Embed Size (px)
Citation preview

Postgrad. med. J. (April 1968) 44. 277-285.
Measurement of personality and attitude:applications to clinical research
ISAAC MARKSM.D., D.P.M.
Senior Lecturer, Institute of Psychiatry, Maudsley Hospital, London, S.E.5
CHANGES in personality and attitudes are a salientaspect of many psychiatric disorders. It is there-fore important for psychiatrists to have accuratemeasures of personality functions and relevantattitudes. Over the last 50 years many measuresof personality have been developed, mainly bypsychologists, but until recently few of these hadmuch clinical utility. Most measures in this areawere devised to explore normal personality func-tion, or to test socio-psychological theories, orfor special purposes like vocational guidance. Inthe last few years more attention has been paidto clinical application of these measures so thatinstruments are now emerging which hold pro-mise for psychiatric research, although none ofthese instruments is yet suitable for routine clini-cal work.At first glance there is a daunting array of
measures with strange names and varied theo-retical premises. In fact many of them are con-structed on similar principles and overlapconsiderably. The most important point for aninitiate is whether a particular measure is rele-vant to the clinical issue in question, and if itis, whether that measure is reliable, valid andsensitive to clinical change.The question of relevance is crucial. The term
'personality' denotes the characteristic ways inwhich an individual behaves in a wide varietyof situations. It includes the way in which hegets along with his family, friends and work-mates, his appearance, abilities, motives, and am-bitions, his emotional reactivity, whether he isgenerous or mean, dominant or submissive,energetic or apathetic, hysterical or hypochon-driacal, cheerful or depressed. Furthermore, itincludes his psychiatric complaints. It is clearlyunrealistic to expect any single measure to en-compass all these facets, or to expect all thesefacets to be relevant to a given psychiatric dis-turbance. The clinician has to select thoseaspects which are germane to his clinical in-terests. If he is interested in an individual'sability to get on with his peers he will want a
measure of social adjustment and will not beparticularly interested in measures of creativityor sexual satisfaction.Many personality measures have tried to
reduce the multiple characteristics of personalityinto a few dimensions, but so far none has suc-ceeded. As a noted text commented '[personalityinventories] remain fallible instruments andtheir improvement is one of the pressing tasksfacing psychology' (Hilgard, 1962). If one hasmore limited aims and tries not to encompassthe total personality but to follow a given sectorof personality function instead then certainmeasures become less fallible and indeed havesome clinical use.
Attitude is an aspect of personality, and maybe defined as an orientation and a readiness torespond toward or away from some object, con-cept or situation. Attitudes involve emotional,motivational and intellectual aspects, i.e. atti-tudes involve feelings about an object orsituation, an action tendency toward it and cer-tain beliefs about it. The degree of favourable-ness or unfavourableness of an attitude to anobject is called the valency of that attitude.Attitudes show some consistency in the feelings,beliefs and overt actions called forth by theobject of those attitudes. Knowing an individual'sattitude to a situation will give some clue to theway that individual will behave in the situationconcerned, though there are many variables inaddition to attitude which determine whether ornot an individual will act in a given situation. Inother words, attitude is only one interveningvariable between feeling and overt behaviour.In psychiatric work attitude is best used togetherwith other measures including clinical assess-ment.Enduring attitudes develop through many
learning experiences related to other people. Asattitudes become interwoven with experiencethey develop into abiding personality characteris-tics, so that an individual's attitudes to certainsituations, e.g. religion, are an aspect of his per-
copyright. on A
pril 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.44.510.277 on 1 A
pril 1968. Dow
nloaded from

Isaac Marks
sonality. Measurement of attitude thereforeinvolves measuring a facet of personality.Hundreds of personality measures exist, most
of which are personality inventories and pro-jective techniques. A comprehensive survey isavailable in the Mental Measurements YearBook (Buros, 1965). The principles of psycho-logical test construction are given by Anastasi(1961), and Vernon (1964) supplies a usefulcritique of personality measures. This paper willonly consider those instruments which are incommon use, with illustrations of some clinicalapplications.A brief explanation is necessary of the type
of scale most used in psychological testing, in-cluding measures of personality and attitude.Scales in general can be divided into three types;ratio, interval and ordinal scales.Ratio scales start with a true zero and have
equal intervals between successive units. Anexample of a ratio scale is our measure oflength, where a rod 10 cm in length is twice aslong as another rod 5 cm in length.
Interval scales, on the other hand, have anarbitrary zero though they still have equal in-tervals between successive units. Examples ofthis are our Centigrade and Fahrenheit measuresof temperature. An object at a temperature of60°C is not twice as hot as an object at a tem-perature of 30°C.The third type of scale-ordinal scales-has
neither a true zero nor truly equal intervalsbetween successive units, successive items merelybeing placed in their order of size. Manypsychological tests are of this variety. Anexample would be a measure of 'neuroticism'which simply tells us how 'neurotic' an individualis with regard to a standard population. It hasno true zero and does not allow us to say thatan individual with a score of, say, 40 on a giventest is twice as 'neurotic' as someone with ascore of 20. Furthermore, the interval betweena score of 15 and 20 is not necessarily equivalentto that between 35 and 40.
