Embed Size (px)
Citation preview
S T E L L A B . L E G A R D AM D
ILF Brain Training to Remediate Medically Refractory Involuntary Movement Disorders
M O N TA G E M E D I C A L G R O U P, M O N T E R E Y, C A
Methods
• Subjects: two individuals with distressingly constant involuntary tremors unresponsive to medications for
Parkinson’s Disease and/ or essential tremor
• Subject A: writing tremors; pre-session data
• Subject B: resting tremors; pre-session data
• ILF brain training (Othmer method)
• Results: real time trend graphs, immediate post-session and long-term clinical outcomes
• Review of the current literature on EEG dynamics
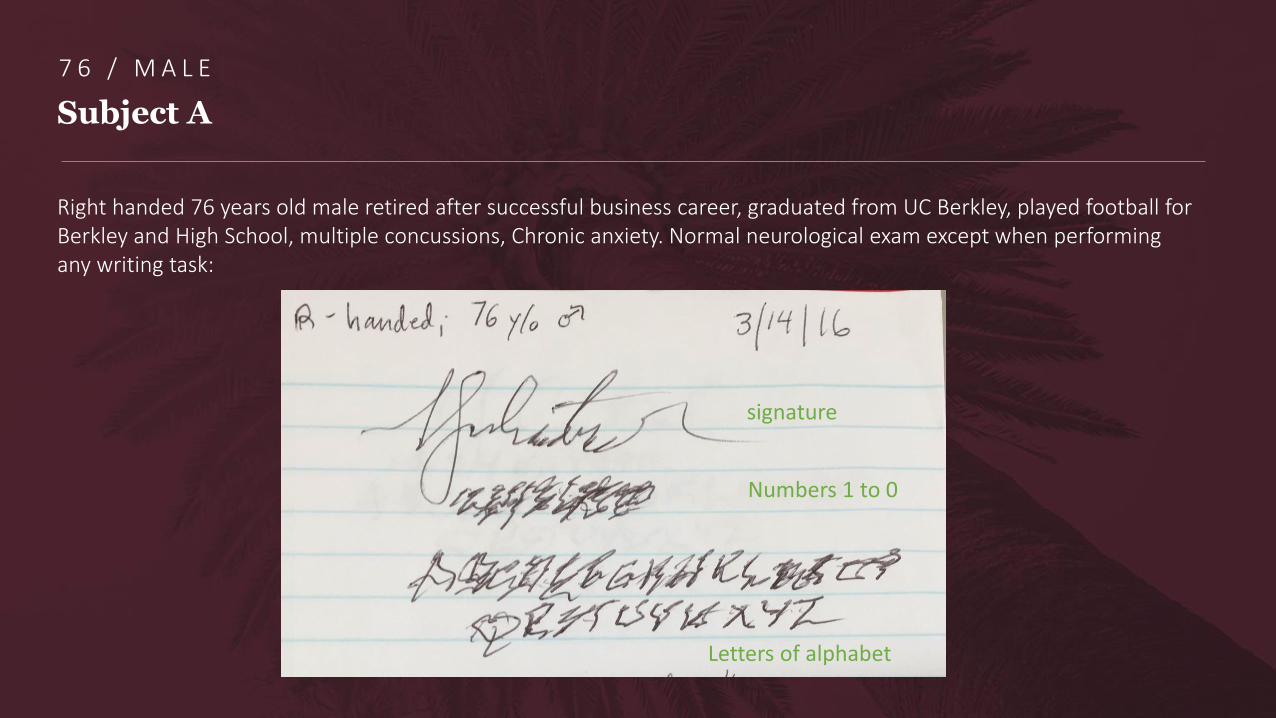
Subject A
Right handed 76 years old male retired after successful business career, graduated from UC Berkley, played football for Berkley and High School, multiple concussions, Chronic anxiety. Normal neurological exam except when performing any writing task:
signature
Numbers 1 to 0
Letters of alphabet
7 6 / M A L E
Subject B
• Right-handed 75 y/o female with Masters in Psychology. Diagnosis of essential tremor made by a
neurologist in 2010.
