Embed Size (px)
DESCRIPTION
MDCT COMPLEMENTARY TO CORONARY ANGIOGRAPHY. Radiology departement La rabta hospital. INTRODUCTION. - PowerPoint PPT Presentation
Citation preview

MDCT COMPLEMENTARY TO CORONARY ANGIOGRAPHY
Radiology departement
La rabta hospital

INTRODUCTION• The possibility to perform cardiac and coronary imaging was a major
driving force behind an ongoing, rapid evolution of scanner technology,
accompanied by improvements of software and post-processing tools.
• The most recent generations of MDCT with the ability to acquire 64 slices
simultaneously allow relatively robust morphological and functional
imaging of the heart.
• Although initially, clinical applications were restricted to the detection of
coronary calcium, visualization of the coronary artery lumen (non-invasive
coronary angiography) has now become the major focus of cardiac MDCT.

PATIENTS AND METHODS• Analytical descriptive and prospective study about
37 patients who subsequently received a computed tomographic
coronary angiography in addition to exploration with coronary
angiography when it could not be formally conclusive.
=> The results and limitations of MDCT were evaluated according to
different clinical and anatomical situations.
• Patients explored with usual MDCT coronary angiography technique.
• Use of beta blockers when heart rate above 65 b / min

RESULTS1. DEMOGRAPHIC AND CLINICAL DATA:
• The average age of our patients was 60,1 years, from to years.
• There were women and men with sex ratio 2.7/1.
INDICATIONS OF CORONARY ANGIOGRAPHY:
• Coronary angiography was performed after an acute coronary syndrome or
chest pain 91% of cases.
• 2 patients were admitted to investigate a dilated cardiomyopathy (n =2).
• One patient was admitted for congestive heart failure revealing an aortic
coarctation associated with an atrial septal defect
MDCT INDICATIONS:
• Further study of congenital anomalies of the coronary arteries (n=7).
• Not visualized coronary artery bypass grafts (n=11).
• Exploration of ostial coronary lesions (n = 14).
• Not catheterized coronary (n = 2).

2. STUDY OF CONGENITAL ANOMALIES OF THE CORONARY
ARTERIES
• 7 patients.
• Indications were:
• Further study of the origin or path of an abnormal origin
of a coronary artery from the contralateral sinus of
Valsalva side.(n=)
• Suspicion of a single coronary artery(n=)
• Exploration of a coronary – pulmonary fistula (n=)

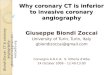
IVA arising from right anterior sinus. incidence in cranial and anterior right oblique, note the recovery of right coronary system
Coronary angiography:ooccluded right coronary artery from its origin back through the network contralateral side.oleft anterior descending arising from right anterior sinus.
The data of coronary angiography could not formally identify the pre, retro or inter aorto pulmonary course
• 48 years old man • Having already received a right coronary stenting.• Currently admitted for a recurrence of chest pain on optimal medical
therapy.
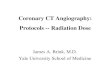
Case 1

3D MDCT reconstructions (left), volume rendering mode and 2D curvilinear (right): The IVA artery arises from the segment I of the right coronary artery, describing a inter aorto-pulmonary course before being in the inter-ventricular furrow.
The patient underwent a multidetector CT which confirmed the presence of an abnormal origin of the left anterior artery arising from the right coronary artery, with inter aortopulmonary course.

Case 2
Coronary angiography: left profile, right coronary dominant giving PDA which seems to extend through an LAD
• Female, 55 years old, diabetic, hypertensive and obese.• Admitted to explore a dilated cardiomyopathy.Coronary angiography failed to opacify the left coronary system, but described a large dominant right coronary artery with a posterior descending artery giving back into a semblance left anterior descending.

Reconstruction 3D Volume rendering: Lack of individualization of a left coronary artery, the coronary system can be summarized in a single large right coronary artery.
The MDCT revealed: The right coronary artery gives an PDA repeating in part the territory of the LADReverse left ventricular territory includes part of the marginal=> Confirming the fact whether a single coronary artery

Case 3
Coronary angiography: catheterization of the left coronary shows the arising of a vessel from the common core that seems to irrigate an undetermined structure.
• Man aged 32, Type I diabetic, and hypothyroid,• Admitted for exploration of dilated cardiomyopathy.
Coronary angiography:o has not objectified atheromatous lesion.oaffirmed the existence of an artery emerging from a common core with undetermined irrigation

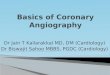
MDCT in axial and sagittal reconstruction. The vessel described above comes into contact with the anterior trunk of the left pulmonary artery with evidence of passage of contrast in the pulmonary artery, confirming coronary pulmonary fistula
• The CT scan examination was performed with biphasic injection of contrast whose goal is to get on the acquisition of a significant enhancement in the left cavities contrasting with little opacified right cavities.
• This biphasic injection helped to reveal the coronary pulmonary fistula.