Personality inventoriesMost personality inventories are self-report
questionnaires or card sorts. In a typical inven-tory the subject answers a list of up to 500 ques-tions with a simple 'yes' or 'no' or 'cannot say'.Alternatively, the questions may be printed oncards, and the patient answers by sorting thecards into the three categories 'yes', 'no' or'cannot say'. Another way would be for thepatient to make a choice between pairs of state-ments, lists of these pairs being printed together
on a sheet of paper or separately on cards, onepair of statements per card.
It is obvious that the utility of a personalityinventory depends in the first place on the state-ments which go to make up that inventory. Theitems in an inventory are usually chosen intui-tively for their relevance to personality or clinicalproblems. After empirical testing the most usefulitems are retained from a large initial pool ofstatements. Many inventories contain similarquestions, e.g. the Taylor Manifest Anxiety Scale(Taylor, 1953) is derived from part of theM.M.P.I. (Hathaway & Meehl, 1951), and theMaudsley and Eysenck Personality Inventories(Eysenck, 1959; Eysenck & Eysenck, 1964), theCornell Medical Index (Brodman et al., 1949)and the Tavistock Self Assessment Inventory(Dixon, de Monchaux & Sandler, 1957a, b)share many items, and in fact the scores forthese questionnaires correlate highly with oneanother (Marks, 1967).
1. The M.M.P.I. (Minnesota Multiphasic Per-sonality Inventory) (Hathaway & Meehl, 1951)is probably the most widely used of all inven-tories, especially in North America. It wasoriginally developed as a clinical instrument tomeasure the characteristic traits of disablingpsychological disorders. It consists of 550 state-ments which have to be answered 'true', 'false'or 'cannot say'. The statements cover many areasfrom physical health to neurological disordersand political and social attitudes. Two examplesof statements are 'I believe I am being plottedagainst' and 'I am worried about sex matters'.The 550 statements fall into ten clinical groups
with labels like 'depression', 'hysteria' and 'para-noid'. There are also four groups of items whichcheck for carelessness, malingering and similarproblems. Each group of items has been workedout empirically on groups of patients diagnosedas depressive, hysteric, paranoid, etc. The scoreson these items are also known for control popu-lations. The test results are plotted as a profilewhich can be compared with that obtained innormal people and with different types ofpatients. It is also possible to see whether theprofile changes after a given treatment (e.g. Brillet al., 1964).The disadvantage of the M.M.P.I. is that it
is quite cumbersome, and that the originalgrouping of items was made intuitively and maynot reflect the most natural groups which occurin practice. Finally, the M.M.P.I. does not assesspersonality function within the normal range ofadjustment.
2. M.P.I (Maudsley Personality Inventory)(Eysenck, 1959; Eysenck & Eysenck, 1964).
278copyright.
on April 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.44.510.277 on 1 April 1968. D
ownloaded from

Measurement of personality and attitude
This is one of the most widely used inven-tories in Britain and has recently been revisedand renamed the E.P.I. (Eysenck PersonalityInventory). There are two alternative forms offorty-eight questions and each question has tobe answered 'yes' or 'no'. These questions werebased on an analysis of 250 questions appearingin other well-known inventories. The forty-eightquestions fall into two groups named extra-version (E) and neuroticism (N) and the resultis reported in terms of an extraversion andneuroticism score. It is claimed that theserepresent fundamental dimensions of personalitybut in fact these two dimensions can be brokendown into further categories depending upon themethod of analysis employed (Eysenck, Hend-rickson & Eysenck, 1968). The usual scores areknown for groups of normal subjects and forpatients with certain abnormalities. The scoresremain reasonably stable from one occasion tothe next and the test is easy to give and score.The M.P.I. has been helpful in following the
changes in some patients. It is dubious, however,whether the N score is more valuable thansimilar instruments like the Cornell MedicalIndex and the Taylor Manifest Anxiety Scalewith which the N score correlates highly, orwhether the E score is more valuable thanother measures of sociability.An example of a study in which the M.P.I.
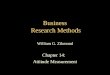
has been useful comes from Levinson & Meyer(1965) who studied the changes in two groupsof neurotic patients after modified leucotomy.Fig. 1 shows the change in scores before andafter leucotomy. After operation the patientsbecame more 'extraverted' (i.e. sociable) and less'neurotic' (i.e. had fewer complaints), and thischange agreed with the overall condition as-sessed clinically. It is noteworthy that the changein the Taylor scale (marked 'Anxiety' (MAS))runs parallel to that in the N score.The M.P.I. has also been useful in showing
how the partners in a marriage come to re-semble one another more as the years go by(Kreitman, 1964), and in studying psychiatricmorbidity in a new town (Hare & Shaw, 1965).
