Embed Size (px)
Citation preview

7/31/12
1
HOSPITAL/PHYSICIAN ALIGNMENT MODELS AND THE ALIGNMENT PROCESS
August 13, 2012
Presented by: Max Reiboldt, CPA President/CEO
AGENDA
Ø Current Alignment Trends
Ø Alignment Models
Ø Process for Hospital/Physician Alignment
Ø Compliance
Ø Impact of Healthcare Reform 2
CURRENT ALIGNMENT TRENDS

7/31/12
2
HOSPITAL /PHYSICIAN ALIGNMENT
• In the 90’s, hospitals focused on purchasing exisNng pracNces to build their referral network
• CapitaNon drove this desire to employ physicians • Physicians were compensated via salary guarantees • No (or very liTle) requirement for producNvity or producNvity-‐based incenNve plans
• Hospitals failed to “partner” with physicians in decision making process that affected the pracNces
• Physicians resented the hospital’s focus on cost cu[ng programs
THEN
4
HOSPITAL /PHYSICIAN ALIGNMENT
• Hospitals are purchasing pracNces for Fair Market Value (FMV), entailing liTle up-‐front payments and virtually no goodwill
• Physician producNvity is a key matrix in provider compensaNon
• Hospitals and physicians are striving to form true “partnerships” that focus on quality of paNent care, delivery of services, and cost effecNve management
• Non-‐employment models (like PSAs) are frequently viable alternaNves and preferred
NOW
5
HOSPITAL /PHYSICIAN ALIGNMENT
• Hospitals o`en realize a value proposiNon by acquiring the ancillaries and being able to realize greater reimbursement
• There is an emphasis on informaNon technology (IT) integraNon and conNnuity of care; clinical integraNon is primary goal
• LiTle, if any, intangible value is being paid to physicians under current agreements
• Tangible assets and possibly sign-‐on / retenNon bonuses are the norm (at FMV)
• Accountable Care OrganizaNons are being piloted for managing care of Medicare paNents and for reimbursement
NOW
6

7/31/12
3
REASONS FOR ALIGNMENT
Physicians are interested in aligning with hospitals for several reasons
Financial Stability — Improved compensaSon
MalpracSce Insurance – Shared risk
Lifestyle — Improved quality of life
Infrastructure Support — AdministraSve hassles off-‐loaded
PracSce Style – ShiY variances to hospital
Recruitment and RetenSon — Private pracSces cannot compete
Succession Strategy – No “cash-‐out” value in private pracSces
7
CURRENT TRENDS
• Employment of physicians by hospitals is on the rise § 81% of surveyed hospital leaders indicated a moderate to high interest in acquiring pracNces and/or physician employment*
• Outside of employment, numerous other alignment iniNaNves are underway
Key Trend: Stronger collaboraSon between health
systems and physicians/pracSces
8 *Source: HealthLeaders Media-Intelligence; M&A: Hospitals Take Control, January 2012
9
How will you respond to low Medicare/Medicaid Reimbursements?
Source: HealthLeaders Media 2012 Industry Survey: Physician Leaders Report
SURVEY OF HEALTHCARE LEADERS
50%

7/31/12
4
TRENDS • Physician hospital employment increased 34% in 2010, over the previous ten years*
• Hospitals employ about 25% of all acNve physicians*
• 63% of physician recruitment in 2011 was for hospitals, up from 56% the previous year, and 11% eight years ago**
• Family physicians and general internists topped the list of most comment physician recruitments**
Source: *AHA study **Statistics from a Merritt Hawkins 2012 report of their recruiting assignments
TRENDS
11
PROJECTION
Source: Merritt Hawkins Annual 2012 Report
3 in 4 doctors hired in 2014 will work for hospitals
12 Source: HealthLeaders Media-Intelligence; M&A: Hospitals Take Control, January 2012
SURVEY OF HEALTHCARE LEADERS

7/31/12
5
ALIGNMENT MODELS
ALIGNMENT STRATEGIES
Physicians and hospitals face unprecedented challenges to their ability to maintain viability
Partnering alternaNves are without quesNon the best soluNons to respond to these challenging issues and to the new federal themes
Most pracNces (and definitely all hospitals) should assume a pluralisNc approach to alignment
" Merge operaNons " Service sNpends " Clinical co-‐management/service line
management " Different forms of employment/employment
“lite” 14
ALIGNMENT CHALLENGES
15

