Embed Size (px)
Citation preview

ORIGINAL PAPER
Maxillo-mandibular relationship in untreated and surgicallytreated patients with unilateral complete cleft lip and palate:A cephalometric evaluation
Rohit Khanna & Tripti Tikku & R. K. Mishra &
R. P. Maurya & Sneh Lata Verma & Kamna Srivastava &
Sumit Anand
Received: 13 June 2013 /Accepted: 24 July 2013 /Published online: 27 August 2013# Springer-Verlag Berlin Heidelberg 2013
AbstractBackground Cleft lip and palate is the most frequently en-countered birth defect resulting from an incomplete union ofthe lateral nasal process and maxillary process during devel-opment. A cephalometric assessment was carried out to com-pare the maxillo-mandibular relationship in untreated andsurgically treated patients with unilateral complete cleft lipand palate (UCCLP).Methods This retrospective study included lateral and frontalcephalograms of 100 non-syndromic UCCLP patients ofIndian origin within an age range of 12–20 years, divided into two groups. Group I consisted of 50 untreated UCCLPpatients. Group II consisted of 50 UCCLP patients who hadundergone surgical intervention for cleft lip and palate repairbefore puberty.Results Maxilla in surgically treated patients was found to besignificantly shorter in the anteroposterior and vertical directionalong with retroposition and clockwise rotation with respect tothe cranial base. The mandible was found shorter in length andposteriorly positioned with respect to the cranial base along withdownward and backward rotation in group II patients. Class IIIskeletal pattern was observed in group II patients but was not assevere as anticipated though the maxilla is short andretropositioned because of some compensation being done bythe shorter mandibular length and clockwise rotation of themandible. Measurements on frontal cephalogram showed de-creased maxillary width, nasal height and nasal width in surgi-cally treated cases.
Conclusions The findings of this study suggested that surgicalintervention at early age has significant restraining effect onmaxillary growth that results in class III skeletal relationship/tendency.Level of Evidence: Level IV, therapeutic study.
Keywords Unilateral complete cleft lip and palate .
Non-syndromic .Maxillo-mandibular relationship
Introduction
Cleft lip and palate is the most frequently encountered birthdefect resulting from an incomplete union of the lateral nasalprocess and maxillary process during development. Whiteshave higher rate of occurrence in comparison to blacks whohave the lowest incidence (0.18 to 1.67 per 1,000) [1]. Theincidence of cleft in India is 1 in 500 live births [2]. Completeunilateral cleft lip and palate (UCCLP) accounts for 30 % ofthese births. Cleft lip and palate can be syndromic or non-syndromic.
Factors affecting the craniofacial growth in patients withcleft lip and palate include intrinsic developmental deficien-cies (morbidity) and functional disorders (speech, feeding,respiration). The main long-term effect of postsurgical conse-quences is believed to be due to surgical repair of the cleftincluding the timing and technique to close the defect [3]. Thetiming of closure of the cleft had been a controversial issue.Several attempts have been made in the past to study andcompare the growth pattern as well as functional disordersbetween the surgically unoperated and operated patients withunilateral cleft lip and palate. In a study conducted on adultpersons with unoperated unilateral cleft lip, alveolus andpalate, it was found that they had a normal potential for facialgrowth [4]. Conversely, patients who underwent surgical treat-ment showed growth impairment of the midface due to altered
R. Khanna : T. Tikku : R. P. Maurya : S. L. Verma :K. Srivastava :S. Anand (*)Department of Orthodontics, Babu Banarasi Das College of DentalSciences, Lucknow, Indiae-mail: [email protected]
R. K. MishraBurns and Trauma Centre, Sushrut Institute of Plastic Surgery,Lucknow, India
Eur J Plast Surg (2013) 36:739–748DOI 10.1007/s00238-013-0880-x

functional matrices. On the contrary, in children born withorofacial clefts, speech and voice specialists claim that the firstyear of life is of paramount importance for acquiring speechand language; hence, normal anatomical conditions should bereconstructed in infancy to allow correct kinaesthetic patternsto develop, before compensatory articulations become incor-porated into the speech system [5–7].