3. Cornell Medical Index (C.M.I.) (Brodman etal., 1949).This instrument is not usually called a per-
sonality inventory but albeit by accident it servesas one and is widely used in psychiatric work.The C.M.I. is a list of 195 questions aboutphysical and mental health which was designedas a rapid scan of patients' complaints beforethey saw a doctor. About half the items (sec-tions A-L) concern physical symptoms, and theother half (sections M-R) deal with psycho-B
logical problems. The total score is a measureof how many complaints the patient has. Thescore on sections M-R correlates highly withneuroticism of the M.P.I. and anxiety of theTaylor scale. The C.M.I. has been useful inidentifying patients with multiple complaints whoare likely to seek medical help and has beenused extensively in epidemiological and clinicalwork (e.g. Shepherd et al., 1966, Ingram, Evans& Oppenheim, 1963; Brown & Fry, 1962; Kreit-man, 1964). Usual scores are available for nor-mal subjects and for groups of patients withdifferent abnormalities. The scores are reason-ably stable from one occasion to the next. Thetest takes no account of the tendency forpatients to show a response set, i.e. to answer'yes' or 'no' repeatedly to any questions regard-less of their content. The questionnaire alsogives no indication about the normal aspects ofa patient's personality.
0 25
W 200
' 15
° 300n
z 25c_a2 20
% 3530u 30.
< 2520
M 15
Extroversion
_Normals
Neuroticism
Normals
1iAnxiety (M.A.S.)
Normals -1 _ ~
Before3 weeks
9 months 5 years
FIG. 1. Effect of leucotomy in 207 patients. Note changein scores of 'extraversion' and 'neuroticism' on theMaudsley Personality Inventory and in scores on theTaylor Manifest Anxiety Scale (based on data ofLevinson& Meyer, 1965).
Other well-known personality inventories in-clude the Edwards Personal Preference Schedule(Edwards, 1953) which appraises motivationaldispositions, and Cattell's 16F (personality fac-
.~~ lr
279copyright.
on April 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.44.510.277 on 1 April 1968. D
ownloaded from

Isaac Marks
tor) Questionnaire (Cattell, 1957, 1965) whichscans sixteen areas of personality function, in-cluding aspects of anxiety.
Comparison of personality and intelligence testsOn the whole, personality inventories have
not fulfilled the earlier promise with which theywere regarded after intelligence tests had provedtheir usefulness in the first decades of this cen-tury. In fact there are major differences be-tween intelligence and personality tests. Intellig-ence tests are tests of ability which seek toascertain an individual's maximum performance.Any single item has a correct answer andpatients usually strive to perform to their bestability. Faking a wrong answer results in anincorrect answer and a lower intelligence score,not a higher one. Faking is not generally aproblem except in those rare instances whereintelligent subjects wish to conceal their ability.In contrast, personality inventories seek thecharacteristic performance rather than a bestone and no single item has an independentcorrect answer. Consistently wrong answers cantherefore result in false negatives and false posi-tives, i.e. normals may simulate disturbance anddisturbed people can conceal their problems andpass as normal.Another difference between intelligence and
personality tests is that intelligence tests haveclearer criteria by which they can be validated.They are tests of ability and results can becompared with scholastic performance. Per-sonality inventories, on the other hand, haveless clear-cut criteria by which they can beevaluated. This is partly because personality ismore complex than intelligence, and partly be-cause we lack external criteria for personalityperformance of the sort we have for intelligencetests in the form of scholastic attainments.
Projective techniquesPatients filling in personality inventories can
only reply according to fixed alternatives. Pro-jective tests were devised to allow the patientto answer more freely by interpreting ambi-guous items such as ink-blots and poorly struc-tured pictures, or by creative activities in fingerpainting and drawing. It is assumed that thepatient's interpretations will reflect his inner feel-ings, and that the freer situation will allow thepatient to project his personality through thetest. The principle employed is that devised byHamlet: 'the play's the thing wherein I'll catchthe conscience of the king'.
Projective techniques are widely employed.One of the best known is the Rorschach inkblot
test in which the patient gives his associationsto a series of complex inkblots. Another com-monly used method is the Thematic Apper-ception Test (TAT) in which the patient tellsstories about a series of pictures which he isshown; the stories tend to form round basicthemes which reflect various aspects of his per-sonality. The Sentence Completion Test is selfexplanatory. For children, structured forms ofdoll-play are used as projective methods.
