Embed Size (px)
Citation preview

Corporate Presentation - November 2018
Mauna Kea Technologies

©2018 Mauna Kea Technologies!2
Disclaimer• This document has been prepared by Mauna Kea Technologies (the "Company") and is provided for information purposes only. • The information and opinions contained in this document speak only as of the date of this document and may be updated, supplemented, revised, verified
or amended, and such information may be subject to significant changes. Mauna Kea Technologies is not under any obligation to update the information contained herein and any opinion expressed in this document is subject to change without prior notice.
• The information contained in this document has not been independently verified. No representation, warranty or undertaking, express or implied, is made as to the accuracy, completeness or appropriateness of the information and opinions contained in this document. The Company, its subsidiary, its advisors and representatives accept no responsibility for and shall not be held liable for any loss or damage that may arise from the use of this document or the information or opinions contained herein.
• This document contains information on the Company’s markets and competitive position, and more specifically, on the size of its markets. This information has been drawn from various sources or from the Company’s own estimates. Investors should not base their investment decision on this information.
• This document contains certain forward-looking statements. These statements are not guarantees of the Company's future performance. These forward-looking statements relate to the Company's future prospects, developments and marketing strategy and are based on analyses of earnings forecasts and estimates of amounts not yet determinable. Forward-looking statements are subject to a variety of risks and uncertainties as they relate to future events and are dependent on circumstances that may or may not materialize in the future. Mauna Kea Technologies draws your attention to the fact that as forward-looking statements cannot under any circumstance be construed as a guarantee of the Company's future performance and that the Company’s actual financial position, results and cash flow, as well as the trends in the sector in which the Company operate may differ materially from those proposed or reflected in the forward-looking statements contained in this document. Furthermore, even if Mauna Kea Technologies’ financial position, results, cash-flows and developments in the sector in which the Company operates were to conform to the forward-looking statements contained in this document, such results or developments cannot be construed as a reliable indication of the Company's future results or developments. The Company does not undertake any obligation to update or to confirm projections or estimates made by analysts or to make public any correction to any prospective information in order to reflect an event or circumstance that may occur after the date of this presentation. A description of those events that may have a material adverse effect on the business, financial position or results of Mauna Kea Technologies, or on its ability to meet its targets, appears in the "Risk Factors" section of Mauna Kea Technologies Registration Document registered with the Autorité des marches financiers on April 27, 2018 under number R.18-0429.
• Certain figures and numbers appearing in this document have been rounded. Consequently, the total amounts and percentages appearing in the tables are therefore not necessarily equal to the sum of the individually rounded figures, amounts or percentages.
• This document does not constitute or form part of an offer to sell or to purchase securities or the solicitation of an offer to purchase securities in the United States of America or in any other jurisdiction. The securities mentioned in this presentation have not been and will not be registered under the U.S. Securities Act of 1933, as amended (the “Securities Act”) or under any other legislation of any jurisdiction in the United States of America and may not be offered or sold in the United States absent registration or an applicable exemption from registration under the Securities Act.

Cellvizio®: cellular vision at your fingertips
First miniaturized confocal microscope designed to provide physicians and surgeons with digital cellular visualization at the bedside

©2017 Mauna Kea Technologies
Investment opportunity : A highly attractive value proposition
1 First and only: Transformational probe-based Confocal Laser Endomicroscopy Platform
2 Large addressable market: GI, Urology, Interventional Pulmonology, others
3 Clinically-validated: 1,100+ publications on endomicroscopy
4Strong regulatory support: Approved in 40+ countries; 15 US FDA 510(k) clearances
Favorable economics: Strong CMS reimbursement in the US; plan to secure commercial payers
5
6
7
9
Utilization-focused: Driving US adoption & recurring revenue via pay-per-use model
Robust R&D pipeline to drive growth through application expansion
Broad IP protection: 236 issued patents on Cellvizio® technologies
8
New seasoned US based executive leadership to drive commercial expansion
!4

A breakthrough technology platform

©2018 Mauna Kea Technologies©2018 Mauna Kea Technologies
Tissue characterization relies on old paradigms
!6
Random/blind samples
Low sensitivity
Diagnostic and treatment uncertainty
Invasive, multi-step process
Repeat procedures
Creates anxiety for patients and frustration for surgeons
Real-time digital biopsies to eliminate uncertainties and provide instantaneous, reliable and actionable results
Biopsy today Unmet need

Digital optical biopsies: a powerful new paradigm
“Patients are better served if biopsies can be better targeted. That’s where in vivo
microscopy comes in”.
©2018 Mauna Kea Technologies!7
From H&E histology…one image - static view
…to Cellvizio® 720 live biopsies per minute - functional view
Brain Colon Esophagus

©2018 Mauna Kea Technologies!8
Probe-based Confocal Laser Endomicroscopy (pCLE) provides real time digital optical sections of tissues through all types of access methods
Cellvizio reveals key invisible information
pCLE (lap / robotics)
nCLE (needle)
pCLE (probe/catheter)

©2018 Mauna Kea Technologies
Seamless integration into endoscopy workflow
1During an endoscopic procedure, an area of interest is identified
Cellvizio miniprobe is inserted into operating channel of any endoscope 2
3Simple contact between the tip of the miniprobe and the tissue generates real-time microscopic cellular images viewed directed on the Cellvizio screen
Our mission: eliminate diagnostic and treatment uncertainties

Gastroenterology applications

©2018 Mauna Kea Technologies 11
Core commercial focus: A significant Cellvizio U.S. gastroenterology
market opportunity
Society recom-
mendations and
increased CMS reimbursement
rates
Key Market Drivers
U.S. Procedure volume
U.S. market opportunity
3.6 million*
annual upper GI procedures
$2.8 billion* annual
recurring revenue
U.S. Target Hospitals
3,000+* with large GI volume
* Millenium research group : Custom Urology report 2014 and 2012; 2013 U.S. laparoscopic proceduresMedtech Insight : U.S. Procedure Volume 2010iData : 2015 EUS Market; U.S. Procedure volume 2012; 2015 ERCP report, M&A acquisition figures : Covidien; Medtronic Advamed presentations : 2013 Advamed presentation; E&Y; Presentations citing other sources

©2016 Mauna Kea Technologies©2016 Mauna Kea Technologies
Enhancing traditional endoscopy is a recognised need…
Dr. Brian Fennerty, past President, ASGE (American Society of Gastrointestinal Endoscopy)
New York Society of Gastroenterology meeting, 17 Dec 2010, New York
!12

©2010-2018 Mauna Kea Technologies
… for important reasons
More than 25% of esophageal adenocarcinoma are diagnosed within a year after the index endoscopy
among adults with non dysplastic Barrett’s esophagus (or Barrett’s esophagus with low-grade dysplasia) (1)
1.Visrodia K et al. Magnitude of Missed Esophageal
Adenocarcinoma After Barrett’s Esophagus Diagnosis: A
Systematic Review and Meta-analysis. Gastroenterology. 2016
!13
Additional resources / technologies should be allocated to detect missed cases

