Embed Size (px)
Citation preview
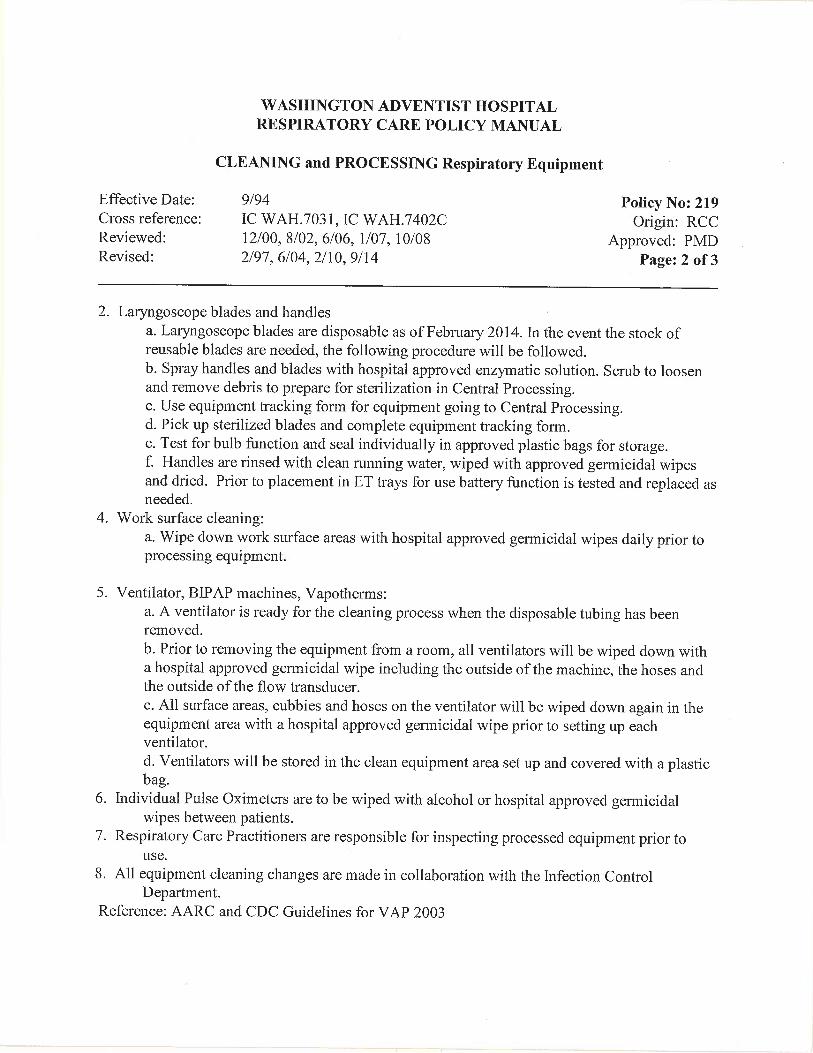
WASHINGTON ADVENTIST HOSPITAL
WOMEN’S SERVICES POLICY AND PROCEDURE
Effective Date: 4/13 Policy: WWS.9170 Comments: Origin: Women's Svcs Reviewed: Approved: 3/13 Revised: New Page 1 of 5
MATERNAL/NEWBORN TRANSFER TO A HIGHER LEVEL OF CARE
SCOPE: All of Women’s services
I PURPOSE: To establish guidelines and criteria for the safe transfer of a mother and/or newborn
from our facility to a facility that can provide a higher level of care. II DEFINITIONS: A communication system, which provides receiving physician with appropriate
verbal and written information pertaining to the mother/neonate being transferred between health care facilities. To ensure that the receiving facility has the information required to begin caring for the patient when the patient arrives at the facility and to assure the continuity of care for patient safety and to minimize the potential for errors in handing off
III POLICY: In the event a patient transfer is needed Shady Grove Adventist Hospital (SGAH) will
be contacted first. If Shady Grove is unable to accept the patient calls will be made by the OB/Pediatrician to another facility based on the care needed.
IV PROCEDURE:
A Once a decision to transfer is made the charge nurse and nursing supervisor should be notified by the patient’s primary nurse.
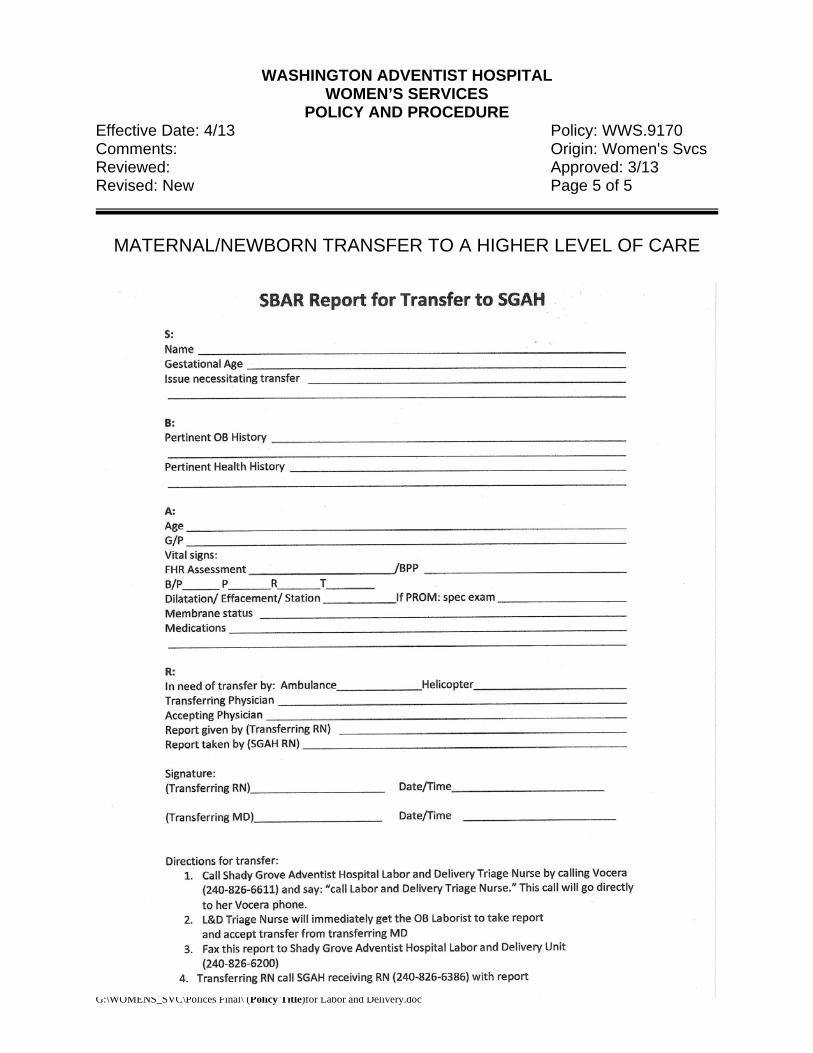
B For a Maternal transfer to SGAH 1 The Labor and Delivery charge nurse will contact the Labor & Delivery charge nurse at SGAH 2 Transferring OB will give report to receiving OB 3 Patients primary nurse will fill out the Transfer SBAR form (see attached) and fax it to SGAH
Labor & Delivery 4 Call to arrange transport 5 Make a copy of the complete chart for SGAH
C For a Maternal transfer to a facility other than SGAH 1 The OB will call the OB at other facilities to request transfer 2 Once the transfer request has been accepted the charge nurse will call the L&D charge nurse
at the receiving facility to give a brief report on the patient. 3 Call to arrange transport 4 Complete the ED/MCH Transfer/Transport to another facility form
D For Newborn transfer to SGAH A. For Newborn transfer to SGAH
1. .Pediatrician will order transfer after consultation with neonatologist at tertiary facility. The transferring Neonatologist/Pediatrician gives report to SGAH Neonatologist/Pediatrician
2. The Special Care Nursery (SCN) RN will verify that the transfer order is written and Physician’s order is signed and contacts SGAH Charge Nurse Neonatal Intensive Care Unit (NICU).She fills out the Transfer SBAR form and faxes it to SGAH NICU
G:\WOMENS_SVC\Polices Final\ (Policy Title)for Labor and Delivery.doc
WASHINGTON ADVENTIST HOSPITAL
WOMEN’S SERVICES POLICY AND PROCEDURE
Effective Date: 4/13 Policy: WWS.9170 Comments: Origin: Women's Svcs Reviewed: Approved: 3/13 Revised: New Page 2 of 5
MATERNAL/NEWBORN TRANSFER TO A HIGHER LEVEL OF CARE
3. Unit 3100 Charge Nurse will call the Nursing Supervisor to alert the Supervisor of
transfer and mode.
4. Print the face sheet for the transport team
5. Make copy of the complete mother and baby’s chart for SGAH.
6. Ensure parents consent to transfer and obtain parents’ contact details
7. Encourage parents to visit with baby in nursery while awaiting transport team arrival and for reassurance of baby’s safety and well being. Involve family and answer questions. Provide hospital information and directions, including contact details of accepting hospital to make transition easier
8. Provide emotional support as indicated; refer to Chaplain Care if appropriate. Contact the family clergyman if requested.
9. Take Polaroid picture of infant and give to parents (where applicable).
10. Record and document a minimum of: Vital Signs, including non-invasive Blood pressure and O2 Saturation, Weight, Length, and Head and Chest Measurements.
11. Assemble CD of relevant X-rays along with chart if available.
12. Remove EBM from freezer on leaving the unit.
13. Prepare baby’s belonging for transfer. For example baby’s Teddy bear
14. SCN RN will perform and document Neonatal Metabolic Screen
15. SCN RN will notify attending Obstetrician of baby’s transfer to another facility
16. SCN RN will remove ID bracelet from baby in parents’ presence, per identification procedure, and attach it to the Newborn Identification Sheet.
17. Note on chart the time transport team arrives to assume responsibility for baby and departure time.
18. Give transport team an update and report on baby, including lab reports, medications, IVs given, and current vital signs.
19. Good documentation and communication is an essential component of transportation, both for clinical and audit purposes. Parents will be kept up to date with progress and proposed plans.
G:\WOMENS_SVC\Polices Final\ (Policy Title)for Labor and Delivery.doc
WASHINGTON ADVENTIST HOSPITAL
WOMEN’S SERVICES POLICY AND PROCEDURE
Effective Date: 4/13 Policy: WWS.9170 Comments: Origin: Women's Svcs Reviewed: Approved: 3/13 Revised: New Page 3 of 5
MATERNAL/NEWBORN TRANSFER TO A HIGHER LEVEL OF CARE
20. Inform bed control of the transfer including the MD responsible for the transfer,
baby’s diagnosis, the reason for transfer, the receiving facility and the MD accepting the baby.
21. Discharge baby in the system stating reason for baby’s trans to another facility
22. Record information in Newborn transport log.
For Newborn transfer to a facility other than SGAH
1. Follow same procedure from # 4 through 22 above
2. Once the team leaves with the baby, the primary nurse should call the NICU Charge Nurse at the receiving facility to inform her that the patient is in route and to give a detailed report
E Make a copy of the complete chart for the receiving facility F Print a face sheet for the transport team G The primary L&D nurse should give report to the transport team H Once the team has left with the patient the primary nurse should call the charge nurse at the
receiving facility to inform her that the patient is in route and to give a detailed report I Put the patient’s information into the transfer log.
Non-Acute Back Transfers to SCN
Prior to accepting a baby complete liaise with consultant and decision with multidisciplinary team agreement that infant is clinically suitable for back transfer. All transfers must be accompanied by written medical and nursing summaries and handover documentation, and there must be verbal handover between the teams at each stage of the transfer.
Criteria for Back Transfer Babies must meet the following set criteria, before back transfer can be considered.
Gestational age more than 32weeks
• Weight more than 1500 grams • Less than 2 liters Nasal Cannula if on respiratory support • Less than 30% oxygen requirements with satisfactory blood gases • No major Apneas • At least one po feeding in 24 hour period • Satisfactory stable condition • Bed availability
G:\WOMENS_SVC\Polices Final\ (Policy Title)for Labor and Delivery.doc
WASHINGTON ADVENTIST HOSPITAL
WOMEN’S SERVICES POLICY AND PROCEDURE
Effective Date: 4/13 Policy: WWS.9170 Comments: Origin: Women's Svcs Reviewed: Approved: 3/13 Revised: New Page 4 of 5
MATERNAL/NEWBORN TRANSFER TO A HIGHER LEVEL OF CARE
The Process
1. Prepare a warmer/Isolette to receive the baby 2. Once the transport team arrives, check the Identification bands with the Transport Nurse 3. If the infant has had a particularly difficult or complicated course of care, medical staff at the transferring unit must give a more detailed hand-over of care
4. Obtain initial Vital signs . Perform initial and ongoing assessments. a. Do a head to toe examination. b. Observe the infant for any changes in condition, including his/her response to the stress of transport.
5. Document an admission note, the clinical status of the baby and the time of arrival in medical and nursing notes. 6. Good documentation and communication is an essential component of transportation, both for clinical and audit purposes. Keep parents informed with progress and proposed plan of care. Make them as comfortable as possible.
7. Inform bed control of the transfer including the MD responsible baby’s diagnosis, the reason for transfer, and the facility that transferred the baby.
REFERENCES: Altimier, L., Brown, B. And Tedeschi, L. (2006). Transport NANN Guidelines for Neonatal Nursing Policies, Procedures, Competencies, and Clinical Pathways. p.193-204. Glenview: National Association of Neonatal Nurses. Hansmann, G. (2009). Neonatal Emergencies; A Practical Guide for Resuscitation, Transport, and Critical Care of Newborn Infants. p. 494 - 500. New York: Cambridge University Press Karlsen, Kristine A., (2012) New! The S.T.A.B.L.E. Program Learner Manual, 6th Edition
G:\WOMENS_SVC\Polices Final\ (Policy Title)for Labor and Delivery.doc
WASHINGTON ADVENTIST HOSPITAL
WOMEN’S SERVICES POLICY AND PROCEDURE
Effective Date: 4/13 Policy: WWS.9170 Comments: Origin: Women's Svcs Reviewed: Approved: 3/13 Revised: New Page 5 of 5
MATERNAL/NEWBORN TRANSFER TO A HIGHER LEVEL OF CARE
G:\WOMENS_SVC\Polices Final\ (Policy Title)for Labor and Delivery.doc
WASHINGTON ADVENTIST HOSPITAL PATIENT CARE POLICY MANUAL
RESUSCITATION Effective Date: 4/74 Policy No.WAH.5736 Cross Referenced: 5738, Nursing Procedure 1001 Origin: NRSG Reviewed: 7/91, 1/96, 7/07 Authority: SM Revised: 1/86, 10/87, 10/88, 12/89, 5/90, 3/94, 4/95, 10/97, 9/00, 6/01, 1/04, 3/04, 11/04, 7/07, 1/10, 1/11, 1/12, 10/13.