Projective techniques are an ingenious way toreveal hidden aspects of personality in certaincases. However, projective tests have fulfilledtheir earlier promise even less than personalityinventories because of the difficulty in gettingdependable scores and interpretations. Recentattempts have been made to improve projectivemethods (e.g. Holtzman et al., 1961). Despitesuch efforts Munn (1965) noted that 'until (pro-jective methods) are more standardized, quanti-fied and validated they will be of limited useful-ness in personality research'. In a detailedcritique of projective methods Zubin, Eron &Schumer (1965) came to the same conclusion.Zubin (1967) suggested that more useful infor-mation is obtained from clinical interviewscarried out in a systematic structured manner.
Other measures of personality1. Kelly's Repertory Grid (Kelly, 1955).This is a card-sorting method which allows a
patient to reveal his personality by the way inwhich he judges a number of elements, e.g.people, objects or emotions on a series of con-structs which are usually a pair of contrastingadjectives. Constructs can be either supplied tothe subject or elicited from him. Eliciting isachieved by presenting the patient with threeelements (e.g. three well-known people) and ask-ing the patient to name some way in which twoof the people are alike and thereby differentfrom the third person. The patient might res-pond by saying that two of the people areintelligent but the third is stupid. One wouldthen infer that the construct 'intelligent-stupid'was relevant for the patient in making judge-ments about his world. In this way a series ofconstructs can be elicited and the patient canthen rate each element given to him on theseries of constructs he has produced. One canthen study the patient's ratings of the elementsand constructs, and the relations among them, byspecial statistical analysis. This allows one tomake useful inferences about the patient's wayof viewing his world.The technique is particularly useful when
280copyright.
on April 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.44.510.277 on 1 April 1968. D
ownloaded from

Measurement of personality and attitude
working with an individual patient. It is quitetime-consuming and is rather cumbersome foruse in a group of subjects. It has been usedamongst other things as a measure of transfer-ence (Crisp, 1964), i.e. of the patient's feelingsabout the therapist, and this transference mea-sure has then been related to clinical changesin patients with writer's cramp (Crisp & Mol-dofsky, 1965). The repertory grid method isrelated to another technique which will be dis-cussed below, viz. the semantic differential. Aclear exposition of repertory grid procedure hasbeen given by Bannister (1965) and computerprograms now simplify the analysis of results(Slater, 1965).2. Shapiro's Personal Questionnaire (Shapiro,1961, 1963)This is a card-sorting test which allows a
patient to rate his symptoms repeatedly and re-liably thus allowing detailed study of the changesduring treatment. It is quite time-consuming andso is suitable only for intensive individual casestudies. Fig. 2 shows the change in threesymptoms in one case during two different treat-ments, viz. ECT and leucotomy. Each symptomwas rated on a Personal Questionnaire card sort.The differential effect of the two treatments isobvious. This technique is useful for studyingdetailed changes in individual cases, though itis quite possible that simpler scales would servejust as well.3. Q sort technique (Stephenson, 1953)
This technique is based on a principle similarto that of the repertory grid and semantic dif-ferential, and has to some extent been replacedby them. A review of its status was given byWittenborn (1961). It has been useful for in-dividual case studies in psychotherapy and per-sonality research.
Attitude scalesAttitude scales are constructed on lines similar
to personality inventories except that they mea-sure responses to a more limited variety ofsituations, and tend to be scored in terms offavourableness or unfavourableness. There areseveral types of attitude scale, and a good intro-ductory discussion of these is to be found inKrech, Crutchfield & Ballachey (1962) and Hil-gard (1962).Well-known attitudes scales include the Thur-
stone Scales (Thurstone & Chave, 1929), LikertScales (Likert, 1932), and Guttman's Scalogram(Guttmann, 1950). Thurstone Scales are anassembly of statements concerning a topic someof which are mildly favourable and unfavour-
able, others of which are strongly favourableand unfavourable. These statements can beranked in order of favourableness. Subjects areasked which statements they can endorse andthe attitude score corresponds to the averagescale position of the items he has endorsed.On the Likert Scales a given topic is rated on ascale with the five points 'strongly approve','approve', 'undecided', 'disapprove', 'strongly dis-approve'. Results on Likert scales agree withThurstone scales in discriminating between thosepeople who hold favourable and those who holdunfavourable attitudes to a given issue (Hilgard,1962).
0
cc:
0 3uocnc
0
0cx
l~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~I Anxiety
ECT
4
3
Depression2
ECT- t
'I2 4 6 8 10 12 14 16 2468
Weeks
FIG. 2. Personal Questionnaire Scores before and afterleucotomy in one patient (based on unpublished data ofM. B. Shapiro).
Guttman's Scalogram seeks 'pure' scales alonga single dimension. Items are arranged in a waywhich is increasingly favourable from the firstto the tenth item and if an individual marks, say,item 4 favourably then all items above that willbe rated favourably.