©2018 Mauna Kea Technologies©2018 Mauna Kea Technologies
Growing, unmet need in esophageal cancer
!14
Esophageal cancer is the fastest growing cancer2
Symptoms of acid reflux, including
heartburn, occur monthly in
44% of adults11 Shaheen N, Ransohoff DF. Gastroesophageal reflux, Barrett's esophagus and esophageal cancer. Journal of the American Medical Association. 2002; 287: 1972-1981. 2. The Wall Street Journal - Emerging Type of Heartburn Defies Drugs, Diagnosis - online.wsj.com/news/articles/SB10001424127887323894704578115031699278010 3. K. Visrodia, at al. Magnitude of Missed Esophageal Adenocarcinoma After Barrett's Esophagus Diagnosis: A Systematic Review and Meta-analysis. AGA Institute, 2016.
25% of esophageal cancers diagnosed within one year of
standard endoscopy3

©2018 Mauna Kea Technologies
Addressing the Random Biopsy Limitation
!15
6% yieldInefficient random
sampling1
1. M. Canto, et al. In vivo endomicroscopy improves detection of Barrett’s esophagus–related neoplasia: a multicenter international randomized controlled trial, GIE 2013. 2. Guidelines for Surgical Treatment of GERD. SAGES. February 2010. 3.Sharma P et al. White Paper AGA: Advanced Imaging in Barrett's Esophagus. Clin Gastroenterol Hepatol. 2015
Seattle Protocol
“biopsies of columnar lined epithelium in the esophagus[…]because of sampling error,
goblet cells may not be detected, thereby underdiagnosing BE”3
…random biopsy protocol can be time-consuming, expensive, and prone to sampling error, as very little of
the esophageal surface area is actually sampled.”2
Goblet cells
The Cellvizio digital optical biopsy solution
intestinal metaplasiasquamous epithelium

©2016 Mauna Kea Technologies©2016 Mauna Kea Technologies!16
Improved detection of Barrett’s Esophagus for enhanced patient management
2. M. Canto, et al. In vivo endomicroscopy improves detection of Barrett’s esophagus–related neoplasia: a multicenter international randomized controlled trial, GIE 2013.
1. Sharma P. et al. Real-time Increased Detection of Neoplastic Tissue in Barrett’s Esophagus with probe- based Confocal Laser Endomicroscopy: Final Results of a Multi-center Prospective International Randomized Controlled Trial. GIE 2011.
3. Bertani H. et al. Improved Detection of Incident Dysplasia by Probe-Based Confocal Laser Endomicroscopy in a Barrett’s Esophagus Surveillance Program. Digestive Diseases and Sciences, 2013.
DON'T BIOPCE trial multi-center, randomized controlled
trial, 101 patients, 2 arms 4
68%
76%
pCLE or WLE
pCLE or
WLE or NBI
WLE or NBI
WLE
WLE : White Light Endoscopy NBI : Narrow Band Imaging
pCLE: endomicroscopy
x 1.7
34%
45%
Sensitivity
x 2
Sensitivity
CEBE trial multi-center, randomized controlled
trial, 192 patients, 2 arms 5
40%
96%
HD-WLE +
CLE
HD-WLE : High Definition White Light Endoscopy CLE: endomicroscopy
HD-WLE
x 2.4
Sensitivity
MODENA BARRETT’S STUDY single-center, randomized trial, 100
patients, 2 arms
Dysplasia Detection tripled with Cellvizio
over white light
Biopsies could have been
avoided for 58% of patients
White Light
White Light +
Cellvizio
10%
28%
~2x improvement in sensitivity for dysplasia detection 36% of patient treatment plans improved
3x diagnostic yield

©2018 Mauna Kea Technologies©2018 Mauna Kea Technologies
New data on improved detection of Barrett’s Esophagus
!17
1. Sharma P. et al. Real-time Increased Detection of Neoplastic Tissue in Barrett’s Esophagus with probe- based Confocal Laser Endomicroscopy: Final Results of a Multi-center Prospective International Randomized Controlled Trial. GIE 2011.
2. Xiong Y-Q, et al. Comparison of narrow-band imaging and confocal laser endomi- croscopy for the detection of neoplasia in Barrett’s esophagus: A meta-analysis. Clin Res Hepatol Gastroenterol (2017), https://doi.org/10.1016/j.clinre.2017.05.005
2017 Meta analysis of detection of neoplasia in BE with NBI vs CLE 2
• Using Cellvizio, physicians at 8 non academic medical centers detected more than double the number of patients with Barrett’s Esophagus than with the Seattle Protocol.
• This number was confirmed by expert review on discrepant cases where biopsies were negative.
20
40
60
80
100
120
140
Seattle Protocol
Positive for IMNegative for IM
>+100% with
Cellvizio
172 patients

©2016 Mauna Kea Technologies!18
Strong endorsements from medical societies
AGA white paper December 2015 “Why should practice change?”
Sharma P et al. White Paper AGA: Advanced Imaging in Barrett's Esophagus. Cl in Gastroenterol Hepatol. 2015
Screening: “BE (specifically shorter disease) is often misdiagnosed during
endoscopy... often attributed to ...lack of goblet cells in biopsies obtained from
columnar lined epithelium in the esophagus.”
“Workshop panelists agreed that in the hands of endoscopists who have met
the PIVI thresholds with specific enhanced imaging techniques (NBI & Confocal Laser Endomicroscopy), use
of the technique in BE patients is appropriate”
“Cellvizio, very clearly, is integral to the comprehensive assessment of
patients suffering from reflux disease”
American Society of General Surgeons Position Statement on Confocal Laser Endomicroscopy published September
2016
“Clinicians and patients alike need and deserve access to Cellvizio® (pCLE) in
order to obtain a comprehensive assessment of the extent of disease and to make real-time therapeutic treatment
decisions.”
https://theasgs.org/position-statements/position-statement-on-confocal-laser-endomicroscopy/
http://www.cghjournal.org/article/S1542-3565(15)01306-3/fulltext