7/31/12
6
ALIGNMENT MODELS -‐ LIMITED STRATEGY BASIC CONCEPT COMPENSATION FRAMEWORK
Managed Care Networks (IPAs, PHOs)
• Loosely formed alliances • Primarily for contracNng purposes • Limited in ability unless clinically integrated • Being used as a plaiorm for ACO development
• No true impact on pay unless through improved payer contracts • If used as plaiorm for ACO, could result in distribuNon of incenNves received
Call Coverage SSpends
• CompensaNon for the personal, financial and risk burden associated with ED coverage
• Payment can come in the form of a daily sNpend, fee for service payment or hybrid payment
Medical Directorships
• Payment for defined administraNve services • Must be a true need for the services
• Typically paid via a market-‐based hourly rate
Recruitment/IncubaSon
• TradiNonal style of a hospital financially supporNng a new recruit
• Allows exisNng physicians in pracNce to not see a decrease in their pay as a new physician comes on board
16
ALIGNMENT MODELS -‐ MODERATE STRATEGY BASIC CONCEPT COMPENSATION FRAMEWORK
Management Services OrganizaSon (MSO)
• Services such as revenue cycle, human resources, IT, etc. • Can be hospital-‐owned, joint venture, private pracNce owned
• Can provide an addiNonal revenue stream
Equity Model AssimilaSon
• Ties all enNNes via legal agreements • Can jointly contract with payers • May be with a hospital partner; may be with a private group
• Can result in increased profitability through beTer payer contracts and other efficiencies
Target Cost ObjecSves
• Focus to ensure delivery of cost effecNve care while sNll maintaining quality
• Savings shared with providers • Percentage • Hourly fee • Fixed fee
Provider Equity (Joint ventures, investments)
• Joint ventures such as specialty hospitals, surgery centers, etc.
• Can provide an addiNonal revenue stream to private pracNce physicians
Clinical co-‐management/ service line management
• Provision of administraNve services and work toward certain strategic iniNaNves within a service line • May include pay-‐for-‐call, medical directorships, etc.
• Involves hourly payment for administraNve Nme and incenNve payment for achieving established metrics
17
ALIGNMENT MODELS -‐ FULL STRATEGY BASIC CONCEPT COMPENSATION FRAMEWORK
Employment lite (“PSA model”)
• Allows pracNce to remain private, but hedge payer risk • Hospital owns receivables • Hospital owns payer contracts • Contract with pracNce for professional services
• Hospital provides payment, o`en on wRVU basis, which is intended to provide FMV compensaNon, benefits and other overhead costs incurred by pracNce
Employment -‐ TradiSonal
• TradiNonal employment arrangement with a hospital
• Typically includes producNvity payment and potenNally some other incenNves for quality, cost control
Employment – Group PracSce Subsidiary (GPS)
• The larger single or mulNspecialty pracNce operates as a standalone wholly owned subsidiary of the hospital
• Entails a group income distribuNon plan (IDP) wherein enNty dynamics remain at play
18
7/31/12
7
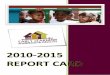
COMPARISON OF ALIGNMENT MODELS
STRATEGY ADVANTAGES DISADVANTAGES Managed Care Networks (IPAs, PHOs)
• Some economic align • Loyalty is to the contracts, not the other party
Call Coverage SSpends
• Can alleviate economic, personal and liability burdens
• Can alleviate economic, personal and liability burdens
Medical Directorships
• Flexible; can include as many physicians as necessary
• Can create poliNcal conflicts; requires physician Nme commitment
Recruitment/IncubaSon
• Flexible as long as there is demonstrated need
• Short-‐lived; no guarantees of loyalty or collaboraNon
19
LIMITED
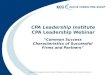
STRATEGY ADVANTAGES DISADVANTAGES Management Services OrganizaSon (MSO)
• Ties hospitals to physicians’ business success
• Costly; can hurt more than help if not done well
Equity Model AssimilaSon
• Ties all enNNes via legal agreements
• Can be difficult to transiNon; requires high level of trust
Target Cost ObjecSves
• Provides economic benefits for hospitals and physicians
• Short-‐lived; takes Nme to implement
Provider Equity (Joint ventures, investments)
• Closely unites parNes under common enterprise
• Costly; challenging to implement and govern; may increase operaNng costs
Clinical Co-‐Management/ Service Line Management
• Strong economic and strategic alignment; somewhat easier to unwind if necessary
• ContracNng potenNally complex; requires strong combined vision and agreement on strategic goals and operaNng principles
20
M0DERATE
COMPARISON OF ALIGNMENT MODELS
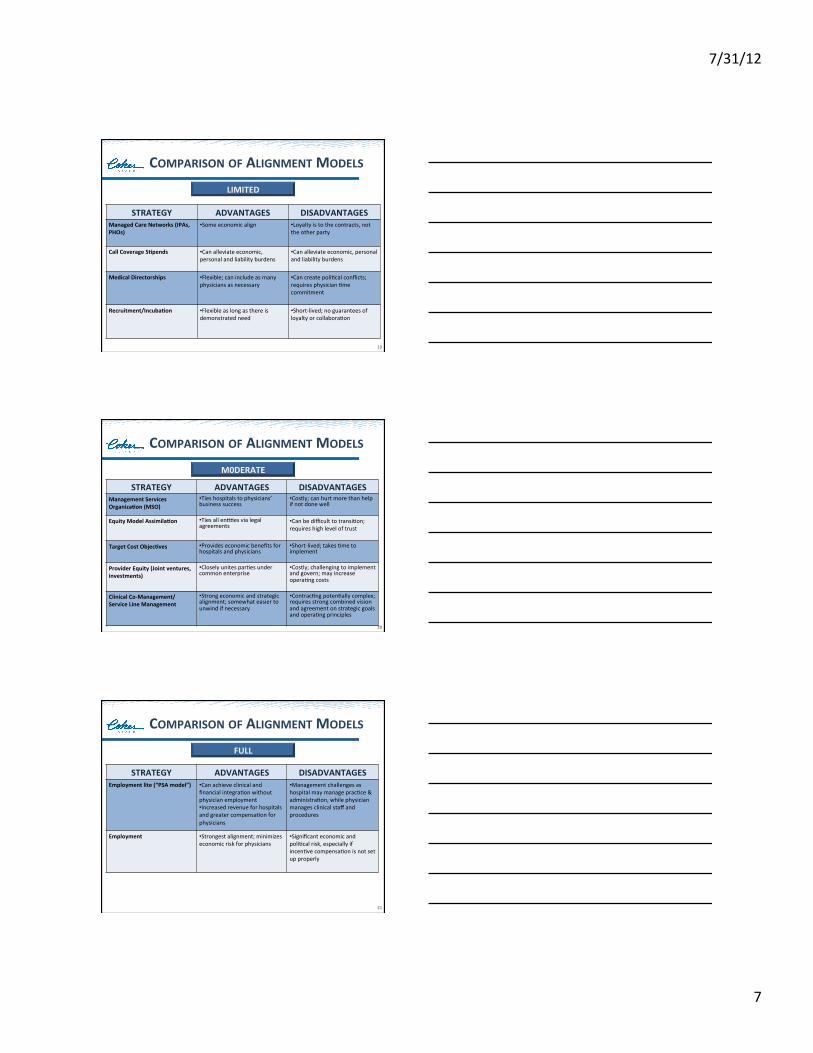
STRATEGY ADVANTAGES DISADVANTAGES Employment lite (“PSA model”)
• Can achieve clinical and financial integraNon without physician employment • Increased revenue for hospitals and greater compensaNon for physicians
• Management challenges as hospital may manage pracNce & administraNon, while physician manages clinical staff and procedures
Employment
• Strongest alignment; minimizes economic risk for physicians
• Significant economic and poliNcal risk, especially if incenNve compensaNon is not set up properly
21
FULL
COMPARISON OF ALIGNMENT MODELS