281
4~
I
copyright. on A
pril 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.44.510.277 on 1 A
pril 1968. Dow
nloaded from

Isaac Marks
A host of attitude scales has been constructedto measure attitudes to a great number of situ-ations, for example, ethnic prejudice (Bogardus,1925), masculinity and so on. Many of these areto be found in the Mental Measurements YearBook (Buros, 1965). The value of each measurewill depend partly on its relevance to the pro-blem in hand. A measure of prejudice, forexample, is not of much help in a study of themasculinity of a patient's personality.
Attitude scales have a more limited aim thanmost measures of personality and have beenrather more useful in a clinical setting. Onedrawback which has not been overcome, how-ever, is that sophisticated observers could faketheir replies to produce a spurious picture ifthey wished. In practice this rarely happens butfor this reason attitude scales, like personalitymeasures, should not be used alone in clinicalwork but rather should be used with other evid-ence from clinical sources. Just as in clinicalwork one prefers to make decisions on the basisof consistent evidence from many sources ratherthan on the basis of a single sign or symptom,so too in the use of attitude measures one isconcerned with consistency of response and theway replies tally with other evidence.
Semantic differentialThis is a method which was designed by
Osgood (Osgood, Suci & Tannenbaum, 1957;Osgood, 1962) to measure the meaning of con-cepts in a reliable and scorable fashion. Inrecent years the semantic differential techniquehas also been used increasingly to measure atti-tude and is now the most widely used instrumentin psychiatric work for this purpose. Because ofits utility it deserves detailed description. Theprinciple is simple: patients are asked to rateconcepts on a series of bi-polar seven point ad-jectival scales. A typical form might be asfollows:
Concept to be rated: MY MOTHER Score'pleasant :X: : : unpleasant 2
Bipolar bad : : :Xgood 1adjectival. . . -XgodsdJctale kind * .X: ***cruel 3scales _
i friendlyX : : unfriendly 1Evaluative 'factor' score 7
The scales are arranged so that the same poleof the scale sometimes appears on the left andsometimes on the right hand margin of thepage to avoid the patients developing a responseset. If one wishes the patient to rate twenty con-cepts on nine scales one would prepare a 20-page booklet with a separate concept written at
the top of each page and with the same ninescales appearing below the concept on everypage.Osgood originally found that of all the pos-
sible adjectival scales one could use to measuremeaning most scales fell into three groups or'factors' which he called evaluation (e.g. pleasantunpleasant, good-bad), potency (e.g. strong-weak, powerful-helpless) and activity (e.g. active-passive, fast-slow). Subsequent workers haveshown that only an evaluative factor is usedregularly in judging a wide variety of situationsand that the other two factors are not alwaysemployed. Evaluative scales are used to judgemany situations and in fact give a useful mea-sure of attitude valency, i.e. whether a patientis favourably or unfavourably disposed to agiven situation (Krech et al., 1962).
Semantic differential measures methods haveproved their usefulness in psychiatric work whereattitude is relevant to the research problem.There are many examples of psychiatric appli-cations. In one study group, obsessive-compul-sive and psychopath in-patients could bedifferentiated from one another and from nor-mal subjects by their meanings of concepts like'myself', 'my father' and 'my mother' (Marks,1965, 1966) on evaluative scales. In another study(Marks & Gelder, 1967) changes in sexual de-viance could be followed during treatment bythe patient rating concepts related to his devianceon evaluative scales. Fig. 3 (B and C) shows theway in which a transvestite's attitude to severaldeviant concepts became unfavourable as aver-sion (electric shocks) was given while he woredifferent garments in turn, first brassieres thencorsets and panties. Before this, attitudes hadbeen unchanged after the patient had spent hisfirst 3 days in hospital without shocks (Fig. 3A).Only deviant concepts became unfavourable bythe end of treatment, and other concepts like'my mother' and 'sexual intercourse' remainedfavourable on discharge (Fig. 3D). The selectivechange in attitude was accompanied by selectivediminution in erections, and paralleled clinicalimprovement. When relapse occurred after dis-charge, this clinical change too was mirrored bya change in attitudes, which reverted back totheir original orientation (Fig. 3E).
Fresh scales can be constructed when they arerelevant to the research problem. For examplea series of sex scales (e.g. seductive-repulsive,erotic-frigid) has proved useful when added toevaluative scales for the assessment of progressduring treatment of sexual deviations (Marks &Sartorius, 1968). The semantic differential tech-nique can also be used as a repertory grid with
282copyright.
on April 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.44.510.277 on 1 April 1968. D
ownloaded from

Measurement of personality and attitude
the concepts being the elements and the scalesbeing the constructs in Kelly's terminology (e.g.Marks & Sartorius, 1968).
Provided one is careful to tailor the conceptsand scales to one's research question andchecks are made that the scale-scores clustertogether to form genuine factors then the seman-tic differential is a useful and versatile instru-ment to measure attitudes in psychiatric work.