• 2014: propranolol, without benefit. Stanford, performed DaTscan = negative Diagnosis: “ET or dystonic
tremor, but could be PD”
• Was on clonazepam for sleep, no help with tremor.
• Gabapentin for pain led to cognitive issues.
• Tried low dose Sinemet led to nausea and "feeing hungover"
• Tried pramipexole led to nausea and fatigue.
7 5 / F E M A L E
Subject B
CURRENT SYMPTOMS:
• Tremor - Is located in both hands, more in left. Occurs at rest and with action. Has been progressive, now occurs
most of the day. Is bothersome. Interferes with writing, eating, hobbies, putting jewelry on. Able to complete ADLs. Etoh does not improve tremor. Has tremor in head, leg and has an internal tremor. Voice tremor noted lately. No tremor in chin. Has cousins with PD and tremors. Caffeine use: large cup coffee daily and tea in the afternoon.Worse with stress.
• Bradykinesia - all tasks of day
• Weakness: in hands
• Speech changes - hypophonia, mild recent tremor. No dysarthria
• Sleep - Gets 6hrs/night. Is not interrupted. Takes trazodone 50mg.
• Anxiety - chronic. not treated. Controlled.
Subject B
• Poor attention and concentration - significant issues, diagnosed with ADD. Was on Ritalin for a short time - helpful,
but led to sleep issues and felt jittery.
• Difficulty with memory - has difficulty with word-finding. Forgets details of familiar topics. Difficulty with sequencing.
Had to stop her psychotherapy practice last month.
• Labs: 10/14/15: CMP wnl, except Na 132, heavy metals negative, Lyme reactive to 1 (negative), CBC wnl, B12 594,
folate 10.8, TSH 1.6, FT4 1, FT3 4.1, Thyroid Ab neg.
• DaTscan at Stanford 5/20/15: normal
• MRI Brain 3/13/15: Mild atrophy and chronic small vessel ischemic change. No evidence of acute stroke, mass or
hemorrhage.
Takes Propranolol 2 mg tree times a day; held second dose for this afternoon session = her second neurofeedback session
Subject B Resting Tremors
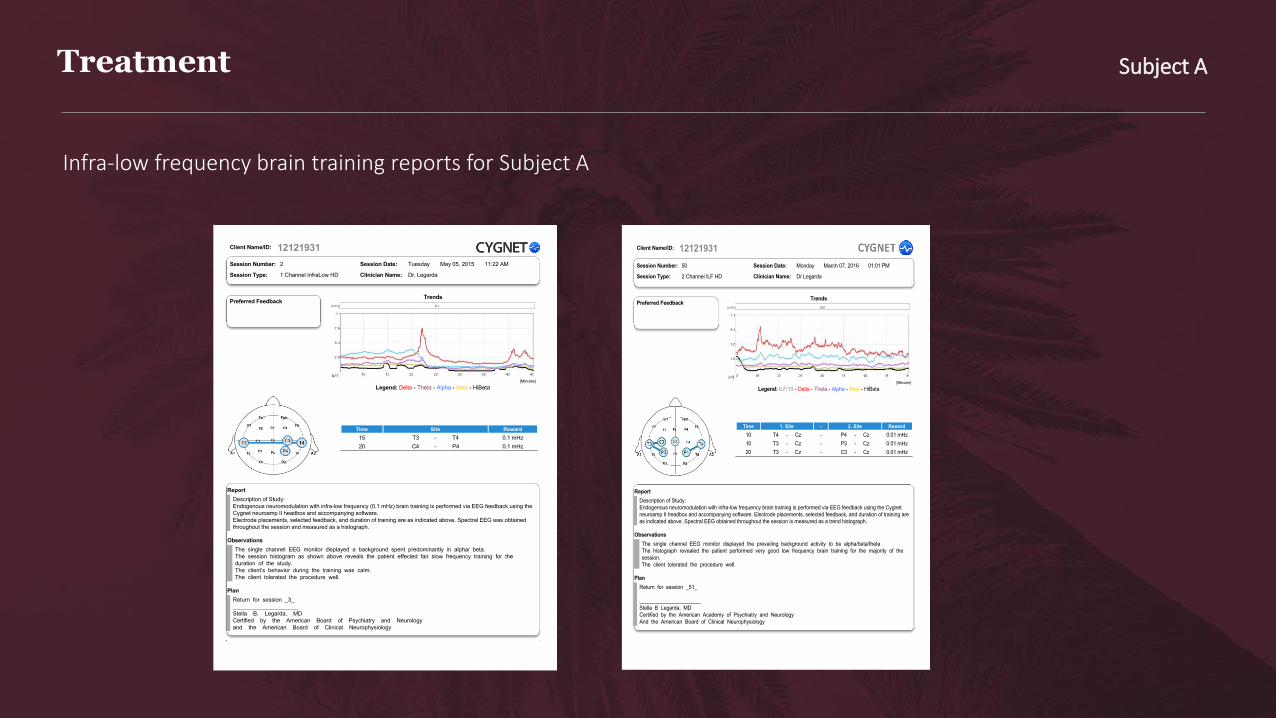
Infra-low frequency brain training reports for Subject A
Treatment Subject A
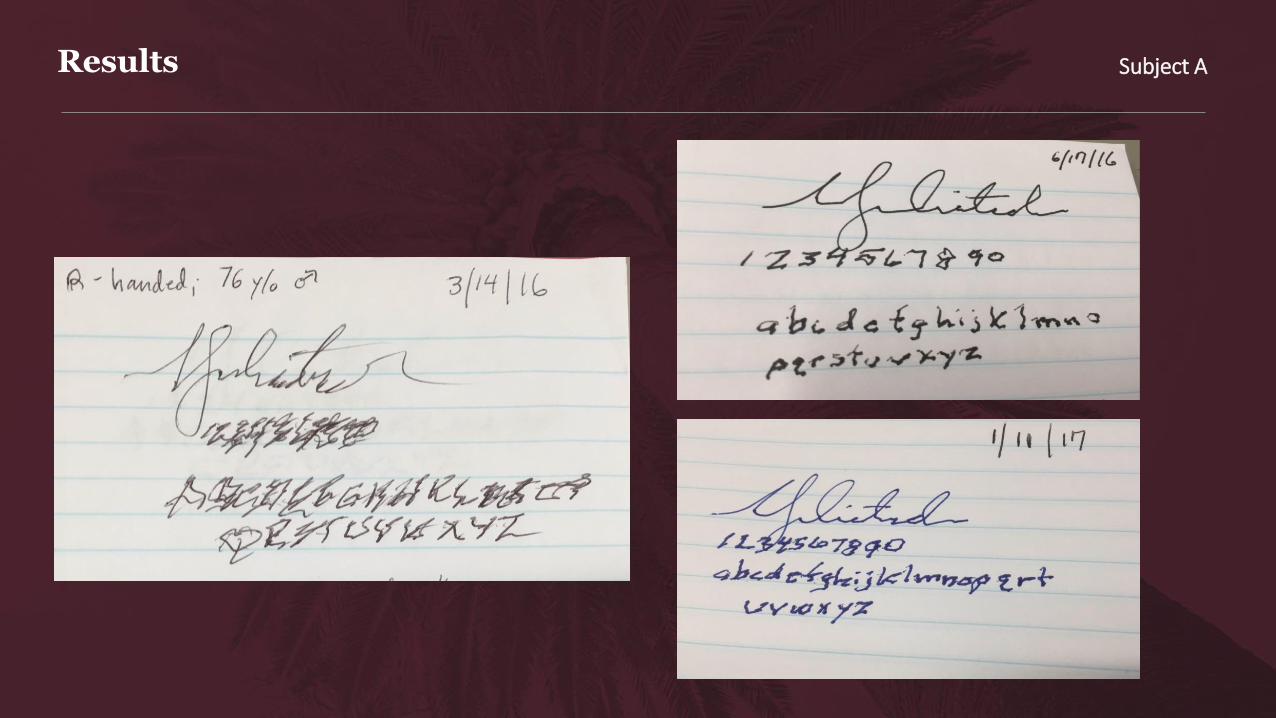