Thus, these two diversified issues, i.e. effect on craniofacialgrowth and speech, should be evaluated for accessing the out-come of surgical intervention on UCCLP patients. We are notassessing the functional disorder (speech) in the present study.
This study was aimed to determine the effect of morbidityand long-term effect of postsurgical scarring secondary tosurgical act on maxillo-mandibular relationship by comparingvarious parameters on lateral and frontal cephalogram ofuntreated and surgically treated patients with unilateral com-plete cleft lip and palate.
Materials and methods
This retrospective study included 100 non-syndromic UCCLPpatients of Indian origin with an age range of 12–20 years(mean16.49±2.87 years), with minimum of 12 years of agesince the growth of maxilla is anticipated to be complete by thisage. The subjects thus collected were divided in two groups.Group I consisted of 50 patients (mean age 17.02±2.87 years)with UCCLP with no surgical or orthodontic intervention forthe correction of morbidity. Group II consisted of 50 patients(mean age 15.96±2.87 years) with UCCLPwho had undergonesurgical intervention for cleft lip and palate before puberty, andno orthodontic procedures were carried out thereafter. Writtenconsent was taken from all the patients or their parents, andapproval was also taken from the ethical committee.
The digital lateral and frontal cephalograms of the selectedindividuals were taken on a cephalostat machine from AgfaImaging Systems. The exposure value was set at 70 kV, 8 mAand exposure time of 3 s from a distance of 60 in. from thesource to the midsagittal plane.
All the digital cephalograms were taken with functionalhead positioner, and patients were made to stand in naturalhead position with relaxed lip and teeth in maximumintercuspation. The ear posts were used for correct sidewaysalignment of the patient's head so that the image would besymmetric and undistorted in right–left direction. The digitallateral and frontal cephalograms of the two selected groupswere transferred to Nemotech Digital Imaging software(Nemotech Dental Imaging Systems 2004). After markingthe landmarks accurately, analysis was done with the help ofthe Nemotech software, and data thus obtained were subjectedto statistical analysis.
Linear and angular parameters for all three planes, i.e.sagittal, vertical and transverse planes, were taken to assess
the size, position and orientation of the maxilla, mandible andthe maxillo-mandibular relationship. To maintain the unifor-mity in locating the landmarks, identification of all landmarkswas carried out by the same operator. Seven reference planes(Fig. 1) on lateral cephalogram and two reference planes onfrontal cephalogram (Fig. 2) were taken for the study. All thereference planes used in the study were constructed by theNemotech software. Thirty-one hard tissue parameters onlateral cephalogram (16 linear and 15 angular) (Figs. 3, 4and 5) and 11 hard tissue parameters (6 linear and 5 angular)(Fig. 6) on frontal cephalograms were measured.
Statistical analysis
Mean and standard deviation of all measurements from thedigital frontal and lateral cephalograms of group I and group IIwere recorded and subjected to Student t test to determine thelevel of significance (p) of the parameters amongst the groups.All the parameters were compared between the two groups andgraphically displayed in a box plot (whisker plot) (Figs. 7, 8, 9,10, 11, 12 and 13) which consists of theminimum andmaximumrange values, the upper and lower quartiles and themedian of thedata. One of the major advantages of the box plot is its simplicityof design. Critical information about a distribution of data'ssymmetry and skewness can be quickly expressed.
Measurement reliability
In order to minimise the error in the measurements of theobserver, the lateral and frontal cephalograms of ten patientswere randomly selected, and the values were measured again.Student t test was applied to see the difference amongst thevalues recorded earlier and the values repeated after 20 days.No significant difference was found in any of the randomlyselected parameters.
