Embed Size (px)
Citation preview

Meaningful Use: What You Really Need to Know to Earn the
Incentives
Stacey Novogoratz – WHITEC Field Operations Manager

The Wisconsin Health Information Technology Extension Center
(WHITEC)

Objectives
• Provide a high-level background of Meaningful Use (MU ) and the HITECH Act
• Outline the Medicare & Medicaid EHR Incentive Programs
• Provide tips for navigating the MU measures• Discuss Registration & Attestation processes

Background

American Recovery and Reinvestment Act of 2009 (ARRA)
• Signed February 17, 2009 by President Obama
• Established the Health Information Technology for Economic and Clinical Health (HITECH) Act

Regional extension centers
Workforce training
Medicare & Medicaid Incentives and penalties
State grants for health Information exchange
Standards & certificationframework
Privacy & Securityframework
Adoption of EHRs
Meaningful Use of EHRs
Exchange of healthinformation
•Improved individual and population health outcomes•Increased transparency and efficiency•Improved ability to study and improve care delivery
Research to enhance HIT
HITECH Act
Blumenthal D. Launching HITECH. N Engl J Med. 2010 Jan 4.

A Seasonal View of MU...
Snow Meaningful Use of Snow
Andrew McFarlane Melinda Shelton

Meaningful use is…
8
Using certified EHR technology1 to: • Improve quality, safety, efficiency, and reduce
health disparities• Engage patients and families• Improve care coordination, and population
and public health• Maintain privacy and security
Source: http://www.cms.gov/EHRIncentivePrograms/Downloads/MU_Stage1_ReqOverview.pdf
1 Certification as defined by ONC-Authorized Testing and Certification Body (ONC-ATCB). For more information on certified EHRs and the process of certification, visit http://onc-chpl.force.com/ehrcert.

Meaningful Use: Path to better outcomes and quality
Better clinical outcomes Improved population health outcomes Increased transparency and efficiency Empowered individuals More robust research data on health
system

Dr. David Blumenthal, former National Coordinator of HIT, emphasizes:
“HIT is the means, but not the end. Getting an EHR up and running in health care is not the main objective behind the incentives provided by the federal government under ARRA. Improving health is. Promoting health care reform is.”
- At the National HIPAA Summit in Washington, D.C. on September 16, 2009

• Electronically capturing health information in a standardized format
• Using that information to track key clinical conditions• Communicating that information for care coordination
processes• Initiating the reporting of clinical quality measures and
public health information• Using information to engage patients and their families in
their care
11
Stage 1 MU criteria focuses on…
Source: http://www.cms.gov/EHRIncentivePrograms/Downloads/MU_Stage1_ReqOverview.pdf
STAGE 1 STAGE 2 STAGE 3

• More rigorous health information exchange (HIE)• Increased requirements for e-prescribing and
incorporating lab results• Electronic transmission of patient care
summaries across multiple settings• More patient-controlled data
12
Stage 2 MU criteria will focus on…
STAGE 1 STAGE 2 STAGE 3

• Improving quality, safety and efficiency, leading to improved health outcomes
• Decision support for national high priority conditions
• Patient access to self-management tools• Access to comprehensive patient data through
patient-centered HIE• Improving population health
13
Stage 3 MU criteria will focus on…
STAGE 1 STAGE 2 STAGE 3

Medicare and Medicaid EHR Incentive Programs

15
The Centers for Medicare & Medicaid Services (CMS) is making available up to $27 billion in EHR incentive payments, or as much as $44,000 (through Medicare) or $63,750 (through Medicaid) per
eligible professional.

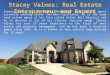
Payment Timeline for EPs
Fall 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021
$18,000 $12,000 $8,000 $4,000 $2,000
$18,000 $12,000 $8,000 $4,000 $2,000
$15,000 $12,000 $8,000 $4,000
$12,000 $8,000 $4,000
$21,250 $8,500 $8,500 $8,500 $8,500 $8,500
$21,250 $8,500 $8,500 $8,500 $8,500 $8,500
$21,250 $8,500 $8,500 $8,500 $8,500 $8,500
$21,250 $8,500 $8,500 $8,500 $8,500 $8,500
$21,250 $8,500 $8,500 $8,500 $8,500 $8,500
$21,250 $8,500 $8,500 $8,500 $8,500 $8,500
Stage 1Stage 2 Stage 3
Medicare Incentive Payments
Medicaid Incentive Payments
$44,000
$44,000
$39,000
$24,000
$63,750
$63,750
$63,750
$63,750
$63,750
$63,750
Maximum Payments
Sources: http://www.cms.gov/EHRIncentivePrograms/60_Medicare_Eligibile_Professional.asphttp://www.cms.gov/EHRIncentivePrograms/65_Medicaid_Eligible_Professional.asp
The sooner professionals start successfully demonstrating meaningful use, the sooner they will maximize their EHR incentive payments.

