Embed Size (px)
Citation preview

Page 1 of 5
Short communication
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Valentini P, Hadchiti W, Abensur D, Testori T, Herman P. Maxillary sinus grafting: A proposal for avoidance of postoperative complications. Annals of Oral & Maxillofacial Surgery 2013 Aug 01;1(3):23. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Impl
anto
logy Maxillary sinus grafting: A proposal for avoidance of
postoperative complicationsP Valentini1*, W Hadchiti2, D Abensur1, T Testori3, P Herman4
AbstractIntroductionAccording to the literature, it is well known that the occurrence of post-operative sinusitis, in conjunction with maxillary sinus graft, appears to be limited to patients with a predis-position for this. In order to prevent post- and also intraoperative compli-cations, it is essential to be able to be precise in anatomical particularities and to diagnose the health status of maxillary sinus prior the grafting procedure. A team approach gather-ing the implant surgeon and the ENT specialist to identify those parame-ters is crucial for the patient selection and the prevention of complications. The aim of this short communication was to discuss a proposal for avoid-ance in postoperative complications in maxillary sinus grafting.Short communicationPrevention of complications is essen-tial for the success of the procedure. A strict protocol must be implement-ed for patient selection in order to prevent complications. ConclusionThe team approach gathering the im-plant surgeon and the ENT specialist is essential for outcome of the procedure.
IntroductionNowadays, the lateral approach for maxillary sinus grafting has become a routine technique that allows to ob-tain a long-term implant survival rate over 96%1–3 the maxillary posterior region.
However, this technique can give way to complications that can impact on the short- and long-term implant survival rate. They can be classified into two categories— intraopera-tive complications and postoperative complications that are, mostly infec-tious complications”.
The first category includes dam-age of the alveolo-antral artery and perforations of the sinus mem-brane. Their frequency is inversely proportional to the surgeon’s skill and they have no influence on im-plant survival, if they are properly managed4.
The second category includes in-fectious complications that occur in the form of chronic or acute sinusi-tis. Their frequency ranges from 3 to 5%5–7.
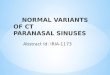
They can result from an inade-quate management of intraoperative complications, or from a poor evalu-ation of the sinus pathology before surgery. In both cases, they may have severe consequences (Figure 1).
According to Timmenga et al., postoperative sinusitis seems to oc-cur only in patients with a specific predisposition for this type of pa-thology.
Therefore, it is essential to be able to identify the pathologies or the spe-cific anatomical variations leading to this predisposition. The aim of this article was to discuss ways to avoid postoperative complications in max-illary sinus grafting.
Short communicationThe authors have referenced some of their own studies in this short communication. These referenced studies have been conducted in accordance with the Declaration of Helsinki (1964), and the protocols of these studies have been approved by the relevant ethics committees re-lated to the institution in which they were performed. All human subjects, in these referenced studies, gave informed consent to participate in these studies.
Before performing any maxillary sinus graft in order to place implants, it is important to be able to answer two questions:
1. Is the sinus to be grafted healthy or not?
2. If the sinus is healthy, is there any infectious risk after grafting?
Is the sinus to be grafted healthy or not? Lateral window procedure, although performed with the utmost sterility of the surgical field, may neverthe-less bring some bacteria from the oral flora inside the sinus in case of tearing of the sinus membrane. In a normal sinus, those bacteria will be trapped in the gel phase of the mucus and propelled through the natural ostium of the sinus by the mucocili-ary clearance. Therefore, risk is mini-mal as soon as the sinus ostium is patent and the mucociliary clearance is preserved.
Conversely, the presence of bacte-ria inside the sinus may contaminate the bed of the graft during the eleva-tion of the sinus membrane.
Since sinus opacities are frequent-ly observed on CT scan prescribed
* Corresponding Author E-mail: [email protected] Institute of Health, Department of Oral Im-
plantology Tattone Hospital, University of Corsica Pasquale Paoli, Corte, France
2 Department of Periodontology, Rothshild Hospital, AP-HP, Paris 7 - Denis Diderot Uni-versity, Paris, France
3 Istituto Ortopedico Galeazzi, Section of Im-plant Dentistry and Oral Rehabilitation, Uni-versity of Milan, Italy
4 Professor and Head Department of Ear, Nose and Throat, Lariboisière Hospital, Paris 7 - Denis Diderot University, Paris, France

