Embed Size (px)
Citation preview

Mehdi ebrahimi
MD. Assistance professor of
endocrinology

Agenda:
1) Epidemiology of senile diabetes:
2) Pathogenesis of DM in older adult :
3) Clinical presentation:
4) Screening and diagnosis
5)Recommendations for treatment

Epidemiology

Diabetes mellitus is a group of metabolic
disorders characterized by hyperglycemia
due to :
abnormalities in insulin secretion
Insulin action
or both

Type 2 diabetes mellitus (DM) is an
epidemic that continues to increase rapidly,
affecting millions of people worldwide
It is one of the most common chronic
diseases affecting older adults
population is aging and rate of obesity are
increasing among middle-aged adults ,
people ≥65 years old will constitute the
majority of diabetic adults in the coming
decades.
Prevalence DM in 65 to 75 y subjects is
approximately 15-20%
Prevalence DM in subjects older than 80
y is 40%
Nearly half of people with DM
are
≥65 years old.
Baillikre's Clinical Endocrinology and Metabolism-- 389Vol.
11, No. 2, July 1997

ADA classifies DM affecting older adults in to
three types :
A) Type 1 : is the result of an absolute deficiency in insulin secretion
due to autoimmune destruction of the ß cells of the
pancreas.
B) Type 2 : is most commonly due to tissue resistance to insulin
action and relative insulin deficiency.
C) Secondary DM: injuries to the exocrine pancreas ; endocrinopathies characterized
by excesses of hormones , such as growth hormone , cortical ,
glucagon , and epinephrine, which antagonize insulin action ; drug

Diabetes mellitus, results in:
-decreased life expectancy -numerous complications and co morbidities -higher risk of other common geriatric conditions
1) polypharmacy 2) urinary incontinence 3) falls 4) cognitive impairment 5) depression 6)chronic pain

Older adults with diabetes can expect :
10- years reduction in life expectancy
mortality rate nearly twice that of people
without disease.

In older adults with diabetes:
The rates of myocardial infarction , stroke , and kidney failure are increased approximately 2-fold .
The risk of blindness is increased approximately 40%,
Most patients ≥65 years old who require dialysis have diabetes.
Mobility problems are about 2 to 3 time more
likely in older adults

older patients are frequently on multiple
medications, increased risk of drug
interactions with greater risk of adverse
effects, most commonly hypoglycemia .

Thus, management of DM in the elderly is
challenging and requires multi-dimensional
approach focusing on:
preventing diabetic complications,
early interventions for vascular disease,
and disability assessment.
Because of the heterogeneity in the older population , treatment goals must be carefully individualized

Pathogenesis of DM in
older adult :

The prevalence of both type 2 diabetes and
glucose intolerance increases with age the
reasons for this are not fully known.
there appears to be an interaction among
several factors , including:

1)Obesity contribute to impairments in insulin action.
2)decline in pancreatic ß-cell function and in the insulin-signaling mechanism
3)Changes in body composition such as increased visceral fat leading to insulin resistance .

4)Decreased level of physical activity
5)An altered inflammatory environment with aging
6) Some medications commonly taken by older adults
-diuretics , sympathomimetics, Glucocorticoids , niacin , and olanzapine-change carbohydrate
metabolism and increase glucose concentration.

Signs and Symptoms

elderly diabetics may not present with
classical symptoms which makes diagnosis
more difficult.
Polyuria may be seen as incontinence or
prostate problems.
Glucosuria may be missing due to chronic
renal disease.
glycosuria may be absent because the renal
threshold for glucose also increases with age

presenting symptoms may be
Dehydration,
confusion,
urinary incontinence,
urinary tract infections,
slow wound healing in the legs and feet,
complications related to DM
functional disability

Diabetic patients tend to have an accelerated ageing process that places them at greater risk of developing frailty at an earlier age

Frailty is characterized by:
deterioration in muscle and nerve function,
anemia,
declining cardiopulmonary reserve,
loss of executive function

The Cardiovascular Health Study showed:
25% of frail subjects were diabetic,
18.2% of pre-frail subjects were diabetic,
only 12% of non-frail subjects were diabetic.