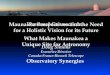
Where to Biopsy?Patients with Barrett esophagus are at risk of developing carcinoma. Patients often undergo multiple repeat biopsies. Even using a 1 cm or 2 cm, four quadrant biopsy protocol, the rate of detecting dysplasia can be low and many unnecessary biopsies are taken.
Traditional “white light” endoscopy shows Barrett-type epithelium in the distal esophagus. Surveillance requires numerous biopsies.
Targeted BiopsiesGiven the usual small size of the dysplastic areas, traditional screening is a shotgun approach to detection. IVM can help target higher-yield, more diagnostic sites.
Prepared by the In Vivo Microscopy Work Group: Maria M. Shevchuck, MD, FCAP (chair), and Gary Tearney, MD, PhD, FCAP (vice chair). Illustrations by Eric F. Glassy, MD, FCAP. For more information, email [email protected]
The architectural and cellular patterns generated by in vivo microscopy are interpretable by pathologists to make differential diagnoses and to identify areas for biopsy, improving diagnostic yield. The image on the left shows a focus of malignant glands.
Photographs reprinted from Kiesslich R, et al. In vivo histology of Barrett’s esophagus and associated neoplasia by confocal laser endomicroscopy. Clin Gastroenterol Hepatol. 2006;4(8):979-987, with permission from Elsevier.
In Vivo Microscopy for the Evaluation of Barrett EsophagusIn vivo microscopy uses light of various wavelengths to produce 2D and 3D microscopic images of living (in vivo) human tissues. One important clinical application is imaging of the gastrointestinal tract.
© 2015 College of American Pathologists. All rights reserved. 23487.0315
cap.org
Patients are better served if the biopsies can be better targeted. That’s where in vivo microscopy comes in.
Traditional surgical biopsy, taken transverse to the tissue plane, shows malignant glands corresponding to the in vivo confocal image on the right.
IVM Optical Biopsy Guides Site SelectionAn optical biopsy, using confocal laser endomicroscopy, for example, is a noninvasive in vivo microscopic assessment of tissue architectural and cellular morphology. It provides 2D images in a parallel tissue plane (en face) with 1 μm–2 μm resolution at a depth of 10 μm.
©2016 Mauna Kea Technologies
A shifting paradigm with in vivo microscopy
!19
“Patients are better served if biopsies can be better targeted. That’s where in vivo
microscopy comes in”.
CAP is actively promoting awareness and better understanding of IVM opportunities
for pathologists
http://www.cap.org/web/home/involved/council-committees/ivm-committee/ivm-topic-center?_afrLoop=817409063069337#!%40%40%3F_afrLoop%3D817409063069337%26_adf.ctrl-state%3D16bmzn84t_4

©2018 Mauna Kea Technologies
Favorable US reimbursement for upper GI
Setting 2016 Rate 2017 Rate 2017 Change ($)
2017 Change
(%)2018 Rate
Hospital $1,088.00 $2,509.64 $1,421.64 131% $2743.26
ASC $608.39 $1,134.02 $525.63 86% $1212.19
CPT Code Description
43252
Upper gastrointestinal endoscopy including esophagus, stomach, and either the duodenum and/or jejunum as appropriate; with optical endomicroscopy
CMS Covered Services
Endomicroscopy in upper GI endoscopy procedures, including GERD, Barrett’s Esophagus and pancreatic lesions
Effective January 1, 2017
! Catalyst for Cellvizio adoption and utilization
! Enhances economical model for Cellvizio customers
! Positive tailwind for commercial coverage
!20
Very positive payment trends in the past 2 years

©2016 Mauna Kea Technologies
2018 Hospital and ASC Reimbursement for Upper GI Endoscopy
!21
Patient with GERD/BE getting
an EGD
Biopsy (Seattle Protocol)
Patient with GERD/BE getting
an EGD
Targeted biopsy protocol with
improved sensitivity
*Multi-Procedure Rule
CPT 43239 : $743 Hospital / $387 ASC medicare payment
CPT 43252 + (CPT 43239)/2 : $3,114* HOPPS / $1,405 ASC medicare payment
WITH Endomicroscopy
WITHOUT Endomicroscopy

©2016 Mauna Kea Technologies©2016 Mauna Kea Technologies
New business model and sales team to address large market
Focus on upper GI endoscopies (EGDs)
• 60% in hospital outpatient setting
• 40% in the 1200 GI-focused ASCs
• New pay-per-use business model provides attractive adoption option for hospitals
•New sales team in place since February 2018
• 2 divisional sales manager, 12 area sales managers, 6 clinical account managers
!22
Potential US Customers
# o
f ce
nte
rs#
of
pro
ce
du
res in
th
ou
san
ds
Potential number of procedures per year
Sources: Burden of Gastrointestinal Disease in the United States: 2012 Update; Peery et al, Gastroenterology. 2012 November ; 143(5): 1179–1187.e3. doi:10.1053/j.gastro.2012.08.002. Repeated Upper Endoscopy in the Medicare Population, Pohl et al, Ann Intern Med. 2014;160:154-160. US census; Medicare website.

©2018 Mauna Kea Technologies
• Consignment program enables physicians to utilize Cellvizio without upfront capital equipment purchase
• Confirmed U.S. commercial traction with 20 systems placed under consignment in Q3 and 36 ytd vs 12 ytd last year.
• Pay-per-use approach provides attractive physician economics
• Pay-per-use revenue up 81% compared to Q3 2017
Continuous momentum with new US sales team
!23
New US sales team trained end of January 2018
0
5
10
15
20
Q1 Q2 Q3
20
11
54
2
6
Consignment systems placed per quarter since launch of program

Corporate information and performance

©2018 Mauna Kea Technologies
Leadership Transition to Support New Phase of Growth
!25October 22, 2018 Proprietary and Confidential. Not to be distributed or reproduced without permission
Rob Gershon
• Most recently CEO of Bovie Medical (NYSE: BVX), where he oversaw the successful repositioning of the Company’s product portfolio and commercial operations
• Prior roles included leadership positions with Henry Schein and Covidien (now Medtronic)
• Rob has been serving as an advisor to Mauna Kea for several months
Mr. Rob Gershon Chief Executive Officer (CEO)
• Brings 30 years of commercial leadership experience
• Joins Mauna Kea’s board of directors
"I share Sacha’s enthusiasm for Cellvizio’s transformational nature and commercial potential both in the United States
and globally. Moreover, I am confident that my experience as a CEO and marketing executive will allow me to build on the remarkable foundation that Sacha and his team have created
over the past 18 years. I welcome the responsibility of building value on behalf of our employees, shareholders and
clinical partners.“ – Robert L. Gershon

©2018 Mauna Kea Technologies
Unrivaled regulatory foundations create high barriers to entry
!26
“Cellvizio® 100 Series Systems with Confocal
Miniprobes™ are confocal laser systems with fiber
optic probes that are intended to allow imaging
of the internal microstructure of tissues including,
but not limited to, the identification of cells and
vessels and their organization or architecture” —
FDA clearance December 2017
Above images are not FDA cleared and are shown as
illustrative examples15 510(k) Clearances
CE mark Clearances in China, Korea and Japan

©2018 Mauna Kea Technologies
A growing installed base worldwide
Preclinical
30+ units
Clinical
100+ units
Clinical
130+ units
Approx. 645 systems installed worldwide
Clinical
160+ units
Preclinical
70+ units
Preclinical
60+ units
!27

