.5 12 301
Registered midwives 3 6 172
Enrolled nurses 2.5 12 201
Enrolled Midwives 2.5 11 221
ENT officers 1 1 13
Anaesthetic officers 1 2 8
Discussion
• From the rates seen above, it is obvious that medical personnel are carrying out duties for which they are not fully trained, particularly nursing staff and clinical officers.
• Equipping these cadre of staff with the relevant skills may be a solution to some of the HR problems faced in the health sector.
• BUT they are already overworked ……….
Conclusions• Need innovative solutions. • Task shifting is taking place whether the Ministry of
Health wants to acknowledge it or not.• A multi-sectoral approach is required if task shifting is
to be effected. It requires: – changes in curriculum– changes in policies– changes in salary scales
• The implications of effecting task shifting are not known - need to address this knowledge gap. Otherwise most countries are not eager to tackle the issue.
• Thank you
Ref
• Uganda HSSP II, Ministry of health• Human for health audit report 2010; capacity program




![Brugha Structuring and Weighting Criteria MCDM98mis.ucd.ie/Members/cbrugha/pubs/Brugha Structuring and Weighting... · 13th International Conference on Multiple Criteria ... [MCDA]](https://img.pdfslide.us/doc/110x75/5ae1e8fd7f8b9a495c8b6eb5/brugha-structuring-and-weighting-criteria-structuring-and-weighting13th-international.jpg)











![journal of globaljogh.org/documents/issue201402/Awor FINAL.pdfKangwana et al. 2011 [19] The impact of retail–sector delivery of artemether–lumefantrine on malaria treatment of](https://img.pdfslide.us/doc/110x75/5f2f8bc37a4e2a3c1b2d49e6/journal-of-finalpdf-kangwana-et-al-2011-19-the-impact-of-retailasector-delivery.jpg)