Results
Table 1 shows overall mean and standard deviation t andp values of the various parameters of group I and group II.Comparison of the mean value of various parameters betweensurgically untreated (group I) and treated (group II) subjectsrevealed a statistically significant difference for maxillary size,position and orientation. Total maxillary length (ANS-PNS)and total midface length (Co-Point A) were found significant-ly shorter (p≤0.001) in surgically treated patients as comparedto untreated UCCLP patients. Anterior maxillary position wassignificantly (p<0.05) behind in group II. SNA (p<0.001) andN┴A┴FH (p<0.05) values were significantly smaller in treat-ed individuals. Vertical positioning when comparing the ante-rior maxilla (N to ANS┴HP) (p<0.05) and posterior maxilla (Nto PNS┴HP) (p>0.001) with respect to the cranial base was
740 Eur J Plast Surg (2013) 36:739–748

significantly shorter in group II, showing cranial positioning ofthe maxilla in treated UCCLP patients. Palatal plane angleshowed significant increase (p<0.05), and inclination angleshowed decrease in value in group II. The anterior maxilla ismore caudally tipped in group II when compared with group I,showing the downward rotation of the maxilla.
For measurements describing mandibular orientation, man-dibular plane and occlusal plane, the angle had higher meanvalue in group II, but again it was not statistically significant(p<0.05).
Mean differences between various parameters measured toevaluate maxillo-mandibular relationship like the A point–nasion–B point (ANB), maxillo-mandibular difference, angleof convexity and WITS were higher up to a statisticallysignificant level (p>0.001) and show that the mandible ismore anteriorly positioned with respect to the maxillary basein group II. For the remaining maxillo-mandibular relation-ship parameters, viz. lower anterior facial height (p>0.05) andbasal plane angle (p>0.05), the mean value of the treatedgroup was lower as compared to that of untreated group, yetthe difference was not significant statistically.
Table 2 shows the measurements obtained from theposteroanterior cephalograms of the untreated and surgicallytreated patients which were subjected to Student t test todetermine the level of significant difference between the ob-servations. The nasal width, nasal height and maxillary widthwere found significantly less (p≤0.001) in surgically treatedpatients (group II) when compared to untreated patients(group I) of UCCLP.
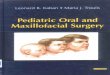
Fig. 2 Landmarks and reference planes used in posteroanteriorcephalogram. (1) Crista galli (Cg). (2) ZR/ZL plane. (3) ZA/AZ plane.(4) NC point. (5) J/J′ point. (6) Antigonial point (AG/GA). (7) A1 point.(8) B1 point. (9) Maximum convexity on maxillary molar (A6). (10)Maximum convexity onmandibular molar (B6). (11) Anterior nasal spine(ANS). (12) Menton (Me). (13) Midsagittal reference plane (MSR). (14)Horizontal reference plane (Hr plane)
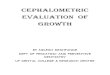
Fig. 1 Landmarks and referenceplane on lateral cephalogram. (1)Nasion (N). (2) Sella (S). (3)Sellion (Se). (4) Porion (Po). (5)Basion (Ba). (6) Pterygomaxillaryfissure (Ptm). (7) Orbitale (Or).(8) Anterior nasal spine (NAS).(9) Subspinale (point A). (10)Posterior nasal spine (PNS). (11)Articular (Ar). (12) Condylion(Co). (13) Gonion (Go). (14)Supramentale (point B). (15)Supra pogonion (PM). (16)Pogonion (Pog). (17) Gnathion(Gn). (18) Menton (Me). (19) Xipoint. (20) True horizontal plane(HP). (21) Sella–nasion plane(S-N plane). (22) Frankfort–horizontal plane (F-H plane). (23)Palatal plane (PP). (24) Occlusalplane (OP). (25) Mandibularplane (Go–Gn) (MP). (26) Truevertical line (TVL)
Eur J Plast Surg (2013) 36:739–748 741

Discussion
Amongst the various factors affecting the craniofacial growthin unilateral complete cleft lip and palate patients, surgicalrepair is believed to be a major factor. The timing and tech-nique for repair of the defect seem controversial. Severalattempts have been made in the past to study and comparethe growth pattern between the surgically unoperated andoperated patients with unilateral cleft lip and palate. Nolletet al [8] reported that delayed palate repair may lead to better
postsurgical craniofacial morphology. Contrary to this,Rohrich et al. [9] and Holland et al. [10] suggested thatdelayed palate repair has no benefit on craniofacial growthor phonetic ability as also reported by Savaci et al. [11], Liaoand Mars [12] and Liao et al. [13]. Children with a history ofcleft palate or submucous cleft are at risk for resonance andspeech problems due to velopharyngeal dysfunction.
