Embed Size (px)
Citation preview

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
1
Lecture 8 – Study Design I XS and Cohort Studies
Mathew J. Reeves BVSc, PhD
Associate Professor, Epidemiology
EPI-546 Block I

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
2
Objectives - Concepts
• Uses of risk factor information• Association vs. causation• Architecture of study designs (Grimes I)• Cross sectional (XS) studies• Cohort studies (Grimes II)• Measures of association – RR, PAR, PARF• Selection and confounding bias• Advantages and disadvantages of cohort studies

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
3
Objectives - Skills
• Recognize different study designs • Define a cohort study • Explain the organization of a cohort study
• Distinguish prospective from retrospective
• Define, calculate, interpret RR, PAR and PARF • Understand and detect selection and confounding
bias

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
4
“Risk Factor” – heard almost daily
Cholesterol and heart diseaseHPV infection and cervical CACell phones and brain cancer
TV watching and childhood obesity
However, “association does not mean causation”!

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
5
Why care about risk factors? Fletcher lists the ways risk factors can be used:
• Identifying individuals/groups “at-risk”• But ability to predict future disease in individual patients is very
limited even for well established risk factors • e.g., cholesterol and CHD
• Causation (causative agent vs. marker) • Establish pretest probability (Bayes’ theorem)• Risk stratification to identify target population
• Example: Age > 40 for mammography screening
• Prevention• Remove causative agent & prevent disease

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
6
Predicting disease in individual patients
Fig. Percentage distribution of serum cholesterol levels (mg/dl) in men aged 50-62 who did or did not subsequently develop coronary heart disease (Framingham Study)

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
7
Causation vs. Association
• An association between a risk factor and disease can be due to:• the risk factor being a cause of the disease (= a causative
agent) OR• the risk factor is NOT a cause but is merely associated with
the disease (= a marker)
• Must guard against thinking that A causes B when really B causes A (reverse causation).• e.g. sedentariness and obesity.

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
8
A B
A B
A B
C
A B

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
9
Prevention
• Removing a true cause → ↓ disease incidence.• Decrease aspirin use → ↓ Reye’s Syndrome• Discourage prone position
“Back to Sleep” → ↓ SIDS

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
10
Back-To-Sleep Campaign Began in 1992

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
11
Architecture of study designs
• Experimental vs. observational
• Experimental studies• Randomization?
– RCT vs. quasi-randomized or natural experiments
• Observational studies• Analytical vs. descriptive
• Analytical– XS, Cohort, CCS
• Descriptive– Case report, case series

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
12
Grimes DA and Schulz KF 2002. An overview of clinical research. Lancet 359:57-61.

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
13
Grimes DA and Schulz KF 2002. An overview of clinical research. Lancet 359:57-61.

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
14
Cross-sectional studies
• Also called a prevalence study
• Prevalence measured by conducting a survey of the population of interest e.g.,
• Interview of clinic patients• Random-digit-dialing telephone survey
• Mainstay of descriptive epidemiology• patterns of occurrence by time, place and person• estimate disease frequency (prevalence) and time trends
• Useful for:• program planning • resource allocation• generate hypotheses

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
15
Cross-sectional Studies
• Select sample of individual subjects and report disease prevalence (%)
• Can also simultaneously classify subjects according to exposure and disease status to draw inferences• Describe association between exposure and disease
prevalence using the Odds Ratio (OR)

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
16
Cross-sectional Studies
• Examples:• Prevalence of Asthma in School-aged Children in Michigan
• Trends and changing epidemiology of hepatitis in Italy
• Characteristics of teenage smokers in Michigan
• Prevalence of stroke in Olmstead County, MN

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
17
Concept of the Prevalence “Pool”
New cases
DeathRecovery

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
18
Cross-sectional Studies
• Advantages:• quick, inexpensive, useful
• Disadvantages:• uncertain temporal relationships
• survivor effect
• low prevalence due to – rare disease – short duration