7/31/12
8
PROCESS FOR PHYSICIAN/HOSPITAL ALIGNMENT
SAMPLE PHASES FOR ALIGNMENT PROCESS
Implement
Develop transiSon plan
DraY definiSve agreements
Finalize leher of intent (LOI)
Develop/modify physician compensaSon plan, if applicable
NegoSate and resolve all issues
DraY term sheet
Conduct financial analysis, if applicable
Discuss alignment opSons
Evaluate situaSon: for both sides
23
SAMPLE TIMELINE
Discussions
Execute LOI
Valuation
24
Discussions
Financial Analysis
Finalized LOI & TransiSon Plan
Dec. Oct. Sept. Aug. July June April March Feb. Jan May Nov.
NegoSaSons
Alignment Implemented & OperaSonal
LOI
7/31/12
9
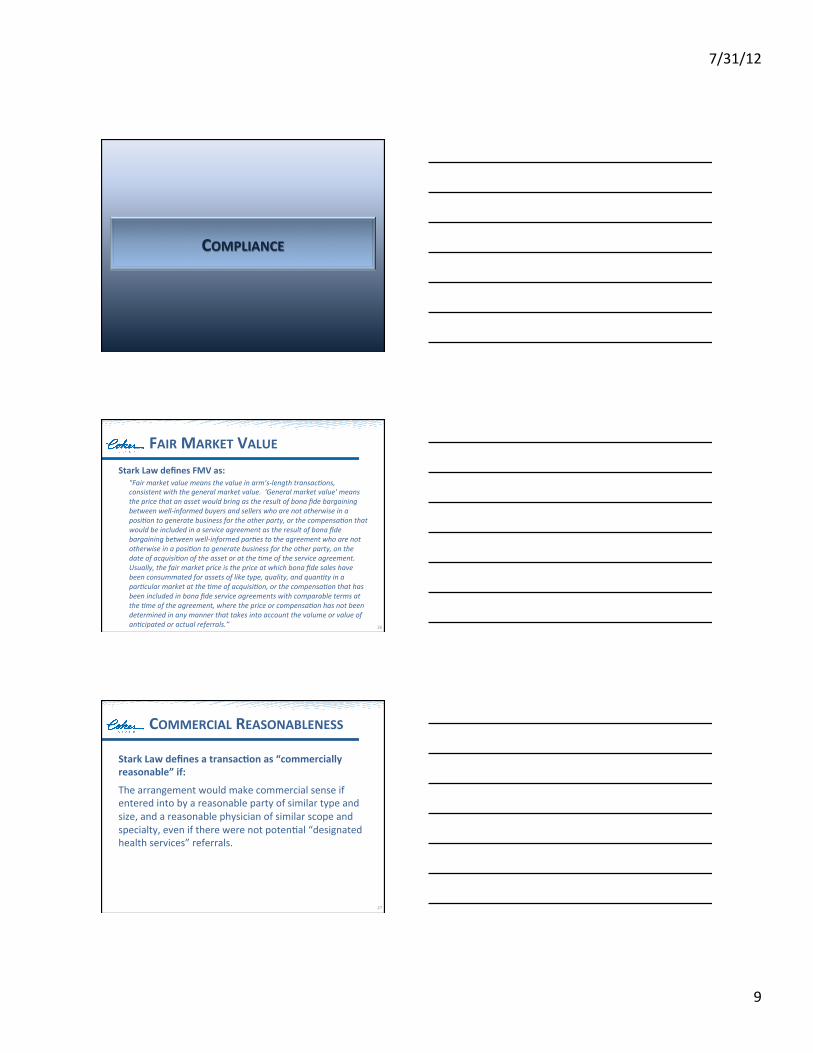
COMPLIANCE
FAIR MARKET VALUE Stark Law defines FMV as:
"Fair market value means the value in arm's-‐length transac5ons, consistent with the general market value. 'General market value' means the price that an asset would bring as the result of bona fide bargaining between well-‐informed buyers and sellers who are not otherwise in a posi5on to generate business for the other party, or the compensa5on that would be included in a service agreement as the result of bona fide bargaining between well-‐informed par5es to the agreement who are not otherwise in a posi5on to generate business for the other party, on the date of acquisi5on of the asset or at the 5me of the service agreement. Usually, the fair market price is the price at which bona fide sales have been consummated for assets of like type, quality, and quan5ty in a par5cular market at the 5me of acquisi5on, or the compensa5on that has been included in bona fide service agreements with comparable terms at the 5me of the agreement, where the price or compensa5on has not been determined in any manner that takes into account the volume or value of an5cipated or actual referrals.” 26
COMMERCIAL REASONABLENESS
Stark Law defines a transacSon as “commercially reasonable” if:
The arrangement would make commercial sense if entered into by a reasonable party of similar type and size, and a reasonable physician of similar scope and specialty, even if there were not potenNal “designated health services” referrals.
27
7/31/12
10
FMV/CR CONCEPTS
• Arrangements subject to FMV/CR:
§ EssenNally, any transacNon wherein money is exchanged between hospitals and physicians
§ Important to understand the FMV risk o Under or overpayment
• Employment • Co-‐management
• Medical directorships • Space/equipment/staff lease • Call coverage • Per click arrangements • Graduate medical educaNon • Contract services • CollecNons guarantees • ConsulNng fees (DME) • Service line management
28
FMV/CR CONCEPTS
• FMV deals with the dollars in the transacNon • CR deals with whether transacNon makes “sense”
§ Business purpose § Overnight increase in pay § Supply/demand § Recruitment efforts
• Growing emphasis on commercial reasonableness • TransacSons can be FMV and NOT CR!
29
FMV/CR CONCEPTS
• Key Areas of Concern: § High guaranteed pay
§ Long contracts, with no ability to adjust variables
§ AdministraNve services with no tracking mechanisms
§ Ill-‐defined non-‐producNvity incenNves
§ Significant increases in pay for no addiNonal work
30