17
Medicare EHR Incentive Program Medicaid EHR Incentive Program
Year 1 options Must be a meaningful user in Year 1
Adopt/Implement/Upgrade option in Year 1
Who is eligible? 5 types of EPs, subsection (d) hospitals and CAHs
5 types of EPs, acute care hospitals (including CAHs) and children’s hospitals
Important dates Last year to start is 2014Last payment is in 2016
Last year to start is 2016Last payment is in 2021
Fee schedule reductions Begin in 2015 for EPs that are not meaningful users
None
Meaningful use definition MU definition will be common for Medicare
States can adopt a more rigorous definition (based on common one)
Who will implement? Federal government (will be an option nationally)
Voluntary for states to implement
Sources: http://www.cms.gov/EHRIncentivePrograms/Downloads/MU_Stage1_ReqOverview.pdf
Overview of Medicare and Medicaid EHR Incentive Programs

Medicare-only Eligible Professionals
Could be eligible for both Medicare &
Medicaid incentives
Medicaid-only Eligible Professionals
Eligibility

19
Comparing Medicare and Medicaid EHR Incentive Programs for EPs
Source: http://www.cms.gov/EHRIncentivePrograms/Downloads/MU_Stage1_ReqOverview.pdf
Medicare EHR IncentivePayments
Medicaid EHR Incentive Payments
• Maximum incentives are $44,000 over 5 consecutive years
• Incentive payments decrease if starting after 2012
• Incentive payments based on Fee-for-Service allowable charges
• Must begin by 2014 to receive incentive payments; last payment year is 2016
• Extra amount available for EPs practicing in predominantly Health Professional Shortage Areas
• Maximum incentives are $63,750 over 6 years (do not need to be consecutive)
• The first year payment is $21,250; $8,500 for next 5 years
• Must begin by 2016 to receive incentive payments; last payment year is 2021

EP Eligibility: Medicaid • Must be one of 5 types of EPs• Must either:
– Have ≥ 30% Medicaid patient volume (≥ 20% for pediatricians only); or
– Practice predominantly in an FQHC or RHC with ≥30% needy individual patient volume
• Licensed, credentialed• No OIG exclusions, living• Must not be hospital-based

Other Eligibility Considerations
• An EP who works at multiple locations, but does not have certified EHR technology available at all of them:– Must have 50% of total patient encounters at location(s)
where certified EHR technology is available– Must base all MU measures only on encounters that
occurred at those locations• An EP cannot be hospital-based
– 90% of services performed in Place of Service (POS) 21 (Inpatient) or 23 (Emergency Dept)

Other Eligibility Considerations – cont’d
• An EP may switch programs once after receipt of an incentive payment, but must do so before 2014
• An EP who practices in multiple states and qualifies for Medicaid incentives must choose one state from which to receive payment

Medicare Penalties– An EP who does not demonstrate MU by
2015 will be subject to payment reductions in their Medicare reimbursement schedule
• Medicaid-only EPs are not subject to payment reductions
• Payment reductions may apply for any EP who accepts Medicare, even if you only participate in the Medicaid EHR incentive program
– Payment reductions start at 1%, increasing a percentage each year, to a maximum of 5%

Meaningful Use

MU criteria for Eligible Professionals• 15 core objectives
• 5 objectives out of 10 from menu set– Including one public health measure
• 6 total Clinical Quality Measures – 3 core or alternate core– 3 out of 38 from additional set
25Source: http://www.cms.gov/EHRIncentivePrograms/Downloads/MU_Stage1_ReqOverview.pdf
STAGE 1 STAGE 2 STAGE 3

26
Use CPOE e-Prescribing Drug-drug & drug allergy
checks Medication list Allergy list Problem list Decision support Record demographics
Source: http://www.cms.gov/EHRIncentivePrograms/Downloads/MU_Stage1_ReqOverview.pdf
Core Set: Must Do All 15
Smoking status Vital signs Clinical summaries to
patient Electronic exchange Health info to patients Clinical quality measures Protect health information
Stage 1 Objectives for EPs

Incorporate clinical labs Medication reconciliation Implement drug-
formulary checks Generate patient list Patient electronic access Send reminder Patient-specific
education
Stage 1 Objectives for EPsMenu Set: Must do 5 of 10
Clinical summaries to provider
Submit electronic data to immunization registry*
Submit electronic syndromic surveillance data*
*At least 1 public health objective must be selected.
Source: http://www.cms.gov/EHRIncentivePrograms/Downloads/MU_Stage1_ReqOverview.pdf