3. CORONARY ARTERY BYPASS GRAFTS:
• 11 coronary patients, having already undergone coronary artery bypass
grafting
• 10 men and one woman.
• Average age of 63.5 years
• These patients accounted for 26 bridges to analyze which types were:
o Saphenous vein grafts in 14 cases
o Internal mammary graft in 10 cases
o Radial graft in 2 cases.
• The anastomoses were on:
o LAD in 9 cases
o the marginal artery in 9 cases
o the diagonal artery in 4 cases
o the right coronary artery in 6 cases

CORONAY ANGIOGRAPHY DATA:
• 6 of 10 internal mammary grafts were patent, four were not
opacified.
• 6 of 15 venous grafts were patent, the grafts were not opacified in
eight cases, one was thrombosed.
• The two radial graftss were not opacified.
MDCT DATA:
• All not opacified grafts were studied on CT :
• the four non-opacified internal mammary grafts:
o 2 were patent.
o one was thrombosed.
o One was analyzed only in part, the distal anastomosis could not be
studied because of the occurrence of tachycardia.

the 8 non-opacified venous grafts:
o 5 were thrombosed
o two were patent
o one was the site of a distal anastomotic stricture
o The two radial graftss were occluded.
• For segments opacified by both methods, the
findings of the scanner were identical to those of
coronary angiography.
• Functional grafts studied with coronary
angiography were also permeable on CT.

coronary angiography: Graft ISV/2 nd diagonal permeable and of good size ISV / 1 st lateral permeable good caliber The bypass LIMA / LAD was impossible to opacify.
• Man, 63 years old, smoking and diabetes• Background:• double angioplasty of the circumflex and right coronary six years earlier• then triple coronary artery bypass grafting LAD/LIMA Second-diagonal /ISV First-Side / ISV• This patient was admitted for treatment of chest pain
Case 4

• Coronary Computed tomography described
• A graft on the left internal mammary /LAD
permeable.
• The analysis of the rest of the thoracic led
to the discovery of a highly suspicious apical
left mass without associated signs of
mediastinal extension.

4. EXPLORATION OF OSTIAL CORONARY LESIONS :
• 14 patients with mean age of 57.75 years (41-74 years).
• / patients were investigated after a confirmed acute coronary syndrom
or suspected chest pain.
• X patient has been explored in the context of dilated cardiomyopathy.
• The ostial lesions:
o Lesions of the left main trunk (n = )
o Ostial lesion of the right coronary (n = )
o Ostial stenosis of the LAD
• Computed tomography coronary helped give a useful answer to the
diagnostic management and / or therapeutic clinical situations in /14

• The ostial lesions:
o Lesions of the left main trunk (n = )
o Ostial lesion of the right coronary (n = )
o Ostial stenosis of the LAD
• Computed tomography coronary helped give a
useful answer to the diagnostic management and /
or therapeutic clinical situations in /14

Case 5
caudal LAO coronary incidence. : Ostial stenosis of the left coronary artery, difficult to quantify
• Male 65 years old, smoking hypertension, diabetes• Admitted for acute coronary syndromes without ST segment above.• The ECG and ultrasound trans chest were unremarkable.Coronary angiography was suspected without affirming, ostial stenosis of the left coronary artery.The LAD was infiltrated without significant stenosis and right coronary artery was small and dominated.

MDCT-Reconstruction curvilinear and cross section for measuring the flatness of the core and confirming the closeness of the stenosis. Stenosis hypodense non-calcified plaque.
• Computed tomography of the coronary arteries showed: the presence of a hypodense ostial plaque in left coronary trunk responsible for stenosis with a minimum area of 3.6 mm2 to planimetry.This patient underwent a double bypass of the LAD by the left internal mammary artery and lateral saphenous vein.

Case 6
Coronary angiography: left anterior oblique Incidence showing a calcified ostial stenosis of the right coronary artery
• Patient aged 59 years, smoking• Admitted for acute coronary syndrome.
Coronary angiography has described a right coronary ostial calcified stenosis whose severity is poorly quantified, the rest of the tree was healthy.