7/31/12
11
FMV/CR CONCEPTS
• Key Areas of Concern: § “Stacked” compensaNon
§ ProducNvity incenNves with rate per wRVU well above median
§ Overall effecNve rate per wRVU at/above 75th percenNle
§ Total pay above 90th percenNle
§ Significant investment per physician
31
FMV/CR CONCEPTS
• Ensuring Compliance § Use common sense (“the sniff test”) § Establish consistent compensaNon methodology where there is confidence that FMV pay will result o PotenNally test for FMV on the compensaNon plan level
§ Establish internal benchmarks that trigger addiNonal levels of review o FMV tests occur on the individual physician level
§ Establish ceilings on pay and the effecNve rate/wRVU o Can be “hard” or “so`”
§ Be conservaNve on what is guaranteed o Less FMV risk when pay is “at risk”
32
IMPACT OF HEALTHCARE REFORM

7/31/12
12
SUMMARY OF IMPACT OF HC REFORM
Ø Provide paNents with greater access to insurance coverage, thus enhancing providers’ ability to increase revenue
Ø Provide some addiNonal payments to certain classificaNons of providers
Ø Mandate coverage to all ciNzens, which could increase provider revenue, but also greatly strain the system due to lack of PCPs
Ø Require addiNonal “paperwork” and other requirements
Ø Penalize some types of providers for failure to meet certain quality requirements or other provisions
34
KEY PROVISIONS FOR PPACA
§ Allow providers organized into accountable care organizaNons (ACOs) who meet thresholds, to share in cost savings they achieve under Medicare program
§ Reduce Medicare payments that would otherwise be made to hospitals as specified percentages to account for excess (and preventable) hospital readmissions
§ Establish value-‐based purchasing program for Medicare and develop plans to implement such programs for SNFs, home health agencies and ASCs
§ Establish naNonal Medicare pilot program to develop bundled payment for acute, inpaNent hospital services, physician services, outpaNent hosp services & post-‐acute care for an episode of care
35
2012 & Beyond -‐ AffecSng Healthcare and Employers
KEY PROVISIONS FOR PPACA
§ Reduce Medicare DisproporNonate Share Hospital (DSH) payments iniNally by 75% and subsequently increase payments based on the percent of uninsured populaNon & amount of uncompensated care provided
§ Increase Medicaid payments for primary care services by PCPs for 2013 & 2014 with federal funding
§ Require enhanced collecNon and reporNng of data on race, ethnicity, sex, primary language, disability status and for underserved rural and fronNer populaNons
§ Require US ciNzens and legal residents to have qualifying health coverage by 2014
36
2012 & Beyond -‐ AffecSng Healthcare and Employers

7/31/12
13
KEY PROVISIONS FOR PPACA
§ Simplify insurance administraNon by adopNng a single set of operaNng rules for eligibility verificaNon and claims status, EFTs, health care payments, remiTance rules, referral cerNficaNon and authorizaNons
§ Impose a 2.3% excise tax on sale of taxable medical devices § Expand Medicaid to all non-‐eligible Medicare individuals with
incomes of up to 133% of federal poverty level § Reduce Medicare payments to certain hospitals by 1% for
hospital-‐acquired condiNons (2015) § CreaNon of accountable care organizaNons
37
2012 & Beyond -‐ AffecSng Healthcare and Employers
ACOS
ACO
38
ACOS
39
CMS Medicare Shared Savings Program
Pioneer Model
Physician or Hospital
Sponsored
Payer Sponsored
Employer Sponsored PRIVATE
7/31/12
14
ACOS Whether CMS or private, all possess the same characterisScs:
40
PaSent-‐centered care
Focus on quality
Focus on coordinated care
Focus on reduced expenses (fewer hospital admissions and fewer ER visits)
More ambulatory & home care services
SHARED SAVINGS PROGRAM (SSP)
• IniNal ACO program introduced by CMS
• Focused to allow any eligible providers to parNcipate
• Two tracks, with Track 1 having no pay-‐back penalty for losses
PIONEER MODEL
• Designed for organizaNons already experienced in managing coordinated paNent care in an ACO-‐type of environment
• Greater incenNve percentages for savings; and sharing of losses
• Quality measures are the same as the SSP
CMS ACOS
CMS SHARED SAVINGS PROGRAM (SSP)
Quality
Cost Benchmarks
Two Tracks Offered
42