©2018 Mauna Kea Technologies
Strong clinical evidence and intellectual property
!28 See appendix for references
Nu
mb
er
of
pu
blicati
on
s
2004
2005
20062007
2008
20092010
20112012
20132014
20152016
20172018
100
50
150
1,100+ Articles on PubMed for endomicroscopy across
multiple applications
230+ issued patents in optics, optronics, image
processing on probe-based Confocal Laser
Endomicroscopy (CLE)
Optoelectronics
Image Processing
Machine Learning

©2018 Mauna Kea Technologies
H1 Key figures
!29
Contacts
€ 2,7m
Down
-18%
Net Sales Gross margin
Opex Ebitda Cash
€ 1,7m
64% Vs 68%
€ -7,7m
Up
3,4%
€ -5,5m
down
-0,7m
€ 15,1 m
Vs
€ 9,4 m
• Q1 Sales impact 1H Sales
• Gross margin at 64% Vs 68% due to COGS of PPU probes (Costs and transportation) with differed logs revenues.
• Effective management of Operating expenses
• Strong cash position

©2018 Mauna Kea Technologies
• U.S. commercial focus gaining traction with 16 systems placed under consignment (compared to 8 systems in 1H17)
• APAC sales +8% above last year,
• EMEA and LATAM still low.
H1 2018 Sales
System Sales & Consignment Sales
0
8
15
23
30
1H17 1H18
914
16
8
New Consignments Placed NewSystem Straight Sales
1H18 vs. 1H17 Sales
'- 0
875
1 750
2 625
3 500
'- 0
825
1 650
2 475
3 300
1H17 1H18
Sales Systems (LTM*) Consumables (LTM*)
2 707
3 285
1H18 Sales by Product
1H18 Sales by Category
18,4%
81,6%
Pre Clinical Clinical
990
1 197
520
Systems Probes Services
!30

©2018 Mauna Kea Technologies
Opex under control
• Opex (excluding COGS & Depreciation) up 3,4% :
▪ Marketing and sales expenses under control and down 20%.
▪ Payroll in the US up 34%, in line with the strategy.
▪ G&A expenses increase : US recruitment fees and HR staffing.
€ 2,0 m€ 1,6 m
€ 3,9 m€ 4,0 m
€ 1,9 m€ 1,9m
0,0
1,0
2,0
3,0
4,0
5,0
6,0
7,0
8,0
9,0
1H 2018 1H 2017
G&A M&S R&D
G&A
R&D
M&S

©2017 Mauna Kea Technologies
Balance sheet
• PPE increases due to PPU model deployment, with 16 new LSU installed in 1H 2018
• Inventories mainly increase due to anticipated purchases.
!32
• Swap of 4M€ from LT debts to Short term due to IPF covenants renegotiation.
• Other short term debt includes Coface advance (150 K€), fully reimbursed as of sept 2018.
1
ASSETS (in K€) 30/06/2018 31/12/2017
Intangible assets 1 873 2 100
Property, plant, and equipment 1 813 1 466
Non-current financial assets 140 138
Total of non-current assets 3 825 3 704
Inventories & Work in progress 2 251 1 969
Trade receivables 1 618 2 034
Other current assets 2 333 2 462
Current financial assets 40 125
Cash and cash equivalents 15 132 17 453
Total of current asets 21 374 24 043
TOTAL OF ASSETS 25 199 27 747
LIABILITIES (in K€) 30/06/2018 31/12/2017
Equity 13 738 16 744
Long-term loans and borrowings 2 749 6 567
Non-current provisions 379 283
Total of non-current liabilities 3 128 6 850
Short-term loans and borrowings 4 333 386
Trade payables 1 910 1 663
Other current liabilities 2 091 2 104
Total of current liabilities 8 334 4 153
TOTAL OF EQUITY AND LIABILITIES 25 199 27 747

©2018 Mauna Kea Technologies
Liquidity Update : a strong cash position at the end ofJune
17 453
-5 638 - 248
3 625 15 193
BoP Cash Operating CF Investing CF Financing CF EoP Cash
0
2 000
4 000
6 000
8 000
10 000
12 000
14 000
16 000
18 000
20 000
HY 2018 Cash variation - in K€
Hausse Baisse Total
Key drivers to Cash burn
• Change in EBITDA drives the change in cash (€ 0,7m
• Change in working capital
- Increase in inventories due to sales gap.-
- Positive impact on trade payables
•Capex
- New web sites, PLM software development
•Cash flow from financing
- Paceo capital raise for 3.8 M€

©2018 Mauna Kea Technologies
Re-orders & Pay-Per-Use Probe Units
0
55
110
165
220
Q1 Q2 Q3
215
146
101
161
108107
20172018
Q3 2018 Highlights • 20 U.S. consignment placements in Q3 vs. 4 in Q3 2017 • 38% year-over-year increase in U.S. consumable miniprobes sales • Global sales up 4% year-over-year, with global miniprobes sales up 31%
Continued Momentum of U.S. Sales Team
!34
Placed more PPU systems in 3Q18 than 1H18 and FY17
0
5
10
15
20
Q1 Q2 Q3
20
11
5 42
6

©2018 Mauna Kea Technologies
Total Float > 80%
Shareholding Profile
!35
Investor Relations U.S.
Lee Roth The Ruth Group +1 (646) 536-7012 [email protected]
Investor Relations Europe
Newcap Pierre Laurent +33 (0) 1 44 71 94 94 [email protected]
Contacts
Contacts
Market Cap (1)Shares
outstandingCoverage
• Goetz Partners-M.Brunninger
• Kepler Chevreux- A.Guekam
• Gilbert Dupont - X.Regnard25,2 MM66 M€
Liquidity (2)
0% 20% 40% 60% 80% 100%
Mauna kea Technologies
Directors & Management
Other registered
Institutional investors
Free Floating
Shareholders
0% 20% 40% 60% 80% 100%
Japan
Benelux
Germany
Switz.
France
Shareholders by Region
(1) As of Oct. 12, 2018
(2) 6 months Avg as of Oct. 12, 2018
92 K / day