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
19
Cohort Studies
• A cohort is a group with something in common e.g., an exposure
• Start with disease-free “at-risk” population• i.e., susceptible to the disease of interest
• Determine eligibility and exposure status
• Follow-up and count incident events
• a.k.a prospective, follow-up, incidence or longitudinal
• Similar in many ways to the RCT except that exposures are chosen by “nature” rather than by randomization

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
20
Types of Cohort Studies
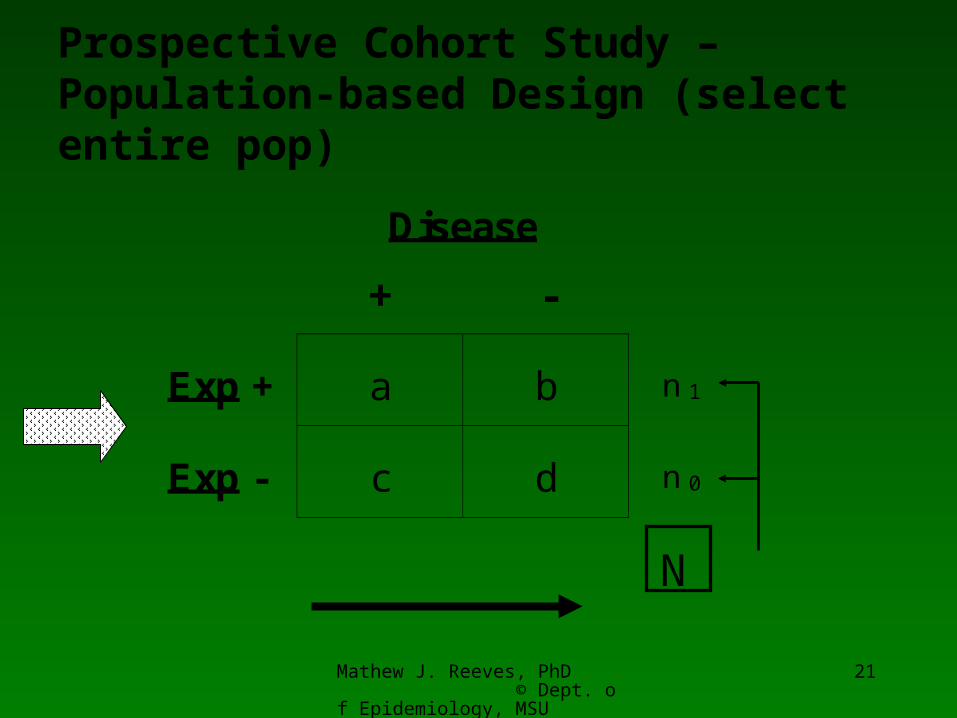
• Population-based (one-sample)• select entire popl (N) or known fraction of popl (n)• p (Exposed) in population can be determined
• Multi-sample• select subgroups with known exposures
– e.g., smokers and non-smokers
– e.g., coal miners and uranium miners
• p (Exposed) in population cannot be determined
Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
21
Disease
+ -
Exp + a b n 1
Exp - c d n 0
N
Prospective Cohort Study – Population-based Design (select entire pop)

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
22
Disease
+ -
Exp + a b n 1
Exp - c d n 0
Prospective Cohort Study – Multi-sample Design (select specific exposure groups)
Rate= c/ n 0
Rate= a/ n 1