7/31/12
15
CMS SSP -‐ QUALITY
4 Domains (categories) – 33 Measures
PaSent/ Caregiver Experience
Care CoordinaSon/PaSent Safety
PrevenSve Health
At-‐Risk PopulaSon
43
-‐Based upon Parts A & B FFS historical claims data for beneficiaries assigned to an ACO
-‐Cost benchmark established for each ACO at a per capita level
-‐If below certain threshold, savings are shared
-‐If over certain threshold, costs must be paid back to CMS (Track 2)
CMS SSP – COST BENCHMARKS
44
CMS SSP:– TWO TRACKS OFFERED
TRACK 1
Shared savings only; no pay back for losses
TRACK 2
Shared savings, but losses must be paid back
45

7/31/12
16
CMS: PIONEER ACO MODEL
• Designed for providers already working in collaboraNve group who have been focused on coordinaNng paNent care
• Program launched January 1, 2012 and runs through December 31, 2014
• CMS limited this pilot program to 32 organizaNons and they project Medicare savings up to $430 million over three years
• Uses same quality metrics as the Shared Savings Program
46
QUESTIONS & ANSWERS
THANK YOU
MAX REIBOLDT, CPA PRESIDENT, CEO
[email protected] 678-‐832-‐2000
www.cokergroup.com

7/31/12
17
APPENDIX
49
LIMITED
• “Loosely” formed alliances
• Primarily for contracNng purposes
• Limited in ability unless clinically integrated
• Normally, no more than a messenger model
• Limited collaboraNve usefulness
MANAGED CARE NETWORKS (IPAS, PHOS)
51

7/31/12
18
• Pay for unassigned ED call • By specialty • Fair market value • Per diem • Per “click” • Fixed sNpend
• Physicians seeing all paNents (paying and non-‐paying), causing them to request addiNonal compensaNon from hospitals
• Other forms of alignment are becoming a reasonable alternaNve
• Most primary care physicians are not subject to these as hospitalist programs saNsfy their needs
CALL COVERAGE STIPENDS
52
MEDICAL DIRECTORSHIPS
Common alternaSve payment arrangement
for a physician’s administraSve duSes associated with their parScular specialty and/or department
Should document hours worked and services provided
Separate from employment compensaSon
contract
Subject to Stark provisions and
corresponding fair market value determinaSons
53
Hospitals provide financial support to newly-‐recruited providers:
• Income guarantees
• TuiNon payments
• IncubaNon • Provider planning (supply/demand)
RECRUITMENT GUARANTEES/INCUBATIONS
54

7/31/12
19
MODERATE
• Management processes provided to pracNces • Revenue cycle • Personnel/human resources • InformaNon technology • Compliance
• MSO ownership • Joint hospital/provider • Hospital only • Private investors
• Strategy to align with providers • Also may be in the form of an ISO
MANAGEMENT SERVICES ORGANIZATION (MSO); OR INFORMATION SERVICES ORGANIZATION (ISO)
56
Business • Physicians and potenSally hospital form NewCo, LLC to provide specific management and administraSve services
• Management Co., LLC hires or leases personnel necessary to provide management services
• Hospital pays Management Co., LLC a fair market management fee for specified management services
• Management fee may be a fixed amount per month of fixed percentage of revenues from service
• Can include performance incenSves
Legal • Management Co., LLC must have demonstrable benefit (cost and/or quality) as compared to alternaSves
• PotenSal anS-‐kickback remains an issue with percentage management fees
• Fee paid must be commercially reasonable
• Must comply with Rev. Proc. 97-‐13
MANAGEMENT SERVICES ARRANGEMENTS BUSINESS/LEGAL DESCRIPTION
57

7/31/12
20
Advantages Disadvantages
Ties all enNNes via legal agreements Governance and voNng can be a challenge
Can jointly contract with payers UNlizaNon of hospital benefits may be more costly
Can jointly develop ancillaries TransiNoning could present some challenges
Joint markeNng strategy would be possible CompensaNon of the providers can be challenging
Aligns interests as to profitability and return on investment
Joint investments will be required, and return on those investments must be dependent upon the individual enNty (no hospital subsidy)
One provider number will be easier to administer
Requires high level of trust
EQUITY MODEL GROUP ASSIMILATION (JOINTLY OWNED PRACTICES)
58
• Program works to ensure delivery of cost effecNve care while sNll maintaining quality and paNent saNsfacNon
• Savings are shared with providers § Percentage payment § Hourly fee § Fixed fee
• Physicians are integral in the planning process to determine how these savings can be actualized
• This model is limited in duraNon § Not meant as a long term alignment soluNon
59
TARGET COST OBJECTIVES
JOINT VENTURES
Structures • Specialty Hospitals • Management Services
Arrangements
• Real estate developments
• Freestanding Centers
• Pay for Performance
• Block Leases
• Medical Directorships
“Laws” to Consider • Stark • AnN-‐Kickback • Reimbursement • Tax ImplicaNons • State Law
60