The number of samples of treated and untreated patients inalmost all the previous studies was not sufficient, or thecontrol group included normal individuals, i.e. without any
Fig. 4 Mandibular size, position,and orientation. (1) Mandibulararch (DC-Xi-Pm). (2) Corpuslength (Xi-Pm). (3) Co-Gn(McNamara). (4) N–B (II HP). (5)N-Pog (II HP). (6) Facial depthangle. (7) Articular angle. (8)Ramus height (Ar-Go). (9)Mandibular body length(Go-Me). (10) Gonial angle. (11)SNB. (12) Facial Axis. (13)Mandibular plane angle(Burstone). (14) Occlusal planeangle (Ricketts)
Fig. 3 Maxillary size, position,and orientation. (1) SNA (2)N┴A┴ (FH). (3) Posteriormaxillary position. (4) ANS-PNS.(5) Condylion to point A. (6) N-A(II HP). (7) N-ANS (┴HP). (8)N-PNS (┴HP). (9) Inclinationangle. (10) Palatal plane angle
742 Eur J Plast Surg (2013) 36:739–748

Fig. 5 Maxillo-mandibularrelationship. (1) ANB angle. (2)Facial convexity. (3) Basal planeangle. (4) Wits appraisal. (5)Lower facial height (Ricketts). (6)Lower facial height (McNamara)
Fig. 6 Skeletal measurements of posteroanterior cephalogram. (1)Maxillo-mandibular left width (MMLW). (2) Maxillo-mandibular rightwidth (MMRW). (3) Postural symmetry left. (4) Postural symmetry right.(5) Nasal width (NW). (6) Nasal height (NH). (7) Maxillary width(MxW). (8) Mandibular width (MdW). (9) Facial width (FW)
GroupGroup –II
(Surgically treated)
Group -I
(Surgically untreated)
120
100
80
60
40
20
Co-AANS-PNS
Fig. 7 Comparison of maxillary size in group I and group II on lateralcephalogram
Eur J Plast Surg (2013) 36:739–748 743

GroupGroup-II
Surgically treated
Group-I
Surgically untreated
100
80
60
40
20
0
-20
POST MAX POSITIONSNA
N - A - FHN - PNS - HP
N - ANS - HP
N TO A II HP
Fig. 8 Comparison of maxillary position in group I and group II onlateral cephalogram
GroupGroup-II
Surgically treated
Group-I
Surgically untreated
100
80
60
40
20
0
-20
PALATEL PLANE ANGLEINCLINATION ANGLE
Fig. 9 Comparison of maxillary orientation in group I and group II onlateral cephalogram
GroupGroup-II
Surgically treated
Group-I
Surgically untreated
140
120
100
80
60
40
20
0
MAND BODY LENGTHCORPUS LENGTH
MAND ARCHGONIAL ANGLE
Co-GnRAMUS HEIGHT
Fig. 10 Comparison of mandibular size in group I and group II on lateralcephalogram
GroupGroup-II
Surgically treated
Group-I
Surgically untreated
200
150
100
50
0
-50
ARTICULAR ANGLEFACIAL AXIS
SNBFACIAL DEPTH ANGLE
NTO POG II HPNTO B II HP
Fig. 11 Comparison of mandibular position in group I and group II onlateral cephalogram
744 Eur J Plast Surg (2013) 36:739–748

cleft. In order to modify the previous shortcomings, thisretrospective cephalometric study was conducted to determinethe effect of morbidity versus long-term effect of postsurgicalconsequences in all three planes, i.e. sagittal, transverse andvertical planes, amongst untreated and surgically treated pa-tients with unilateral cleft lip and palate.