It is clear that diabetes and frailty are closely interrelated, but only minimal evidence suggests the causal relationship between DM and frailty.

Aside from diagnostic challenges, elderly diabetic patients also more commonly have:
functional disabilities, cognitive decline, increased rates of bone fracture, increased hypoglycemic events
which all contribute to the complexity of diabetes care in the elderly population.

Screening and diagnosis

Clinical presentation of diabetes in old age is often asymptomatic and non-specific and clinical diagnosismay be delayed.

screening for and diagnosis of diabetes in older subjects:
should be in accordance with published international/national guidelines and no age modified criteria are currently recognised.

Plasma Glucose Level (mg/dL)
* Third criterion: casual plasma glucose 200 mg/dL (regardless of time since last meal) plus
classic symptoms of diabetes (polyuria, polydipsia, unexplained weight loss)
Stage of
Glycemic Control
Fasting Plasma
Glucose
OGTT
(2-hr Post-load Glucose)
<100
100 –125
126
<140
140 –199
200
Normal
IFGor
IGT
Diabetes*
ADA. Diabetes Care. 2007; 30:S5
Criteria for the Diagnosis of
Diabetes: 2007 ADA Guidelines
29

IFG = FPG 100 mg/dl (5.6 mmol/l) to 125
mg/dl (6.9 mmol/l)
IGT = 2-h plasma glucose 140 mg/dl ( 7.8
mmol/l) to 199 mg/dl (11.0 mmol/l)
Pre-diabetes
ADA. Diabetes Care. 2007; 30:S5
30

Glucose Tolerance Categories
FPG
126 mg/dL
100 mg/dL
7.0 mmol/L
5.6 mmol/L
Impaired Fasting
Glucose
Normal
2-Hour PG on OGTT
200 mg/dL
140 mg/dL
11.1 mmol/L
7.8 mmol/L
Diabetes Mellitus
Impaired Glucose
Tolerance
Normal
Diabetes Mellitus
ADA; Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 2007; 30:S4531

The prevalence and incidence rates of diabetes mellitus in elderly subjects (> 65 years) may be underestimated when using only fasting plasma glucose.
presence of isolated post-challenge hyperglycaemia (IPH) is common in older subjects and should alert the clinician to screen for cardiovascular disease
In high-risk older subjects with a normal fasting glucose:
1)OGTT 2)IF OGTT is not feasible,HbA1c
may be helpful in the diagnosis of diabetes.
A value of HbA1c > 6.5% may indicate the likely presence of diabetes.
Prevention and lifestyle change

1. In older adults with IGT regular exercise reduce the risks of developing type 2 diabetes independently of BMI.
2. Lifestyle intervention is preferable to metformin in reducing the risks of type 2

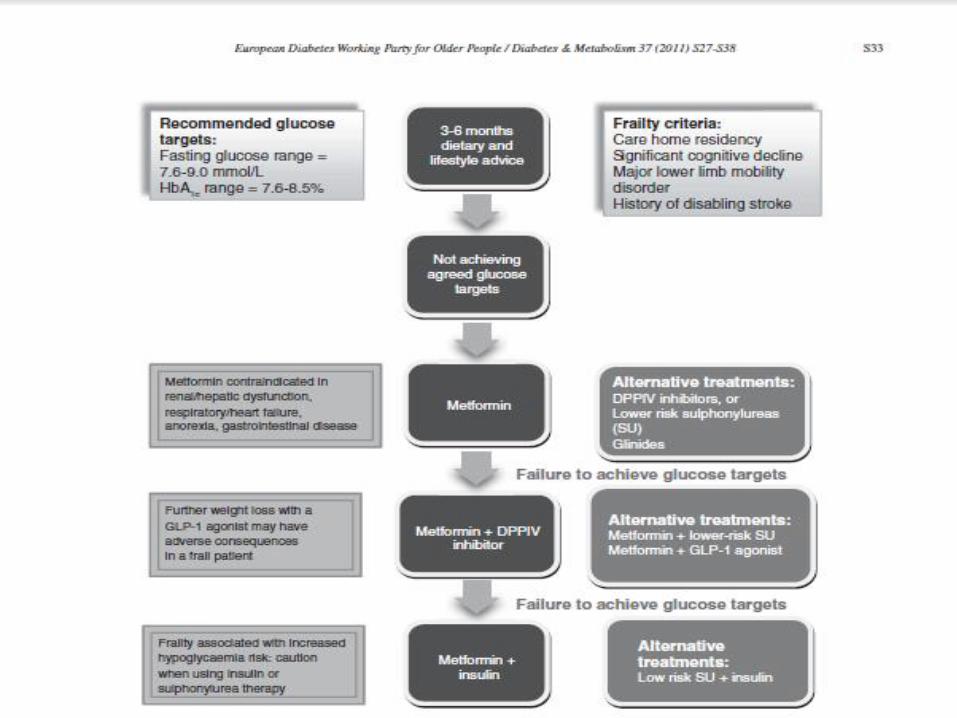
Recommendations for
treatment
A)Glucose regulation Targets
1. For older patients with type 2 diabetes, with single system involvement (free of other major co-morbidities)
HbA1c range of 7-7.5% should be aimed
FBS range of 90 -130mg/dl can be regarded as indicating good control.