Applications pipeline

©2018 Mauna Kea Technologies
Major improvement in pancreatic cystic lesions management
!37
(9)
1Mucinous cystic lesions can be confirmed with very high specificity in about 7 cases out of 10 (1, 2)
0 % 25 % 50 % 75 % 100 %
Sensitivity: 59 - 77%
Specificity: 100%
INSPECT study, 65 patients, multi-centric (9) DETECT study, 30 patients, mono-centric (10)
2Serous cystadenomas can be confirmed with very high specificity in 9 cases out of 10 (3)
CONTACT 2 study, 78 patients, multi-centric (11)0 % 25 % 50 % 75 % 100 %
Sensitivity: 95%
Specificity: 100%
1. Konda V.J. et al. A pilot study of in vivo identification of pancreatic cystic neoplasms with needle-based confocal laser endomicroscopy under endosonographic guidance. Endoscopy 2013 2. Nakai Y. et al. Diagnosis of pancreatic cysts: EUS-guided, through the needle confocal laser-induced endomicroscopy and cystoscopy trial: DETECT study. GIE 2015 3. Napoleon B, et al. Needle-based Confocal Laser Endomicroscopy (nCLE) for the diagnosis of pancreatic cystic lesions: preliminary results of the first prospective multicenter study, presentation at UEGW 2016
Addressing a fast growing interventional market (3-10% prevalence) with unique solution

©2018 Mauna Kea Technologies
Robotic Assisted Radical Prostatectomy
!38
Lopez et al, “Intraoperative Optical Biopsy during Robotic Assisted Radical Prostatectomy Using Confocal Endomicroscopy”. Journal of Urology, April 2016 * source Intuitive Surgical investor presentation
Cellvizio now FDA cleared and CE marked for use in conjunction with surgical robotics systems. User experience is easy and seamless.
Provide specificity to pre-op imaging report on tumor extension in order to improve on resection margins
Lymph node interrogation / Nerve sparing guidance

©2018 Mauna Kea Technologies
Peripheral Nodules / Lymph Nodes / Mediastinal Nodules
!39
Unique through-the-scope access to the lungs now through needles for direct access to the inside of
peripheral and mediastinal lesions
Compatible with Electro-Magnetic Navigation systems and novel flexible robotics systems
0.8 mm AQ-Flex probe
compatible with 19 gauge needles
On target Target missed * CE marked, not yet FDA cleared

©2018 Mauna Kea Technologies
Inflammatory Bowel Disease / Syndrome
!40
Clinical evidence has shown that functional
mucosal healing is key to predict disease course
➡ Cell shedding and barrier loss detected by Cellvizio predict relapse of IBD
➡ Direct visualisation can provide immediate assessment of food allergies / IBS
•Liu J. et al, GIE, 2011. Increased epithelial gaps in the small intestines of patients with inflammatory bowel disease: density matters
• Turcotte A et al, Clinical and Translational Gastroenterology (2012). Increased Epithelial Gaps in the Small Intestine Are Predictive of Hospitalization and Surgery in Patients With Inflammatory Bowel Disease
Random biopsies - or even
targeted biopsies - fail to
provide the information
needed to assess
functional healing, while
Cellvizio does exactly that
• Neumann, H. Et al, Inflamm Bowel Dis, 2012. Assessment of Crohn’s Disease Activity by Confocal Laser Endomicroscopy
• Fritscher-Ravens A et al, Gastroenterology. 2014, Confocal endomicroscopy shows food-associated changes in the intestinal mucosa of patients with irritable bowel syndrome

©2018 Mauna Kea Technologies
Upper Tract Urothelial Cancer (UTUC)
• Important unmet medical needs:
• Limitations of white light endoscopy
• Suboptimal yield of endoscopic biopsy
• Suboptimal clinical staging
• Optimizing patient selection for organ sparing endoscopic management
•Solid clinical data showing Cellvizio can impact UTUC patient management significantly
• Bui et al, 2015; Villa et al 2016; Breda et al 2017; Liem et al 2018
• Use of Cellvizio for UTUC now liste in very short list of very promising technologies in EAU guidelines
!41

©2018 Mauna Kea Technologies©2018 Mauna Kea Technologies
AI: Taking endomicroscopy to the next level
!42
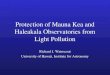
Diagnostic Accuracy of Cellvizio in Bladder
0 %
20 %
40 %
60 %
80 %
100 %
Accuracy Sensitivity Specificity
Machine Urologists (n=8)
87%90%
79%79%77%
82%
Chang et al. EUS 2017 Szegedy C, et al. Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, 2015:1-9
Work performed by the Stanford Bioinformatics program on a dataset of 81 subjects (458 Cellvizio videos, 171,000 images, 21 layer CNN)

©2017 Mauna Kea Technologies
Endomicroscopy is now a booming field
Carl Zeiss announced its Convivo Confocal Laser Endomicroscopy system for neurosurgical applications at the latest Neurosurgery shows
Olympus announced the launch of its Endocytoscopy system, integrated in vivo microscopy in a high-end endoscope.
Caliber ID obtained strong reimbursement for skin optical biopsy with Confocal Microscopy.
!43
Cellvizio and its future generations are unparalleled products for in vivo optical biopsy applications

©2018 Mauna Kea Technologies
In vivo microscopic molecular imaging roadmap
!44 * Not cleared by FDA for human use
Molecular markers +
wide-field fluorescence +
in vivo microscopy =
precision surgery
Mauna Kea is the unique provider
of in vivo molecular
microscopic dual-band imaging*
Fluorescence-guided surgery (open, laparoscopic, robotic) is now the
norm with wide-field imaging systems from a dozen players
(Stryker+Novadaq, Olympus, Intuitive Surgical, Bracco, Fluoptics,
SurgVision…)

©2018 Mauna Kea Technologies
Unlimited discoveries with Cellvizio
!45
March 27th, 2018

©2018 Mauna Kea Technologies
Cellvizio is at the core of key trends in medicine and surgery
!46
Real time microscopic imaging &
characterization
Data-driven digital surgery
Endoluminal therapies
Minimally invasive interventions
Our technologies are key to the future of image-guided and data-driven interventions
Robotic
Surgery

Appendix

©2016 Mauna Kea Technologies 48
Beating uncertainty with CLE
State of the art + pCLE
BE Metaplasia (1) 66 32
BE Dysplasia (1) 55 24
Inflammatory Biliary Strictures (2) 27 (73 % NPV) 18 (82 % NPV)
Malignant Biliary Strictures (2) 44 15-24 11
Hyperplastic Polyps (3) 28 0
Adenocarcinoma (3) 9 (91 % NPV) 0 (100 % NPV)
Serous cystadenoma (4) 50 40 31 0
Mucinous Cysts (5) 50 40 23-41 0
% False Negatives % False Positives % False Negatives % False Positives
(1) DONT BIOPCE study, 101 patients, multi-centric (2)FOCUS study, 112 patients, multi-centric (3)Shahid et al., 92 patients, multi-centric (4)CONTACT study, 31 patients, multi-centric
(5)INSPECT study, 65 patients, multi-centric,
DETECT study, 30 patients, mono-centric