Maxillary length (ANS-PNS) and total midface length (Co-Point A) showed significant reduction in treated patients (groupII) as compared to group I (Table 1). This suggests that surgeryhas an inhibitory effect on linear sagittal growth of the maxilla.The above findings were in accordance with those of the studyof Ross [3] and Smahel andMullarova [14]. According to studyconducted by Hermann et al. [15] and Shetye [4], there isnormal growth potential for the maxilla of individuals withclefts, and shortening of the maxilla develops due to scar tissueformation which is a consequence of surgical repair. The pre-maxilla was posteriorly positioned with respect to the cranialbase in operated UCCLP patients. The value of posterior max-illary positioning (Schwartz) with respect to the cranial basewas also found to be reduced in surgically operated cases,showing retropositioning of the maxillary base. These changescould be due to the pull effect occurring due to fibrosis causedby the surgical repair of the soft palate. Anterior maxillaryheight (N to ANS┴HP) and posterior maxillary height (N toPNS┴HP) with respect to the cranial base was significantlyreduced in group II, suggestive of the fact that the verticaldescent of the maxilla is also restricted in treated patients.These findings are in accordance with those of previous studiesdone by Doğan et al. [16] that maxillary retrognathism inrelation to the cranial base was attributed to decreasedmaxillarylength, reduced anterior maxillary height and retrusion of theentire maxilla. However, few authors such as Bishara andIversen [17] have suggested no significant difference in maxil-lary position in operated and unoperated patients.
The parameters describing the orientation of the maxilla,like palatal plane angle and inclination angle (Table 1), reflectthe clockwise rotation of maxilla. The rotation of the palatalplane could be the consequence of surgical scar tissue, whichis present in the repaired area which affects the growth patternof the maxilla. The findings are in accordance with those ofSeo et al. [18] and Xu et al. [19].
While comparing the various parameters to assess man-dibular size, position and orientation, only the ramal heightshowed statistically significant reduction in group II pa-tients. Though statistically insignificant, the mandible wasfound to be shorter and clockwise rotated in group II (asdepicted by increased gonial angle, mandibular plane angleand occlusal plane angle). Increased articular angle in sur-gically treated group suggested posterior positioning of themandible with respect to the cranial base. This probably bedue to retropositioned maxillary anterior teeth and scaringof orbicularis oris, which is a circular group of muscle,resulting in a restraining effect on the mandible.
GroupGroup-II
Surgically treated
Group-I
Surgically untreated
50
40
30
20
10
0
OCCLUSAL PLANEINCLINATION
MAND PLANE ANGLE
Fig. 12 Comparison of mandibular orientation in group I and group II onlateral cephalogram
GroupGroup-II
Surgically treated
Group-I
Surgically untreated
150
100
50
0
OCCLUSAL CANTFACIAL WIDTHMAND WIDTH
MAX WIDTHNASAL HEIGHTNASAL WIDTH
POSTURAL SYMMETRY RIGHT
POSTURAL SYMMETRY LEFT
MAX MAND MIDLINEMAX - MAND RIGHTMAX - MAND LEFT
Fig. 13 Comparison between group I and group II on frontal cephalogram
Eur J Plast Surg (2013) 36:739–748 745

Assessment of maxillo-mandibular relationship showed(Table 1) significantly reduced values of ANB angle, WITSand angle of convexity in group II, indicating tendencytowards class III skeletal relation. The maxillo-mandibulardifference (McNamara) was significantly higher in group IIpatients, again suggesting class III tendency. That maybe attributed to surgical intervention which affects thestretching of muscular fibres of the orbicularis oris, resultsin a restraining effect on the maxilla as well as the mandi-ble. It was observed that there was restricted mandibulargrowth, though statistically insignificant in addition to the
retrusion and retroposition of the maxilla. The studies bySeo et al. [18] had also demonstrated that there is a likeli-hood of class III jaw relationship in treated patients. Basalplane angle showed insignificant increase in group II thatcould be due to downward and backward rotation of themaxilla as well as the mandible. Though statistically insig-nificant, the mean value of the anterior lower facial heightwas decreased in group II patients despite of the downwardand backward rotations of the mandible. This could beattributed to reduction in the vertical descent of the maxillafrom the cranial base.
