Embed Size (px)
DESCRIPTION
MCB 135E: Mid-Term II Review. November 7, 2005 GSI: Jason Lowry. Mid-Term II Material. Labor and Delivery Transition and Adaptation The Normal Newborn and Newborn Risks and Diseases Lactation and Breast Feeding Gastrointestinal Function Liver Detoxification Development of Kidney Function - PowerPoint PPT Presentation
Citation preview

MCB 135E:Mid-Term II
Review
November 7, 2005
GSI: Jason Lowry

Mid-Term II Material
1. Labor and Delivery
2. Transition and Adaptation
3. The Normal Newborn and Newborn Risks and Diseases
4. Lactation and Breast Feeding
5. Gastrointestinal Function
6. Liver Detoxification
7. Development of Kidney Function
8. Development of Water, Electrolyte and Acid/Base Balance
9. Characteristics of Growth
10. Endocrinology of Growth

Parturition
• Birth Process – 38 Weeks after fertilization– 40 Weeks after last menstrual period
• Onset of Labor– Process that is not completely understood, but
involves a combination of mechanical and hormonal factors

Hormones• Fetal Hormones
– CRH, ACTH, Cortisol
• Estrogen– Increases uterine contractility– Inhibited by P during most of pregnancy
• Progesterone– Inhibits E induced uterine contractility– Ratio of E:P change late in pregnancy removing P inhibition of E
• Oxytocin– Stimulates uterine contractions– “Hormone of Love”
• Prostoglandins– Promote uterine contractions
• Relaxin– Secreted by ovary and placenta to prepare pelvis for delivery– Loosens ligaments holding pelvic bones together


Delivery Phases
• Dilation and Effacement– Contractions <10 minutes apart– Cervix Dilating and thinning– Average 7-12 hours in duration
• Descent and Expulsion– Cervix fully dilated (10cm)– Contractions are strongest at top pushing fetus downward– Average 20-50 minutes in duration
• Expulsion of the Placenta– Uterus contracts reducing area of attachment– Separation of placenta results in bleeding and clotting– Pitocin given to assist uterine contractions– Average 15 minutes duration


Transitional Physiology
• Newborn Structure1. Bronchi/Airways
2. Air sacks / alveoli
3. Pulmonary Vein
4. Pulmonary Artery
5. Diaphragm
• Fetal Equivalent1. Uterine Artery
2. Placental Sinusoids
3. Umbilical Vein
4. Umbilical Artery
5. Maternal Myocardium

Transitional Physiology
• Changes in fetal circulation at birth:– Loss of placenta– Opening of pulmonary arteries– Functionality of the lungs
• Blood is allowed to flow to lungs due to less pressure (the path of least resistance)
– Apoptosis of fetal modifications

Respiration
• First breath– Responsible for opening of lungs– 30-100mmHg in newborn vs. 5-10 mmHg
normal adult
• Close ductus arteriosus– First functional, later anatomical
• Removal of lung fluid

Removal of Lung Fluid at Birth1. Fetus = Cl- pumps move fluid into potential air space.
2. Very little protein in potential air space liquid.
3. Result = osmotic pressure draws liquid from the alveolar space to the interstitium = circulation.
4. Newborn = Cl- pumping stops and Na+ pump moves fluid out of alveoli.
5. Air pressure in the alveoli drives liquid out and into interstitium.
6. Expansion of the lung stretches open the pulmonary vessels and thereby reducing pulmonary vessel pressure and hydrostatic pressure.
7. Net result = liquid leaves air spaces and exits the interstitial space via the lymph and microcirculation.

The Apgar ScoreAssessment of transition
Score 0 1 2Heart rate
Respiratory effort
Muscle tone
Reflex irritability
Color
Absent
Absent
Limp
Absent
Blue, pale
Less than 100/min
Slow, irregular
Some flexion of extremities
Grimace
Body pink/extremities blue (acrocyanosis)
More than 100/min
Good, crying
Active motion
Grimace and cough or sneeze
Completely pink

What to Expect…
• The first week of life:– Vitamin K
• control blood clotting and is essential for synthesizing the liver protein that controls the clotting (thrombin)
– Antibiotic Eye Drops
– Hepatitis B Vaccine
– Jaundice (Common Problem)• Indicator of postbirth adaptations
• Caused by an incomplete metabolism of bilirubin – Bilirubin is a waste product of hemoglobin breakdown

The New Born
• Risk Factors– Fetal Distress– Meconium Aspiration– Fetal Sepsis (Group B Streptococcal)– Congenital Anomalies– Maternal Diseases– Toxins– Premature Birth

Thermoregulation• The Problem of Heat Loss
– Fetal – Heat loss through maternal blood– Infant – Large SA:volume ratio makes it difficult to maintain
body temperature– Adult – Able to maintain body temperature in a 5C enviroment
• Effects of Environment– Thermoneutral zone is range where metabolic rate is minimal– Outside this range there is a caloric cost to regulate temperature
• Nonshivering Thermogenesis• Mechanisms of Heat Loss