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
23
Exposed
Eligible subjects
Unexposed
Disease
Disease
No disease
No disease
FUTURENOW
Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
24
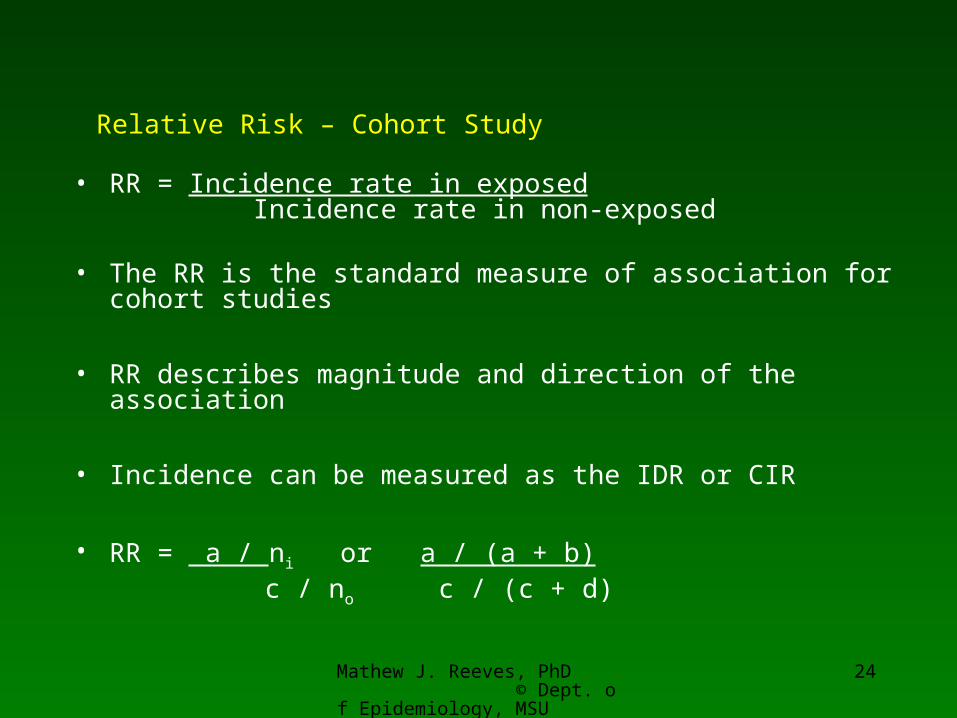
Relative Risk – Cohort Study
• RR = Incidence rate in exposed Incidence rate in non-exposed
• The RR is the standard measure of association for cohort studies
• RR describes magnitude and direction of the association
• Incidence can be measured as the IDR or CIR
• RR = a / ni or a / (a + b) c / noc / (c + d)

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
25
Example - Smoking and Myocardial Infarction (MI)
MI
+ -
Smk + 30 970 Rate = 30 / 1000
Smk - 10 990 Rate = 10 / 1000
RR= 3
Study: Desert island, pop= 2,000 people, smoking prevalence= 50%Population-based cohort study. Followed for one year. What is the risk of MI among smokers compared to non-smokers?

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
26
RR - Interpretation
• RR = 1.0 • indicates the rate (risk) of disease among exposed and non-
exposed (= referent category) are identical (= null value)
• RR = 2.0 • rate (risk) is twice as high in exposed versus non-exposed
• RR = 0.5• rate (risk) in exposed is half that in non-exposed

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
27
RR - Interpretation
• RR = > 5.0 or < 0.2 • BIG
• RR = 2.0 – 5.0 or 0.5 – 0.2 • MODERATE
• RR = <2.0 or >0.5• SMALL

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
28
Sources of Cohorts
• Geographically defined groups:• Framingham, MA (sampled 6,500 of 28,000, 30-50 yrs of
age)• Tecumseh, MI (8,641 persons, 88% of population)
• Special resource groups• Medical plans e.g., Kaiser Permanente• Medical professionals e.g.,
• Physicians Health Study, Nurses Health Study
• Veterans• College graduates e.g., Harvard Alumni

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
29
Sources of Cohorts
• Special exposure groups• Occupational exposures
– e.g., pb workers, U miners – If everyone exposed then need an external cohort
non-exposed cohort for comparison purposes– e.g., compare pb workers to car assembly workers
• Specific risk factor groups – e.g., smokers, IV drug users, HIV+

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
30
Cohort Design Options
• variation in timing of E and D measurement
Design Past
Prospective
Retrospective
Historical/pros.
E D
E E D
DE
Present Future

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
31
Disease
+ -
Exp + a b n 1
Exp - c d n 0
Retrospective Cohort Study – DesignGo back and determine exposure status based on historical information and then classify subjects according to their current disease status
Rate= c/ n 0
Rate= a/ n 1