Table 1 Comparison between group I and group II on lateral cephalogram
Variable Surgically untreatedgroup I (n=50)
Surgically treatedgroup II (n=50)
Statistical significance
Mean SD Mean SD Student's t p value Level
Maxillary size Maxillary length (ANS-PNS) (Schwartz) 47.39 4.77 43.01 5.54 4.237 0.000 ***
Total midface (Co-A) (McNamara) 83.61 6.88 78.61 8.34 3.270 0.001 **
Maxillary position N to A II HP (Burstone) 5.09 5.87 8.45 6.97 −2.607 0.011 *
N to ANS┴HP (Burstone) 45.93 4.01 43.75 5.18 2.353 0.021 *
N to PNS┴HP (Burstone) 54.07 5.77 49.57 6.91 3.535 0.001 ***
N┴A┴FH (McNamara) −1.23 4.27 −3.24 5.09 2.139 0.035 *
SNA (Steiner) 81.1 4.54 77.01 5.85 3.906 0.000 ***
Posterior maxillary position (Schwartz) 18.35 3.44 16.9 3.72 2.024 0.046 *
Maxillary orientation Inclination angle (Schwartz) 87.09 3.14 85.55 3.01 2.505 0.014 *
Palatal plane angle −0.428 4.71 1.806 4.63 −2.392 0.019 **
Mandibullar size Ramus height (Jarabak) 44.90 6.41 42.44 4.85 2.164 0.033 *
Total mandibular length Co-Gn (McNamara) 107.42 9.10 104.91 9.78 1.329 0.187 NS
Gonial angle (Jarabak) 124.89 7.68 125.69 8.55 −0.492 0.624 NS
Mandibular arch (Ricketts) 34.58 6.66 33.32 6.46 0.960 0.339 NS
Corpus length (Ricketts) 64.72 6.25 64.27 5.92 0.370 0.712 NS
Mandibular body length (Jarabak) 65.29 6.14 64.32 6.62 0.760 0.449 NS
Mandibular position N to B II HP (Burstone) 9.23 9.20 9.30 13.70 −0.030 0.976 NS
N to POG II HP (Burstone) 6.81 7.74 7.06 12.10 −0.123 0.902 NS
Facial depth angle (Ricketts) 85.20 3.76 84.89 4.46 0.376 0.708 NS
SNB (Steiner) 77.23 4.21 77.16 3.72 0.088 0.930 NS
Facial axis (Ricketts) 88.36 5.06 87.97 6.06 0.349 0.728 NS
Articulare angle (Jarabak) 141.81 8.69 143.30 7.44 −0.921 0.359 NS
Mandibular orientation Mandibular plane angle (Burstone) 26.91 10.00 27.70 6.76 −0.463 0.645 NS
Occlusal plane angle (Ricketts) 22.65 6.08 22.86 6.57 −0.166 0.869 NS
Maxillo-mandibular relation Lower facial height (McNamara) 46.85 5.75 46.68 6.82 0.135 0.893 NS
ANB (Reidel) 3.93 3.66 −1.05 4.51 6.063 0.000 ***
Maxillo-mandibular difference (McNamara) 23.51 6.55 26.31 7.04 −2.29 0.030 *
LAFH (Ricketts) 66.14 7.83 63.83 6.76 1.588 0.116 NS
Basal plane angle 24.46 7.72 25.16 8.63 −0.427 0.670 NS
Angle of convexity (Downs) 2.85 7.77 −0.88 8.78 3.186 0.002 **
WITS 2.92 4.83 −0.64 4.95 3.645 0.000 ***
NS not significant at p>0.05
*p<0.05 (just significant); **p<0.01 (significant); ***p≤0.001 (highly significant)
746 Eur J Plast Surg (2013) 36:739–748

Knowledge concerning the effect of surgery on the trans-verse growth of craniofacial morphology in cleft lip and palateis still incomplete [20]. Hence, for multidirectional assessmentof growth in untreated and surgically treated UCCLP patients,several parameters in transverse and vertical planes were alsoevaluated on frontal cephalogram (Table 2).
The significant reduction was observed in nasal width,nasal height and maxillary width in group II (Table 2). Thiscould be attributed to the formation of fibrous scar tissue in thepalatal region which has a significant restraining effect on thetransverse maxillary growth [21, 22].