Results Subject A
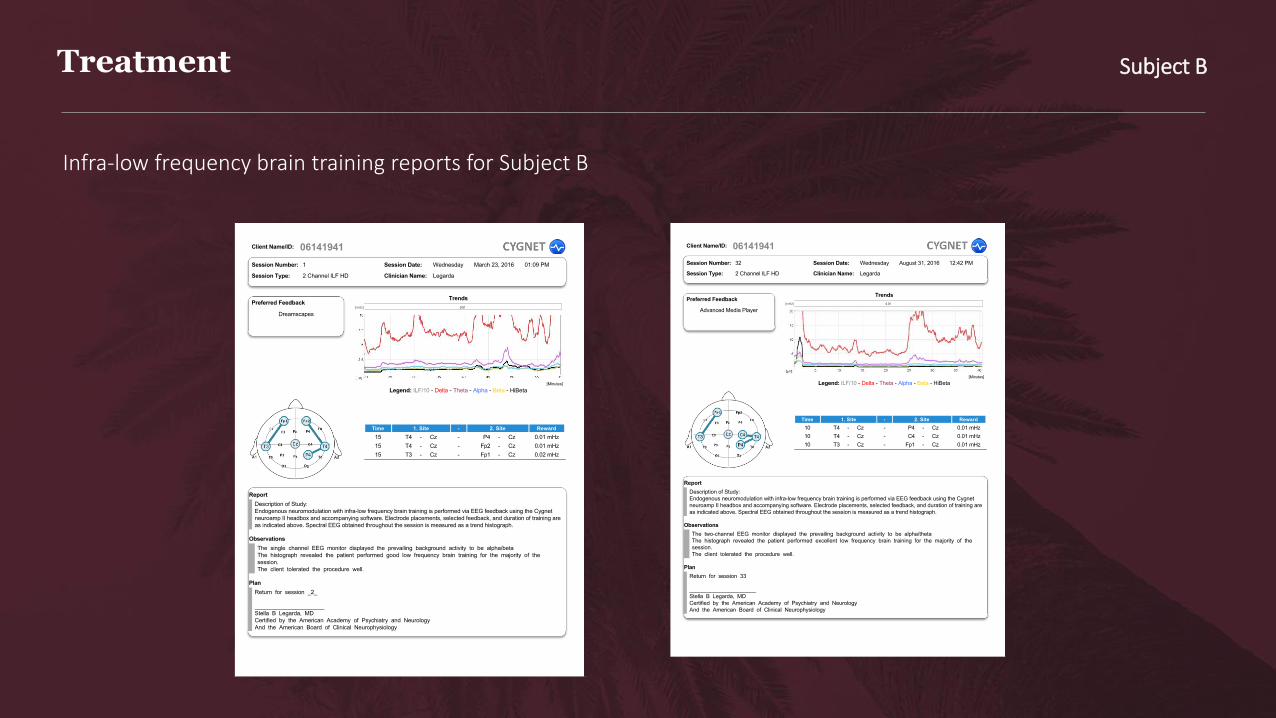
Infra-low frequency brain training reports for Subject B
Treatment Subject B

Subject B: immediately after 2nd neurofeedback session
Results Subject B
Conclusions
• Measurable and observable improvements of motor behavior before and immediately following ILF brain training
(Othmer method) provide objective evidence of the ability to remediate acquired involuntary movement disorders through correlated involuntary network domains
• Motor networks are representative of other salient networks
• A strategic scalp placement accesses the targeted network through highest order neuronal pool dendritic subsystem hubs,
(e.g. T3-C3 for right hand tremor)
• Brain networks utilize repetitive patterns of organizational systems, correlating and integrating brain function for the
purposes of homeostasis and adaptation (ergo survival)
• Clinical benefits of ILF brain training result an optimizing experiential shift within alert resting state networks
towards homeostasis, and reinforcement is needed for learning (adaptation)
