Embed Size (px)
Citation preview
Meaningful Use Audits
Focus on Success
Jim TateAugust 10, 2016
1

Presenter
Jim Tate is recognized as the most experienced authority on the CMS EHR Incentive Programs. Jim is the President of EMR Advocate, Inc., Partner at Answers Media Company, and Partner at OneRecord.
He has worked with over 200 EHR vendors on their certification projects, authored the first step-by-step manual on meaningful use: The Incentive Roadmap, and served as a Subject Matter Expert to the federally funded Regional Extension Centers for the adoption and implementation of electronic health records. Jim and his team have provided expertise and leadership in over 250 meaningful use audits.
www.meaningfuluseaudits.com
Jim Tate
2
History
CMS, and its contractors, will perform audits on Medicare and dually-eligible Medicare/ Medicaid providers
States, and their contractors, will perform audits on Medicaid providers
CMS and states will also manage appeals processes
3
Audit Basics
Achieve, Document, Attest to MU
Medicare vs. Medicaid incentive programs
Audit based on individual attestation
Subject of audit is the EP, not the practice
All or nothing
Pre- and Post-payment audits
4
Audit Basics (Pt.2)
Audits up to 6 years post attestation
CMS states the aim is to audit 5%+
EPs failure rate 20% - 25%
#1 cause of failure: Security Risk Analysis
5
Audit Basics (Pt.3)
Medicare or Medicaid Incentive Program?
Could switch once during MU participation (not after 2015)
Medicaid – audits and appeal at State level
Medicare – CMS contractor: Figliozzi & Co.
Active auditing against 2011/2015 attestations
6
What Brings an Audit?
Random
Suspicious data
Patterns
Reach back, reach forward, reach sideways
Risk profile
7
The Audit Process
Letter of engagement via email
Request for documentation with deadline
Extension opportunity
Submission via portal
Auditor requests additional documentation and/or clarification and sets new deadline
Final determination
8
Letter of Engagement
“This letter is to inform you that you have been selected by CMS for an audit of your meaningful use of certified EHR technology for the attestation period. Attached to this letter is an information request list. Be aware that this list may not be all-inclusive and that we may request additional information necessary to complete the audit.”
9
10
Audit Final Decision - Good
“We performed a review of your meaningful use attestation for the Program Year 2011 and Payment Year 1. Based on our review of the supporting documentation furnished by you, we have determined that you have met the meaningful use criteria.”
11
Audit Final Decision – Bad“We performed a review of your meaningful use attestation for the Program Year 2011 and Payment Year 1. Based on our review of the supporting documentation furnished by you, we have determined that you have not met the meaningful use criteria, for the following reasons: - Failed Eligible Professional Meaningful Use Core Measure 15 -Protect Electronic Health Information”
“Since you did not meet the meaningful use criteria, the incentive payment will be recouped. You will receive a demand letter for your total Medicare EHR incentive payment shortly from the EHR HITECH Incentive Payment Center. The demand letter will include all information regarding the repayment process. You have the option to appeal this decision and in order to start the appeal process, you must submit the appropriate appeals filing form found at: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Appeals.html”
“Failure to submit the appeal form within 30 days from the date of this letter will forfeit your option to appeal. Please also note that this audit does not preclude you from future, prior or subsequent year audits.”
12
Audit Response Best Practices
Maintain all attestation related material in a secure location for a minimum of 6 years past attestation
During an audit have one point of contact to communicate with the auditor
Ask the auditor if you need any clarification on their expectations
Adhere to all deadlines
Request additional time to supply information if necessary before any deadline
Enlist your EHR vendor as a source for resources and documentation
Only provide what is specifically requested
13
The Appeal Process
“If you have been denied an EHR incentive payment, have been determined to be ineligible for the program, or have received an audit decision that you believe to be in error, you can appeal the decision. Medicare eligible professionals (EPs) should file appeals with CMS, while Medicaid eligible professionals should contact their State Medicaid Agency for information about filing an appeal.”
14
The Appeal Process (Pt.2)
“In order to begin the appeals process EPs, hospitals, or CAHs must complete the appropriate filing request below. It is important to follow the instructions specific to your appeal type on the filing request. Please note that the appeals submission process is time sensitive with a 30 day window for submission period. The filing request and supporting documentation must be submitted electronically to [email protected]. The appeal will only be processed if all documentation is provided at the time of submission.”