Page: 1 of 22 SCOPE This policy has hospital-wide application. PURPOSE To provide for appropriate emergency response to situations requiring initiation of Basic Life Support (BLS)/ Advanced Cardiac Life Support (ACLS). DEFINITITIONS Code Blue - Adult – Cardiopulmonary arrest in person > 35 kg. or 12 years of age. Code Blue - Child – Cardiopulmonary arrest in person between 1 year and 12 years of age or < 35 kg. Code Blue - Infant – Cardiopulmonary arrest in person birth to 1 year of age. POLICY In the absence of a “Do Not Resuscitate” (DNR) order, all patients with cardiac and respiratory arrests will be treated in compliance with a resuscitation policy. Resuscitation efforts will be maintained until a physician determines that such measure should be terminated. “Code Blue-Adult” will be announced for adult resuscitation events, “Code Blue-Child” for pediatric resuscitation events, and “Code Blue-Infant” for neonatal and infant resuscitation events. (This policy does not prohibit the presence of family during a code.) PROCEDURE I. INITIATION OF CODE BLUE – In-House: Call Page Operator at 5555. If Initiation of Code is Outside the Main Hospital Building: Call the Page Operator at 301-891-5555 or 301-891-7600 and activate EMS through calling 911. II. CODE BLUE TEAM MEMBERS
A. Code Blue Adult – Team Members 1. First Responder 2. Second Responder 3. Unit Charge Nurse 4. Patient’s Primary RN 5. Crisis/ED/ICU RN 6. Director/ Clinical Nurse Specialist/Administrative Supervisor 7. Critical Care Physician/ED Physician/Anesthesiologist assigned to the Code Pager (if available)
8. Respiratory Care Practitioner (RCP) 9. Transporter 10. Pastoral Care 11. Unit Support Coordinator
12. Security (If initiating a code outside the Main Hospital Building)
B. Code Blue Child – Team Members 1. Neonatologist/Pediatrician 2. ED Physician 3. ED RN 4. ED Technician 5. Respiratory Care Practitioner (RCP) 6. Supervisor/Charge RCP 7. Anesthesiologist assigned code pager (if available) 8. Administrative Supervisor
9. Transporter
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 2 of 22
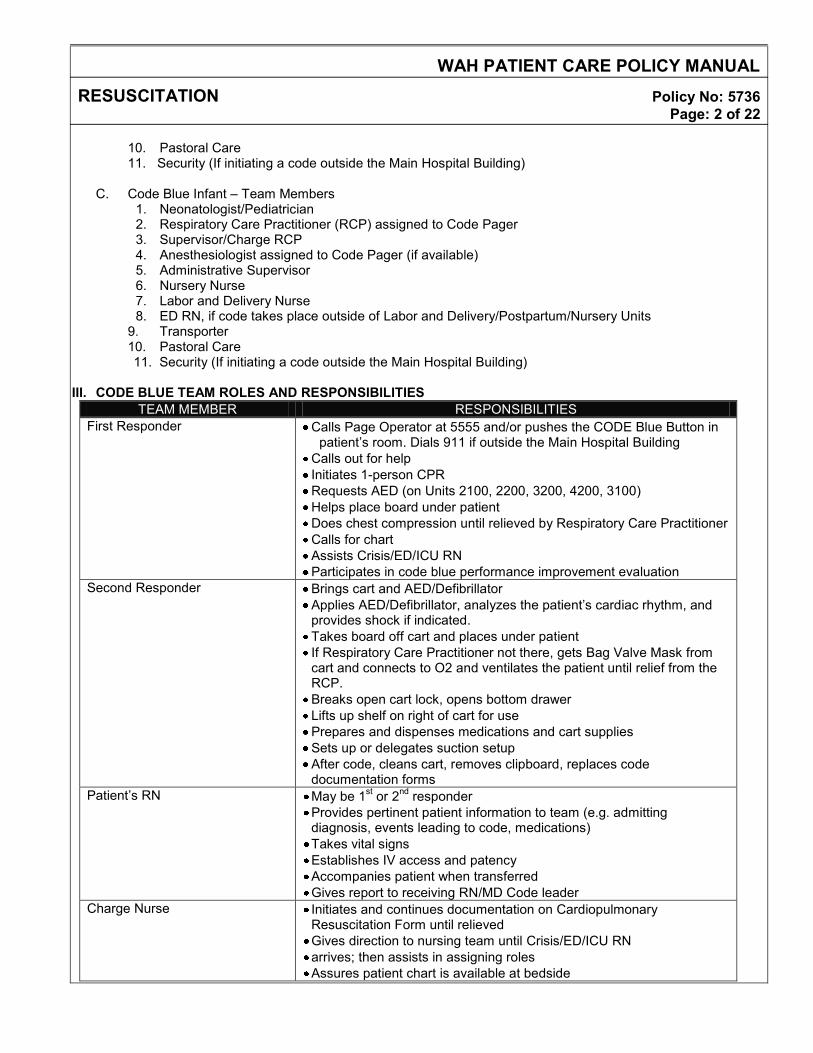
10. Pastoral Care 11. Security (If initiating a code outside the Main Hospital Building)
C. Code Blue Infant – Team Members 1. Neonatologist/Pediatrician 2. Respiratory Care Practitioner (RCP) assigned to Code Pager 3. Supervisor/Charge RCP 4. Anesthesiologist assigned to Code Pager (if available) 5. Administrative Supervisor 6. Nursery Nurse 7. Labor and Delivery Nurse 8. ED RN, if code takes place outside of Labor and Delivery/Postpartum/Nursery Units
9. Transporter 10. Pastoral Care
11. Security (If initiating a code outside the Main Hospital Building)
III. CODE BLUE TEAM ROLES AND RESPONSIBILITIES TEAM MEMBER RESPONSIBILITIES
First Responder Calls Page Operator at 5555 and/or pushes the CODE Blue Button in patient’s room. Dials 911 if outside the Main Hospital Building
Calls out for help Initiates 1-person CPR Requests AED (on Units 2100, 2200, 3200, 4200, 3100) Helps place board under patient Does chest compression until relieved by Respiratory Care Practitioner Calls for chart Assists Crisis/ED/ICU RN Participates in code blue performance improvement evaluation
Second Responder Brings cart and AED/Defibrillator Applies AED/Defibrillator, analyzes the patient’s cardiac rhythm, and provides shock if indicated. Takes board off cart and places under patient If Respiratory Care Practitioner not there, gets Bag Valve Mask from cart and connects to O2 and ventilates the patient until relief from the RCP. Breaks open cart lock, opens bottom drawer Lifts up shelf on right of cart for use Prepares and dispenses medications and cart supplies Sets up or delegates suction setup After code, cleans cart, removes clipboard, replaces code documentation forms
Patient’s RN May be 1st or 2nd responder Provides pertinent patient information to team (e.g. admitting diagnosis, events leading to code, medications) Takes vital signs Establishes IV access and patency Accompanies patient when transferred Gives report to receiving RN/MD Code leader
Charge Nurse Initiates and continues documentation on Cardiopulmonary Resuscitation Form until relieved Gives direction to nursing team until Crisis/ED/ICU RN arrives; then assists in assigning roles Assures patient chart is available at bedside
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 3 of 22
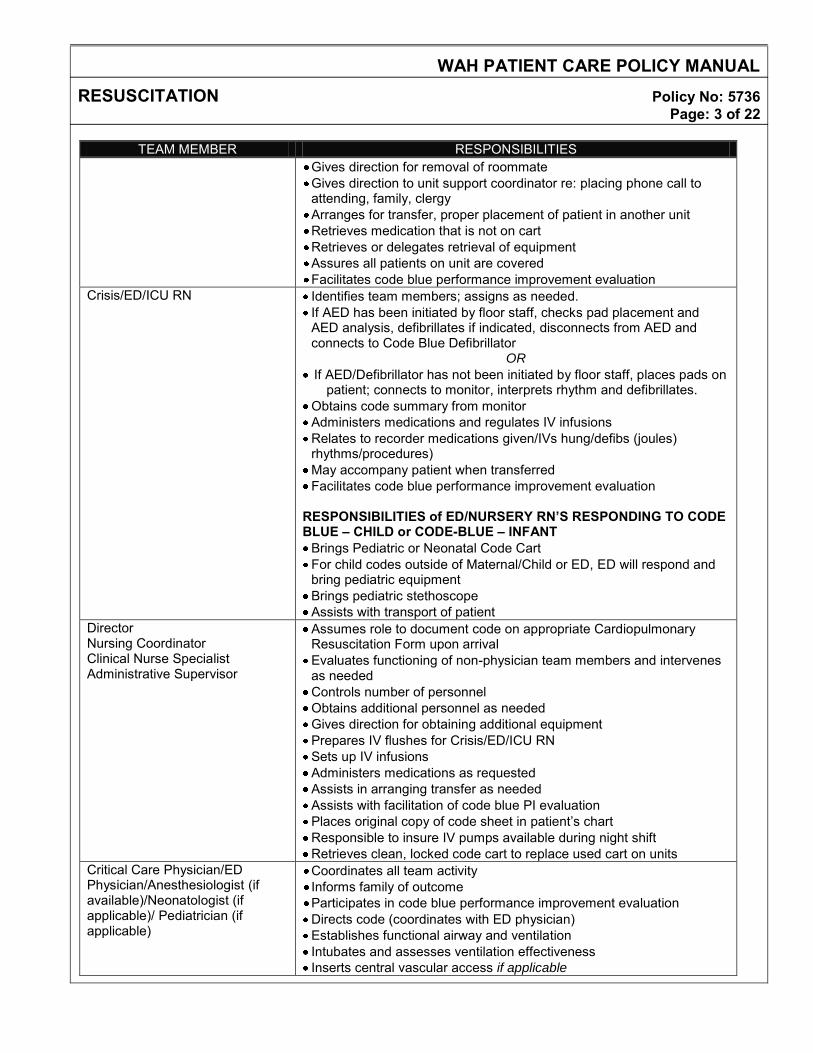
TEAM MEMBER RESPONSIBILITIES Gives direction for removal of roommate Gives direction to unit support coordinator re: placing phone call to attending, family, clergy Arranges for transfer, proper placement of patient in another unit Retrieves medication that is not on cart Retrieves or delegates retrieval of equipment Assures all patients on unit are covered Facilitates code blue performance improvement evaluation
Crisis/ED/ICU RN Identifies team members; assigns as needed. If AED has been initiated by floor staff, checks pad placement and AED analysis, defibrillates if indicated, disconnects from AED and connects to Code Blue Defibrillator
OR
If AED/Defibrillator has not been initiated by floor staff, places pads on patient; connects to monitor, interprets rhythm and defibrillates.
Obtains code summary from monitor Administers medications and regulates IV infusions Relates to recorder medications given/IVs hung/defibs (joules) rhythms/procedures) May accompany patient when transferred Facilitates code blue performance improvement evaluation
RESPONSIBILITIES of ED/NURSERY RN’S RESPONDING TO CODE BLUE – CHILD or CODE-BLUE – INFANT Brings Pediatric or Neonatal Code Cart For child codes outside of Maternal/Child or ED, ED will respond and bring pediatric equipment Brings pediatric stethoscope Assists with transport of patient
Director Nursing Coordinator Clinical Nurse Specialist Administrative Supervisor
Assumes role to document code on appropriate Cardiopulmonary Resuscitation Form upon arrival Evaluates functioning of non-physician team members and intervenes as needed Controls number of personnel Obtains additional personnel as needed Gives direction for obtaining additional equipment Prepares IV flushes for Crisis/ED/ICU RN Sets up IV infusions Administers medications as requested Assists in arranging transfer as needed Assists with facilitation of code blue PI evaluation Places original copy of code sheet in patient’s chart Responsible to insure IV pumps available during night shift Retrieves clean, locked code cart to replace used cart on units
Critical Care Physician/ED Physician/Anesthesiologist (if available)/Neonatologist (if applicable)/ Pediatrician (if applicable)
Coordinates all team activity Informs family of outcome Participates in code blue performance improvement evaluation Directs code (coordinates with ED physician) Establishes functional airway and ventilation Intubates and assesses ventilation effectiveness Inserts central vascular access if applicable
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 4 of 22
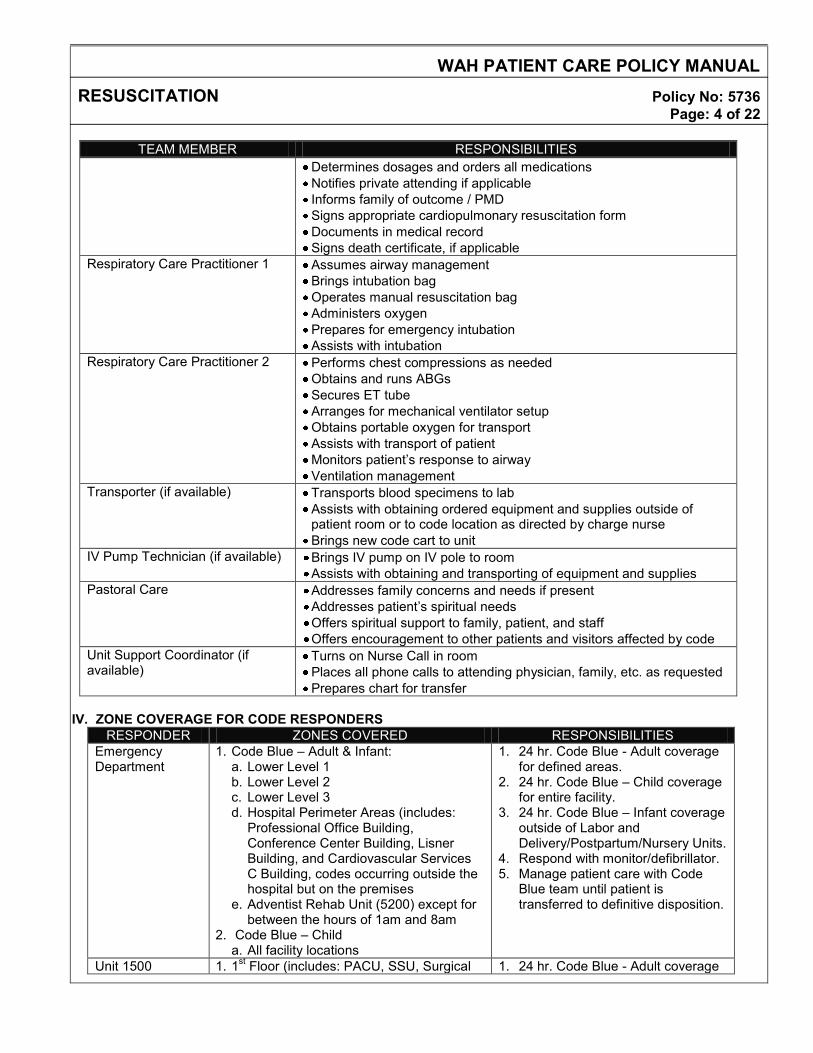
TEAM MEMBER RESPONSIBILITIES Determines dosages and orders all medications Notifies private attending if applicable Informs family of outcome / PMD Signs appropriate cardiopulmonary resuscitation form Documents in medical record Signs death certificate, if applicable
Respiratory Care Practitioner 1 Assumes airway management Brings intubation bag Operates manual resuscitation bag Administers oxygen Prepares for emergency intubation Assists with intubation
Respiratory Care Practitioner 2 Performs chest compressions as needed Obtains and runs ABGs Secures ET tube Arranges for mechanical ventilator setup Obtains portable oxygen for transport Assists with transport of patient Monitors patient’s response to airway Ventilation management
Transporter (if available) Transports blood specimens to lab Assists with obtaining ordered equipment and supplies outside of patient room or to code location as directed by charge nurse Brings new code cart to unit
IV Pump Technician (if available) Brings IV pump on IV pole to room Assists with obtaining and transporting of equipment and supplies
Pastoral Care Addresses family concerns and needs if present Addresses patient’s spiritual needs Offers spiritual support to family, patient, and staff Offers encouragement to other patients and visitors affected by code
Unit Support Coordinator (if available)
Turns on Nurse Call in room Places all phone calls to attending physician, family, etc. as requested Prepares chart for transfer
IV. ZONE COVERAGE FOR CODE RESPONDERS
RESPONDER ZONES COVERED RESPONSIBILITIES Emergency Department
1. Code Blue – Adult & Infant: a. Lower Level 1 b. Lower Level 2 c. Lower Level 3 d. Hospital Perimeter Areas (includes:
Professional Office Building, Conference Center Building, Lisner Building, and Cardiovascular Services C Building, codes occurring outside the hospital but on the premises
e. Adventist Rehab Unit (5200) except for between the hours of 1am and 8am
2. Code Blue – Child a. All facility locations
1. 24 hr. Code Blue - Adult coverage for defined areas.
2. 24 hr. Code Blue – Child coverage for entire facility.
3. 24 hr. Code Blue – Infant coverage outside of Labor and Delivery/Postpartum/Nursery Units.
4. Respond with monitor/defibrillator. 5. Manage patient care with Code
Blue team until patient is transferred to definitive disposition.
Unit 1500 1. 1st Floor (includes: PACU, SSU, Surgical 1. 24 hr. Code Blue - Adult coverage
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 5 of 22
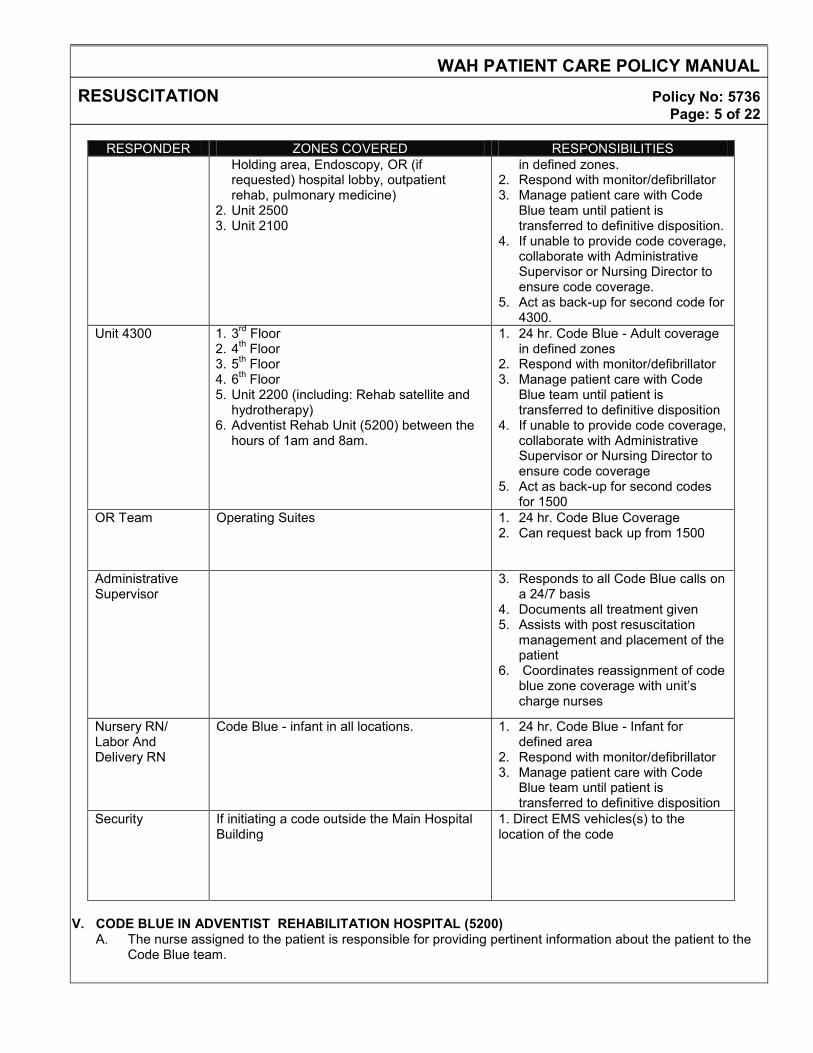
RESPONDER ZONES COVERED RESPONSIBILITIES Holding area, Endoscopy, OR (if requested) hospital lobby, outpatient rehab, pulmonary medicine)
2. Unit 2500 3. Unit 2100
in defined zones. 2. Respond with monitor/defibrillator 3. Manage patient care with Code
Blue team until patient is transferred to definitive disposition.
4. If unable to provide code coverage, collaborate with Administrative Supervisor or Nursing Director to ensure code coverage.
5. Act as back-up for second code for 4300.
Unit 4300 1. 3rd Floor 2. 4th Floor 3. 5th Floor 4. 6th Floor 5. Unit 2200 (including: Rehab satellite and
hydrotherapy) 6. Adventist Rehab Unit (5200) between the
hours of 1am and 8am.
1. 24 hr. Code Blue - Adult coverage in defined zones
2. Respond with monitor/defibrillator 3. Manage patient care with Code
Blue team until patient is transferred to definitive disposition
4. If unable to provide code coverage, collaborate with Administrative Supervisor or Nursing Director to ensure code coverage
5. Act as back-up for second codes for 1500
OR Team Operating Suites 1. 24 hr. Code Blue Coverage 2. Can request back up from 1500
Administrative Supervisor
3. Responds to all Code Blue calls on a 24/7 basis
4. Documents all treatment given 5. Assists with post resuscitation
management and placement of the patient
6. Coordinates reassignment of code blue zone coverage with unit’s charge nurses
Nursery RN/ Labor And Delivery RN
Code Blue - infant in all locations. 1. 24 hr. Code Blue - Infant for defined area
2. Respond with monitor/defibrillator 3. Manage patient care with Code
Blue team until patient is transferred to definitive disposition
Security
If initiating a code outside the Main Hospital Building
1. Direct EMS vehicles(s) to the location of the code
V. CODE BLUE IN ADVENTIST REHABILITATION HOSPITAL (5200)
A. The nurse assigned to the patient is responsible for providing pertinent information about the patient to the Code Blue team.