Discussion
• 3 main types of brain connectivity
Dec 2016 Thatcher et al
Structural(anatomic)
Functional(coherence/ correlation)
Effective/ PSI(information flow)
• Phase shift; phase shift duration; phase slope index
• Phase lock; phase lock duration
• Small-world model: correlates with prolonged phase shift duration and reduced phase lock duration
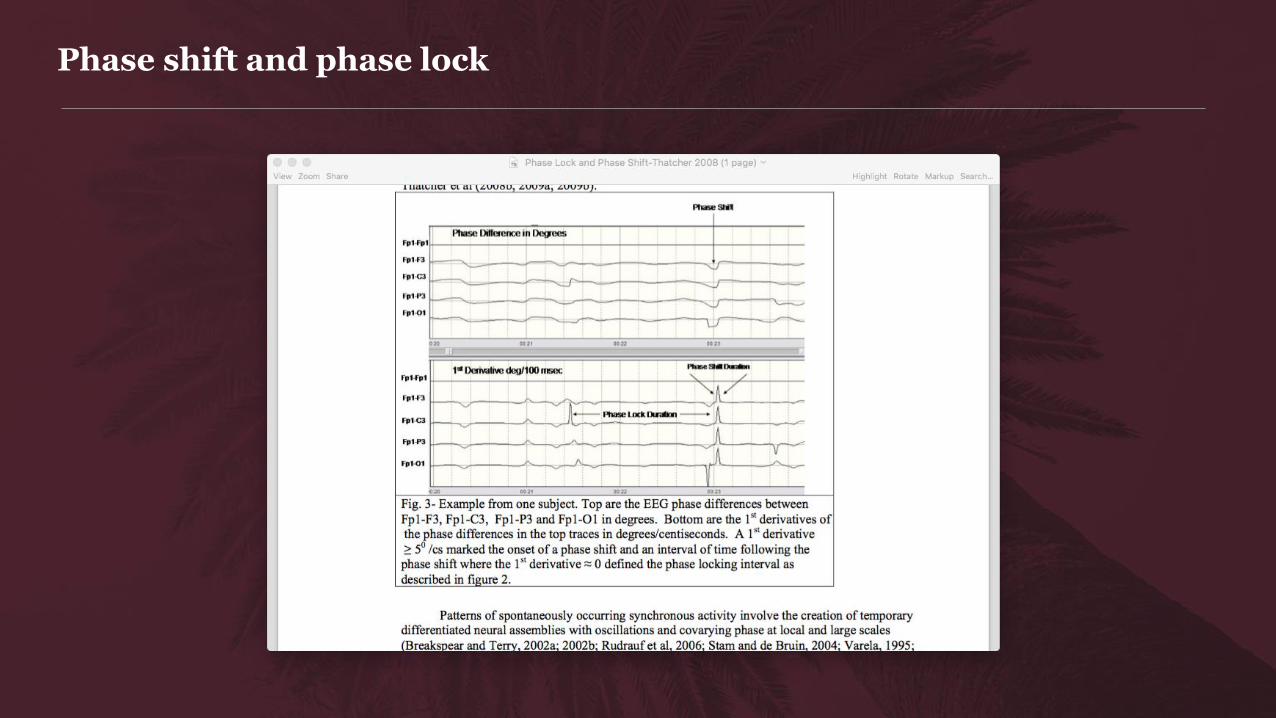
Phase shift and phase lock
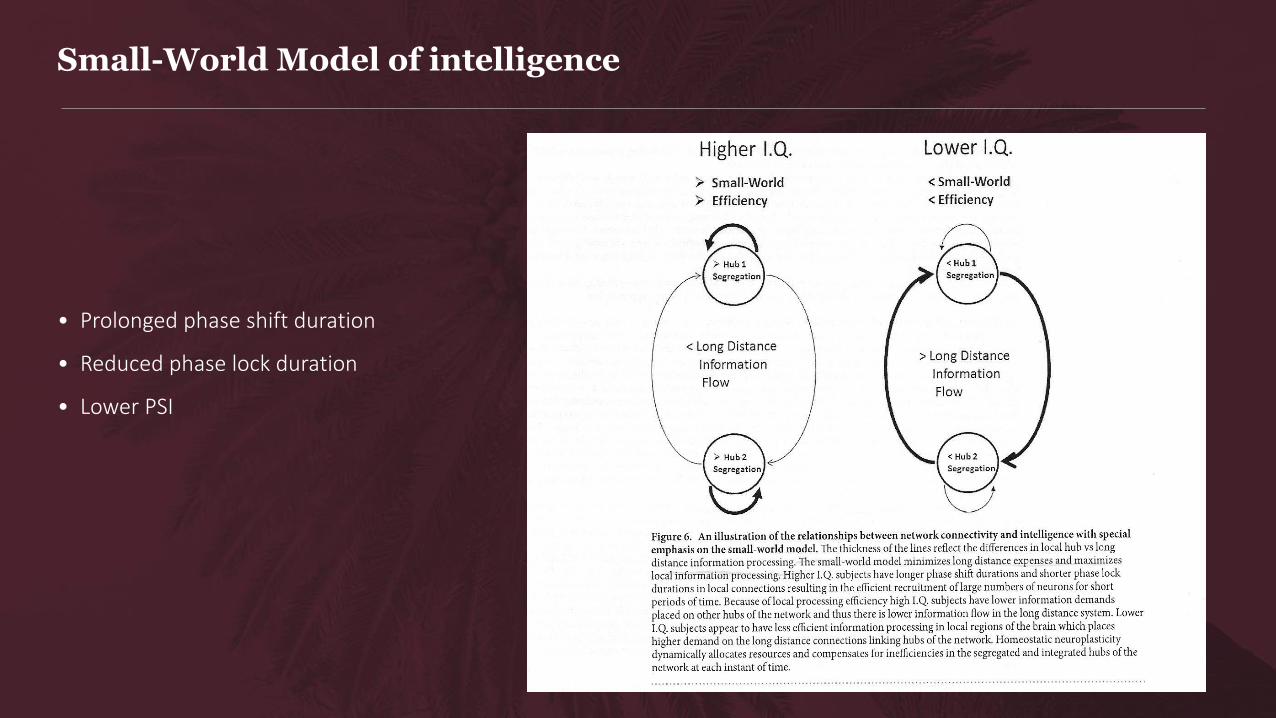
Small-World Model of intelligence
• Prolonged phase shift duration
• Reduced phase lock duration
• Lower PSI
Inhibitory homeostatic neuroplasticity
• Maintenance of small world dynamic
• Minimizes long distance processing
• Maximizes efficiency of local information processing
• Hellyer et al 2016 model network:
1) local inhibitory plasticity can maintain cortex E/I through a homeostatic mechanism
2) locality constrains the resulting dynamics that emerge across the network: criticality
3) the inhibitory weights at each node evolve with learning to reflect… local efficiency
Conclusions / Hypotheses
• Voluntary motor system dysfunction is remediable through involuntary pathways associated with motor control: network dynamics
• Small world model of intelligence is promoted by ILF
• Attention and motivation are prerequisites*
• Conducting the training through strategic scalp site placements optimizes local inhibitory plasticity
• “local inhibitory plasticity tunes macroscopic brain dynamics and allows the emergence of functional brain
networks” (Hellyer et al Jan 2016)
Neurologist Perspective
• Remediation of otherwise untreatable primary neurological disorders is revolutionized by Othmer method; local control to system control
• Nonpharmacological approach
• Empowers patients towards self-healing
• The more troubling conditions respond best; phase shift dynamics autism spetrum, Asperger, concussion, CTE, PTSD, intractable headaches, CVA
• Families, schools, communities and society - positively impacted by the healing of one troubled individual
• Future directions