Clinical Quality MeasuresCore Set: Must Do 3
NQF Measure Number & PQRI Implementation Number
Clinical Quality Measure Title
NQF 0013 Hypertension: Blood Pressure Measurement
NQF 0028 Preventive Care and Screening Measure Pair: a) Tobacco Use Assessment, b) Tobacco Cessation Intervention
NQF 0421PQRI 128
Adult Weight Screening and Follow-up

Clinical Quality MeasuresAlternate Core Set: Can choose from if Core Set measures do not apply
NQF Measure Number & PQRI Implementation Number
Clinical Quality Measure Title
NQF 0024 Weight Assessment and Counseling for Children and Adolescents
NQF 0041PQRI 110
Preventive Care and Screening: Influenza Immunization for Patients 50 Years Old or Older
NQF 0038 Childhood Immunization Status

Reporting Clinical Quality Measures to Medicare2011 Submit aggregate CQM numerator,
denominator, and exclusion data to CMS or the States by ATTESTATION.
2012 Required to electronically submit aggregate CQM numerator, denominator, and exclusion data to CMS or the States.
• Electronic submission of CQM reports for Medicaid not required until 2013

Applicability of MU objectives & measures
31
• Not all MU objectives are applicable to every practice– For example, Chiropractors don’t e-prescribe;
Dentists don’t immunize• EPs who qualify for the Medicare and Medicaid EHR
Incentive Programs would be excluded from having to meet non-applicable measures– Must attest a zero denominator for that objective– Exclusions do not count against the 5 deferred
measures
Source: http://www.cms.gov/EHRIncentivePrograms/Downloads/MU_Stage1_ReqOverview.pdf

Tips for navigating the MU measures
• Understand your vendor’s certification– Reports are dependent on data in certain fields
• Could require some workflow changes– You must have the ability to acquire all components of
the Complete EHR• Even if you are not selecting a certain menu set measure
(e.g. patient portal), you need to at least have the ability to acquire the functionality
• Remember that measures for EPs are based on individual providers– Consider how to handle different gaps for different
providers– Develop communication strategy and process for
tracking

Tips for navigating the MU measures
• Objectives that are attestation only (Yes / No):1. Implement drug-drug & drug-allergy interaction checks2. Report ambulatory clinical quality measures 3. Implement one clinical decision support rule4. Capability to exchange key clinical information5. Protect electronic health information 6. Implement drug formulary checks7. Generate lists of patients by specific conditions 8. Capability to submit electronic data to immunization registries9. Capability to submit electronic syndromic surveillance data to
public health agencies

Tips for navigating the MU measures
• Objectives that have NO exclusions:1. Implement drug-drug & drug-allergy interaction checks2. Maintain an up-to-date problem list 3. Maintain active medication list4. Record demographics5. Report ambulatory clinical quality measures 6. Implement one clinical decision support rule7. Capability to exchange key clinical information8. Protect electronic health information 9. Generate lists of patients by specific conditions10.Use certified EHR technology to identify patient-specific
education resources

Tips for navigating the MU measures
• Core Measure 3 – Maintain Problem List– Must be stored as structured data
• ICD-9 and SNOMED-CT® are the standard
– Based on unique patients• One patient seen multiple times only counts once in the
denominator• Problem list doesn’t necessarily need to be updated every time
– An indication that there are no problems is acceptable

Tips for navigating the MU measures• Core Measure 4 – e-Prescribing (eRx)
– Number of prescriptions written for drugs requiring a prescription in order to be dispensed other than controlled substances during the EHR reporting period.
• Does not include authorizations for other items or services (e.g. durable medical equipment
• If a patient requests a paper prescription, this cannot be excluded from the denominator
– EPs cannot receive incentive payments from the Medicare Improvements for Patients and Providers Act of 2008 (MIPPA) and the Medicare EHR Incentive Program for the same year
• EPs can receive MIPPA and Medicaid EHR Incentive payments in the same year

Tips for navigating the MU measures• Core Measure 10 – Clinical Quality Measures
(CQMs)– EPs may submit results for CQMs that were not certified
by the vendor– CQM reports must be generated by certified technology
• If pulling from a data warehouse, the data warehouse may need to be certified
– Denominators of zero are acceptable, however...• If zero for a core measure denominator, the EP must report on an
alternate core measure, up to three• Even if all 6 core measures have zero denominators, the EP must
still report on 3 of the 38 additional measures– The three additional measures can’t be from the alternate
core set