7
a>0
0
c0
B.- <!! _ u - _~sn c (n - - wzucB.o-C_ cE 0 o E! E u; °,~an ELuX°c °°n i
A B C D E
FIG. 3. Selective attitude change in a transvestite follow-ing selective aversion treatment (taken from Marks &Gelder, 1967). Attitude was measured on evaluativescales of the semantic differential: 1 = good, friendly,approachable; 7 bad, unfriendly, distant. A, 3 days in
hospital without shocks; B, 1 day of shocks to brassieres;C, 2 days of shocks to corsets and panties; D, I I days ofshocks to all garments; E, 5 weeks follow-up, gradualclinical relapse. mot = mother, s.i. = sexual intercourse,cors = corsets, pant = panties, bras = brassieres.
Psychiatric rating scalesFor psychiatrists an important aspect of per-
sonality is a patient's social adjustment and thedegree with which he suffers from a wide varietyof abnormal symptoms. These are usually ob-tained by a detailed clinical interview with thepatient and independent observers. However,interviews are difficult to score, therefore manyrating scales have been developed to ratepatients' symptoms and social adjustment in amanner which allows the results to be treatedstatistically. Among the earlier scales to be usedwere those of Wittenborn (1955) and Miles,Barrabee & Finesinger (1951).Frank et al. (1963) successfully followed the
progress of patients on a Discomfort Scale (Par-loff, Kelman & Frank, 1954; Kelman & Parloff,1957) and the Hildreth Feeling and AttitudeScales (Hildreth, 1946). Gelder & Marks (1966)and Gelder, Marks & Wolff (1967) found themodified scales of Miles et al. (1951) useful inassessing the treatment of phobic patients.Among the most sophisticated clinical scales
are those of Katz and of Lorr. The Katz adjust-ment scales (Katz & Lyerly, 1963) are designed
to assess different aspects of the patient's func-tioning in the community from the points ofview of close relatives and the patient. Separatescales were designed for the relative and for thepatient. The scales involve reports of the patient'ssymptoms, social behaviour, home activities andfree-time activities. The derived scores permitestimates of his adjustment in the clinical, socialand personal areas.On the Lorr scales (Lorr et al., 1962, 1963,
1966) the clinician rates patients in a clinicalinterview on seventy-five scales. These scales fallinto ten groups and ten scores result from therating to produce a ten-element profile. Bystatistical analysis profiles can be divided intomutually exclusive subgroups of similar profilesor types. The scales can be used to classifypatients and to follow their progress in treat-ment. As Zubin (1967) noted, this type of scaleattempts an objective translation of what thegreat descriptive psychiatrists, Kraepelin, Bleulerand Meyer sought to do intuitively. It is stilltoo early to know the limitations of scales suchas those of Katz and of Lorr but they areamong the most interesting clinical scales devisedso far.
Other scales are available to follow more limi-ted aspects of patient function, such as theClyde Mood Scale (Clyde, 1963) which is helpfulin obtaining repeated self-reports in changes ofmood.
ConclusionPersonality and attitude measures have their
uses and facilitate more sophisticated psychiatricresearch than is possible without them. Thesemeasures are an aid to the clinician and in no wayreplace him-they only try to apply clinical judg-ment in a measurable way. As Meehl (1954) con-cluded in an excellent review of this problem,clinical and actuarial methods each have their rolein clinical research.
AppendixSuggestions for further readingFor a general discussion of the value of clini-
cal versus actuarial prediction see Meehl (1954).Detailed appraisal of most psychological tests,with comprehensive references, appears in theSixth Mental Measurements Year Book (Buros,1965). A good introductory discussion of per-sonality and attitude measures is given by Hil-gard (1962). Krech et al. (1962) give a valuablereview of attitude measures. Principles of psycho-logical test construction are detailed by Anastasi(1961), and reviewed by Vernon (1954). Psychi-atric rating scales are well reviewed in Lorr et
283copyright.
on April 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.44.510.277 on 1 April 1968. D
ownloaded from

284 Isaac Marks
al. (1963). An introduction to Kelly's RepertoryGrid is provided by Bannister (1965) and to thesemantic differential by Marks (1965, 1966).
AcknowledgmentsMany thanks are due to Dr M. Crowe, Dr S. Rachman and
Mr A. Mathews for their valuable comments on the manu-script.
ReferencesANASTASI, A (1961) Psychological Testing. MacMillan, New
York.BANNISTER, D (1965) The rationale and clinical relevance of
repertory grid technique. Brit. J. Psychiat. 111, 977.BOGARDUS, E S (1925) Measuring social distance. J. appl.
Sociol. 9, 299 (cited in Krech et al., 1962).BRILL, N.Q., KOEGLER, R.R., EPSTEIN, L.J. & FORGY, E.W.