©2018 Mauna Kea Technologies
References - Clinical Evidence
GENERAL 1. Wang, K. K., Carr-Locke, D. L., Singh, S. K., Neumann, H., Bertani, H., Galmiche, J. - P., Arsenescu, R.I.; Caillol, F.; Chang, K.J.; Chaussade, S.; Coron, E.; Costamagna, G.; Dlugosz, A.; Ian Gan,
S.; Giovannini, M.; Gress, F.G.; Haluszka, O.; Ho, K.Y.; Kahaleh, M.; Konda, V.J.; Prat, F.; Shah, R.J.; Sharma, P.; Slivka, A.; Wolfsen, H.C.; Zfass, A.. (2015). Use of probe-based confocal laser endomicroscopy (pCLE) in gastrointestinal applications. A consensus report based on clinical evidence. United European Gastroenterol J, 3(3), 230–254.
2. Queneherve L et al., nouvelles stratégies d'analyse endoscopique des maladies digestives. Médecine/sciences 2015 ;31:777-83 3. Sabina Beg, Krish Ragunath,, Image-enhanced endoscopy technology in the gastrointestinal tract: What is available?, Best Practice & Research Clinical Gastroenterology 29 (2015)
627e638 4. Ussui Vivian et al. Probe-based confocal laser endomicroscopy with cap for image stabilization… Endosc Int Open 2015
BE/GERD 1. Guo, J., Li, C. - Q., Li, M., Zuo, X. - L., Yu, T., Liu, J. - W., et al. (2015). Diagnostic value of probe-based confocal laser endomicroscopy and high-definition virtual chromoendoscopy in
early esophageal squamous neoplasia. Gastrointest Endosc, 81(6), 1346–1354. 2. Robles, L. Y., Singh, S., & Fisichella, P. M. (2015). Emerging enhanced imaging technologies of the esophagus: spectroscopy, confocal laser endomicroscopy, and optical
coherence tomography. J Surg Res, 195(2), 502–514. 3. Muthusamy, V. R., Kim, S., & Wallace, M. B. (2015). Advanced Imaging in Barrett's Esophagus. Gastroenterol Clin North Am, 44(2), 439–458. 4. Singh, R., Yeap, S. P., & Cheong, K. L. (2015). Detection and characterization of early malignancy in the esophagus: What is the best management algorithm? Best Pract Res Clin
Gastroenterol, 29(4), 533–544. 5. Leggett CL, Gorospe EC, Chan DK, Muppa P, Owens V, Smyrk TC, Anderson M, Lutzke LS, Tearney G, Wang KK, Comparative Diagnostic Performance of Volumetric
Laser Endomicroscopy and Confocal Laser Endomicroscopy in the Detection of Dysplasia Associated with Barrett’s Esophagus, Gastrointestinal Endoscopy (2015) 6. Prueksapanich, P., Pittayanon, R., Rerknimitr, R., Wisedopas, N., & Kullavanijaya, P. (2015). Value of probe-based confocal laser endomicroscopy (pCLE) and dual focus narrow-band
imaging (dNBI) in diagnosing early squamous cell neoplasms in esophageal Lugol's voiding lesions. Endosc Int Open, 3(4), E281–8. 7. Massimiliano di Pietro , Elizabeth L. Bird-Lieberman ,Bchir, , Xinxue Liu , Mphil, Tara Nuckcheddy-Grant , Helga Bertani ,Maria O’Donovan, Rebecca C. Fitzgerald,Autofluorescence-
directed confocal endomicroscopy in combination with a three-biomarker panel can inform management decisions in Barrett's Esophagus, Am J Gastroenterol, 2015 8. Rzouq F, Vennalaganti P, Pakseresht K, Kanakadandi V, Parasa S, Mathur SC, Alsop BR, Hornung B, Gupta N, Sharma P, In-class didactic versus self-directed teaching of the porbe-
based confocal laser endomicroscopy (pCLE) criteria for Barrett's Esopahgus, Endoscopy. 2015 Oct 1 9. Sharma P, Brill J, Canto M, DeMarco D, Fennerty B, Gupta N, Laine L, Lieberman D, Lightdale C, Montgomery E, Odze R, Tokar J, Kockman M. White Paper AGA: Advanced
Imaging in Barrett's Esophagus. Clin Gastroenterol Hepatol. 2015 Dec;13(13):2209-18.
STOMACH 1. Li, Z., Zuo, X. - L., Li, C. - Q., Liu, Z. - Y., Ji, R., Liu, J., et al. (2015). New Classification of Gastric Pit Patterns and Vessel Architecture Using Probe-based Confocal Laser Endomicroscopy. J
Clin Gastroenterol, . 2. Li, C. - Q., Zuo, X. - L. I., Guo, J., Yuan, J., Liu, J. - W., & Li, Y. - Q. (2014). Sa1492 A Paralleled Comparison Between Two Sets of Confocal LASER Endomicroscopy in Gastrointestinal
Tract. Gastrointestinal Endoscopy, 79(5), Ab233. 3. Imaeda, A. (2015). Confocal laser endomicroscopy for the detection of atrophic gastritis: a new application for confocal endomicroscopy? J Clin Gastroenterol, 49(5), 355–357