7/31/12
21
Legally permissible if one of the following is met:
The physicians must contribute 8inancial
capital
The physicians must provide business
expertise The physicians must have
a business risk
JOINT VENTURES
61
CLINICAL CO-‐MANAGEMENT ARRANGEMENT DESCRIPTION
• Purpose of the arrangement is to reward physicians for their efforts in developing, managing and improving the quality and efficiency of a parNcular hospital service line
• A contractual relaNonship between the hospital and the service line management enNty
• CompensaNon is performance based in part, Ned to achievement of specific quality objecNves
62
CLINICAL CO-‐MANAGEMENT ARRANGEMENT DESCRIPTION
Provide medical management services for specific IP or OP
service line
Provide compensaSon at FMV, partly
performance –based, Sed to specific objecSves
Provider(s) Hospital
63

7/31/12
22
CO-‐MANAGEMENT: MODEL A
ExisSng Physician Professional CorporaSon
Hospital (Service Line)
Management Services
Management Fees
Management Agreement
64
EXAMPLE: ORTHOPEDIC SURGERY
ExisSng Physician Professional CorporaSon
Hospital
Clinical Co-‐Management
Agreement for Oversight of Orthopedic Services
Fixed Fee ConNngent Fee
Sports Medicine
Hand
Spine
Management CommiTee RepresentaNves
and Medical Director
Management CommiTee RepresentaNves
65
CO-‐MANAGEMENT: MODEL B
Newly-‐ Created Management EnSty
Physician Ownership
Hospital (Service Line)
Management Services Management Fees Management Agreement
66

7/31/12
23
CO-‐MANAGEMENT: MODEL C
Joint Venture Management
EnSty
Hospital Ownership
Physician Ownership
Hospital (Service Line)
Management Services
Management Fees
Management Agreement
67
CO-‐MANAGEMENT: MODEL D
Joint Oversight CommiTee
Physician Group
Physician Group
Management Agreement between Hospital and Physician Group for a subset of management services and payment of a part of the total service line management fees
Management Agreement between Hospital and Physician Group for a subset of management services and payment of a part of the total service line management fees
Hospital
68
CCMA MANAGEMENT FEES
• Management fees include a base fee and an incenNve fee
• The fee is fixed in advance, including both base and incenNve components, for a period of at least one year
69

7/31/12
24
CCMA BASE FEE
• The base fee is reimbursement for the Nme and efforts parNcipaNng physicians dedicate to the performance of specific management acNviNes
• Commonly, the base fee equals 50-‐70% of the total fee
• The base fee is typically an hourly rate (at FMV) for services provided and documented
70
CCMA INCENTIVE FEE
• The incenNve fee is a series of pre-‐determined payment amounts conNngent on achievement of specific, objecNvely measurable, program development, quality improvement and efficiency goals
• Can incent the reducNon of administraNve or medically unnecessary costs as long as quality is not adversely affected and volume/case mix changes are not rewarded
71
CCMA INCENTIVE FEE
15%
10%
50%
25% PaNent SaNsfacNon
Employee Engagement
Clinical Quality
OperaNng Efficiency
Sample CCMA Incentive Fee Structure
72

7/31/12
25
FULL
FULL ALIGNMENT MODELS
Six Common Models Used by Hospitals for Physician Employment
PSA (professional service agreement) models PracNce management
arrangement
Group or ‘group without walls’
Hospital-‐employed mulN-‐specialty group
Hospital-‐employed specialty pods
Hospital-‐employed network model
EMPLOYMENT “LITE”

7/31/12
26
PROFESSIONAL SERVICES AGREEMENT
• Achieve clinical and financial integraNon without employment
• Contracted services, mulNple opNons
Clinical (Professional) Services
Wraparounds (administraNve, call, quality, etc.)
• Typically paid on a top-‐line basis per wRVU. Wraparounds can take other forms of payment, if included.
76
PURPOSE
RELATIONSHIP
SERVICES
REMUNERATION
PSA – EMPLOYMENT “LITE”
1. Tradi5onal PSA: Hospital contracts with physicians for professional services; hospital employs staff and “owns” administraNve structure
2. Global Payment PSA: Hospital contracts with pracNce for Global Payment; pracNce retains all management responsibiliNes
3. Prac5ce Management Arrangement: PracNce enNty retained and contracts with hospital; administraNve management and staff not employed by hospital
4. Hybrid Model: Hospital employs/contracts with physicians; pracNce enNty spun-‐off into a jointly-‐owned MSO/ISO
FOUR POSSIBLE SCENARIOS OF PSA MODEL
77
PSA – TRADITIONAL MODEL
• Hospital contracts with physicians for professional services
§ As such, the physicians are not employed by the hospital, but remain employed by the pracNce
• However, the hospital employs all support staff § This typically includes pracNce administrators/ management staff
• Under this model, many of the operaNonal and administraNve duNes become the responsibility of the hospital, as opposed to the pracNce
• Ancillaries are usually acquired by the hospital 78