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 6 of 22
B. The Code Blue – Adult team will respond to all cardio-pulmonary emergencies. (Note: The ED Physician will
respond to 5200 except for between the hours of 1am and 8am when the Intensivist will respond.
VI. CODE BLUE ADULT OUTSIDE HOSPITAL BUILDING BUT ON PREMISES (Professional Office Building, Conference Center Building, Lisner Building, and Cardiovascular Services Building and any other areas covered by the EMTALA regulation) A. Initiate Code Blue by calling hospital operator at 301-891-5555 or 301-891-7600. Report exact location of the
Code to the operator. B. In conjunction with calling the hospital operator, dial 911 to dispatch nearest medic unit/ambulance to the site. C. Hospital Security will direct EMS vehicle to the location of the code.
D. The ED physician and ED RN manages the care of the patient until the patient is transferred to the ED.
E. Responding hospital staff will assist ambulance/medic unit, as requested, with transport of patient to ED. F. Documentation of events prior and during resuscitation is the responsibility of the facility’s staff.
VI. DOCUMENTATION
A. The Cardiopulmonary Resuscitation Form (WAH 650-173) is used for all Code Blue - Adult and Child codes.
B. The Cardiopulmonary Resuscitation Infant Form (WAH 650-154A) is used for all Code Blue-Infant codes.
1. The Code Blue - Infant Cardiopulmonary Resuscitation Form is to be initiated in L&D for any of the following: a. All Code Blue - Infant. b. If neonate’s 1 minute APGAR score is equal to or less than 3 c. If the 5 minute APGAR is equal to or less than 5 d. Any baby with respiratory depression and/or cardiac symptoms requiring positive ventilation.
C. Complete all sections of the documentation form leaving no blanks. 1. Record the time, rhythm, joules delivered and presence of a pulse each time a patient undergoes
cardioversion or defibrillation. 2. Record the time, rhythm and pulse before each medication is given as well as any change in rhythm and
pulse after each medication is given. Include dose & route of administration for each medication. 3. Record the type of intravenous solution and what time they are hung. 4. Record vital signs, presence of a pulse and rhythm at least every 5 minutes during the code. Write 0 if vital
sign is absent. 5. The physician is responsible for documenting the post-arrest diagnosis in the progress notes and for
signing the code documentation form. The physician’s signature on the code form covers all interventions administered during the code.
6. The primary nurse will record a summary statement in the nursing progress notes including events leading up to the code and times, the patient’s condition and disposition after the code.
VII. CODE CARTS
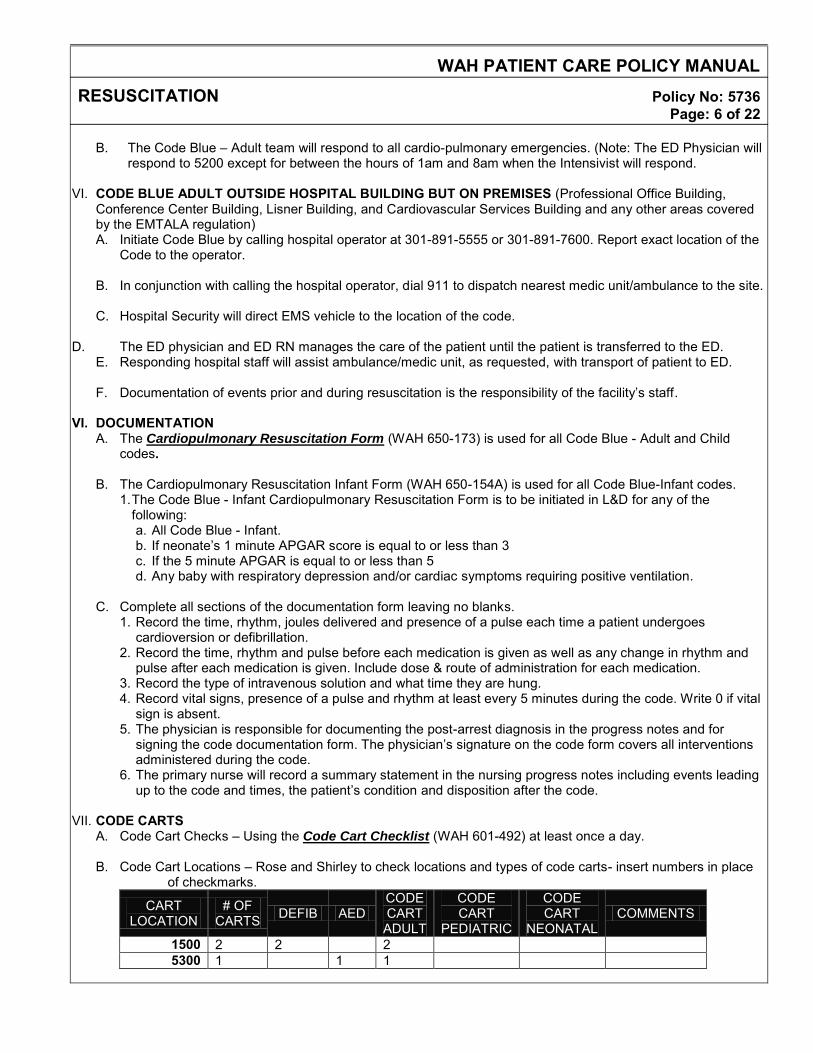
A. Code Cart Checks – Using the Code Cart Checklist (WAH 601-492) at least once a day. B. Code Cart Locations – Rose and Shirley to check locations and types of code carts- insert numbers in place
of checkmarks.
CART LOCATION
# OF CARTS DEFIB AED
CODE CART ADULT
CODE CART
PEDIATRIC
CODE CART
NEONATAL COMMENTS
1500 2 2 2 5300 1 1 1
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 7 of 22
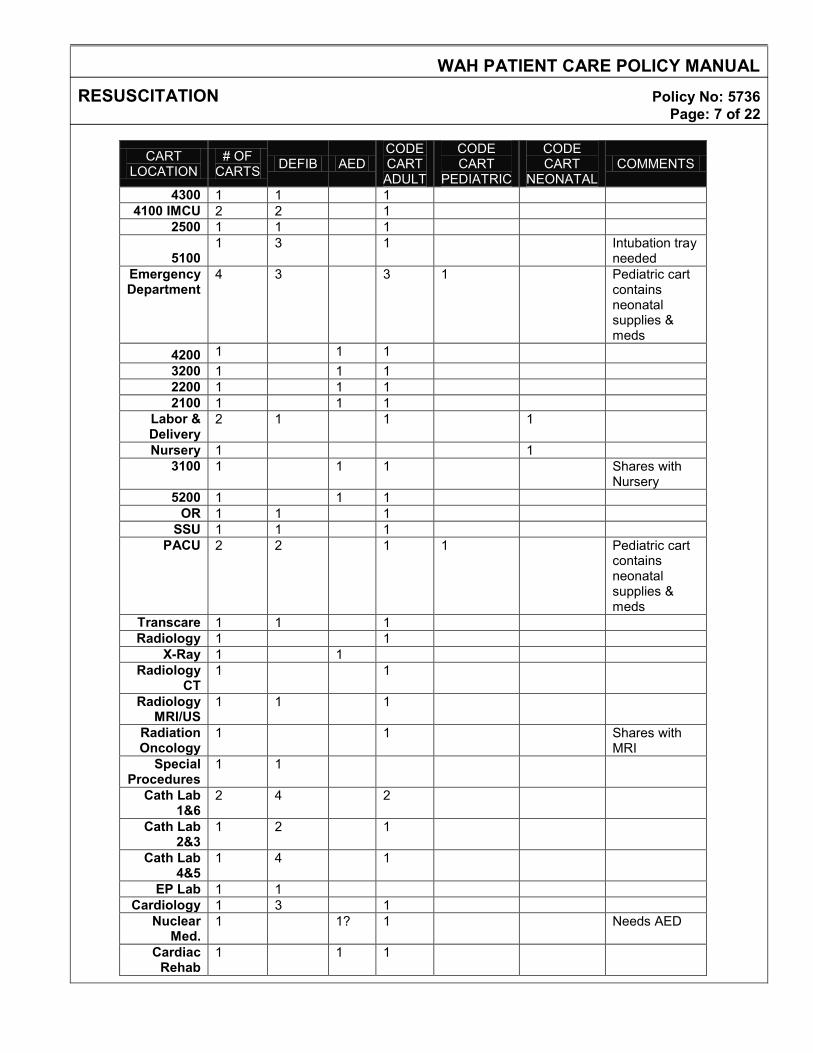
CART LOCATION
# OF CARTS DEFIB AED
CODE CART ADULT
CODE CART
PEDIATRIC
CODE CART
NEONATAL COMMENTS
4300 1 1 1 4100 IMCU 2 2 1
2500 1 1 1
5100 1 3 1 Intubation tray
needed Emergency Department
4 3 3 1 Pediatric cart contains neonatal supplies & meds
4200 1 1 1 3200 1 1 1 2200 1 1 1 2100 1 1 1
Labor & Delivery
2 1 1 1
Nursery 1 1 3100 1 1 1 Shares with
Nursery 5200 1 1 1
OR 1 1 1 SSU 1 1 1
PACU 2 2 1 1 Pediatric cart contains neonatal supplies & meds
Transcare 1 1 1 Radiology 1 1
X-Ray 1 1 Radiology
CT 1 1
Radiology MRI/US
1 1 1
Radiation Oncology
1 1 Shares with MRI
Special Procedures
1 1
Cath Lab 1&6
2 4 2
Cath Lab 2&3
1 2 1
Cath Lab 4&5
1 4 1
EP Lab 1 1 Cardiology 1 3 1
Nuclear Med.
1 1? 1 Needs AED
Cardiac Rehab
1 1 1
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 8 of 22
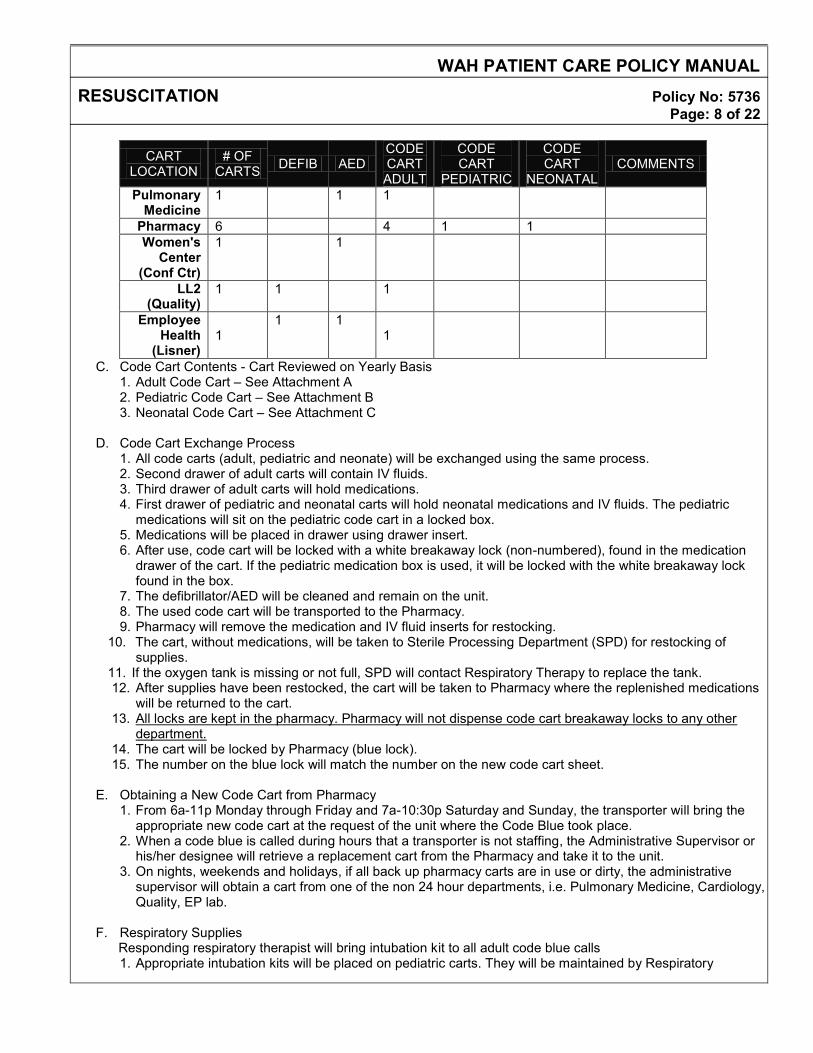
CART LOCATION
# OF CARTS DEFIB AED
CODE CART ADULT
CODE CART
PEDIATRIC
CODE CART
NEONATAL COMMENTS
Pulmonary Medicine
1 1 1
Pharmacy 6 4 1 1 Women's
Center (Conf Ctr)
1 1
LL2 (Quality)
1 1 1
Employee Health
(Lisner)
1
1 1 1
C. Code Cart Contents - Cart Reviewed on Yearly Basis 1. Adult Code Cart – See Attachment A 2. Pediatric Code Cart – See Attachment B 3. Neonatal Code Cart – See Attachment C
D. Code Cart Exchange Process
1. All code carts (adult, pediatric and neonate) will be exchanged using the same process. 2. Second drawer of adult carts will contain IV fluids. 3. Third drawer of adult carts will hold medications. 4. First drawer of pediatric and neonatal carts will hold neonatal medications and IV fluids. The pediatric
medications will sit on the pediatric code cart in a locked box. 5. Medications will be placed in drawer using drawer insert. 6. After use, code cart will be locked with a white breakaway lock (non-numbered), found in the medication
drawer of the cart. If the pediatric medication box is used, it will be locked with the white breakaway lock found in the box.
7. The defibrillator/AED will be cleaned and remain on the unit. 8. The used code cart will be transported to the Pharmacy. 9. Pharmacy will remove the medication and IV fluid inserts for restocking.
10. The cart, without medications, will be taken to Sterile Processing Department (SPD) for restocking of supplies.
11. If the oxygen tank is missing or not full, SPD will contact Respiratory Therapy to replace the tank. 12. After supplies have been restocked, the cart will be taken to Pharmacy where the replenished medications
will be returned to the cart. 13. All locks are kept in the pharmacy. Pharmacy will not dispense code cart breakaway locks to any other
department. 14. The cart will be locked by Pharmacy (blue lock). 15. The number on the blue lock will match the number on the new code cart sheet.
E. Obtaining a New Code Cart from Pharmacy
1. From 6a-11p Monday through Friday and 7a-10:30p Saturday and Sunday, the transporter will bring the appropriate new code cart at the request of the unit where the Code Blue took place.
2. When a code blue is called during hours that a transporter is not staffing, the Administrative Supervisor or his/her designee will retrieve a replacement cart from the Pharmacy and take it to the unit.
3. On nights, weekends and holidays, if all back up pharmacy carts are in use or dirty, the administrative supervisor will obtain a cart from one of the non 24 hour departments, i.e. Pulmonary Medicine, Cardiology, Quality, EP lab.
F. Respiratory Supplies
Responding respiratory therapist will bring intubation kit to all adult code blue calls 1. Appropriate intubation kits will be placed on pediatric carts. They will be maintained by Respiratory
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 9 of 22
Therapy.
2. Appropriate intubation kits will be placed on neonatal carts. They will be maintained by Respiratory Therapy.
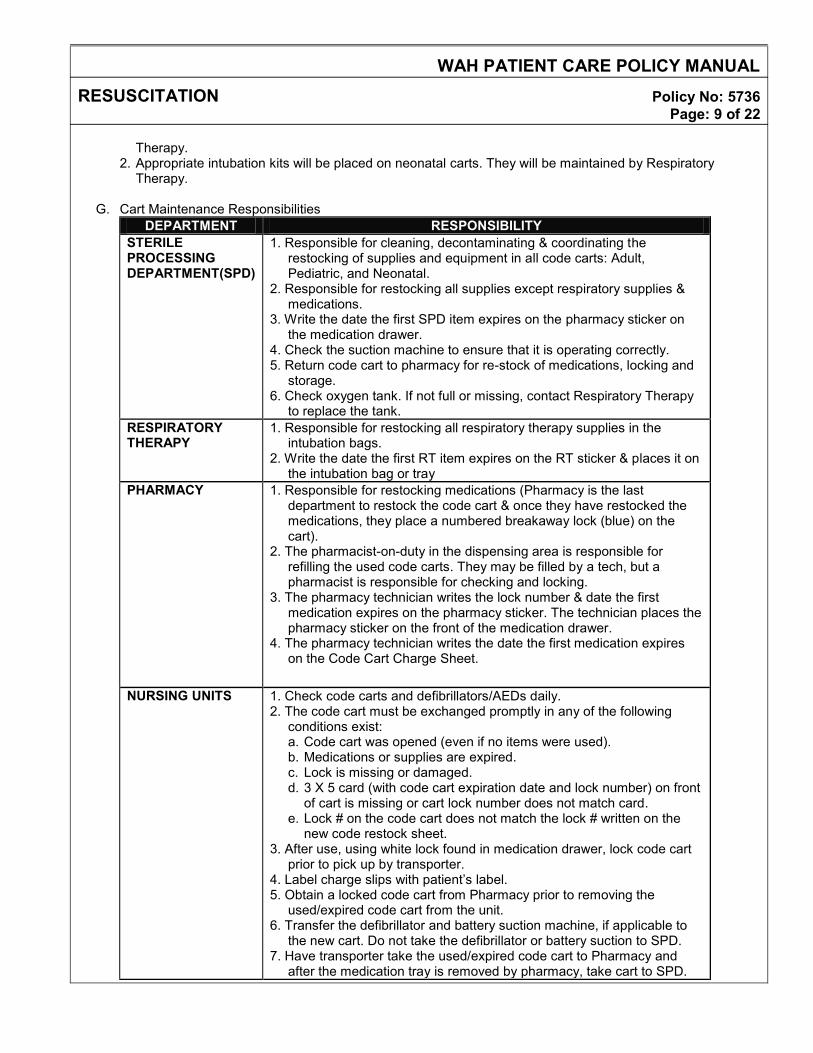
G. Cart Maintenance Responsibilities
DEPARTMENT RESPONSIBILITY STERILE PROCESSING DEPARTMENT(SPD)
1. Responsible for cleaning, decontaminating & coordinating the restocking of supplies and equipment in all code carts: Adult, Pediatric, and Neonatal.