Tips for navigating the MU measures
• Core Measure 14 - Electronic Exchange of Clinical Information – The use of physical media (e.g. USB, CD) does not meet
the measure– Exchange must be with a different legal entity not sharing
a common database– Options to test exchange may include:
• Vendor-specific functionality• Direct through the Wisconsin Statewide Health Information
Network (WISHIN)• Other Health Information Service Providers (HISPs)

Registration and Attestation

Medicare & Medicaid EHR Incentive Program Registration and
Attestation Systemhttps://ehrincentives.cms.gov/hitech/login.action
• Start here for both programs– Medicare: Complete both registration & attestation
through this site– Medicaid: Register through this site, then complete
application through ForwardHealth Portal

Registration – What you need for EPs
• Logging in:– National Provider Identifier (NPI)– National Plan and Provider Enumeration System (NPPES) User
ID and Password
• Choosing a program:– You must know whether you are applying for the Medicare or
Medicaid EHR Incentive Program
• Reassigning payments:– Payee Tax Identification Number (if you are reassigning your
benefits). – Payee National Provider Identifier (NPI) (if you are reassigning
your benefits).

Registering or attesting on behalf of an EP• You must have an active Identity and
Access Management System (I&A) web user account – Must be associated with the EP’s NPI
(requires EP’s approval)

Attestation – What you need for Medicare EPs
• EHR certification number • Dates of 90-day reporting period• Numerators & denominators for applicable
measures – Ex: Clinical summaries provided to patients for more
than 50% of all office visits within 3 business days• Good idea to print the summary page at the end
of successful attestation – You will not receive an e-mail confirmation

Applying for the WI Medicaid EHR Incentive Program
• Begin at CMS site – select Medicaid– Must wait 2 full business days before proceeding to application
for WI program
• ForwardHealth Portal account is required– Portal Administrators will automatically have access to the
Wisconsin Medicaid EHR Incentive Program application
• Will need patient volume data for 90-day reporting period– For EPs using the eligible member patient volume, a standard
deduction of 8.08% is applied to account for CHIP encounters

Adopt/Implement/Upgrade (AIU) for Medicaid EPs• Adopt = demonstrate acquisition, installation, or
contractual proof of a future acquisition of certified EHR technology
• Implement = meet the criteria for adopting certified EHR technology and demonstrate actual implementation, installation, or utilization of certified EHR technology
• Upgrade = meet the criteria for adopting and implementing and demonstrate expansion of the certified EHR technology’s functionality such as the addition of an e-prescribing functionality or Computerized Physician Order Entry.

Documentation of AIU• Adoption
– Receipt(s) for certified EHR technology – Contract for certified EHR technology
• Implementation– One from each List
• List One: Receipt(s), Contract• List Two: Maintenance agreement, Installation contract or receipt(s),
system logs, Evidence of cost, contract, or third party certification of certified EHR technology training
• Upgrade– Receipt(s)– Executed contract
*Additional documentation may be considered but must, at a minimum, identify the certified EHR technology adopted, implemented or upgraded and indicate the certified EHR technology acquired or purchased.

Certified Health IT Product List (CHPL) http://healthit.hhs.gov/chpl
• For EPs, select Ambulatory Practice Type• Search to find the product you use• Add product(s) to your cart until your product(s) meet 100% of the
CMS required criteria• Request a CMS EHR Certification ID for CMS attestation
– ID contains 15 alphanumeric characters – Is NOT the same as the CHPL Product Number– Only need to get this once if attesting for multiple EPs who use the
same system• You must have a complete EHR, even if not attesting to menu
set measures that may require additional modules

Incentive Payments
• Medicare– EPs will receive full $18K (2011 & 2012) once they
have $24K in allowed Part B charges for a calendar year
• This is tracked by Medicare
• Medicaid– Payments reassigned to an organization will be sent
through an electronic funds transfer (EFT) – EPs receiving payments themselves are encouraged
to set up an ETF, however, can receive paper checks

Other Resources
• CMS EHR Incentive Programs – www.cms.gov/EHRIncentivePrograms
• Office of the National Coordinator for Health IT – www.healthit.hhs.gov
• WI DHS – Medicaid EHR Incentive Program – www.dhs.wisconsin.gov/ehrincentive
• WHITEC – www.whitec.org • WISHIN – www.wishin.org

Contact Information
• Stacey Novogoratz, WHITEC Field Operations Manager– [email protected]– (608) 729-2703

WHITEC, operated as a division of MetaStar, is funded through a cooperative agreement award from the Office of the National Coordinator, Department of Health and Human Services Award No. 90RC0011/01
Questions?