(1964) Controlled study of psychiatric outpatient treat-ment. Arch. gen. Psychiat. 10, 581.
BRODMAN, K., ERDMANN, A.J., LORGE, I., WOLFF, H.G. &BROADBENT, T.H. (1949) The Corell Medical Index-Anadjunct to medical interview. J. Amer. med. Ass. 140, 530.
BROWN, A.C. & FRY, J. (1962) The Cornell Medical IndexHealth Questionnaire in the identification of neuroticpatients in general practice. J. psychosom. Res. 6, 185.
BuRoS, O.K. (1965) The Sixth Mental Measurements YearBook. Gryphon Press, Highland Park, New Jersey.
CATTELL, R.B. (1957) Sixteen PersonalityFactor Questionnaire(Rev. Ed.). Institute for Personality and Ability Testing,Champaign, Ill.
CATTELL, R.B. (1965) The Scientific Analysis of Personality.Pelican Books No. A712.
CLYDE, D.J. (1963) Manualfor the Clyde Mood Scale. CoralGables, Florida. Biometric Laboratory, University ofMiami.
CRISP, A.H. (1964) An attempt to measure an aspect oftransference. Brit. J. med. Psychol. 37, 17.
CRISP, A.H. & MOLDOFSKY, H. (1965) A psychosomatic studyof writer's cramp. Brit. J. Psychiat. 111, 841.
DENT, J.K. (1966) A Bibliographic Index of Evaluation inMental Health. Public Health Service Publication No.1545. National Institute of Health, Bethesda, Md. 20014.(For sale by Superintendent of Documents, U.S. Govt.Printing Office, Washington, D.C. 20402-60 cents.)
DIXON, J.J., DE MONCHAUX, C. & SANDLER, J. (1957a)Patterns of anxiety: an analysis of social anxieties. Brit. J.med. Psychol. 30, 107.
DIXON, J.J., DE MONCHAUX, C. & SANDLER, J. (1957b)Patterns of anxiety: the phobias. Brit. J. med. Psychol. 30,34.
EDWARDS, A.L. (1953) Manual of Edwards Personal Pre-ference Schedule. The Psychological Corporation, NewYork.
EYSENCK, H.J. (1959) Manual of the Maudsley PersonalityInventory. London.
EYSENCK, H.J. & EYSENCK, S.B.G. (1964) Manual of theEysenck Personality Inventory. London.
EYSENCK, H.J., HENDRICKSON, A.E. & EYSENCK, S.B.G.(1968) A factor analytic study of personality structure.(In press).
FRANK, J.D., NASH, E.H., STONE, A.R. & IMBER, S.D. (1963)Immediate and long-term symptomatic course of psy-chiatric outpatients. Amer. J. Psychiat. 120, 429.
GELDER, M.G. & MARKS, I.M. (1966) Severe agoraphobia: acontrolled prospective trial of behaviour therapy. Brit. J.Psychiat. 112, 309.
GELDER, M.G., MARKS, I.M. & WOLFF, H.H. (1967) De-sensitization and psychotherapy in the treatment of phobicstates: a controlled inquiry. Brit. J. Psychiat. 113, 53.
GUTTMANN, L. (1950) The basis for scalogram analysis.Stouffer, S.A. et al.: Measurement and Prediction, pp.60-90. Princeton University Press. (Cited by Hilgard, 1962.)
HARE, E.H. & SHAW, G.K. (1965) Mental Health on a NewHousing Estate. Maudsley Monograph No. 12. OxfordUniversity Press.
HATHAWAY, S.R. & MEEHL, P.E. (1951) An Atlas for theMinnesota Multiphasic Personality Inventory. OxfordUniversity Press.
HILDRETH, H.M. (1946) A battery of feeling and attitudescales for clinical use. J. clin. Psychol. 2, 214.
HILGARD, E.R. (1962) Introduction to Psychology. Methuen,London.
HOLTZMAN, W.H., THORPE, J.S., SWARTZ, J.D. & HERROW,E.W. (1961) Inkblot Perception and Personality: HoltzmanInkblot Technique. University of Texas Press. (Cited byHilgard, 1962; Vernon, 1964.)
INGRAM, P.W., EVANS, G. & OPPENHEIM, A.N. (1963) Rightillac fossa pain in young women, with appendix on theCornell Medical Index Questionnaire. Brit. med. J. ii, 149.
KATZ, M.M. & LYERLY, S.B. (1963) Methods for measuringadjustment and social behaviour in the community.Psychol. Repts, 13, 503.
KELLY, G.A. (1955) The Psychology of Personal Constructs.Norton, New York.
KELMAN, H.C. & PARLOFF, M.B. (1957). J. abnorm. Soc.Psychol. 54, 281.
KRECH, D., CRUTCHFIELD, R.S. & BALLACHEY, E.L. (1962)Individual in Society. A Textbook of Social Psychology.McGraw-Hill, London.