2. For frail (dependent; multisystem disease; care home residency including those with dementia)
and patients high risk for hypoglycaemia
target HbA1c range should be 7.6-8.5%.
FBS range of 100-180mg/dl can be regarded as indicating good control.

B)Use of oral agents
1) In non-obese older people with diabetes in whom target levels of glucose or HbA1c have failed to be maintained on dietary/lifestyle first line therapy with
an insulin secretagogue or metformin should be offered.

2. Metformin should normally be first line therapy for older adults
3. An insulin secretagogue may be used in combination with metformin where glycaemictargets have not been achieved

Age per se is not a contraindication to the use ofMetformin
use is contraindicated in those with :
renal impairment (serum creatinine>130 μ/litre), severe coronary, cerebrovascular disease peripheral vascular disease

4) Glibenclamide should be avoided for newly diagnosed type 2 diabetes in older adults (>70 years)
because of the marked risk of hypoglycaemia.

Regularly assess patients for hypoglycemia, as
hypoglycemia risk is linked more to treatment
strategies than to achieved lower A1C.
Strongly consider changing therapy and/or
targets in presence of recurrent or severe
hypoglycemia

Use of insulin
When oral agents fail to lower glucose levels adequately, insulin may be given either as monotherapy or in combinationwith a sulphonylurea or metformin.

In older adults with diabetes, the use of pre-mixed insulin and pre-fi lled insulin pens
lead to a reduction in dosage errors and an improvement in glycaemic control.
Use of a glargine, determir rather than NPH-insulin should be considered in older patients who:
require the assistance of a carer, those residing within a care home, higher risk of hypoglycaemia.

B) Blood pressure regulation
Blood pressure should be measured at
every routine visit.
Patients found to have elevated blood
pressure should have blood pressure
confirmed on a separate day.

1. The threshold for treatment of high blood
pressure in older subjects with type 2 DM
140/80 mmHg or higher
Patients with confirmed blood pressure
should, in addition to lifestyle therapy, have
prompt initiation of pharmacological therapy to
achieve blood pressure goals.

2. In non-frail subjects with diabetes
older than 80 years:
an acceptable blood pressure on
treatment is :
a systolic of 140-145 mmHg,
a diastolic less than 90 mmHg.

3. For frail patients : (dependent; multisystem disease; care home residency including
those with dementia)
where avoidance of heart failure and stroke
may be of greater importance than
microvascular disease,
acceptable blood pressure is <150/90
mmHg.

4. In older patients with a sustained blood
pressure ≥140/80 mmHg and in whom
diabetic renal disease is absent:
first-line therapies include:
use of ACE inhibitors,
angiotensin II receptor antagonists,
long-acting calcium channel blockers,
beta blockers
thiazide diuretics.

5. In older patients with a sustained blood
pressure ≥140/80 mmHg with microalbuminuria
or proteinuria, treatment with:
ACE inhibitor or angiotensin II receptor
antagonist is recommended.