No significant difference was found in linear measurementsof the remaining parameters. These finding suggest that re-stricted maxillary growth has minimal effect on other cranio-facial structures [20]. Though statistically insignificant, thedifference for maxillo-mandibular midline that showed moredeviation in surgically untreated patients may be due to anabnormal force exerted by the lip, cheek and tongue musclecausing movement of the premaxilla away from the midline.Similar findings were observed in the study conducted byMolsted and Dahl [23].
According to speech and voice specialists, the first year of lifeis of paramount importance for acquiring speech and language,and that this must be considered when planning primary surgeryin children born with cleft lip and/or palate. The proponents ofearly closure of cleft for proper development of speech suggestusing less traumatic surgical techniques to reduce the impairmentof maxillary growth resulting from extensive soft tissue damageand secondary circulatory disturbances. Hence, the effect ofdifferent surgical techniques on craniofacial growth and speechcan form a scope for further research. To confirm the results ofthis study, further studies should be conducted on larger sample
size to evaluate the effect on craniofacial growth as well asfunctional problems like speech.
To conclude, the findings of this study suggested that therestraining effect on the maxilla, mandible and their maxillo-mandibular relationship is due to an altered functional matrix,resulting from the formation of scar tissue in the lip and palateregions as a consequence of surgical intervention.
Conclusions
The following conclusions can be drawn from the results ofthe study:
1. The maxilla is most affected by early surgical interventionin group II. The maxilla was significantly shorter andretropositioned with respect to the cranial base along withreduced vertical maxillary height. The orientation of themaxilla showed clockwise rotation in surgically treatedpatients.
2. The mandible was also restrained as the ramal heightshowed statistically significant reduction in group II.Even the mandible was shorter in length and posteriorlypositioned with respect to the cranial base with downwardand backward rotation in group II patients, the differencewas statistically insignificant.
3. There was a tendency towards class III jaw relationship ingroup II patients, but it was not severe despite of the shortand retropositioned maxilla, as some compensation wasbeing done by the shorter and clockwise-rotated mandible.
4. The maxillary width, nasal height and nasal width werereduced in surgically treated patients.
Table 2 Comparison of group I versus group II on posteroanterior cephalogram
Variable Group I (n=50) Group II (n=50) Statistical significance
Mean SD Mean SD Student's t p value Level
Maxillo-mandibular left 10.01 2.86 10.92 2.15 −1.798 0.075 NS
Maxillo-mandibular right 9.59 2.80 10.53 2.53 −1.761 0.081 NS
Maxillo-mandibular midline 0.75 2.84 0.68 2.28 0.126 0.263 NS
Postural symmetry left 15.13 3.21 15.11 3.70 0.029 0.977 NS
Postural symmetry right 14.82 4.10 14.95 4.42 −0.786 0.434 NS
Nasal width 39.99 4.76 37.2 4.46 3.386 0.001 ***
Nasal height 39.60 4.86 34.90 4.6 4.966 0.000 ***
Maxillary width 66.34 6.34 62.926 4.78 3.046 0.003 **
Mandibular width 80.16 7.59 80.78 6.60 −0.436 0.664 NS
Facial width 124.53 11.73 124.07 12.25 0.192 0.848 NS
Occlusal cant −0.52 2.60 −0.02 1.93 −1.092 0.278 NS
NS not significant at p>0.05
*p<0.05 (just Significant); **p<0.01 (significant); ***p≤0.001 (highly significant)
Eur J Plast Surg (2013) 36:739–748 747

Conflict of interest None
References
1. Vanderas AP (1987) Incidence of cleft lip, cleft palate, and cleft lipand palate among races: a review. Cleft Palate J 24:216–225