2. Responsible for restocking all supplies except respiratory supplies & medications.
3. Write the date the first SPD item expires on the pharmacy sticker on the medication drawer.
4. Check the suction machine to ensure that it is operating correctly. 5. Return code cart to pharmacy for re-stock of medications, locking and
storage. 6. Check oxygen tank. If not full or missing, contact Respiratory Therapy
to replace the tank. RESPIRATORY THERAPY
1. Responsible for restocking all respiratory therapy supplies in the intubation bags.
2. Write the date the first RT item expires on the RT sticker & places it on the intubation bag or tray
PHARMACY 1. Responsible for restocking medications (Pharmacy is the last department to restock the code cart & once they have restocked the medications, they place a numbered breakaway lock (blue) on the cart).
2. The pharmacist-on-duty in the dispensing area is responsible for refilling the used code carts. They may be filled by a tech, but a pharmacist is responsible for checking and locking.
3. The pharmacy technician writes the lock number & date the first medication expires on the pharmacy sticker. The technician places the pharmacy sticker on the front of the medication drawer.
4. The pharmacy technician writes the date the first medication expires on the Code Cart Charge Sheet.
NURSING UNITS 1. Check code carts and defibrillators/AEDs daily. 2. The code cart must be exchanged promptly in any of the following
conditions exist: a. Code cart was opened (even if no items were used). b. Medications or supplies are expired. c. Lock is missing or damaged. d. 3 X 5 card (with code cart expiration date and lock number) on front
of cart is missing or cart lock number does not match card. e. Lock # on the code cart does not match the lock # written on the
new code restock sheet. 3. After use, using white lock found in medication drawer, lock code cart
prior to pick up by transporter. 4. Label charge slips with patient’s label. 5. Obtain a locked code cart from Pharmacy prior to removing the
used/expired code cart from the unit. 6. Transfer the defibrillator and battery suction machine, if applicable to
the new cart. Do not take the defibrillator or battery suction to SPD. 7. Have transporter take the used/expired code cart to Pharmacy and
after the medication tray is removed by pharmacy, take cart to SPD.
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 10 of 22
DEPARTMENT RESPONSIBILITY TRANSPORTERS 1. Will take the appropriate Code cart to the unit where the Code Blue
occurred as requested by the unit. 2. Upon completion of a code, take the locked, used code cart to the
pharmacy and after the medication tray is removed by pharmacy, take cart to SPD.
REFERENCES: American Academy of Pediatrics. Neonatal Resuscitation Program. 6th Edition, 2010. AAP/ACOG. Guidelines for Perinatal Care. 5th Edition, 2002. 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science. Circulation. 2010;122:S920–S933.
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 11 of 22
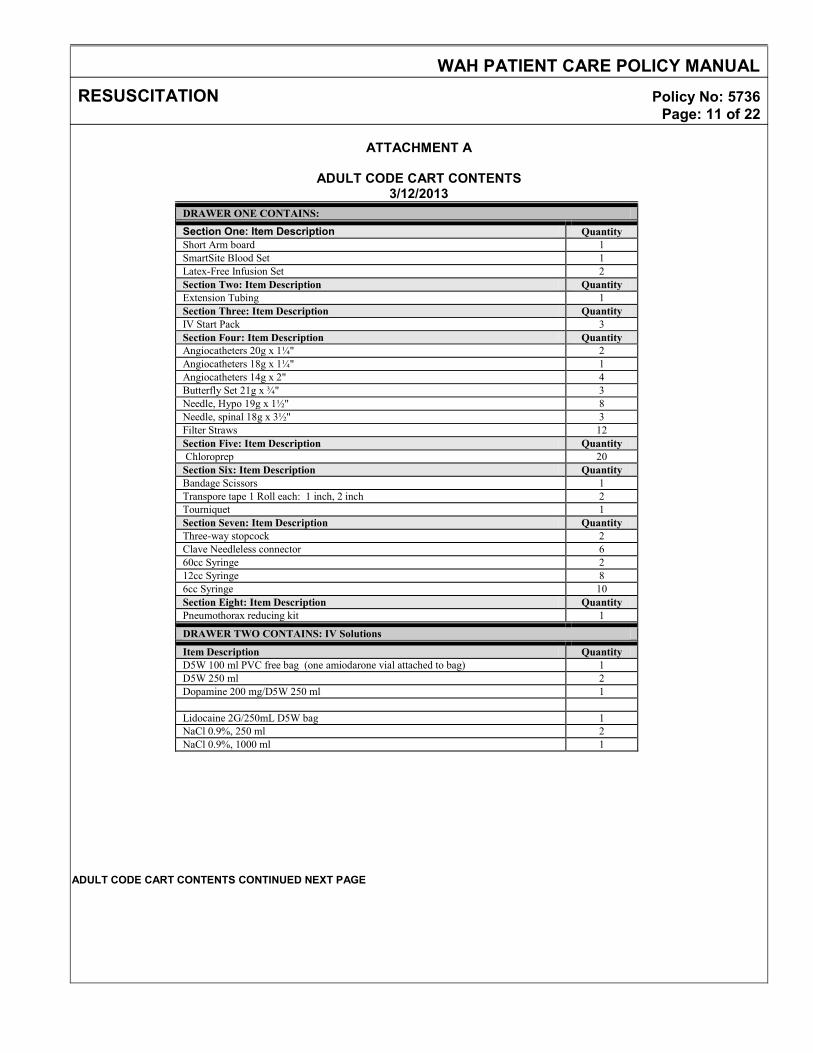
ATTACHMENT A
ADULT CODE CART CONTENTS
3/12/2013 DRAWER ONE CONTAINS:
Section One: Item Description Quantity Short Arm board 1 SmartSite Blood Set 1 Latex-Free Infusion Set 2 Section Two: Item Description Quantity Extension Tubing 1 Section Three: Item Description Quantity IV Start Pack 3 Section Four: Item Description Quantity Angiocatheters 20g x 1¼" 2 Angiocatheters 18g x 1¼" 1 Angiocatheters 14g x 2" 4 Butterfly Set 21g x ¾" 3 Needle, Hypo 19g x 1½" 8 Needle, spinal 18g x 3½" 3 Filter Straws 12 Section Five: Item Description Quantity Chloroprep 20 Section Six: Item Description Quantity Bandage Scissors 1 Transpore tape 1 Roll each: 1 inch, 2 inch 2 Tourniquet 1 Section Seven: Item Description Quantity Three-way stopcock 2 Clave Needleless connector 6 60cc Syringe 2 12cc Syringe 8 6cc Syringe 10 Section Eight: Item Description Quantity Pneumothorax reducing kit 1
DRAWER TWO CONTAINS: IV Solutions
Item Description Quantity D5W 100 ml PVC free bag (one amiodarone vial attached to bag) 1 D5W 250 ml 2 Dopamine 200 mg/D5W 250 ml 1 Lidocaine 2G/250mL D5W bag 1 NaCl 0.9%, 250 ml 2 NaCl 0.9%, 1000 ml 1
ADULT CODE CART CONTENTS CONTINUED NEXT PAGE
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 12 of 22
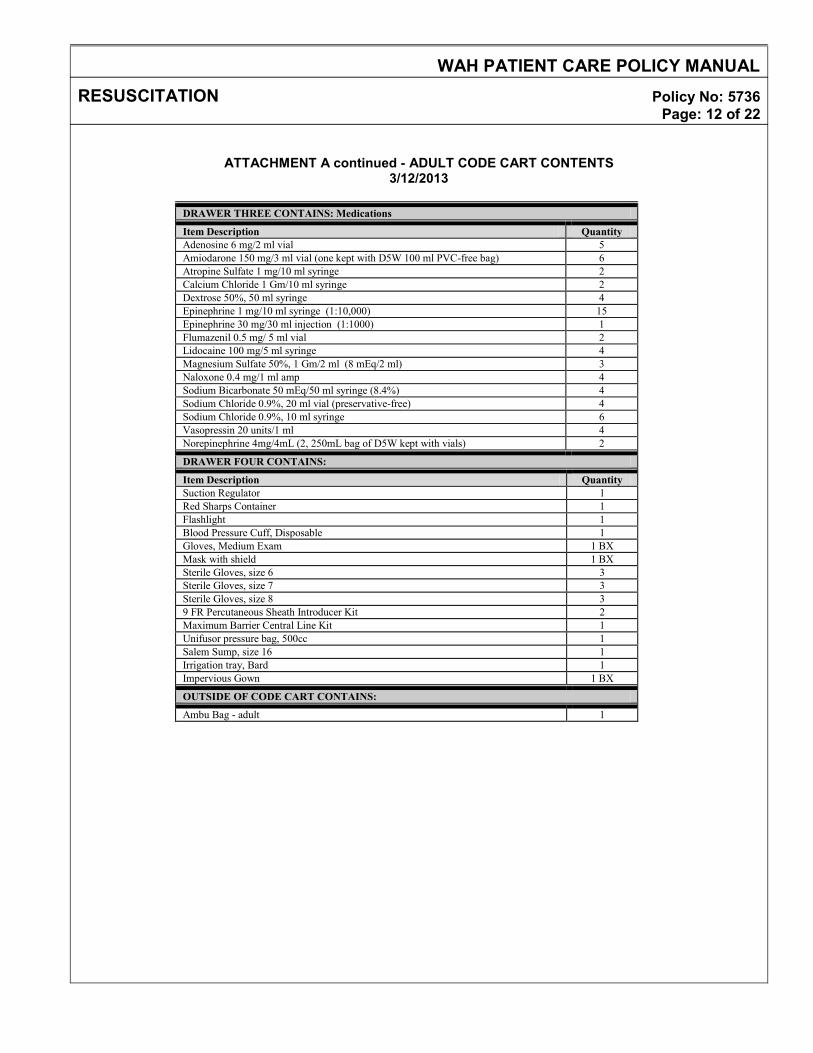
ATTACHMENT A continued - ADULT CODE CART CONTENTS 3/12/2013
DRAWER THREE CONTAINS: Medications
Item Description Quantity Adenosine 6 mg/2 ml vial 5 Amiodarone 150 mg/3 ml vial (one kept with D5W 100 ml PVC-free bag) 6 Atropine Sulfate 1 mg/10 ml syringe 2 Calcium Chloride 1 Gm/10 ml syringe 2 Dextrose 50%, 50 ml syringe 4 Epinephrine 1 mg/10 ml syringe (1:10,000) 15 Epinephrine 30 mg/30 ml injection (1:1000) 1 Flumazenil 0.5 mg/ 5 ml vial 2 Lidocaine 100 mg/5 ml syringe 4 Magnesium Sulfate 50%, 1 Gm/2 ml (8 mEq/2 ml) 3 Naloxone 0.4 mg/1 ml amp 4 Sodium Bicarbonate 50 mEq/50 ml syringe (8.4%) 4 Sodium Chloride 0.9%, 20 ml vial (preservative-free) 4 Sodium Chloride 0.9%, 10 ml syringe 6 Vasopressin 20 units/1 ml 4 Norepinephrine 4mg/4mL (2, 250mL bag of D5W kept with vials) 2
DRAWER FOUR CONTAINS:
Item Description Quantity Suction Regulator 1 Red Sharps Container 1 Flashlight 1 Blood Pressure Cuff, Disposable 1 Gloves, Medium Exam 1 BX Mask with shield 1 BX Sterile Gloves, size 6 3 Sterile Gloves, size 7 3 Sterile Gloves, size 8 3 9 FR Percutaneous Sheath Introducer Kit 2 Maximum Barrier Central Line Kit 1 Unifusor pressure bag, 500cc 1 Salem Sump, size 16 1 Irrigation tray, Bard 1 Impervious Gown 1 BX
OUTSIDE OF CODE CART CONTAINS:
Ambu Bag - adult 1
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 13 of 22
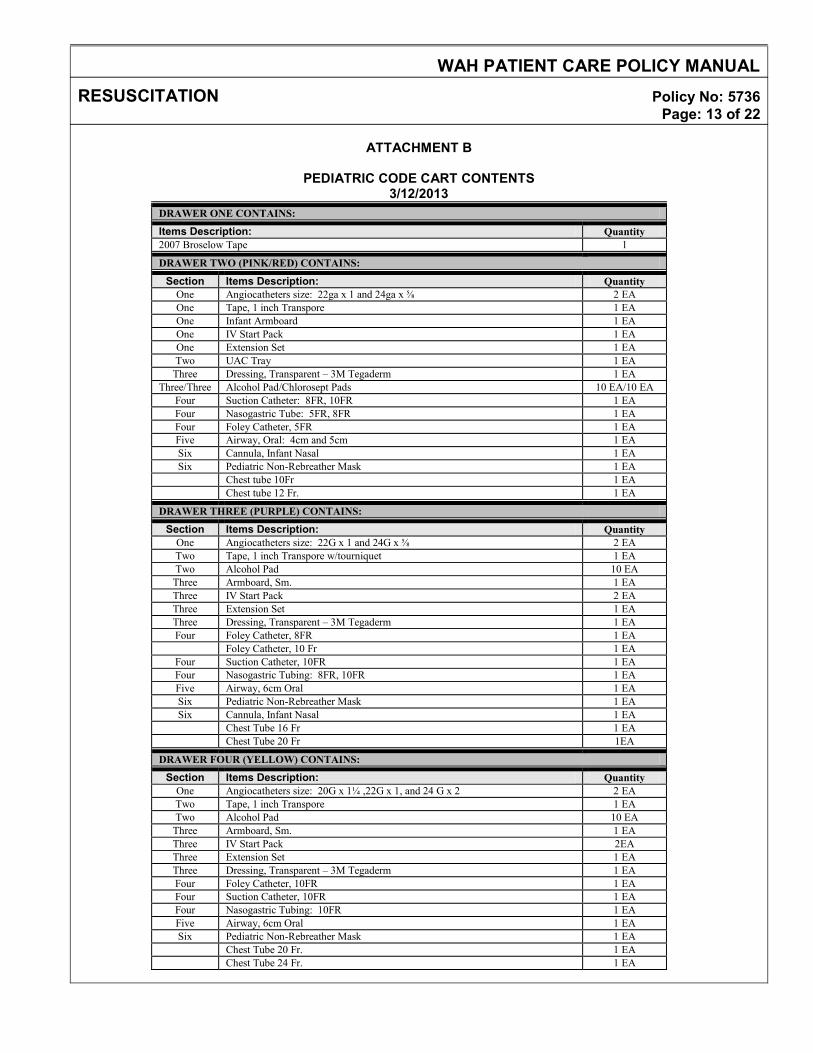
ATTACHMENT B
PEDIATRIC CODE CART CONTENTS
3/12/2013 DRAWER ONE CONTAINS:
Items Description: Quantity 2007 Broselow Tape 1
DRAWER TWO (PINK/RED) CONTAINS:
Section Items Description: Quantity One Angiocatheters size: 22ga x 1 and 24ga x ⅝ 2 EA One Tape, 1 inch Transpore 1 EA One Infant Armboard 1 EA One IV Start Pack 1 EA One Extension Set 1 EA Two UAC Tray 1 EA
Three Dressing, Transparent – 3M Tegaderm 1 EA Three/Three Alcohol Pad/Chlorosept Pads 10 EA/10 EA
Four Suction Catheter: 8FR, 10FR 1 EA Four Nasogastric Tube: 5FR, 8FR 1 EA Four Foley Catheter, 5FR 1 EA Five Airway, Oral: 4cm and 5cm 1 EA Six Cannula, Infant Nasal 1 EA Six Pediatric Non-Rebreather Mask 1 EA