Page 2 of 5
Short communication
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Valentini P, Hadchiti W, Abensur D, Testori T, Herman P. Maxillary sinus grafting: A proposal for avoidance of postoperative complications. Annals of Oral & Maxillofacial Surgery 2013 Aug 01;1(3):23. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
If the sinus is healthy, is there any infectious risk after grafting? The answer to this question requires being able to anticipate the outcome of the sinus physiology following the grafting procedure. There are some local and general factors that may lead to postoperative infectious com-plications.
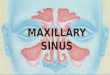
The first factor is anatomical and may affect the drainage pathway through the middle nasal meatus. Any sinus surgery entails oedema of the sinus membrane, which may lead to the ostium stenosis if the natu-ral ostium is particularly narrow. Likewise, the presence of a concha bullosa (Figure 3), which is a pneu-matization of the middle turbinate, may reduce the width of the drain-age pathway. Although the level of evidence is slow8, this may allow, in case of an undetected perforation of the sinus membrane, the granules originating from the graft material to remain trapped inside the ostium (Figure 3).
Then, an antrostomy should ur-gently be performed in order to pre-serve the graft and the implants as
indirectly point at disease inside the sinus. Likewise, polyps may be ob-served in the case of nasal polyposis. On the other hand, the implantologist will analyse with the radiologist the status of the remaining teeth if any, in order to eliminate sinusitis of dental origin.
In case of mucosal disease, the aim of the treatment is to restore muco-ciliary clearance and ostium patency. Medical treatment may adequately restore physiological conditions, such as local or even systemic ster-oids in the case of moderate nasal polyposis, or prolonged antibiotics in case of bacterial sinusitis. How-ever, an antrostomy may be required when this treatment fails or in the case of aspergilloma.
Caution is needed when bacterial sinusitis is related to one tooth and sinus ostium is blocked. Extraction of the causal tooth may allow sinus em-pyema to drain through the alveolar socket, which may result in an oro-antral communication. In such condi-tion, antrostomy may be advised be-fore the extraction in order to avoid this complication.
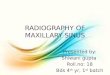
by the implantologist, the main issue is to determine whether they result from a pathology placing the graft at risk (Figure 2). In other words, are those opacities related to benign process such as transient inflamma-tion, as in the course of acute rhinitis, which may heal spontaneously, or to mucous cysts? Alternatively, are they caused by chronic infection, as in the case of aspergilloma, or bacterial si-nusitis possibly of dental origin, or by sustained inflammation as in the course of nasal polyposis? All those conditions will place the patient at risk for the procedure.
In order to solve this problem, it is mandatory for the implantologist to collaborate with an ENT specialist8,9 who will confront patient medical history with the data of the endo-scopic examination. The ostium, that is the natural drainage pathway of the maxillary sinus, may not be directly observed during endoscopy since it is hidden by the uncinate process. However, examination of the middle nasal meatus, the space located un-der the middle turbinate, may allow detecting oedema or secretions that
Figure 1: Oro-antral communication.Figure 2: CT scan of Figure 1.

Page 3 of 5
Short communication
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Valentini P, Hadchiti W, Abensur D, Testori T, Herman P. Maxillary sinus grafting: A proposal for avoidance of postoperative complications. Annals of Oral & Maxillofacial Surgery 2013 Aug 01;1(3):23. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
ide, mometasone) 2 days before and 10 days after surgery.
Mucous cysts are frequently de-tected on CT, which do not require a specific surgery since they are nonsymptomatic and frequently disappear spontaneously. However, at the time of grafting, surgery ele-vation of the sinus membrane might impact the mucous cyst in the sinus ostium and occlude the drainage pathway. This is why it is suggested to drain this cyst at the time of the grafting surgery, by puncture per-formed through the lateral window with an insulin syringe. The second factor is tooth related. In the same way as for the mucous cyst, the presence of endodontic paste rem-nants inside the sinus cavity may be particularly dangerous because they can induce an aspergilloma10. It then becomes imperative to have it removed by the ENT specialist be-fore surgery.
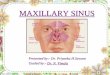
The preservation of some teeth may be at risk11 as illustrated through the following clinical case. In 1992, a female patient underwent a grafting procedure of her maxil-lary left sinus with the simultaneous insertion of two implants in posi-tion 25 and 26. In 2004, she lost the two implants and her bridge as well (Figure 4). The CT scan revealed the cause of the infection (Figure 5). The upper first left premolar sup-porting an iatrogenic prosthetic res-toration was cracked, which led to a chronic infection of the graft and the implant loss.
To prevent this type of compli-cation, the surgeon must be able to identify the teeth at risk and to provide them with an adequate en-dodontic treatment. For a perfect endodontic diagnosis, the CT scan may be a precious tool. However, the teeth will have to be extracted, if the endodontic or prosthetic prognosis remains doubtful.
The last possible factor able to induce infectious complications is a systemic factor. The two follow-
Figure 3: Residues of graft blocked in the meatus (left arrow) causing an acute sinusitis. The concha bullosa (right arrow).
Figure 4: Intraoral situation after the loss of the implants 25 and 26.
well. Some advocate preventing this type of complication by a minimal and functional endonasal surgery.
Similarly, in order to reduce the membrane oedema, it may be wise to prescribe local corticoids (budeson-