2. Ankola AV, Nagesh L, Hedge P, Karibasappa GN (2005) Primarydentition status and treatment needs of children with cleft lip and/orpalate. J Indian Soc Pedod Prev Dent 23:80–82
3. Ross RB (1987) Treatment variables affecting facial growth in com-plete unilateral cleft lip and palate. Cleft Palate J 24(1):5–77
4. Shetye PR (2004) Facial growth of adults with unoperated clefts. ClinPlast Surg 31:361–371
5. Malek R, Martinez H, Mousset MR, Trichet C (1990)Multidisciplinary management of cleft lip and palate in Paris,France. In: Bardach J, Morris HL (eds) Multidisciplinary manage-ment of cleft lip and palate. Saunders, Philadelphia, p 1e10
6. Estrem T, Broen P (1989) Early speech production of children withcleft palate. J Speech Hear Dis 32:12e23
7. O'Gara MM, Logemann JA, Rademaker AW (1994) Phonetic fea-tures by babies with unilateral cleft lip and palate. Cleft PalateCraniofac J 31:446e51
8. Nollet PJ, Katsaros C, Huyskens RW, Borstlap WA, Bronkhorst EM,Kuijpers-Jagtman AM (2008) Cephalometric evaluation of long-termcraniofacial development in unilateral cleft lip and palate patientstreated with delayed hard palate closure. Int J Oral Maxillofac Surg37(2):123–130
9. Rohrich RJ, Rowsell AR, Johns DF, DruryMA, Grieg G,WatsonDJ,Godfrey AM, Poole MD (1996) Timing of hard palatal closure: acritical long-term analysis. Plast Reconstr Surg 98:236–246
10. Holland S, Gabbay J, Justin H, O'hara C, Hurwitz D, Matthew F et al(2007) Delayed closure of the hard palate leads to speech problems anddeleterious maxillary growth. Plast Reconstr Surg 119:1302–1310
11. Savaci N, Hosnuter M, Tosun Z, Demir A (2005) Maxillofacialmorphology in children with complete unilateral cleft lip and palatetreated by one-stage simultaneous repair. Plast Reconstr Surg115:1509–1517
12. Liao Y-F, Mars M (2005) Long-term effects of palate repair oncraniofacial morphology in patients with unilateral cleft lip andpalate. Cleft Palate Craniofac J 42(6):594–600
13. Liao YF, Mars M (2006) Hard palate repair timing and facial growthin cleft lip and palate: a systematic review. Cleft Palate Craniofac J43(5):563–570
14. Smahel Z, Müllerová Z (1994) Facial growth and development inunilateral cleft lip and palate during the period of puberty: compari-son of the development after periosteoplasty and after primary bonegrafting. Cleft Palate Craniofac J 31(2):106–115
15. HermannNV, Darvann TA, Jensen BL, Dahl E, Bolund S, Kreiborg S(2004) Early craniofacial morphology and growth in children withbilateral complete cleft lip and palate. Cleft Palate Craniofacial J41(4):424–438
16. Doğan S, Onçağ G, Akin Y (2006) Craniofacial development inchildren with unilateral cleft lip and palate British. J OralMaxillofac Surg 44(1):28–33
17. Bishara SE, Iversen WW (1974) Cephalometric comparisons on thecranial base and face in individuals with isolated clefts of the palate.Cleft Palate J 11:162–175
18. Seo YJ, Park JW, Kim YH, Baek SH (2011) Initial growth pattern ofchildren with cleft before alveolar bone graft stage according to clefttype. Angle Orthod 81(6):1103–1110
19. Xu X, Zheng Q, Lu D, Huang N, Li J, Li S, Wang Y, Shi B(2012) Timing of palate repair affecting growth in completeunilateral cleft lip and palate. J Craniomaxillofac Surg40(8):e358–e362
20. Dahl E (1979) Transverse maxillary growth in combined cleft lip andpalate. A longitudinal roentgencephalometric study by the implantmethod. Cleft Palate J 16(1):34–41
21. Dahl E, Kreiborg S, Jensen BL, Fogh-Andersen P (1982)Comparison of craniofacial morphology in infants with incom-plete cleft lip and infants with isolated cleft palate. CleftPalate J 19(4):258–266
22. Motohashi N, Kuroda T, Filho LC, Freitas JDS (1994) P-A cephalo-metric analysis of nonoperated adult cleft lip and palate. Cleft PalateCraniofac J 31(3):193–200
23. Molsted K, Dahl E (1990) Asymmetry of the maxilla in children withcomplete unilateral cleft lip and palate. Cleft Palate J 2(2):184–192
748 Eur J Plast Surg (2013) 36:739–748