Chest tube 10Fr 1 EA Chest tube 12 Fr. 1 EA
DRAWER THREE (PURPLE) CONTAINS:
Section Items Description: Quantity One Angiocatheters size: 22G x 1 and 24G x ⅝ 2 EA Two Tape, 1 inch Transpore w/tourniquet 1 EA Two Alcohol Pad 10 EA
Three Armboard, Sm. 1 EA Three IV Start Pack 2 EA Three Extension Set 1 EA Three Dressing, Transparent – 3M Tegaderm 1 EA Four Foley Catheter, 8FR 1 EA
Foley Catheter, 10 Fr 1 EA Four Suction Catheter, 10FR 1 EA Four Nasogastric Tubing: 8FR, 10FR 1 EA Five Airway, 6cm Oral 1 EA Six Pediatric Non-Rebreather Mask 1 EA Six Cannula, Infant Nasal 1 EA
Chest Tube 16 Fr 1 EA Chest Tube 20 Fr 1EA
DRAWER FOUR (YELLOW) CONTAINS:
Section Items Description: Quantity One Angiocatheters size: 20G x 1¼ ,22G x 1, and 24 G x 2 2 EA Two Tape, 1 inch Transpore 1 EA Two Alcohol Pad 10 EA
Three Armboard, Sm. 1 EA Three IV Start Pack 2EA Three Extension Set 1 EA Three Dressing, Transparent – 3M Tegaderm 1 EA Four Foley Catheter, 10FR 1 EA Four Suction Catheter, 10FR 1 EA Four Nasogastric Tubing: 10FR 1 EA Five Airway, 6cm Oral 1 EA Six Pediatric Non-Rebreather Mask 1 EA
Chest Tube 20 Fr. 1 EA Chest Tube 24 Fr. 1 EA
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 14 of 22
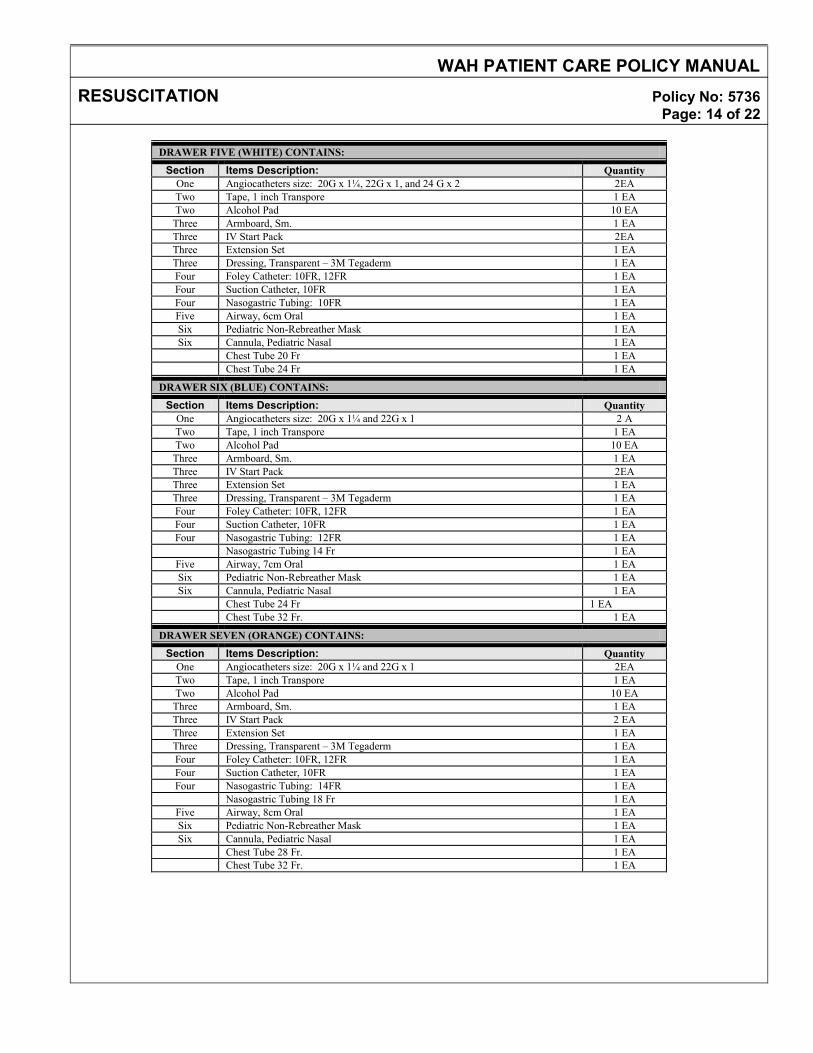
DRAWER FIVE (WHITE) CONTAINS:
Section Items Description: Quantity One Angiocatheters size: 20G x 1¼, 22G x 1, and 24 G x 2 2EA Two Tape, 1 inch Transpore 1 EA Two Alcohol Pad 10 EA
Three Armboard, Sm. 1 EA Three IV Start Pack 2EA Three Extension Set 1 EA Three Dressing, Transparent – 3M Tegaderm 1 EA Four Foley Catheter: 10FR, 12FR 1 EA Four Suction Catheter, 10FR 1 EA Four Nasogastric Tubing: 10FR 1 EA Five Airway, 6cm Oral 1 EA Six Pediatric Non-Rebreather Mask 1 EA Six Cannula, Pediatric Nasal 1 EA
Chest Tube 20 Fr 1 EA Chest Tube 24 Fr 1 EA
DRAWER SIX (BLUE) CONTAINS:
Section Items Description: Quantity One Angiocatheters size: 20G x 1¼ and 22G x 1 2 A Two Tape, 1 inch Transpore 1 EA Two Alcohol Pad 10 EA
Three Armboard, Sm. 1 EA Three IV Start Pack 2EA Three Extension Set 1 EA Three Dressing, Transparent – 3M Tegaderm 1 EA Four Foley Catheter: 10FR, 12FR 1 EA Four Suction Catheter, 10FR 1 EA Four Nasogastric Tubing: 12FR 1 EA
Nasogastric Tubing 14 Fr 1 EA Five Airway, 7cm Oral 1 EA Six Pediatric Non-Rebreather Mask 1 EA Six Cannula, Pediatric Nasal 1 EA
Chest Tube 24 Fr 1 EA Chest Tube 32 Fr. 1 EA
DRAWER SEVEN (ORANGE) CONTAINS:
Section Items Description: Quantity One Angiocatheters size: 20G x 1¼ and 22G x 1 2EA Two Tape, 1 inch Transpore 1 EA Two Alcohol Pad 10 EA
Three Armboard, Sm. 1 EA Three IV Start Pack 2 EA Three Extension Set 1 EA Three Dressing, Transparent – 3M Tegaderm 1 EA Four Foley Catheter: 10FR, 12FR 1 EA Four Suction Catheter, 10FR 1 EA Four Nasogastric Tubing: 14FR 1 EA
Nasogastric Tubing 18 Fr 1 EA Five Airway, 8cm Oral 1 EA Six Pediatric Non-Rebreather Mask 1 EA Six Cannula, Pediatric Nasal 1 EA
Chest Tube 28 Fr. 1 EA Chest Tube 32 Fr. 1 EA
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 15 of 22
ATTACHMENT B continued - PEDIATRIC CODE CART CONTENTS
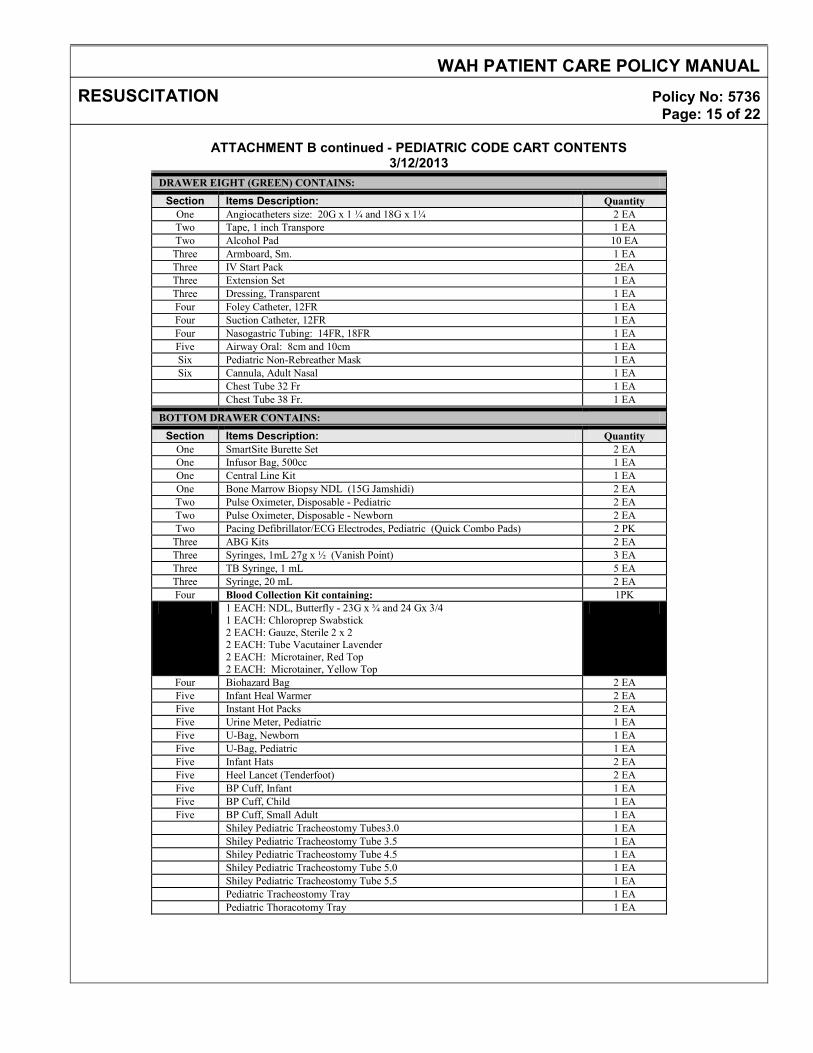
3/12/2013 DRAWER EIGHT (GREEN) CONTAINS:
Section Items Description: Quantity One Angiocatheters size: 20G x 1 ¼ and 18G x 1¼ 2 EA Two Tape, 1 inch Transpore 1 EA Two Alcohol Pad 10 EA
Three Armboard, Sm. 1 EA Three IV Start Pack 2EA Three Extension Set 1 EA Three Dressing, Transparent 1 EA Four Foley Catheter, 12FR 1 EA Four Suction Catheter, 12FR 1 EA Four Nasogastric Tubing: 14FR, 18FR 1 EA Five Airway Oral: 8cm and 10cm 1 EA Six Pediatric Non-Rebreather Mask 1 EA Six Cannula, Adult Nasal 1 EA
Chest Tube 32 Fr 1 EA Chest Tube 38 Fr. 1 EA
BOTTOM DRAWER CONTAINS:
Section Items Description: Quantity One SmartSite Burette Set 2 EA One Infusor Bag, 500cc 1 EA One Central Line Kit 1 EA One Bone Marrow Biopsy NDL (15G Jamshidi) 2 EA Two Pulse Oximeter, Disposable - Pediatric 2 EA Two Pulse Oximeter, Disposable - Newborn 2 EA Two Pacing Defibrillator/ECG Electrodes, Pediatric (Quick Combo Pads) 2 PK
Three ABG Kits 2 EA Three Syringes, 1mL 27g x ½ (Vanish Point) 3 EA Three TB Syringe, 1 mL 5 EA Three Syringe, 20 mL 2 EA Four Blood Collection Kit containing: 1PK
1 EACH: NDL, Butterfly - 23G x ¾ and 24 Gx 3/4 1 EACH: Chloroprep Swabstick 2 EACH: Gauze, Sterile 2 x 2 2 EACH: Tube Vacutainer Lavender 2 EACH: Microtainer, Red Top 2 EACH: Microtainer, Yellow Top
Four Biohazard Bag 2 EA Five Infant Heal Warmer 2 EA Five Instant Hot Packs 2 EA Five Urine Meter, Pediatric 1 EA Five U-Bag, Newborn 1 EA Five U-Bag, Pediatric 1 EA Five Infant Hats 2 EA Five Heel Lancet (Tenderfoot) 2 EA Five BP Cuff, Infant 1 EA Five BP Cuff, Child 1 EA Five BP Cuff, Small Adult 1 EA
Shiley Pediatric Tracheostomy Tubes3.0 1 EA Shiley Pediatric Tracheostomy Tube 3.5 1 EA Shiley Pediatric Tracheostomy Tube 4.5 1 EA Shiley Pediatric Tracheostomy Tube 5.0 1 EA Shiley Pediatric Tracheostomy Tube 5.5 1 EA Pediatric Tracheostomy Tray 1 EA Pediatric Thoracotomy Tray 1 EA
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 16 of 22
ATTACHMENT B continued - PEDIATRIC CODE CART CONTENTS 3/12/2013
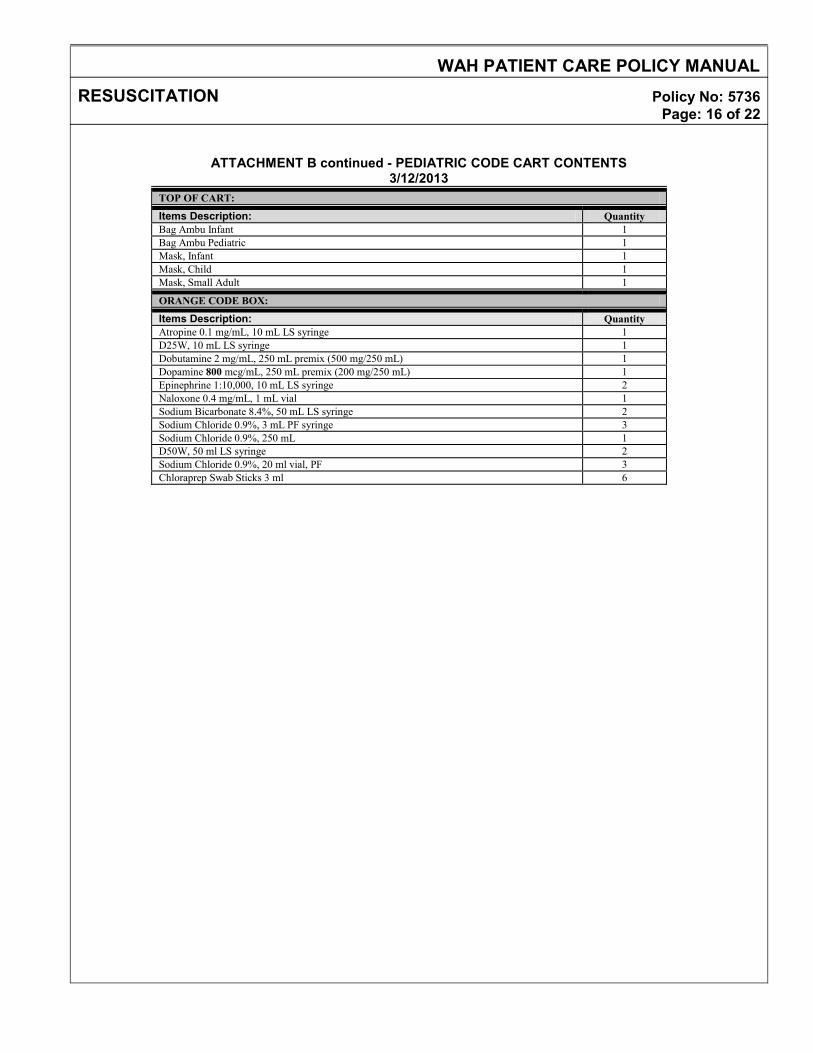
TOP OF CART:
Items Description: Quantity Bag Ambu Infant 1 Bag Ambu Pediatric 1 Mask, Infant 1 Mask, Child 1 Mask, Small Adult 1
ORANGE CODE BOX:
Items Description: Quantity Atropine 0.1 mg/mL, 10 mL LS syringe 1 D25W, 10 mL LS syringe 1 Dobutamine 2 mg/mL, 250 mL premix (500 mg/250 mL) 1 Dopamine 800 mcg/mL, 250 mL premix (200 mg/250 mL) 1 Epinephrine 1:10,000, 10 mL LS syringe 2 Naloxone 0.4 mg/mL, 1 mL vial 1 Sodium Bicarbonate 8.4%, 50 mL LS syringe 2 Sodium Chloride 0.9%, 3 mL PF syringe 3 Sodium Chloride 0.9%, 250 mL 1 D50W, 50 ml LS syringe 2 Sodium Chloride 0.9%, 20 ml vial, PF 3 Chloraprep Swab Sticks 3 ml 6
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 17 of 22
ATTACHMENT C
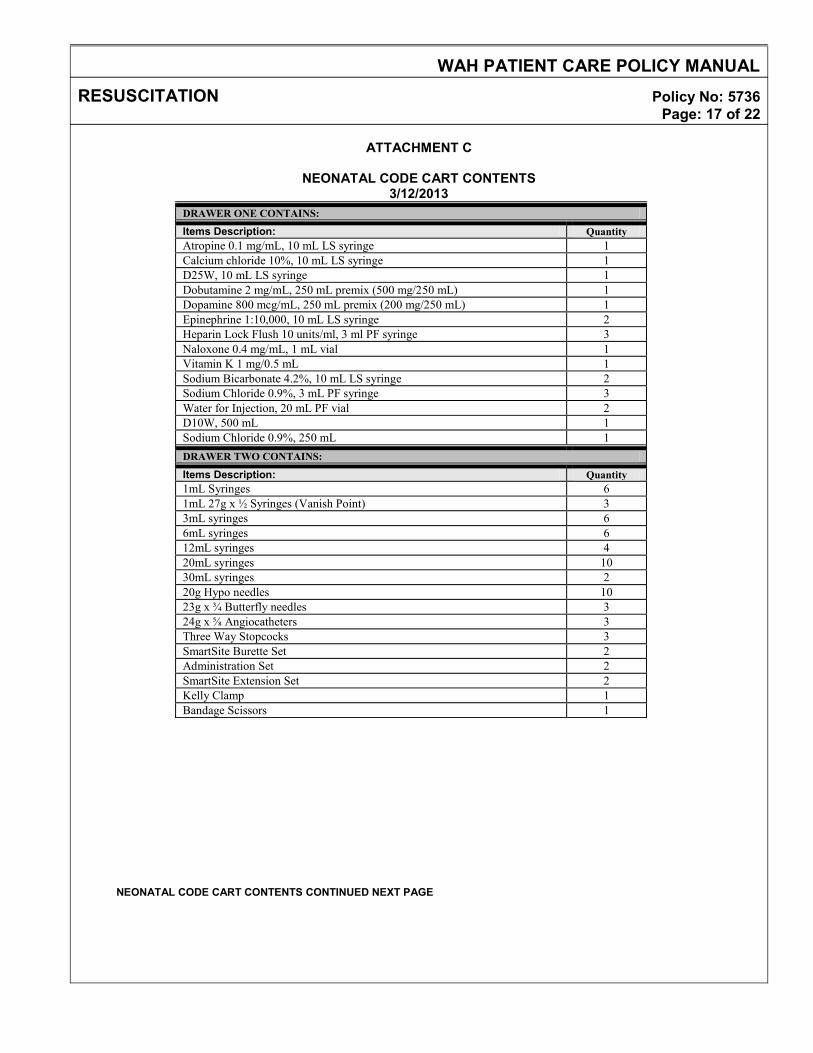
NEONATAL CODE CART CONTENTS
3/12/2013 DRAWER ONE CONTAINS:
Items Description: Quantity Atropine 0.1 mg/mL, 10 mL LS syringe 1 Calcium chloride 10%, 10 mL LS syringe 1 D25W, 10 mL LS syringe 1 Dobutamine 2 mg/mL, 250 mL premix (500 mg/250 mL) 1 Dopamine 800 mcg/mL, 250 mL premix (200 mg/250 mL) 1 Epinephrine 1:10,000, 10 mL LS syringe 2 Heparin Lock Flush 10 units/ml, 3 ml PF syringe 3 Naloxone 0.4 mg/mL, 1 mL vial 1 Vitamin K 1 mg/0.5 mL 1 Sodium Bicarbonate 4.2%, 10 mL LS syringe 2 Sodium Chloride 0.9%, 3 mL PF syringe 3 Water for Injection, 20 mL PF vial 2 D10W, 500 mL 1 Sodium Chloride 0.9%, 250 mL 1 DRAWER TWO CONTAINS:
Items Description: Quantity 1mL Syringes 6 1mL 27g x ½ Syringes (Vanish Point) 3 3mL syringes 6 6mL syringes 6 12mL syringes 4 20mL syringes 10 30mL syringes 2 20g Hypo needles 10 23g x ¾ Butterfly needles 3 24g x ⅝ Angiocatheters 3 Three Way Stopcocks 3 SmartSite Burette Set 2 Administration Set 2 SmartSite Extension Set 2 Kelly Clamp 1 Bandage Scissors 1
NEONATAL CODE CART CONTENTS CONTINUED NEXT PAGE
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 18 of 22
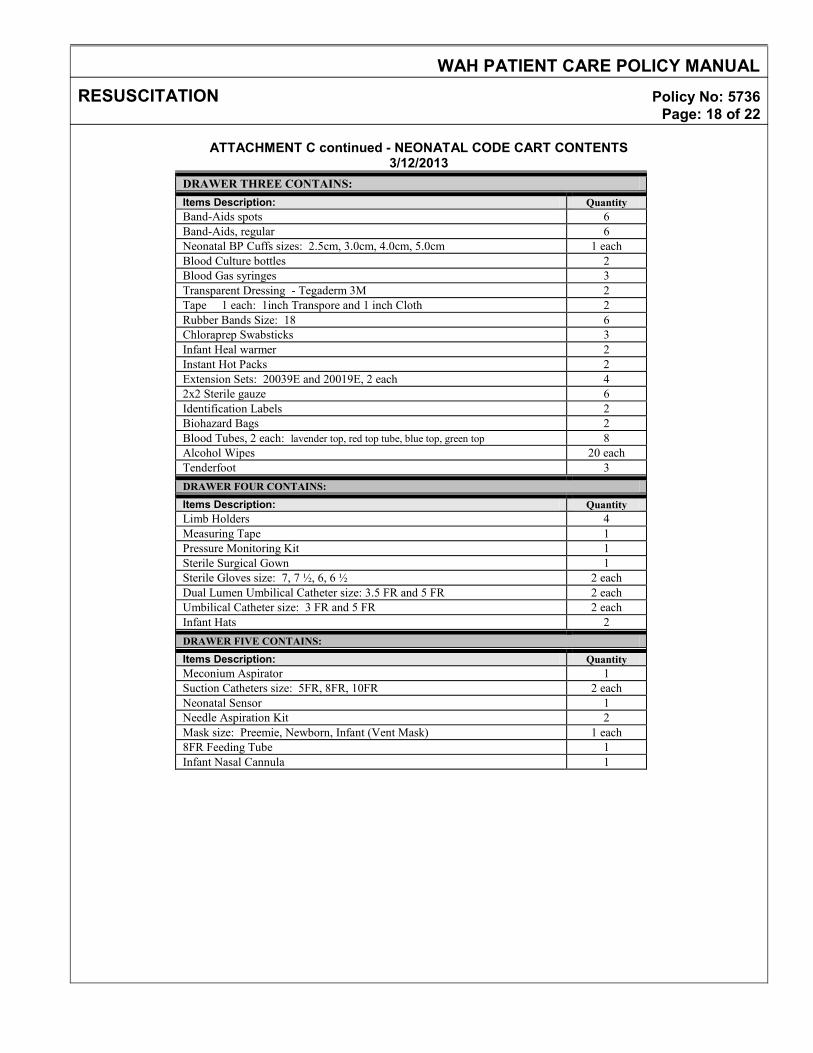
ATTACHMENT C continued - NEONATAL CODE CART CONTENTS
3/12/2013 DRAWER THREE CONTAINS: Items Description: Quantity Band-Aids spots 6 Band-Aids, regular 6 Neonatal BP Cuffs sizes: 2.5cm, 3.0cm, 4.0cm, 5.0cm 1 each Blood Culture bottles 2 Blood Gas syringes 3 Transparent Dressing - Tegaderm 3M 2 Tape 1 each: 1inch Transpore and 1 inch Cloth 2 Rubber Bands Size: 18 6 Chloraprep Swabsticks 3 Infant Heal warmer 2 Instant Hot Packs 2 Extension Sets: 20039E and 20019E, 2 each 4 2x2 Sterile gauze 6 Identification Labels 2 Biohazard Bags 2 Blood Tubes, 2 each: lavender top, red top tube, blue top, green top 8 Alcohol Wipes 20 each Tenderfoot 3 DRAWER FOUR CONTAINS:
Items Description: Quantity Limb Holders 4 Measuring Tape 1 Pressure Monitoring Kit 1 Sterile Surgical Gown 1 Sterile Gloves size: 7, 7 ½, 6, 6 ½ 2 each Dual Lumen Umbilical Catheter size: 3.5 FR and 5 FR 2 each Umbilical Catheter size: 3 FR and 5 FR 2 each Infant Hats 2 DRAWER FIVE CONTAINS:
Items Description: Quantity Meconium Aspirator 1 Suction Catheters size: 5FR, 8FR, 10FR 2 each Neonatal Sensor 1 Needle Aspiration Kit 2 Mask size: Preemie, Newborn, Infant (Vent Mask) 1 each 8FR Feeding Tube 1 Infant Nasal Cannula 1
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 19 of 22
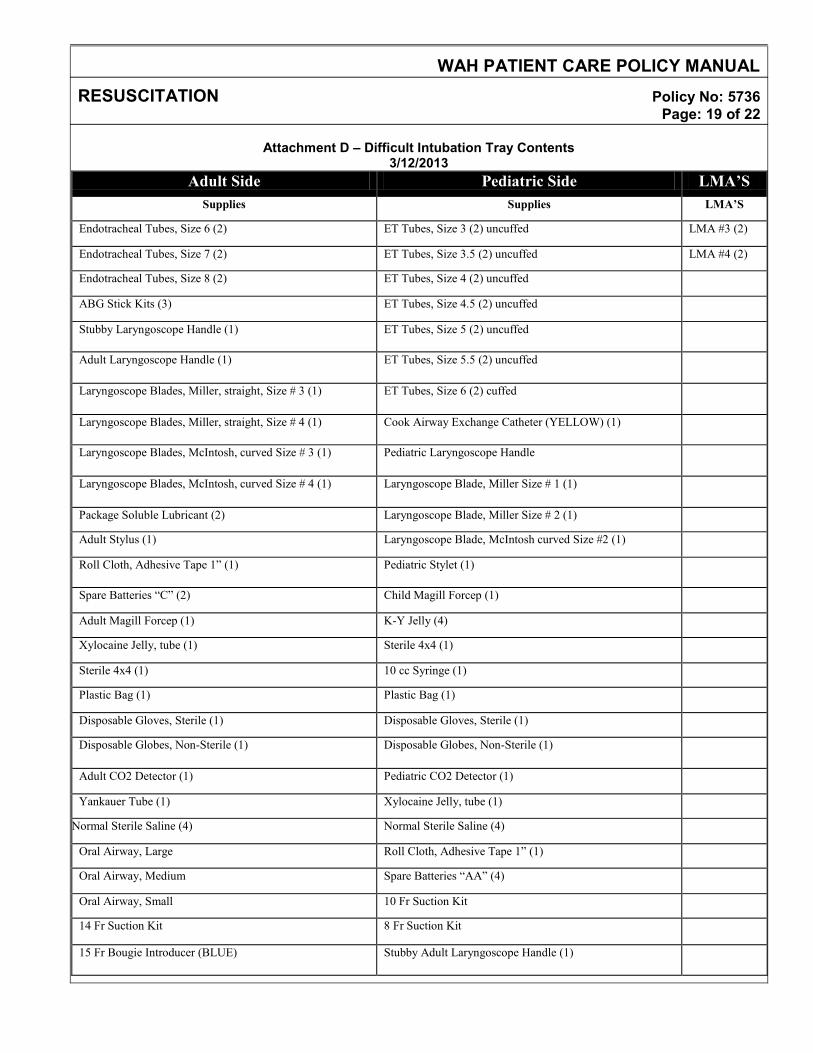
Attachment D – Difficult Intubation Tray Contents
3/12/2013 Adult Side Pediatric Side LMA’S
Supplies Supplies LMA’S
Endotracheal Tubes, Size 6 (2) ET Tubes, Size 3 (2) uncuffed LMA #3 (2)
Endotracheal Tubes, Size 7 (2) ET Tubes, Size 3.5 (2) uncuffed LMA #4 (2)
Endotracheal Tubes, Size 8 (2) ET Tubes, Size 4 (2) uncuffed
ABG Stick Kits (3) ET Tubes, Size 4.5 (2) uncuffed
Stubby Laryngoscope Handle (1) ET Tubes, Size 5 (2) uncuffed
Adult Laryngoscope Handle (1) ET Tubes, Size 5.5 (2) uncuffed
Laryngoscope Blades, Miller, straight, Size # 3 (1) ET Tubes, Size 6 (2) cuffed
Laryngoscope Blades, Miller, straight, Size # 4 (1) Cook Airway Exchange Catheter (YELLOW) (1)
Laryngoscope Blades, McIntosh, curved Size # 3 (1) Pediatric Laryngoscope Handle
Laryngoscope Blades, McIntosh, curved Size # 4 (1) Laryngoscope Blade, Miller Size # 1 (1)
Package Soluble Lubricant (2) Laryngoscope Blade, Miller Size # 2 (1)
Adult Stylus (1) Laryngoscope Blade, McIntosh curved Size #2 (1)
Roll Cloth, Adhesive Tape 1” (1) Pediatric Stylet (1)
Spare Batteries “C” (2) Child Magill Forcep (1)
Adult Magill Forcep (1) K-Y Jelly (4)
Xylocaine Jelly, tube (1) Sterile 4x4 (1)
Sterile 4x4 (1) 10 cc Syringe (1)
Plastic Bag (1) Plastic Bag (1)
Disposable Gloves, Sterile (1) Disposable Gloves, Sterile (1)
Disposable Globes, Non-Sterile (1) Disposable Globes, Non-Sterile (1)
Adult CO2 Detector (1) Pediatric CO2 Detector (1)
Yankauer Tube (1) Xylocaine Jelly, tube (1)
Normal Sterile Saline (4) Normal Sterile Saline (4)
Oral Airway, Large Roll Cloth, Adhesive Tape 1” (1)
Oral Airway, Medium Spare Batteries “AA” (4)
Oral Airway, Small 10 Fr Suction Kit
14 Fr Suction Kit 8 Fr Suction Kit
15 Fr Bougie Introducer (BLUE) Stubby Adult Laryngoscope Handle (1)
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 20 of 22
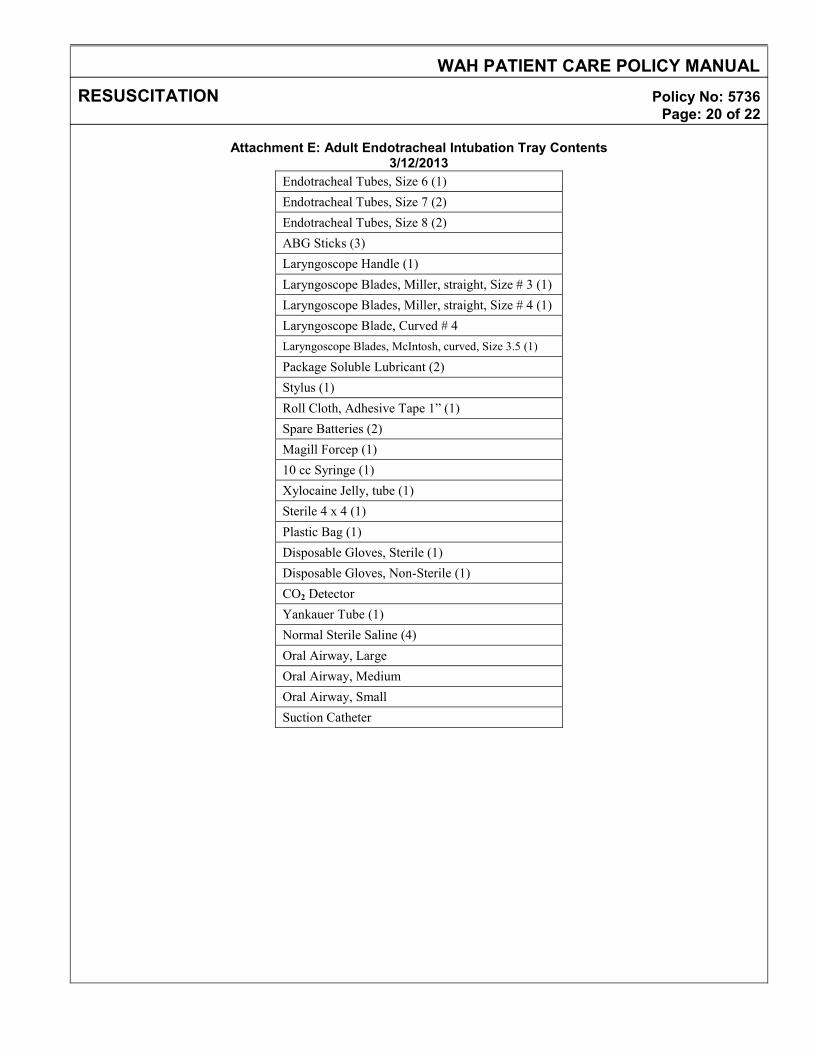
Attachment E: Adult Endotracheal Intubation Tray Contents
3/12/2013 Endotracheal Tubes, Size 6 (1) Endotracheal Tubes, Size 7 (2) Endotracheal Tubes, Size 8 (2) ABG Sticks (3) Laryngoscope Handle (1) Laryngoscope Blades, Miller, straight, Size # 3 (1) Laryngoscope Blades, Miller, straight, Size # 4 (1) Laryngoscope Blade, Curved # 4 Laryngoscope Blades, McIntosh, curved, Size 3.5 (1)
Package Soluble Lubricant (2) Stylus (1) Roll Cloth, Adhesive Tape 1” (1) Spare Batteries (2) Magill Forcep (1) 10 cc Syringe (1) Xylocaine Jelly, tube (1) Sterile 4 x 4 (1) Plastic Bag (1) Disposable Gloves, Sterile (1) Disposable Gloves, Non-Sterile (1) CO2 Detector Yankauer Tube (1) Normal Sterile Saline (4) Oral Airway, Large Oral Airway, Medium Oral Airway, Small Suction Catheter
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 21 of 22
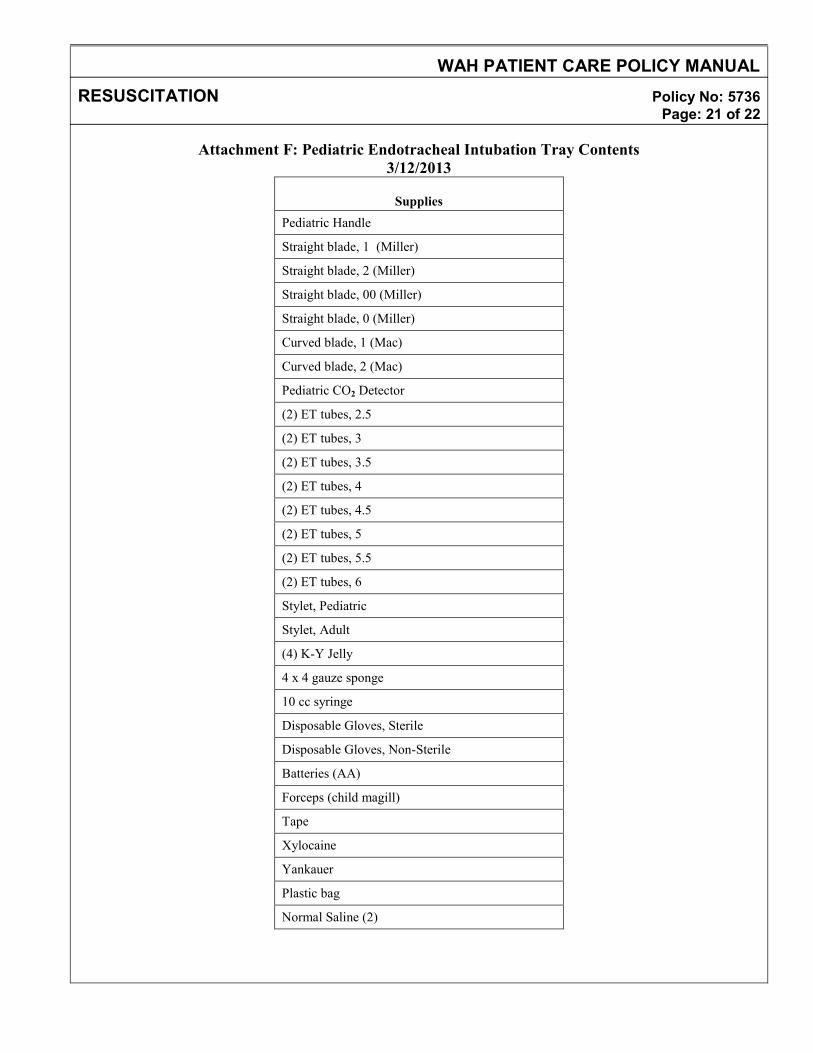
Attachment F: Pediatric Endotracheal Intubation Tray Contents 3/12/2013
Supplies
Pediatric Handle
Straight blade, 1 (Miller)
Straight blade, 2 (Miller)
Straight blade, 00 (Miller)
Straight blade, 0 (Miller)
Curved blade, 1 (Mac)
Curved blade, 2 (Mac)
Pediatric CO2 Detector
(2) ET tubes, 2.5
(2) ET tubes, 3
(2) ET tubes, 3.5
(2) ET tubes, 4
(2) ET tubes, 4.5
(2) ET tubes, 5
(2) ET tubes, 5.5
(2) ET tubes, 6
Stylet, Pediatric
Stylet, Adult
(4) K-Y Jelly
4 x 4 gauze sponge
10 cc syringe
Disposable Gloves, Sterile
Disposable Gloves, Non-Sterile
Batteries (AA)
Forceps (child magill)
Tape
Xylocaine
Yankauer
Plastic bag
Normal Saline (2)
WAH PATIENT CARE POLICY MANUAL
RESUSCITATION Policy No: 5736 Page: 22 of 22
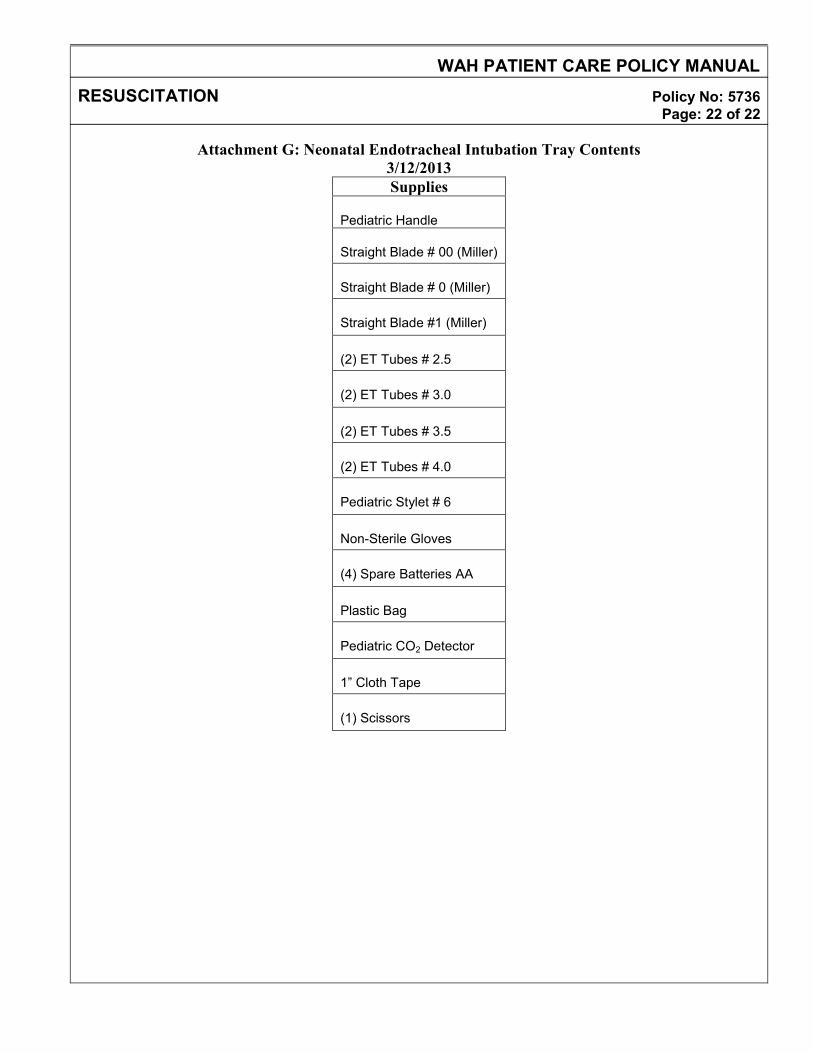
Attachment G: Neonatal Endotracheal Intubation Tray Contents 3/12/2013 Supplies
Pediatric Handle
Straight Blade # 00 (Miller)
Straight Blade # 0 (Miller)
Straight Blade #1 (Miller)
(2) ET Tubes # 2.5
(2) ET Tubes # 3.0
(2) ET Tubes # 3.5
(2) ET Tubes # 4.0
Pediatric Stylet # 6
Non-Sterile Gloves
(4) Spare Batteries AA
Plastic Bag
Pediatric CO2 Detector
1” Cloth Tape
(1) Scissors
WASHINGTON ADVENTIST HOSPITAL SPECIAL CARE NURSERY
WOMEN’S SERVICES COLLABORATIVE PRACTICE STANDARDS
Effective Date: 6/04 Policy: WWS 9302 Comments: Origin: SCN Reviewed:4/13 Approved: 6/04 Revised: New,4/13 Page 1 of 3
Admission To Special Care Nursery
SCOPE: This policy applies to Special Care Nursery I. PURPOSE
To provide care for all infants <28 days of life requiring specialized neonatal care within Washington Adventist Hospital.