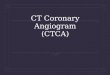
Coronary MDCT: 3D MIP and curvilinear reconstruction of the right coronary artery: partially calcified ostial plaque responsible for a sub-occlusive stenosis
The MDCT confirmed the presence of a large eccentric calcified plaque in right coronary ostial responsible for a severe stenosis.

5. NOT CATHETERIZED CORONARY :
• 60 years old female patient, hypertensive since 30 years.
• Admitted for congestive heart failure revealing a tight aortic
coarctation associated with atrial septal defect (veinosus
sinus).
• Preoperative coronary angiography through the radial
approach could not be achieved, for failure to advance the
probe of the ascending aorta due to a strong collaterally with
tortuosity of the brachiocephalic trunk.
• The MDCTA :
o confirmed coarctation of the aorta.
o studied the collateral circulation.
o studied the coronary system which was free of lesions.

CT angiography: sagittal reconstruction : isthmic coarctation of the aorta

DISCUSSION• Recent technological developments have enabled the
cardiac CT to fit into the diagnostic of coronary disease.
• Coronary angiography remains the standard protocol in
acute coronary syndromes with electrical and / or
enzymatic modifications, and symptomatic patients with
high likelihood of coronary disease.
• The detection of coronary artery disease is the main
indication of cardiac CT retained due to its negative
predictive value close to 100%

ADVANTAGES AND LIMITATION OF MDCT
ADVANTAGES:
• The introduction of multi-detector row computed tomography
(MDCT) led to a significant improvement in the temporal and
spatial resolution of CT, which permitted substantial expansion of
potential indications for CT imaging. Small and rapidly moving
anatomic structures could be visualized with good image quality.
• Coronary CT angiography investigation allows for the accurate
detection of coronary artery stenoses. Especially, the negative
predictive value has uniformly been found to be high, indicating
that the technique may be most suitable as a non-invasive tool
to rule out the presence of obstructive coronary lesions.

• 3D imaging provides a real coronary mapping mode using the
3D volume rendering and MIP.
• CT allows by the measurement of density, to distinguish plaques
with high lipid component called vulnerable, with high risk of
erosion.
• Besides the detection of coronary stenoses, cardiac CT has the
potential to visualize earlier stages of coronary atherosclerosis
• Besides the assessment of the coronary arteries, CT provides for
accurate assessment of general cardiac morphology.
• This can be particularly useful in the context of electrophysiology
when detailed anatomic information (e.g. the pulmonary veins
and left atrium prior to ablation procedures or coronary veins in
CRT for left ventricular lead placement) is needed.

• Similarly, CT imaging can be useful in patients
with congenital heart disease or other structural
cardiac disease.
• Exploration concomitant lung parenchyma;
according to Haller, 5% of coronary CT
examinations are an opportunity to discover an
extracardiac disease (lung cancer, pulmonary
embolism, benign mass, pneumonia)

LIMITATIONS:
• Several situations currently pose challenges for reliable CT imaging
these include
• The patient should be cooperative , able to do a few seconds apnea,
to withstand the supine position for ten minutes, arms above the
head
• patients with arrhythmias,
• patients with advanced CAD and pronounced coronary calcifications,
• and patients with coronary artery stents, which are often difficult to
evaluate. Similarly, although CABGs can be assessed with very high
diagnostic accuracy, detection of stenoses at the site of anastomosis
and in the native coronary arteries of patients after CABG has
reduced accuracy.
• Coronary CT angiography is not routinely recommendable in these
situations.

• Patients with coronary artery stents, which are often difficult to
evaluate. Similarly, although CABGs can be assessed with very high
diagnostic accuracy, detection of stenoses at the site of anastomosis
and in the native coronary arteries of patients after CABG has
reduced accuracy.
• Obesity is a factor of degradation of the quality of the examination
due to the attenuation of X-ray
• One limitation technique is the spatial resolution is lower than that of
conventional angiography makes the exploration of the distal (septal,
diagonal, marginal) difficult.
RISKS OF MDCT
• The usual risks of the injection of iodinated contrast agents (allergic
risk, renal failure)
• The X-ray dose delivered remains significant.
• A coronary MDCT strips is currently two times more radiant than
coronary angiography although the values recorded are well below
accepted standards.