KREITMAN, N. (1964) The patient's spouse. Brit. J. Psychiat.110, 159.
LEVINSON, F. & MEYER, V. (1965) Personality changes inrelation to psychiatric status following orbital cortexundercutting. Brit. J. Psychiat. 111, 207.
LIKERT, R.A. (1932) A technique for the measurement ofattitudes. Arch. Psychol., N.Y. 28, No. 194 (cited byHilgard, 1962).
LORR, M., KLETT, C.J. & MCNAIR, D.M. (1963) Syndromesof Psychosis. Pergamon Press, London.
LORR, M., KLETT, C.J. & MCNAIR, D.M. (1966) Explorationsin Typing Psychotics. Pergamon Press, London.
LORR, M., MCNAIR, D.M., KLETT, C.J. & LASKY, J.J. (1962)Evidence of 10 psychotic syndromes. J. consult. Psychol.26, 185.
LYERLY, S.B. & ABBOTT, P.S. Handbook ofPsychiatric RatingScales. U.S. Govt. Printing Office, Washington. NIMH,Bethesda, Maryland 20014.
MARKS, I.M. (1965) Patterns of Meaning in PsychiatricPatients. Maudlsey Monograph No. 13. Oxford UniversityPress.
MARKS, I.M. (1966) Semantic differential uses in psychiatricpatients. Brit. J. Psychiat. 112, 945.
MARKS, I.M. (1967) Components and correlates in psychiatricquestionnaires. Brit. J. med. Psychol. 40, 261.
MARKS, I.M. & GELDER, M.G. (1967) Transvestism andfetishism: clinical and psychological changes duringfaradic aversion. Brit. J. Psychiat. 113, 711.
MARKS, I.M. & SARTORIUS, N. (1968) A contribution to themeasurement of sexual attitude: The semantic differentialas a measure of sexual attitude in sexual deviations. J. nerv.ment. Dis. 146. (In press).
MEEHL, P.B. (1954) Clinical versus Statistical Prediction; ATheoretical Analysis and Review of the Evidence. Minne-apolis.
MILES, H., BARRABEE, E. & FINESINGER, J. (1951) Evaluationof psychotherapy: with a follow-up study of 62 cases ofanxiety neurosis. Psychosom. Med. 13, 82.
MUNN, N.L. (1965) The Evolution and Growth of HumanBehaviour, 2nd edn. Harrap, London.
copyright. on A
pril 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.44.510.277 on 1 A
pril 1968. Dow
nloaded from

Measurement of personality and attitude 285
OSGOOD, C.E. (1962) The generality of affective meaningsystems. Amer. Psychologist, 17, 10.
OSGOOD, C.E., Suci, G.J. & TANNENBAUM, P.H. (1957) TheMeasurement of Meaning. Illinois.
PARLOFF, M.B., KELMAN, H.C. & FRANK, J.D. (1954) Com-fort, effectiveness and self-awareness as criteria of improve-ment in psychotherapy. Amer. J. Psychiat. 111, 343.
SHAPIRO, M.B. (1961) A method of measuring psychologicalchanges specific to the individual psychiatric patient. Brit.J. med. Psychol. 34, 151.
SHAPIRO, M.B. (1963) In: Methods ofPsychiatric Research. AnIntroduction for Clinical Psychiatrics (Ed. by P. Sainsburyand N. Kreitman). Oxford University Press, London.
SHEPHERD, M., COOPER, B., BROWN, A.C. & KALTON, G.(1966) Psychiatric Illness in General Practice. OxfordUniversity Press.
SLATER, P. (1965) The use of the repertory grid technique inthe individual case. Brit. J. Psychiat. 111, 965.
STEPHENSON, W. (1953) The Study of Behaviour. University ofChicago Press.
TAYLOR, J.A. (1953) A personality scale of manifest anxiety.J. abnorm. soc. Psychol. 48, 285.
THURSTONE, L.L. & CHAVE, E.J. (1929) The Measurement ofAttitudes. University of Chicago Press. (Cited by Krechet al., 1962; Hilgard, 1962.)
VERNON, P.E. (1964) Personality Assessment: A CriticalSurvey. Methuen, London.
WITTENBORN, J.R. (1955) Wittenborn Psychiatric RatingScales. Psychological Corporation, New York. (Cited byLorr et al., 1963.)
WITTENBORN, J.R. (1961) Contributions and current status ofmethodology. Psychol. Bull. 58, 132.
ZUBIN, J. (1967) Classification of the behaviour disorders.Ann. Rev. Psychol. 18, 389.
ZUBIN, J., ERON, L.D. & SCHUMER, F. (1965) An Experi-mental Approach to Projective Techniques. Wiley, NewYork.
copyright. on A
pril 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.44.510.277 on 1 A
pril 1968. Dow
nloaded from