II. POLICY The Special Care Nursery (SCN) is a level II nursery, designated, equipped and staffed to care for ill neonate. Our patient population includes premature infants, infants with respiratory difficulties, infectious disease, nutritional deficits, hematological problems, and those requiring observation for problems following delivery. All infants are admitted under the care of the staff neonatologists/pediatricians. A. Admission Criteria
1. Infants less than 4 lbs. (1818 grams) or less than or equal to 32 weeks gestation. 2. Infants in respiratory distress requiring any ventilatory support or
supplemental oxygen. 3. Infants requiring intravascular fluid or medication. 4. Infants who are cyanotic. 5. Infants with major anomalies. 6. Infants requiring vital signs more frequently than every 4 hours. 7. Infants requiring gavage feeding.
B. Admission Note and Assessment Sheet 1. All patients admitted to the SCN will have an Admission Note and
Newborn Assessment Form completed. 2. Vital signs should be completed within 15 minutes of admission. The
physical assessment will be completed within 6 hours of admission and the Newborn Assessment Form will be completed.
C. Identification Process 1. A four-part bracelet will identify all infants. (See Infant Identification and Safety
CPS.
G:\WOMENS_SVC\ Policies Final\ Admission to Special Care Nursery
WASHINGTON ADVENTIST HOSPITAL SPECIAL CARE NURSERY
WOMEN’S SERVICES COLLABORATIVE PRACTICE STANDARDS
Effective Date: 6/04 Policy: WWS 9302 Comments: Origin: SCN Reviewed:4/13 Approved: 6/04 Revised: New,4/13 Page 2 of 3
Admission To Special Care Nursery
2. A bracelet is placed on each of the infant’s ankles, by the L&D RN; one bracelet is placed on mother’s wrist and the fourth bracelet is placed on the support person’s wrist. The mother will designate the support person. The nurse must apply the bracelet.
3. When the infant is admitted to the SCN, the RN will check the infant’s ID bands to make sure they are properly applied and that the information matches the information on the Newborn Identification Form.
III. PROCEDURE: A. The SCN RN will:
1. Prepare radiant warmer, oxygen, ventilator (as ordered), suction, cardiac monitor, IV fluids, tubes for labs, scale, UAC tray, and warm packs. Notify respiratory therapy practitioner.
2. Check the neonate’s ID band pursuant to Infant Identification and Safety CPS. 3. Check bands for accuracy with L&D RN. 4. Document time and date on the Newborn Identification Sheet and sign with L&D
RN verifying correct and matching baby Identification Bands. 5. Weigh and measure length of the neonate and document. 6. Maintain thermoregulation by placing the neonate under radiant warmer, start
O2 as ordered. 7. Place neonate on the cardiac monitor and oximeter. 8. Obtain neonate’s vital signs: respiratory rate, apical pulse and blood pressure in
all extremities, as ordered by physician. 9. Obtain Accucheck. 10. Administer vitamin K 11. Administer erythromycin ointment 12. Draw blood as ordered. 13. Assist with or insert IV and begin IV therapy per physician’s orders. 14. Document all information on the SCN flow sheet, Code Pink Form if called
for, and Nurses’ Notes and Assessment Sheet. 15. Notify MD of any change in status.
G:\WOMENS_SVC\ Policies Final\ Admission to Special Care Nursery
WASHINGTON ADVENTIST HOSPITAL
SPECIAL CARE NURSERY WOMEN’S SERVICES
COLLABORATIVE PRACTICE STANDARDS
Effective Date: 6/04 Policy: WWS 9302 Comments: Origin: SCN Reviewed:4/13 Approved: 6/04
Revised: New,4/13 Page 3 of 3
Admission To Special Care Nursery
IV . TEACHING:
Educate newborn's parents of the following: A. Purpose of tests, cardiac monitor, IV lines, and care needed.
B Provide emotional support by watching for verbal and nonverbal signs. C..Maintain open communication D. Instruct need for all visitors to wash hands thoroughly prior to entering nursery E. Encourage proper touch, based on needs of baby F. Encourage and initiation pumping if mother plans to breastfeed. G. Encourage parents to ask questions to reduce fears H. Encourage Skin to Skin when appropriate
REFERENCES: AAP & ACOG Guidelines for Perinatal Care 7th Ed Washington DC
Deacon, J. & O'Neill, P. 1999. Core Curriculum for Neonatal Intensive Care Nursing, 2nd
Ed., Philadelphia: W.B. Saunders & Co.
Cloherty, John P., Eichenwald, Eric C., Hansen, Anne R. and Stark, Ann R. Manual of Neonatal Care 7th Ed. 2012 Lippincott Williams & Wilkins
G:\WOMENS_SVC\ Policies Final\ Admission to Special Care Nursery
WASHINGTON ADVENTIST HOSPITAL LABORATORY POLICY
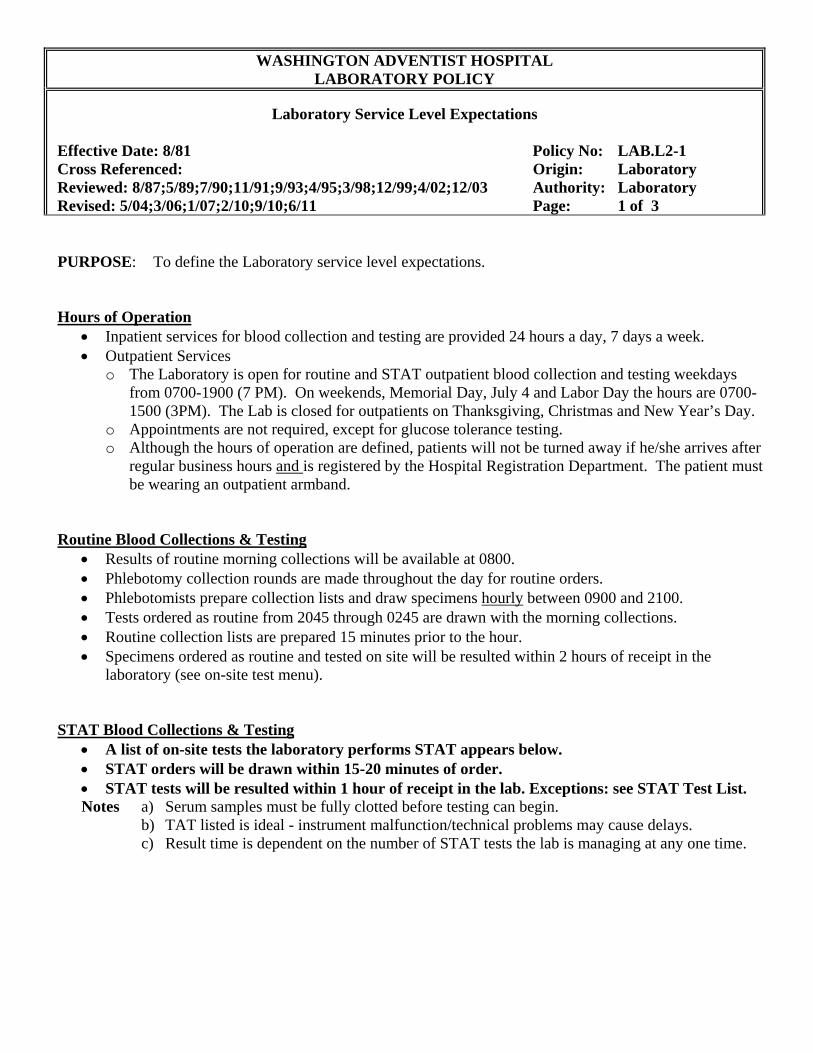
Laboratory Service Level Expectations Effective Date: 8/81 Policy No: LAB.L2-1 Cross Referenced: Origin: Laboratory Reviewed: 8/87;5/89;7/90;11/91;9/93;4/95;3/98;12/99;4/02;12/03 Authority: Laboratory Revised: 5/04;3/06;1/07;2/10;9/10;6/11 Page: 1 of 3 PURPOSE: To define the Laboratory service level expectations. Hours of Operation
Inpatient services for blood collection and testing are provided 24 hours a day, 7 days a week. Outpatient Services
o The Laboratory is open for routine and STAT outpatient blood collection and testing weekdays from 0700-1900 (7 PM). On weekends, Memorial Day, July 4 and Labor Day the hours are 0700-1500 (3PM). The Lab is closed for outpatients on Thanksgiving, Christmas and New Year’s Day.
o Appointments are not required, except for glucose tolerance testing. o Although the hours of operation are defined, patients will not be turned away if he/she arrives after
regular business hours and is registered by the Hospital Registration Department. The patient must be wearing an outpatient armband.
Routine Blood Collections & Testing
Results of routine morning collections will be available at 0800. Phlebotomy collection rounds are made throughout the day for routine orders. Phlebotomists prepare collection lists and draw specimens hourly between 0900 and 2100. Tests ordered as routine from 2045 through 0245 are drawn with the morning collections. Routine collection lists are prepared 15 minutes prior to the hour. Specimens ordered as routine and tested on site will be resulted within 2 hours of receipt in the
laboratory (see on-site test menu). STAT Blood Collections & Testing
A list of on-site tests the laboratory performs STAT appears below. STAT orders will be drawn within 15-20 minutes of order. STAT tests will be resulted within 1 hour of receipt in the lab. Exceptions: see STAT Test List. Notes a) Serum samples must be fully clotted before testing can begin.
b) TAT listed is ideal - instrument malfunction/technical problems may cause delays. c) Result time is dependent on the number of STAT tests the lab is managing at any one time.
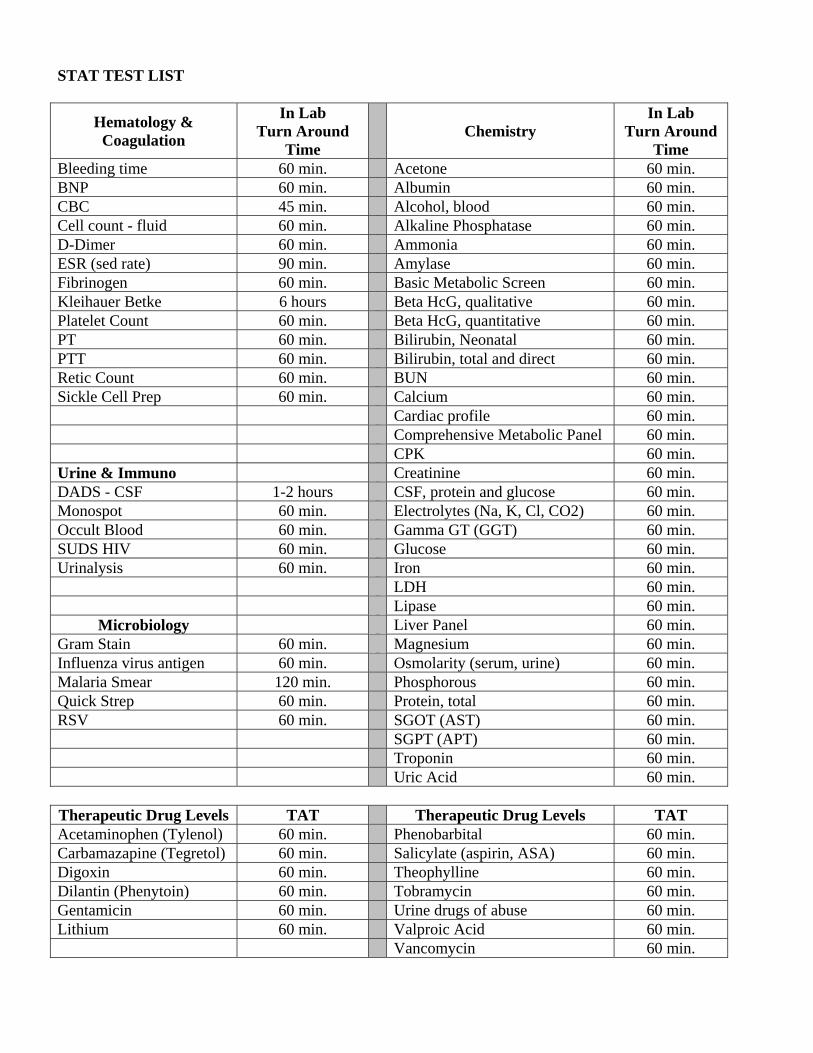
STAT TEST LIST
Hematology & Coagulation
In Lab Turn Around
Time Chemistry
In Lab Turn Around
Time Bleeding time 60 min. Acetone 60 min. BNP 60 min. Albumin 60 min. CBC 45 min. Alcohol, blood 60 min. Cell count - fluid 60 min. Alkaline Phosphatase 60 min. D-Dimer 60 min. Ammonia 60 min. ESR (sed rate) 90 min. Amylase 60 min. Fibrinogen 60 min. Basic Metabolic Screen 60 min. Kleihauer Betke 6 hours Beta HcG, qualitative 60 min. Platelet Count 60 min. Beta HcG, quantitative 60 min. PT 60 min. Bilirubin, Neonatal 60 min. PTT 60 min. Bilirubin, total and direct 60 min. Retic Count 60 min. BUN 60 min. Sickle Cell Prep 60 min. Calcium 60 min. Cardiac profile 60 min.
Comprehensive Metabolic Panel 60 min. CPK 60 min.
Urine & Immuno Creatinine 60 min. DADS - CSF 1-2 hours CSF, protein and glucose 60 min. Monospot 60 min. Electrolytes (Na, K, Cl, CO2) 60 min. Occult Blood 60 min. Gamma GT (GGT) 60 min. SUDS HIV 60 min. Glucose 60 min. Urinalysis 60 min. Iron 60 min.
LDH 60 min. Lipase 60 min.
Microbiology Liver Panel 60 min. Gram Stain 60 min. Magnesium 60 min. Influenza virus antigen 60 min. Osmolarity (serum, urine) 60 min. Malaria Smear 120 min. Phosphorous 60 min. Quick Strep 60 min. Protein, total 60 min. RSV 60 min. SGOT (AST) 60 min.