15
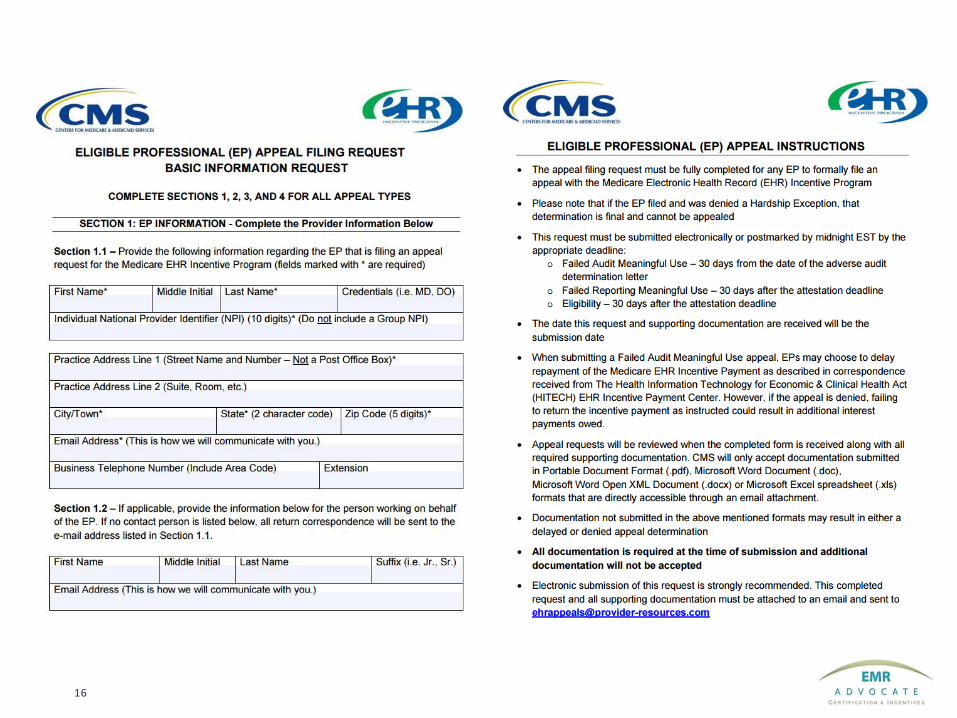
16
Appeal Final Decision - Good
“Based on our review of your Appeal Filing Request, supporting documentation and the Program policies, we have accepted the documentation you provided to support your appeal. Therefore, CMS upholds your appeal.”
17
Appeal Final Decision - Bad
“Based on our review of your Appeal Filing Request, supporting documentation and the Program policies, we have denied the documentation you provided to support your appeal. Therefore, CMS denies your appeal.”
“Any repayment letters sent as a result of an unfavorable audit or appeal are sent to you via a separate process. If the result of this appeal changes that status, please allow six to eight weeks for this processing to occur. Again, the repayment process is a separate process handled by another office.”
“This decision is final and further appeal and inquiry options are not available.”
18
Building the Book of Evidence
Attestation Report
Proof of CEHRT
Patients - Locations
Security Risk Analysis
Percentage Based Measures
Non-percentage Based Measures
Exclusions
Medicaid specific
19
Proof of CEHRT
“As proof of use of a Certified Electronic Health Record Technology system, provide a copy of your licensing agreement with the vendor or invoices.”
“Please ensure that the licensing agreements or invoices identify the vendor, product name, and product version number of the Certified Electronic Health Record Technology system utilized during your attestation period.”
“If the version number is not present on the invoice/contract, please supply a letter from your vendor attesting to the version number used during your attestation period.”
20
Security Risk Analysis
Objective: “Protect electronic health information created or maintained by the certified EHR technology through the implementation of appropriate technical capabilities.”
Measure: “Conduct or review a security risk analysis in accordance with the requirements under 45 CFR 164.308(a)(1) and implement security updates as necessary and correct identified security deficiencies as part of its risk management process.”
21
Medicaid Specific
The Medicaid patient volume calculation method is designated by the State Medicaid Agency and approved by the CMS. In general, patient volume is calculated by dividing the provider’s encounters with Medicaid-enrolled patients over the provider’s total number of service encounters.
Patient volume documentation: “To be eligible to participate in the Medicaid EHR Incentive Program, an EP must either:
• Meet certain Medicaid patient volume thresholds; or
• Practice predominantly in an FQHS or RHC where 30 percent of the patient volume is derived from need individuals.
Note: One exception to this rule is that a pediatrician may have at least 20 percent Medicaid patient volume and still quality but at a reduced incentive.
22
Medicaid Specific (cont.)
• An EP has the option to “leverage a clinic or group practice’s patient volume as a proxy” for their own individual volume calculations. Details at CMS FAQ: https://questions.cms.gov/faq.php?id=5005&faqId=2993
23
MACRA/MIPS – The Future of Audits
• What we know now
• Potential audits
• Effect of audits
24
Meaningful Use AuditsFocus on Success
Q & A
Jim Tate
25