7/31/12
27
DEF Medical Group (“Group”)
Payers ABC Health System
“System”
Real Estate
Group Ancillary Services
OperaSng Expenses
Lease Purchase or Lease
• Independent contractors as a Group
• Group includes all providers • Payment to Group for professional services equal to net collecSons less direct costs paid by System
• Includes site of service differenSal for professional services
• Annual fixed amount to be paid to Group for value of ancillary services
• set in advance • not based on volume of
referrals
• System hospital outpaSent based services
• Ancillary staff are employees of System
• Not always purchased by System, but included in comp via an annual fixed payment to Group set in advance
• Lease paid by System
• Lease expense deducted from professional service revenue to be paid to Group
• Includes: • lease / depreciaSon
expense
• Other direct operaSng expenses
• Deducted from professional service revenue to be paid to Group
Group Staff
• System employees
• Fully loaded expense deducted from professional service revenue to be paid to Group
Independent Contractor
System Employees
System OutpaSent Services
Professional and technical fees
PSA – TRADITIONAL MODEL
79
PSA – GLOBAL PAYMENT MODEL
80
• PracNce is independent contractor
• Physicians sNll “employed” by pracNce
• Self-‐employed status: no benefits from hospital
• PracNce invoices hospital for actual services rendered
§ Usually in wRVUs, converted to dollars
• Hospital pays pracNce directly without any withholding
• Files 1099 with IRS: pracNce responsible for withholding taxes from physician
PSA – GLOBAL PAYMENT MODEL
• CharacterisNcs of employment but stops significantly short of employment
• Comprehensive alignment strategy requiring less integraNon than employment
• Hospital engages pracNce who conNnues to employ physicians to provide comprehensive services through a PSA
§ PracNce is compensated on a global basis § Independent pracNce maintained
81
7/31/12
28
PSA – GLOBAL PAYMENT MODEL
Services to be provided could include: § MulN-‐specialty diagnosNc and procedural services
§ Clinical management and coordinaNon
§ AdministraNve, supervisory teaching and research funcNons
§ Medical directorships
§ Complete service line and clinical co-‐management
§ Call responsibiliNes § Shared cost savings § Quality incenNves
82
PSA – GLOBAL PAYMENT MODEL
• Hospital compensates pracNce for professional fees and other services performed at and for the hospital § Medical directorships, call, service line/clinical co-‐management, etc.
§ Paid at FMV/ commercially reasonable rates • Ancillaries may be sold/leased to hospital who bills at HOPD rates
• Hospital bills at PBR (provider based rates) § This is not a requirement of the model, and in fact, is not always done
83
PSA – GLOBAL PAYMENT MODEL
-‐Accounts receivable owned by hospital
-‐Fee structure established by hospital
-‐Payer contracts negoSated by hospital
-‐PracSce conSnues to perform the billing services for the hospital (at FMV rates)
84

7/31/12
29
PSA – GLOBAL PAYMENT MODEL
• Overhead expenses paid by pracNce
• Hospital provides base fee that should cover all expenses including physician compensaNon*
§ PotenNal for bonuses in addiNon to base fee
§ Ancillary services included (if included in hospital revenue base, must be considered in physicians’ compensaNon, but not directly Ned to same)
85
* At wRVU conversion factor rates, Nered for higher producNon levels, separately calculated by specialty
PSA – GLOBAL PAYMENT MODEL
Global payment rate may: § OpSon One: Include physician compensaNon/benefit expenses and overhead expenses in a single rate/wRVU
§ OpSon Two: Include separate payments for each component o O`en, the overhead component is paid based on a budgeted amount, rather than on an wRVU basis
86
Comp and Benefits
Overhead
Comp and Benefits
Overhead
PSA – GLOBAL PAYMENT MODEL Global Payment Model
Prac5ce Hospital
Real Estate Ownership X
Medical Equipment Ownership (Non-‐Ancillary) X
Medical Equipment Ownership (Ancillary) * *
Employees’ Employer X
Billing Tax ID X
Recipient of Insurance Payments X
Owner of Ancillary Profits/Income * *
Party Responsible for Billing/CollecNons X
Provider of MalpracNce Insurance X
Managed Care ContracNng NegoNaNons X
MD Employment Status X *Depends upon negoNated agreement 87

7/31/12
30
GLOBAL PSA – BENEFITS
§ Physicians maintain independence from hospital
§ Flexibility in structure
§ OpportuniNes to increase and enhance boTom-‐line for both hospital and the pracNce
§ Stability in relaNonship with hospital
88
§ Bonus opportuniNes for excepNonal performance
§ OpportuniNes to expand services together without being fully aligned (i.e., employment)
§ Easy segue to full employment
PSA – GLOBAL PAYMENT EXAMPLE
Hospital (Integrated with
Physician Division Infrastructure) Aggregate
Compensation (Rate per w
RVU)
Clinical Services & Non-compete
Agreement
Asset Ownership/Lease Contracting A/R Owned
Approves Strategy/Finances Oversees Operations/Business Planning Establishes Compensation Principles Achieves Value-Exchange Objectives Is Typically Split 50/50 Between Hospital
and Medical Group
Group Governance Physician Hiring/
Termination Income Distribution Clinical Practice/Quality Malpractice Management and Staffing Billing (3rd-party agent) IT Support
Membership Compensation Hospital Board Medical Group
Board
Management Committee
Medical Group (For-Profit Entity) PSA
89
Medical Group Infrastructure
Ownership
Physicians
Hospital
Employment
Billing/Collections Practice Management
Compensation Benefits
• Physicians retain ownership of their pracNce infrastructure.
• Physicians operate as the managers of the pracNce, providing all administraNve services, space, equipment, and support staff.
• The hospital contracts with the pracNce enNty for these services and pays a fair market value (FMV) fee.
• The compensaNon structure for the employed physicians is a producNvity-‐based system.
• The arrangement can be easily dissolved, as the pracNce enNty stays outside the hospital control structure.
PRACTICE MANAGEMENT ARRANGEMENT
90

7/31/12
31
HYBRID MODEL
HOSPITAL
EMPLOYMENT JOINT OWNERSHIP
Physicians Physicians Physicians Physicians
PRACTICE
MSO/ISO
91
EMPLOYED
Under contract to hospital
Full benefits
Standard employee regulaSons
apply
Employee withholds taxes & social security
Less flexibility; potenSally more job security
EMPLOYED: EMPLOYMENT CONTRACT
93