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
32
Exposed
Eligible subjects
Unexposed
Disease
Disease
No disease
No disease
NOWPAST RECORDS

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
33
Examples retrospective cohort
• Aware of cases of fibromyalgia in women in a large HMO. Go back and determine who had silicone breast implants (past exposure). Compare incidence of disease in exposed and non-exposed.
• Framingham study: use frozen blood bank to determine baseline level of hs-CRP and then measure incidence of CHD by risk groups (quartile)

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
34
PAR and PARF
• Important question for public health • How much can we lower disease incidence if we intervene
to remove this risk factor?
• Want to know how much disease an exposure causes in a population.
• PAR and PARF assume that the risk factor in question is causal
• See Lecture 3 course notes

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
35
Venous thromboemolic disease (VTE) and oral contraceptives (OC) in woman of
reproductive age
• Incidence of VTE:• OC users: 16 per 10,000 person-years • non-OC users: 4 per 10,000 person-years• Total population: 7 per 10,000 person-years
• RR = 16/4 = 4
• Prevalence of exposure to OC: • 25% of woman of reproductive age

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
36
Population attributable risk (PAR)
• The incidence of disease in a population that is associated with a risk factor.
• Calculated from the Attributable risk (or RD) and the prevalence (P) of the risk factor in the population• PAR = Attributable risk x P• PAR = (16-4) x 0.25• PAR = 3 per 10,000 person years
• Equals the excess incidence of VTE in the population due to OC use

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
37
Population attributable risk fraction (PARF)
• The fraction of disease in a population that is attributed to a risk factor.
• PARF = PAR/Total incidence • PARF = 3/7per 10,000 person years• PARF = 43%
• Represents the maximum potential impact on disease incidence if risk factor was removed• So, remove OC’s and incidence of VTE drops 43% in women of
repro age (assuming OC is a cause of VTE)

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
38
Exposed
Eligible subjects
Unexposed
Disease
Disease
No disease
No disease
FUTURENOW
PARF = -

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
39
PARF Calculation
• PARF = P(RR-1)/ [1 + P(RR-1)]where:
• P = prevalence, RR = relative risk
• PARF = 0.25(4-1)/ [1 + 0.25(4-1)]• PARF = 43%
• Note that a factor with a small RR but a large P can cause more disease in a population than a factor with a big RR and a small P.

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
40
Selection Bias
• Selection bias can occur at the time the cohort is first assembled: • Patients assembled for the study differ in ways other than the
exposure under study and these factors may determine the outcome
– e.g., Only the Uranium miners at highest risk of lung cancer (i.e., smokers, prior family history) agree to participate
• Selection bias can occur during the study• e.g., differential loss to follow-up in exposed and un-exposed
groups (same issue as per RCT design)• Loss to follow-up does not occur at random
• To some degree selection bias is almost inevitable.

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
41
Confounding Bias• Confounding bias can occur in cohort studies
because the exposure of interest is not assigned at random and other risk factors may be associated with both the exposure and disease.
• Example: cohort study of lecture attendance
Attendance Exam success
Baseline epi proficiency
-
- +

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
42
Cohort Studies - Advantages
• Can measure disease incidence • Can study the natural history • Provides strong evidence of casual association between E
and D (time order is known)• Provides information on time lag between E and D• Multiple diseases can be examined• Good choice if exposure is rare (assemble special exposure
cohort) • Generally less susceptible to bias vs. CCS

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
43
Cohort Studies - Disadvantages
• Takes time, need large samples, expensive• Complicated to implement and conduct• Not useful for rare diseases/outcomes • Problems of selection bias
• At start = assembling the cohort• During study = loss to follow-up
• With prolonged time period:• loss-to-follow up• exposures change (misclassification)
• Confounding• Exposures not assigned at random

Mathew J. Reeves, PhD © Dept. of Epidemiology, MSU
44
Prognostic Studies - predicting outcomes in those with disease
• Also measured using a cohort design (of affected individuals)
• Factors that predict outcomes among those with disease are called prognostic factors and may be different from risk factors.
• Discussed further in Epi-547