©2018 Mauna Kea Technologies
References - Clinical Evidence
BILIARY 1. Slivka, A., Gan, I., Jamidar, P., Costamagna, G., Cesaro, P., Giovannini, M., et al. (2015). Validation of the diagnostic accuracy of probe-based confocal laser endomicroscopy for
the characterization of indeterminate biliary strictures: results of a prospective multicenter international study. Gastrointest Endosc, 81(2), 282–290. 2. Baillie, J. (2015). Distinguishing malignant from benign biliary strictures: can confocal laser endomicroscopy close the gap? Gastrointest Endosc, 81(2), 291–293. 3. Kahaleh, M., Giovannini, M., Jamidar, P., Gan, S. I., Cesaro, P., Caillol, F., Bernard Filoche, Kunal Karia,1 Ioana Smith, Monica Gaidhane and Adam Slivka. (2015). Probe-based confocal laser
endomicroscopy for indeterminate biliary strictures: refinement of the image interpretation classification. Gastroenterol Res Pract, 2015, 675210. 4. Johannes-Matthias Löhr, R. L., Serena Stigliano1, 2, Stephan L Haas1, Fredrik Swahn, Lars Enochsson, Rozh Noel, Ralf Segersvärd, Marco Del Chiaro, Caroline S Verbeke and Urban Arnelo.
(2015). Outcome of probe-based confocal laser endomicroscopy (pCLE) during endoscopic retrograde cholangiopancreatography: A single-center prospective study in 45 patients. United European Gastroenterol J, .
5. Tringali, A., Lemmers, A., Meves, V., Terheggen, G., Pohl, J., Manfredi, G., Hafner, M.; Costamagna, G.; Deviere, J.; Neuhaus, H.; Caillol, F.; Giovannini, M.; Hassan, C.; Dumonceau, J.-M. (2015). Intraductal biliopancreatic imaging: European Society of Gastrointestinal Endoscopy (ESGE) technology review. Endoscopy, 47(8), 739–753.
6. Coté GA., Probe-based confocal laser endomicroscopy for indeterminate bile duct strictures : the inaccuracies of accuracy when appraising the value of a diagnostic test, Gastroenterology, 2015 Sep;149(3):817-9
7. Karia K, Jamal-Kabani A, Gaidhane M, Tyberg A, Sharaiha RZ, Kahaleh M, Probe-based confocal endomicroscopy in primary sclerosing cholangitis : not all inflammatory strictures are the same, Dig Dis Sci, 2015 Aug 2 Epub ahead of print
8. Singh A, Siddiqui UD. The Role of Endoscopy in the Diagnosis and Management of Cholangiocarcinoma. J Clin Gastroenterol. 2015;49(9):725-37. 9. Balderramo D, Probe-based confocal laser endomicroscopy contribution in the evaluation of indeterminate biliary strictures, Gastrointest Endosc. 2015 Nov;82(5):970
PANCREAS 1. Nakai, Y., Iwashita, T., Park, D. H., Samarasena, J. B., Lee, J. G., & Chang, K. J. (2015). Diagnosis of pancreatic cysts: EUS-guided, through-the-needle confocal laser-induced
endomicroscopy and cystoscopy trial: DETECT study. Gastrointest Endosc, 81(5), 1204–1214. 2. Krishna, S. G., Swanson, B., Conwell, D. L., & Muscarella, P. 2nd. (2015). In vivo and ex vivo needle-based confocal endomicroscopy of intraductal papillary mucinous neoplasm of
the pancreas. Gastrointest Endosc, 82(3), 571–572. 3. Karstensen, J. G., Cartana, T., Klausen, P. H., Hassan, H., Popescu, C. F., Saftoiu, A., Vilmann, P. (2015). Endoscopic ultrasound-guided needle-based confocal laser endomicroscopy: a
pilot study for use in focal pancreatic masses. Pancreas, 44(5), 833–835. 4. Maria, K., Waxman, I., Konda, V. J., Gress, F. G., Sethi, A., Siddiqui, U. D., Sharaiha, R.Z.; Kedia, P.; Jamal-Kabani, A.; Gaidhane, M.; Kahaleh, M. (2015). Needle-based confocal endomicroscopy
for pancreatic cysts: the current agreement in interpretation. Gastrointest Endosc, . 5. Tsujino, T.; Yan-Lin Huang, J.; Nakai, Y.; Samarasena, J.B.; Lee, J.G.; Chang, K.J. Tsujino, T.; Yan-Lin Huang, J.; Nakai, Y.; Samarasena, J.B.; Lee, J.G.; Chang, K.J. In vivo identification of
pancreatic cystic neoplasms with needle-based confocal laser endomicroscopy. Best Practice & Research Clinical Gastroenterology. 20145 29:601-610 6. Napoleon B, Lemaistre AI, Pujol B, Caillol F, Lucidarme D, Bourdariat R, Morellon-Miahle B, Fumex F, Lefort C, Lepilliez V, Palazzo L, Monges G, Poizat F, Giovannini M, In
vivo characterization of pancreatic cystic lesions by needle-based confocal laser endomicroscopy (nCLE) : proposition of a comprehensive nCLE classification confirmed by an external retrospective evaluation, Surg Endosc. 2015 Oct 1

©2018 Mauna Kea Technologies
References - Clinical Evidence
COLON/IBD 1. Tontini, G. E., Mudter, J., Vieth, M., Atreya, R., Gunther, C., Zopf, Y.,Wildner, D.; Kiesslich, R.; Vecchi, M.; Neurath, M.F.; Neumann, H. (2015). Confocal laser endomicroscopy for
the differential diagnosis of ulcerative colitis and Crohn's disease: a pilot study. Endoscopy, 47(5), 437–443. 2. Nguyen, D. L., Lee, J. G., Parekh, N. K., Samarasena, J., Bechtold, M. L., & Chang, K. (2015). The current and future role of endomicroscopy in the management of inflammatory bowel
disease. Ann Gastroenterol, 28(3), 331–336. 3. Buchner, A. M., & Wallace, M. B. (2015). In-vivo microscopy in the diagnosis of intestinal neoplasia and inflammatory conditions. Histopathology, 66(1), 137–146. 4. Gabbani, T., Manetti, N., Bonanomi, A. G., Annese, A. L., & Annese, V. (2015). New endoscopic imaging techniques in surveillance of inflammatory bowel disease. World J Gastrointest
Endosc, 7(3), 230–236. 5. Kattah, M. G., & Mahadevan, U. (2015). Confocal laser endomicroscopy for membrane-bound tumor necrosis factor predicts response to therapy in Crohn's disease. Gastroenterology,
148(5), 1067–1069. 6. Mace, V., Ahluwalia, A., Coron, E., Le Rhun, M., Boureille, A., Bossard, C., Jean-François Mosnier, Tamara Matysiak-Budnik and Andrzej S Tarnawski. (2015). Confocal laser
endomicroscopy: a new gold standard for the assessment of mucosal healing in ulcerative colitis. J Gastroenterol Hepatol, 30 Suppl 1, 85–92. 7. Cheon, J. H. (2015). Advances in the Endoscopic Assessment of Inflammatory Bowel Diseases: Cooperation between Endoscopic and Pathologic Evaluations. J Pathol Transl Med,
49(3), 209–217. 8. Rasmussen, D. N., Karstensen, J. G., Riis, L. B., Brynskov, J., & Vilmann, P. (2015). Confocal Laser Endomicroscopy in Inflammatory Bowel Disease – A Systematic Review. J Crohns
Colitis, . 9. Tontini GE, Pastorelli L, Ishaq S, Neumann H. Advances in endoscopic imaging in ulcerative colitis. Expert Rev Gastroenterol Hepatol. 2015 ; 12:1-13. 10. Neurath M. F. Molecular endoscopy and in vivo imaging in inflammatory bowel diseases, Dig Dis 2015;33(suppl 1):32-36 11. Ott C., From bench to bedsite – predictor of response to an anti-TNF-therapy in patients with Crohn's disease during confocal laser endomicroscopy, Z Gastroenterol,2015 Oct;53(10):
1202-3
DUODENUM 1. Nonaka, K., Ohata, K., Ban, S., Takita, M., Matsuyama, Y., Tashima, T., et al. (2015). In vivo imaging of duodenal follicular lymphoma with confocal laser endomicroscopy. Endoscopy, 47
Suppl 1 UCTN, E16–7. 2. Ohata, K., Nonaka, K., Ban, S., & Matsuhashi, N. (2015). Gastroenterology: Simultaneous practice of narrow band imaging and confocal laser endomicroscopy for a case of early
duodenal cancer. J Gastroenterol Hepatol, 30(6), 966. 3. Rodriguez-Diaz E, Baffy G, Singh SK. Probe-based confocal laser endomicroscopy quantitative morphometric markers associated with portal hypertension in duodenal mucosa. Liver
Int. 2015 4. Dolak, W., Mesteri, I., Asari, R., Preusser, M., Tribl, B., Wrba, F., Schoppmann, S.F.; Hejna, M.; Trauner, M.; Hafner, M.; Puspok, A. (2015). A pilot study of the endomicroscopic assessment
of tumor extension in Barrett's esophagus-associated neoplasia before endoscopic resection. Endosc Int Open, 3(1), E19–28. 5. Rapat Pittayanon1, Rungsun Rerknimitr1, Boonlert Imraporn1, Naruemon Wisedopas2, Pinit Kullavanijaya, Diagnostic values of dual focus narrow band imaging and probe-based
confocal laser endomicroscopy in FAP-related duodenal adenoma, Endosc Int Open, 2015 6. Nonaka K, ohata K, Ichibara S, Ban S, Hiejima Y, Minato Y, Tashima T, Matsuyama Y, Takita M, Matsuhashi N, Takasugi R, Neumann H, Development of a new classification for in vivo
diagnosis of duodenal epithelial tumors with confocal laser endomicrosocpy – a pilot study, Dig Endosc. 2015 Oct 29
!51