Page 4 of 5
Short communication
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Valentini P, Hadchiti W, Abensur D, Testori T, Herman P. Maxillary sinus grafting: A proposal for avoidance of postoperative complications. Annals of Oral & Maxillofacial Surgery 2013 Aug 01;1(3):23. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
left side. The clinical examination revealed a severe oedema but no in-fectious symptoms. The patient said he had been sneezing 30 to 40 times due to a pollen allergy. Despite the recommendations to sneeze with an open mouth, buccal dislodged frag-ment of the graft was revealed when a CT scan was performed on emer-gency (Figure 6).
Following the ENT’s recommenda-tion, antibiotics were immediately prescribed using second-generation quinolones (Levoflaxin), and the patient was operated the next day. After elevating a flap, the dislodged fragments of the main graft were eliminated using a curette, the sta-bility of the implants was checked and the site was rinsed using buc-cal iodine. The graft was completed with a new layer of biomaterial, and then covered with a collagen mem-brane soaked with buccal iodine. The CT scan performed 4 months later shows a perfect healing of the graft (Figure 7). So, obviously, it is pref-erable to avoid surgeries for such patients at springtime and during summer.
The second patient is a totally eden-tulous 63-year-old female who re-ceived a bilateral sinus lift procedure and graft in March. A control CT scan reveals a very poor quality of the graft with central lacunae (Figure 8). When questioned, the patient admitted she had forgotten to inform that she was treated with Alendronate (Fosamax®) since 8 years, which may explain the poor results obtained. Therefore, pa-tients treated with bisphosphonates over a long period of time will have to be excluded, even if these medications are taken orally.
DiscussionThe maxillary sinus grafting tech-nique using a lateral approach is a reliable and predictable technique.
In this aim, case selection must be very strict in order to prevent any complication. Therefore, a pre-operative CT scan or cone beam ex-
Figure 5: Fistula (arrow) in relation with tooth 24.
Figure 6: Dislodged buccal fragment of the graft.
ing clinical cases will illustrate this point.
A 68-year-old male patient un-derwent a maxillary left sinus eleva-tion procedure with simultaneous
grafting and implant placement dur-ing the month of April. Ten days after the surgery, he self-referred to the emergency department complain-ing about significant pain on the

Page 5 of 5
Short communication
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Valentini P, Hadchiti W, Abensur D, Testori T, Herman P. Maxillary sinus grafting: A proposal for avoidance of postoperative complications. Annals of Oral & Maxillofacial Surgery 2013 Aug 01;1(3):23. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
al rates for implants placed in the grafted sinus. Int J Periodontics Restorative Dent. 2004 Dec;24(6):565–77.2. Valentini P, Abensur DJ. Maxillary si-nus grafting with anorganic bovine bone: A clinical report of long-term results. Int J Oral Maxillofac Implants 2003 Jul–Aug;18(4):556–60.3. Wallace SS, Froum SJ. Effect of maxil-lary sinus augmentation on the survival of endosseous dental implants. A sys-tematic review. Ann Periodontol. 2003 Dec;8(1):328–43.4. Schwartz-Arad D, Herzberg R, Dolev E. The prevalence of surgical complications of the sinus graft procedure and their im-pact on implant survival. J Periodontol. 2004 Apr;75(4):511–6.5. Bhattacharyya N. Bilateral chronic maxillary sinusitis after the sinus lift procedure. Am J Otolaryngol. 1999 Mar–Apr;20(2):133–5.6. Levin L, Herzberg R, Dolev E, Schwartz-Arad D. Smoking and complications of onlay grafts and sinus lift operations. Int J Oral Maxillofac Implants 2004 May–Jun;19(3):369–73.7. Timmenga NM, Raghoebar GM, Boer-ing G, Van Weissenbruch R. Maxillary sinus function after sinus lifts for the in-sertion of dental implants. Int J Oral Max-illofac Surg. 1997 Sep;55(9):936–9.8. Cote MT, Segelnick LS, Rastogi A, Schoor R. New York State ENT Specialists ‘Views on Pre Sinus Lift Referral’. J Peri-odontol. 2011 Feb;82(2):227–33.9. Torretta S, Mantovani M, Testori T, Cappadona M, Pignataro L. Impor-tance of ENT assessment in stratify-ing candidates for sinus floor eleva-tion: a prospective clinical study. Clin Oral Implants Res. 2013 Aug;24 Suppl A100:57–62.10. Nicolai P, Lombardi D, Tomenzoli D, Villaret AB, Piccioni M, Mensi M, et al. Fungus ball of the paranasal sinuses: experience in 160 patients treated with endoscopic surgery. Laryngoscope 2009 Nov;119(11):2275–9.11. Greenstein G, Cavallaro J, Jr. Manage-ment of a perplexing sinus lift compli-cation. J Periodontol. 2010 May;81(5): 776–82.
Figure 8: Bilateral osteonecrosis after bisphosphonates treatment.
Figure 7: Healing 4 months later.
amination and a perfect knowledge of the patient’s medical history are essential. The close team approach between the implantologist and the ENT remains the key to success.
ConclusionThe maxillary sinus grafting proce-dure using lateral aproach is a reli-able and predictable technique. How-ever, case selection must be strict to
prevent complications. Therefore, a pre-operative CT scan or cone beam as well a perfect knowledge of the patient medical history are essential. A close team approach between the implantologist and the ENT remains the key for success.
References1. Del Fabbro M, Testori T, Francetti L, Weinstein R. Systematic review of surviv-