• As part of the assessment of older newly-
diagnosed HTN:
investigations to exclude secondary causes
must also be considered

There is less evidence for lipid-lowering
and aspirin therapy,
benefits of these interventions for primary and
secondary prevention are likely to apply to
older adults whose life expectancies is high.
C) Plasma lipid regulation

Recommendations for care
home diabetes
In view of the high rate of undiagnosed
diabetes in care home residents
at the time of admission to a care home
each resident requires to be screened for
the presence of diabetes.

Good clinical practice in care homes
Each resident should have an annual screen for diabetes
Each resident with diabetes should have an individualised diabetes
care plan with the following minimum details: dietary plan, medication
list, glycaemic targets, weight, and nursing plan.
Each care home with diabetes residents should have an agreed Diabetes
Care Policy or Protocol which is regularly audited.
All residents with diabetes require a risk-benefi t analysis in terms of
medication used, metabolic targets agreed, and extent of investigation
of diabetes-related complications.

Residents on insulin secretagogues and/or
insulin must be regularly reviewed for the
presence of hypoglycaemic symptoms

Optimal blood pressure and blood glucose
regulation may help to :
maintain cognitive and physical performance
for each resident with diabetes.

Recommendations in special
categories

a) Falls and immobility
1. As part of their functional evaluation at
diagnosis and at annual review,
older people with diabetes should
have a falls risk assessment.

This will include identifying risk factors which
can be minimised, e.g. certain medications, environmental items, and undertaking
measures of gait and balancee.
It is particularly important to monitor insulin
therapy,
where insulin secretagogues are used in a
patient with other risk factors for falls, an agent
with a lower risk of hypoglycaemia
should be substituted

Tight glycaemic control (HbA1c<7.0%)
must be avoided in older patients with type
2 diabetes who are at increased risk
of falling.

a) Cognitive impairment and low
mood states
1. At the diagnosis and at regular intervals
thereafter, patients 70 y and over
should be screened for the presence
of cognitive impairment
using an age- and language-validated
screening tool such as the MiniMental State Examination score.

2. Regular screening for cognitive impairment
and mood disorder is recommended
for residents with diabetes who are
at high risk of undetected disease.
3. Optimal glucose control may help to maintain
cognitive function in older people with diabetes.

4. Optimal blood pressure control help to
maintain cognitive performance and improve
learning and memory.
5. Prevention of repeated hypoglycaemia in
older patients with diabetes :
decrease the risk of developing cognitive
impairment or dementia.

B) Visual loss and erectile dysfunction
At the time of diagnosis and at regular
intervals thereafter:
all older people with diabetes should have a
standard visual acuity assessment and retinal
examination .

Although direct ophthalmoscopy is a useful
tool for screening in older patients,
they are no substitute for retinal photography and slit lamp
examination in the screening for diabetic retinopathy.

To maintain vision in older patients with
type 2 diabetes and established retinopathy,
optimal blood pressure control (≤140/80 mmHg)
optimal glycaemia (HbA1c 7.0– 7.5%) should be
aimed for.

Older adults with diabetes and erectile
dysfunction
require a comprehensive evaluation of underlying risk
factors.
A detailed cardiovascular evaluation
Oral phosphodiesterase type 5 inhibitors, unless
contraindicated, as a first-line therapy

Each older adult with type 2 diabetes and
cardiovascular disease:
should be asked about their sexual
health.

c) Peripheral neuropathy and pain
1. At the time of diagnosis and at regular
intervals thereafter older patients with
diabetes
should be questioned about symptoms of
neuropathy
examined for the presence of peripheral
neuropathy

2. Gabapentin can be used in older patients
and is superior to placebo in painful diabetic
neuropathy
have fewer side-effects than tricyclic
antidepressants (TCAs).
3-Duloxetine an alternative treatment
for diabetes-related neuropathic pain when
given at doses of 60mg or 120mg daily.
Elderly patients with diabetes are generally
treated following the same approach as in
younger patients:
dietary therapy first,
followed by oral hypoglycaemic agents
insulin.