Non-Shivering Thermogenesis
• Regulation – Involuntary response to cold stress– Receptors in skin, spinal cord, hypothalamus– Vasoconstriction – Increased heat production via brown fat
metabolism

Brown Fat Metabolism• Hypothalamus secretes norepinepherine
– Stimulates specific receptors on the brown fat cell• Beta-adrenergic Lipase pathway• Alpha-adrenergic Thyroid hormone activation
– Lipase breaks down triglyceride• Glycerol and Fatty acids secreted to blood and utilized by other cells• Fatty Acids enter mitochondria of brown fat cell and enter glycolytic
pathway through Beta-oxidation– ATP Synthetase Pathway is by-passed– UCP-1 uncouples mitochondrial oxidative phosphorylation– Proton gradient produces heat rather than ATP
• Process requires large amounts of O2
– Increased thyroid hormone leads to increased mitochondrial activity

Mechanisms of Heat Loss
• Conduction– Heat transfer from one solid body to another
• Convection– Heat transfer from a solid to the surrounding gas or liquid
• Evaporation– Air passing over a body evaporates liquid– Largest form of heat loss in infants
• Radiation– Exchange of infrared photons with the surroundings– Heat can be gained or lost depending on gradient

Lactation
• Mammary Gland Development
• Milk Production, Ejection, Cessation
• Benefits of Breast Feeding

Mammary Gland Development
• 6th week of gestation– Formation of mammary ridges (ectoderm)
• Ridges canalize to form ducts• Results in 15-20 lactiferous ducts at birth• Further development under influence of E (pre-
natal)• Female breasts develop further at puberty
– Again primarily under influence of E– Enlargement due to fat deposits and connective tissue– Further growth and branching of ductal system


Development of Breasts:Puberty
Female breasts develop further after puberty (under influence of E from developing follicle &
corpus luteum each month)
• Enlargement occurs due to deposition of fat & connective tissue
• Nipple becomes enlarged and pigmented
• Further growth & branching of lactiferous ducts

Development of Breasts: Pregnancy• More intense growth and branching of lactiferous
ducts (under high levels of E from corpus luteum & placenta)
• GH, glucocorticoids, prolactin (PRL), insulin all influence growth
• Final development of mammary glands occurs under the influence of progesterone (P), which (in concert with hormones mentioned above) cause alveoli to bud from the ends of the lactiferous ducts
• Each alveolus is lined by milk secreting cells

Milk Production(during pregnancy)
• PRL, secreted by anterior pituitary gland, stimulates milk production
• During pregnancy, PRL levels increase 20 fold but action of PRL inhibited by high E & P levels
• Human chorionic somatomammotropin ( i.e. placental lactogen) plays role in lactogenesis
• Towards end of pregnancy, breasts are fully developed but milk production is suppressed except for small amount of colostrum (same concentration of proteins and lactose as regular milk but hardly any fat)

Milk Production(after birth)
• After birth, E and P levels drop and milk is produced in 1-7 days
• Milk production requires: secretion of hormones involved in protein, glucose & calcium regulation (GH, cortisol, insulin, PTH)
• PRL levels return to normal within a few weeks. Each time an infant feeds, neurohumoral reflex leads to burst of PRL secretion

Milk Ejection• Alveolar milk accumulate in the lactiferous sinuses
(enlargements of ducts near opening of nipple)
• Suckling hypothalamus release of oxytocin from post. pituitary.
Oxytocin contraction of myoepithelial cells around the ducts.
• Negative maternal emotions (frustration, anger, anxiety) can inhibit oxytocin secretion & suppress milk ejection reflex


Benefits of Breast Feeding
• Infant– Reduction in infections
• Secretory IgA
– Initial increased growth
– Decreased obesity in adulthood
– Positive effects on mental development
• Mother– More rapid and
sustained weight loss
– Lactational amenorrhea
• Decreased Breast Cancer for mothers
– Psychological benefits

Immunology• Infant immune system is immature at birth.
• In utero, transfer of antibodies across placenta.
• This protection tapers off quickly after birth.
• Breast milk contains a number of different agents to protect the infant:– Secretory IgA– WBCs: neutrophils and macrophages– Growth factors: EGF, NFG, IFG

G.I. System
• GI Functions– Digestion and Absorption– Defense– Endocrine– Mechanical and Chemical
• Nutrition of the Infant


G.I. System Development
• Smaller size = Shorter duration of food in GI• Developing Stomach
– Spitting, Regurgitating, burping are a result of peristalic waves in opposite direction
– Emptying time • First Month – 1-4 Hours
• Adult – 5-6 Hours
– Size (Volume) much smaller at birth with continual increase in size until adulthood

Nutrition
• Proteins– Synthesized in alveolar cells– Casein and lactalbumin are
predominant proteins– Have antigenic properties
• Vitamins– No supplements required for
infant while breast feeding
• Minerals– Mother needs to take
calcium supplements
• Fats (Breast Milk)– High in essential FA required
for brain and retina development
– Secreted in droplets pinched off from cell into alveolus
• CHO– Lactose – Predominant Milk
Sugar– Glucose – Primary direct
source of energy– Galactose – used as energy
and in biosynthesis pathways