STUDY OF CONGENITAL OF THE CORONARY ARTERIES ANOMALIES
• Although coronary anomalies are rare conditions, possible
consequences include myocardial infarction and sudden death.
• The identification of the origin and course of aberrant coronary
arteries by invasive angiography can be difficult. Because of
the three-dimensional nature of the data set, MDCT is very well
suited to detect and define the anatomic course of coronary
artery anomalies and their relationship to other cardiac and
non-cardiac structures
• Numerous case reports and several research papers have
demonstrated that the CT analysis of coronary anatomy in
these patients is straightforward and very reliable with an
accuracy close to 100%.

=>The robust visualization and classification of anomalous
coronary arteries make CT angiography a first-choice imaging
modality for the investigation of known or suspected coronary
artery anomalies. Radiation dose must be considered often in
the young patients, and measures to keep dose as low as
possible must be employed.
• In our series, angiography and multidetector CT were
complementary.
• In fact, coronary angiography was performed to explore an
acute coronary syndrome whereas CT coronary was
requested further study of the origin or path of an abnormal
origin of from a coronary sinus of Valsalva in contralateral
side.

MDCT ON COMPLEX CORONARY-PULMONARY ARTERY
FISTULA
• Coronary-pulmonary artery fistula is usually detected in 0.1%
to 0.2% of coronary angiograms .
• Although not all coronary-pulmonary artery fistulas are
clinically or hemodynamically significant, some can result in
serious consequences including myocardial ischemia,
myocardial infarction, or sudden death.
• When complex anatomy or intervention is contemplated,
coronary angiography may not be sufficient. An ideal
investigation technique should be noninvasive and provide a
quality anatomic description of the fistula.
• The diagnostic value of coronary angiography is limited by its
planar imaging nature, restricted angle of angiographic
projections, and concern for the contrast load.

• The 3D reconstruction with viewing at an unlimited angle
allows:
o to demonstrate a lesion such as a fistula at its best projection
o without subjecting the patient to repeated radiation exposure
and an additional contrast load.
o makes assessment of the size and exact location of the lesion
feasible.
o quantitative cardiac function analysis.
• This could be helpful for planning future cardiovascular
intervention.

CORONARY ARTERY BYPASS GRAFTS
• Coronary artery bypass grafts (CABGs) move less rapidly and
particularly venous grafts have relatively large diameters
compared with native coronary arteries .
• Occluded grafts and stenoses in the body of bypass conduits
can therefore be detected with very high diagnostic accuracy.
• Accurate assessment of the native coronary arteries by
cardiac CT in patients after CABG is often challenging and
image quality impaired because of advanced CAD and
pronounced coronary calcifications.
• Consequently, the studies that have investigated the
accuracy of CT angiography to evaluate the native arteries in
patients with bypass grafts have reported low accuracies.

• The possibility of a 3-dimensional volumetric study allows easy
viewing of the path of bridges in MDCT , this is crucial before
any redux surgery.
• => Although the clinical application of CT angiography may be
useful in very selected patients in whom only bypass graft
assessment is necessary (e.g. failed visualization of a graft in
invasive angiography), the inability to reliably visualize the
native coronary arteries in patients post-CABG poses severe
restrictions to the general use of CT angiography in post-
bypass patients.

EXPLORATION OF OSTIAL CORONARY LESIONS
• The exploration of the ostium and the first centimeter
of the arteries on coronary angiography is sometimes
delicate. Ostial stenosis may be overlooked, often
hidden or difficult to identify.
• Luminographie planimetry of the core curriculum is
accessible to the scanner.
• Caussin, reports that the 64 slice CT has a sensitivity
and specificity of 87% and 72% in the diagnosis of
significant stenoses of the core compared to IVUS.
• Several authors have also reported the interest of the
scanner in the evaluation of ostial stenosis of the right
coronary.

• The MDCT is as a complementary tool in
the exploration of coronary ostial stenosis
of the core and the right coronary artery.
• It confirms and quantifies stenosis, precise
topography, approach the nature of the
plaque and guide therapeutic decisions.

NOT CATHETERIZED CORONARY
• The noninvasive nature of CT
coronary imaging has allowed a
coronary artery exploration when it is
technically impossible by coronary
angiography.

CONCLUSION
• Although coronary angiography remains the
gold standard investigation for the evaluation of
suspected coronary artery disease. Newer, less
invasive, modalities have been developed that
may complement this. CT coronary angiography
offers high sensitivity and specificity in the
identification of coronary lesions.