©2018 Mauna Kea Technologies
References - Clinical Evidence
UROLOGY
1. G.A. Sonn, K.E. Mach, K. Jensen, P.L. Hsiung S.N. Jones, C.H. Contag, T.D. Wang, J.C. Liao. Fibered Confocal Microscopy of Bladder Tumors: An ex Vivo Study. Journal of endourology 2009;23:2.
2. G.A. Sonn, S.E. Jones, T.V. Tarin, C.B. Du, K.E. Mach, K.C. Jensen and J.C. Liao Optical Biopsy of Human Bladder Neoplasia With In Vivo Confocal Laser Endomicroscopy. The Journal of Urology, 2009
3. W. Adams, K. Wu, J.J. Liu, S.T.T. Hsiao, K.C. Jensen, and J.C. Liao Comparison of 2.6- and 1.4-mm Imaging Probes for Confocal Laser Endomicroscopy of the Urinary Tract. Journal of endourology 2011;25:6
4. K. Wu, J.J. Liu, W. Adams, G.A. Sonn, K.E. Mach, Y. Pan, A.H. Beck, K.C. Jensen, and J.C. Liao Dynamic real-time microscopy of the urinary tract using confocal laser endomicroscopy. The Journal of Urology, 2011.
5. JJ. Liu, TC. Chang, Y . Pan, et al Next generation of optical diagnostics for bladder cancer using probe-based confocal laser endomicroscopy. Proceedings of SPIE, 2012 6. JL. Bonnal, A. Rock, A. Gagnat, et al Confocal laser endomicroscopy of bladder tumors associated with photodynamic diagnosis : an ex vivo pilot study. Journal Urology, 2012 7. TC. Chang, JJ. Liu, ST Hsiao, et al Interobserver agreement of confocal laser endomicroscopy for bladder cancer.J Endourol, 2013 8. J. Liao Optical biopsy of upper tract urothelial carcinoma with confocal laser endomicroscopy (accepted at the congress of American Urological Association AUA, oral presentation
2013) 9. Stephanie P. Chen & Joseph C. Liao Confocal Laser Endomicroscopy of Bladder and Upper Tract Urothelial Carcinoma: A New Era of Optical Diagnosis? Curr Urol Rep (2014) 15:437 10. Aristeo Lopez & Joseph C. Liao Emerging Endoscopic Imaging Technologies for Bladder Cancer Detection Curr Urol Rep (2014) 15:406 11. Lopez A, Liao JC, Emerging endoscopic imaging technologies for bladder dancer detection, Curr Urol Rep, 2014 May ; 15(5):406 12. Chen, S. P., & Liao, J. C. (2014). Confocal laser endomicroscopy of bladder and upper tract urothelial carcinoma: a new era of optical diagnosis? Curr Urol Rep, 15(9), 437. 13. von Rundstedt, F. - C., & Lerner, S. P. (2014). New imaging techniques for nonmuscle invasive bladder cancer. Curr Opin Urol, 24(5), 532–539. 14. Bus, M. T. J., de Bruin, D. M., Faber, D. J., Kamphuis, G. M., Zondervan, P. J., Laguna Pes, M. P., de Reijke, T.M.; Traxer, O.; van Leeuwen, T.G.; de la Rosette, J.J.M.C.H. (2014). Optical
Diagnostics for Upper Urinary Tract Urothelial Cancer: Technology, Thresholds, and Clinical Applications. J Endourol, 15. Pan, Y., Volkmer, J. - P., Mach, K. E., Rouse, R. V., Liu, J. - J., Sahoo, D., Chang, T.C.; Metzner, T.J.; Kang, L.; van de Rijn, M.; Skinner, E.C.; Gambhir, S.S.; Weissman, I.L.; Liao, J.C.. (2014).
Endoscopic molecular imaging of human bladder cancer using a CD47 antibody. Sci Transl Med, 6(260), 260ra148. 16. Zlatev et al., Optical biopsy of bladder cancer using crowd sourced assessment, JAMA surgery, 2015 17. Seong Uk Jeh, Hae Do Jung*, Jong Kyou Kwon et al.,Diagnostic accuracy of probe based confocal laser endomicroscopy in bladder cancer, AUA, 2015 18. Zlatev, D. V., Altobelli, E., & Liao, J. C. (2015). Advances in imaging technologies in the evaluation of high-grade bladder cancer. Urol Clin North Am, 42(2), 147–57, vii. 19. Su LM, Kuo J, Allan RW, Liao JC, Ritari KL, Tomeny PE, Carter CM, Fiberoptic Confocal Laser Endomicroscopy of Small Renal Masses: Towards Real-time Optical Diagnostic Biopsy, The
Journal of Urology® (2015), 20. Bui D, Mach KE, Zlatev DV, Rouse RV, Leppert JT, Liao JC, A pilot study of in vivo confocal laser endomicroscopy of upper tract urothelial carcinoma, J Endourol. 2015 Oct 6 21. Lopez A, Zlatev DV, Mach KE, Bui D, Liu JJ, Rouse RV, Harris T, Leppert JT, Liao JC, Intraoperative optical biopsy during robotic-assisted radical prostatectomy usinf confocal
endomicroscopy. The Journal of Urology 2015, doi: 10.1016/j.juro.2015.10.182 22. Villa L, Cloutier J, Côté JF, Salonia A, Montorsi F, Traxer O, Confocal laser endomicroscopy (CLE) in the management of endoscopically treated upper urinary tract transitional cell
carcinoma (UUT-TCC) – preliminary data, J Endourol. 2015 Oct 16 (in press)