Liver• Functions (Post-Natal)
– Formation of Bile– CHO storage– Formation of Urea– Cholesterol Metabolism– Make plasma proteins– Regulates fat metabolism– Metabolizes some polypeptide hormones– Reduction and conjugation of steroid hormones– Vitamin D3 metabolism– Detoxification

Bile
• Functions– Emulsification of lipids– Activation of enzymes for
digestion of lipids– Conjugation of bilirubin to
form a water soluble product for excretion
– Excretion of cholesterol– Excretion of drugs, heavy
metals, and environmental toxins
– Neutralization of acid delivered to duodenum from stomach
• Constituents– Water (97%)– Bile Salts– Bile Pigments
(Bilirubin and Biliverdin)
– Cholesterol– Inorganic Salts– Fatty Acids– Lecithin

The Kidney and Urinary System
• Anatomy
• Function
• Hormones
• Circulation
• Development



Kidney Functions
• Regulates – Water– Electrolyte balance– pH
• Removes– Waste
• Secretes Hormones– Erythropoiten– Renin– Vitamin D3

Metabolic and Excretory Functions
• Glomerular Filtration– Selective filtration of blood
• Tubular Reabsorption– Takes up some solutes from filtrate and delivers
them to peritubular capillaries
• Tubular Secretion– Adds some of its own products to the filtrate,
passes filtrate on to bladder as urine



Kidney Development
• Mesodermal Nephrogenic Cord Holonephros pronephros (primitive kidney)
• 4th Week Mesonephros
• 20-24 Weeks Metanephros Permanent Kidney
• Metanephros– Mesodermal – glomeruli,
tubules– Ectodermal
• Ureteric Bud

Water Metabolism
• Osmotic Pressure – – Force driving or pulling a solvent from lesser to greater
concentration on either side of a selectively permeable membrane
• Regulation of solute exchange– Selective permeability of membrane
– Influence of hormones and metabolites on membrane
– Simple and exchange diffusion across membrane
– Active secretion by the membrane


Risk Factors of Water Metabolism in Infants
• Skin – Greater water loss through skin (increased surface area)
• GI Tract – Less time for water reabsorption
• Kidney – Less urea; weaker osmotic gradient; Shorter loop of Henle
• Posterior Pituitary – Less ADH Secreted
• Adrenal Cortex –

Acid Base Balance
• Determined By:– Hydrogen Ion Concentration (pH)
• Normal 7.3-7.5
• Max 7.0-7.8
– Alkali reserve• CO2 combing power of plasma
• Normal 50-70% Volume
– Both vary due to exercise and metabolism

Acid-Base Regulation
• Rate and depth of respiration controls CO2 release in lungs
• Excretion of acids and conservation of alkali by kidneys

Urine Acidification Mechanisms
• Reabsorption of Filtered Bicarbonate– In proximal tubule: H+ exchanged for Na+
– In distal tubule and collecting duct• CO2 and HCO3(-) are transported into cell and form H2CO3
by carbonic anhydrase
• Dissociation of H2CO3 releases H+ which is then exchanged for Na+
• Secretion of Ammonia– In distal tubule
• NH3 + H- NH4 (Ammonium) [formation of a titrable acid]

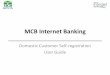
AB
Growth Curves Before Birth
A: Same sigmoid shape of length growth as occurs postnatally
B: The first peak of post natal growth follows a peak of prenatal growth in the 4-6 months.

Growth Hormone (GH)• Stimulates bone and muscle growth
– Accelerates chondrogenesis (proliferation of epiphyseal cartilage)
• Increases protein synthesis by direct action on tissues
• Increases protein synthesis by indirect action: production of growth factors (IGF-1)
• Increases lean body mass
• Decreases body fat
• Exerts anti-insulin effects on muscle & liver

Insulinlike Growth Factors (IGF I & II) (also known as Somatomedins)
• Peptides produced by the liver & resembling structurally insulin
• Relaxin, a peptide secreted during delivery is also related to IGFs
• IGF I is stimulated by growth hormone (GH) and has growth stimulating activity– Factors reducing IGF I secretion are: glucocorticoids,
protein deficiency, large dose of estrogens, diabetes
• IGF II is found primarily in the fetus and is not influenced by GH

Pygmies• Short stature despite normal plasma levels of
GH; however, GH fails to stimulate the production of IGF-1
• Cause of IGF-1 deficiency is unknown
• Malnutrition may induce a similar failure of IGF production but Pygmies are generally not deficient in proteins
• Hybrid Pygmies have IGF levels intermediate between Pygmies and African farmer populations

Other Information
• Adolescence / Puberty Lecture Posted on Web Site
• Exam covers material through Monday, November 7th, 2005
• This exam is not comprehensive
• Bring pen and pencil