7/31/12
32
EMPLOYMENT MODELS
Group or “group without walls”
For this type of model, hospital establishes a separate management company
dedicated to managing physician business.
Group or “group without walls”
MSO Ownership
Medical Group
Hospital
Support Services
Compensa=on
Provides: Staffing and Management
ContracNng Billing Managed Care AdministraNon
RecruiNng IT Support
Owns Assets Controls Financials
Provides Infrastructure
Employs Physicians Manages Clinical OperaNon
EMPLOYMENT MODELS
Hospital-‐employed mulN-‐specialty group
This model entails recruiNng and employing physicians under one integrated structure.
EMPLOYMENT MODELS
7/31/12
33
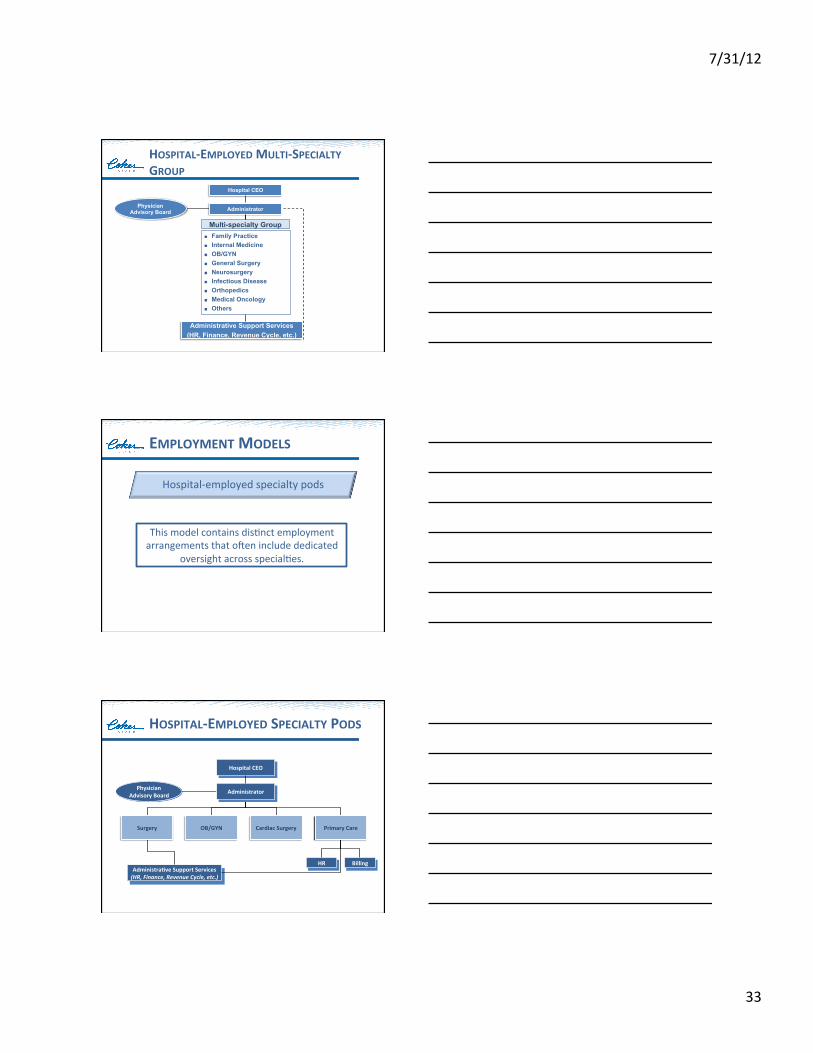
HOSPITAL-‐EMPLOYED MULTI-‐SPECIALTY GROUP
Hospital CEO
Administrative Support Services (HR, Finance, Revenue Cycle, etc.)
Administrator Physician Advisory Board
Multi-specialty Group Family Practice Internal Medicine OB/GYN General Surgery Neurosurgery Infectious Disease Orthopedics Medical Oncology Others
Hospital-‐employed specialty pods
This model contains disNnct employment arrangements that o`en include dedicated
oversight across specialNes.
EMPLOYMENT MODELS
Hospital CEO
AdministraSve Support Services (HR, Finance, Revenue Cycle, etc.)
Physician Advisory Board Administrator
Billing HR
Surgery OB/GYN Cardiac Surgery Primary Care
HOSPITAL-‐EMPLOYED SPECIALTY PODS

7/31/12
34
Hospital-‐employed network model
The network model typically has dedicated oversight but frequently segregates
physicians by service focus.
EMPLOYMENT MODELS
Hospital CEO
AdministraSve Support Services (HR, Finance, Revenue Cycle, etc.)
Dyad Leadership Model Internal Medicine Family PracSce
Pediatrics General Surgery
OB/GYN Urgent Care
MulSspecialty Medical Group Dyad Leadership Model
Cardiac Surgery Emergency Medicine
Endocrinology Gastroenterology
Nephrology Neurology
Pediatric Hospitalists Surgery
Pediatric Network Dyad Leadership Model
Family Medicine Internal Medicine
OB/GYN Surgery
Faculty Physicians Adult Hospitalists Cardiac Surgery
Medical Oncology Neurology
Neurosurgery Orthopedic Surgery Pain Management RadiaSon Oncology
Urgent Care
Adult Specialists
Physician Network CEO
Network Planning
Clinical CoordinaSon
HOSPITAL-‐EMPLOYED NETWORK MODEL