SGPT (APT) 60 min. Troponin 60 min. Uric Acid 60 min.
Therapeutic Drug Levels TAT Therapeutic Drug Levels TAT Acetaminophen (Tylenol) 60 min. Phenobarbital 60 min. Carbamazapine (Tegretol) 60 min. Salicylate (aspirin, ASA) 60 min. Digoxin 60 min. Theophylline 60 min. Dilantin (Phenytoin) 60 min. Tobramycin 60 min. Gentamicin 60 min. Urine drugs of abuse 60 min. Lithium 60 min. Valproic Acid 60 min.
Vancomycin 60 min.
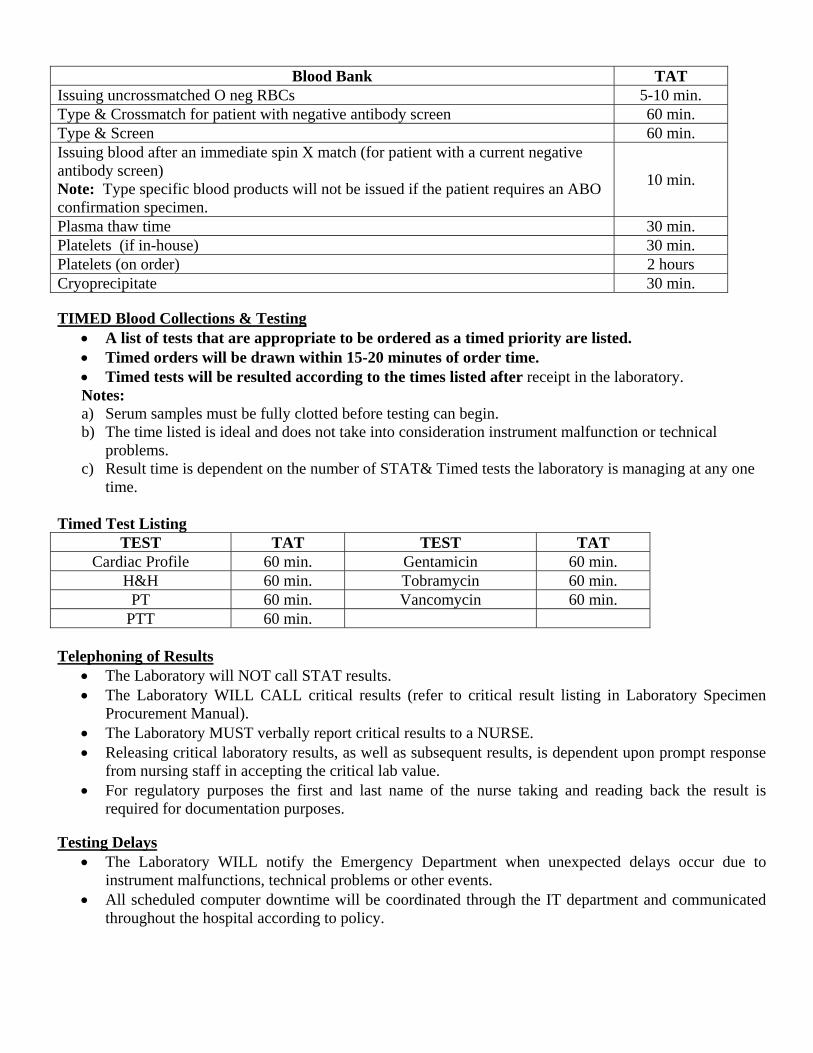
Blood Bank TAT Issuing uncrossmatched O neg RBCs 5-10 min. Type & Crossmatch for patient with negative antibody screen 60 min. Type & Screen 60 min. Issuing blood after an immediate spin X match (for patient with a current negative antibody screen) Note: Type specific blood products will not be issued if the patient requires an ABO confirmation specimen.
10 min.
Plasma thaw time 30 min. Platelets (if in-house) 30 min. Platelets (on order) 2 hours Cryoprecipitate 30 min. TIMED Blood Collections & Testing
A list of tests that are appropriate to be ordered as a timed priority are listed. Timed orders will be drawn within 15-20 minutes of order time. Timed tests will be resulted according to the times listed after receipt in the laboratory. Notes: a) Serum samples must be fully clotted before testing can begin. b) The time listed is ideal and does not take into consideration instrument malfunction or technical
problems. c) Result time is dependent on the number of STAT& Timed tests the laboratory is managing at any one
time. Timed Test Listing
TEST TAT TEST TAT Cardiac Profile 60 min. Gentamicin 60 min.
H&H 60 min. Tobramycin 60 min. PT 60 min. Vancomycin 60 min.
PTT 60 min. Telephoning of Results
The Laboratory will NOT call STAT results. The Laboratory WILL CALL critical results (refer to critical result listing in Laboratory Specimen
Procurement Manual). The Laboratory MUST verbally report critical results to a NURSE. Releasing critical laboratory results, as well as subsequent results, is dependent upon prompt response
from nursing staff in accepting the critical lab value. For regulatory purposes the first and last name of the nurse taking and reading back the result is
required for documentation purposes. Testing Delays
The Laboratory WILL notify the Emergency Department when unexpected delays occur due to instrument malfunctions, technical problems or other events.
All scheduled computer downtime will be coordinated through the IT department and communicated throughout the hospital according to policy.
PATIENT CARE POLICY MANUAL
WASHINGTON ADVENTIST HOSPITAL
REPORTING OF CRITICAL RESULTS OF TESTS AND DIAGNOSTIC PROCEDURES Effective Date: 12/6/93 Policy No. 5204 Cross Referenced: WAH.5911, WAH.5602 Origin: NRSG Reviewed: 5/03, 1/07, 7/10 Authority: SM Revised: 3/98, 10/99, 4/04, 5/06, 1/07, 7/10 Page: 1 of 5
SCOPE: This policy has hospital-wide application. PURPOSE: To provide guidelines for the immediate reporting and documentation of critical results of tests and diagnostic procedures to the responsible Licensed Independent Practitioner (LIP) within the established time frame set forth by the organization. DEFINITIONS: Critical Results of Tests / Diagnostic Procedures: Results, values, or interpretations of tests/diagnostic procedures that have fallen significantly outside the normal range, indicate a life threatening situation, and or any other results that are determined by the laboratorian, radiologist, or any other diagnostician to be critical to the patient’s subsequent treatment decisions. Read-back and confirmation process: The process in which the receiver of the information documents the complete test/diagnostic procedure result in the progress notes in the medical record, reads the test result back, and receives confirmation from the individual who reported the test result. Procedure: Reporting of Critical Results of Tests / Diagnostic Procedures: A call will immediately be initiated to the responsible LIP as soon as a critical result/diagnostic procedure is received. When reporting critical results, the read-back and confirmation process will be used to verify accuracy. The allowable time frame for reporting the critical result of a test and/or diagnostic procedure to the LIP from the time the result is available will not exceed 60 minutes for inpatients and two hours for outpatients. If unable to notify the responsible LIP within 60 minutes, the chain of command for medical management will be followed (Policy WAH.5911 Patient Care Management Issue Resolution). Critical results are not to be left on a recording device or with an answering service or secretary. I. Critical Result Reporting A. Critical Lab Values (including ABG lab)
1. Laboratory personnel will immediately call the result to licensed nursing staff responsible for the patient upon identification of any critical results as defined by the Laboratory portion of the Critical Results Policy (please refer to attachment A.) If the patient’s assigned nurse is unavailable to receive the result, the supervisor (e.g. charge nurse), or another licensed nurse on that patient care unit will receive and document the critical result in accordance with this policy. In some departments (e.g., ABGs in ED and ICUs), the physician responsible for the patient may be notified of the result directly.
2. Results will be documented on the Critical Results Reporting sticker. To document results, place the Critical Results Reporting sticker in the progress notes and enter results into the progress notes on the sticker. Results not received by telephone (e.g., I-Stat results) will also be documented in the progress notes using the Critical Results Reporting sticker, along with any action taken. No need to notify the LIP if protocol/ordered parameters already exist however, it should be documented. [Exception: Results reported directly to the responsible LIP.]
WAH PATIENT CARE POLICY MANUAL
CRITICAL TESTS AND CRITICAL RESULTS REPORTING Policy No: 5204 Page: 2 of 5
3. The read-back and confirmation process will be used to verify accuracy. 4. Upon receipt of the critical result, the nurse will (a) immediately notify the responsible
LIP, or (b) take action based on existing protocols/orders, (e.g. heparin protocol). Communication of the result will include the read-back and confirmation process to verify accuracy. If after 30 minutes, the responsible LIP has failed to return the call, the nurse will place a second call to the physician, and simultaneously call another physician/LIP on the case, if no response from either LIP, initiate chain of command (COC).
5. Discharged Patient Results or Outpatients: Results will be telephoned directly to the physician who ordered the test/physician’s designee, and will include the read-back and confirmation process to verify accuracy.
B. Critical Radiology Results
1. The interpreting physician will immediately notify the responsible LIP of the critical test results as defined in the radiology portion of attachment A.
2. The interpreting physician will also document the critical diagnostic findings, which includes the name of physician who received the results and the date and time of notification in the radiology department critical reports log.
3. The read-back and confirmation process will be used to verify accuracy. 4. Discharged patient results or outpatient results: Results will be called and reported to the
physician in a manner consistent with this policy.
C. Critical Cardio-Diagnostics
1. EKG: Upon completion of any EKG, the technician will provide a copy of the EKG with the preliminary interpretation to the nurse responsible for the patient or the charge nurse. Upon receipt of a critical result (per policy WAH.5602), the nurse will take action based on existing protocols/orders or immediately notify the responsible LIP. If after 30 minutes, the responsible LIP has failed to return the call, the nurse will place a second call to the physician, and simultaneously call another physician/LIP on the case, if no response from either LIP, initiate chain of command (COC).
2. Echocardiogram (ECHO): The interpreting physician will immediately call the critical results as defined by the Cardio-diagnostic portion of this policy (Attachment A) to the responsible LIP.
3. The read-back and confirmation process will be used to verify accuracy. 4. Discharged patient results or outpatients: Results will be called and reported to the
physician in a manner consistent with this policy.
WAH PATIENT CARE POLICY MANUAL
CRITICAL TESTS AND CRITICAL RESULTS REPORTING Policy No: 5204 Page: 3 of 5
Attachment A
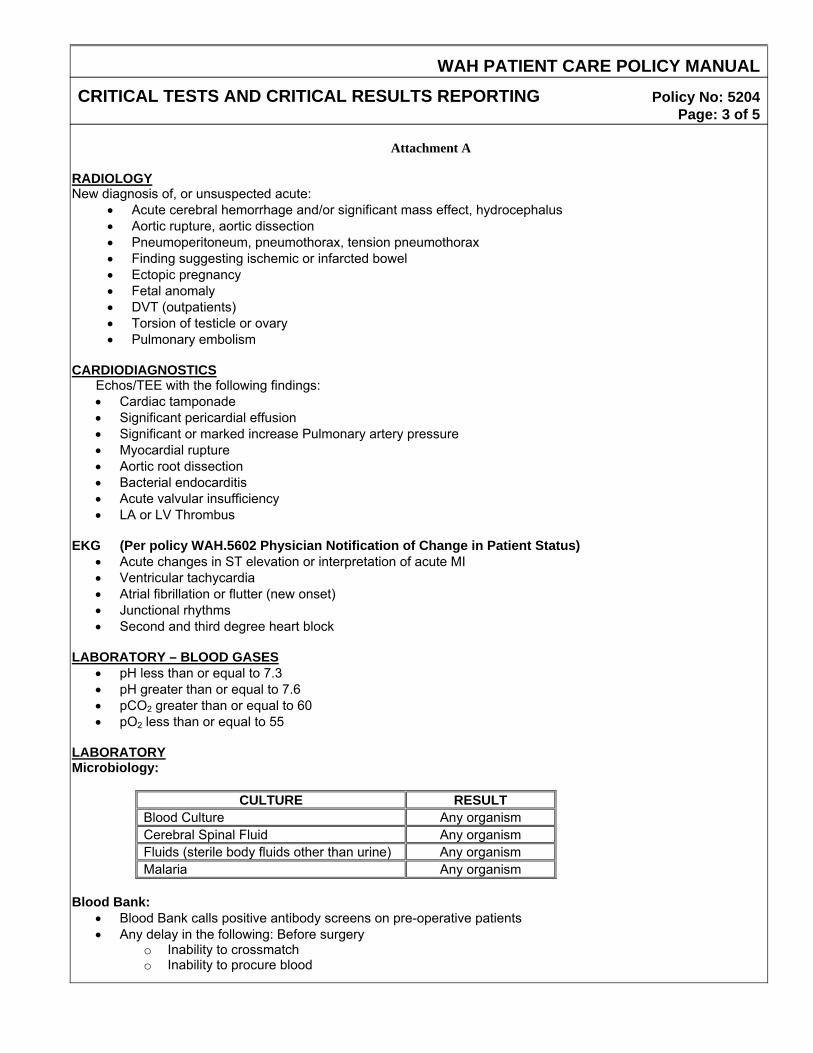
RADIOLOGY New diagnosis of, or unsuspected acute:
• Acute cerebral hemorrhage and/or significant mass effect, hydrocephalus • Aortic rupture, aortic dissection • Pneumoperitoneum, pneumothorax, tension pneumothorax • Finding suggesting ischemic or infarcted bowel • Ectopic pregnancy • Fetal anomaly • DVT (outpatients) • Torsion of testicle or ovary • Pulmonary embolism
CARDIODIAGNOSTICS
Echos/TEE with the following findings: • Cardiac tamponade • Significant pericardial effusion • Significant or marked increase Pulmonary artery pressure • Myocardial rupture • Aortic root dissection • Bacterial endocarditis • Acute valvular insufficiency • LA or LV Thrombus
EKG (Per policy WAH.5602 Physician Notification of Change in Patient Status)
• Acute changes in ST elevation or interpretation of acute MI • Ventricular tachycardia • Atrial fibrillation or flutter (new onset) • Junctional rhythms • Second and third degree heart block
LABORATORY – BLOOD GASES
• pH less than or equal to 7.3 • pH greater than or equal to 7.6 • pCO2 greater than or equal to 60 • pO2 less than or equal to 55
LABORATORY Microbiology:
CULTURE RESULT Blood Culture Any organism Cerebral Spinal Fluid Any organism Fluids (sterile body fluids other than urine) Any organism Malaria Any organism
Blood Bank:
• Blood Bank calls positive antibody screens on pre-operative patients • Any delay in the following: Before surgery
o Inability to crossmatch o Inability to procure blood
WAH PATIENT CARE POLICY MANUAL
CRITICAL TESTS AND CRITICAL RESULTS REPORTING Policy No: 5204 Page: 4 of 5
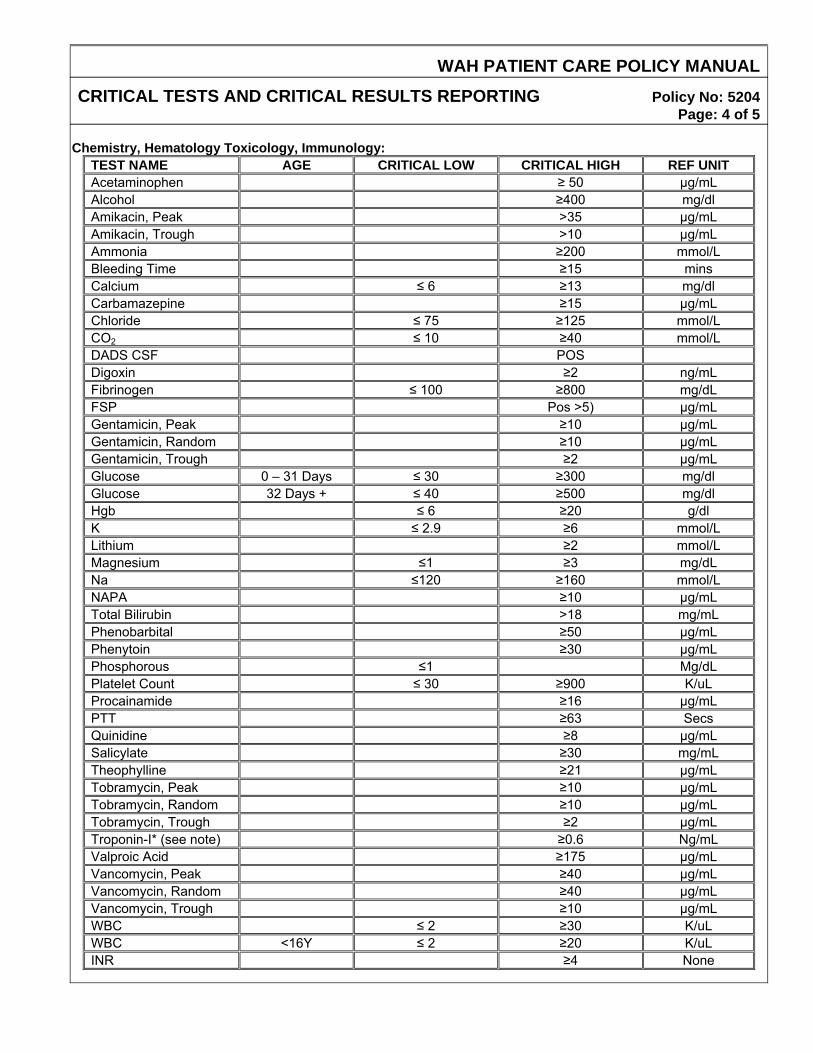
Chemistry, Hematology Toxicology, Immunology:
TEST NAME AGE CRITICAL LOW CRITICAL HIGH REF UNIT Acetaminophen ≥ 50 µg/mL Alcohol ≥400 mg/dl Amikacin, Peak >35 µg/mL Amikacin, Trough >10 µg/mL Ammonia ≥200 mmol/L Bleeding Time ≥15 mins Calcium ≤ 6 ≥13 mg/dl Carbamazepine ≥15 µg/mL Chloride ≤ 75 ≥125 mmol/L CO2 ≤ 10 ≥40 mmol/L DADS CSF POS Digoxin ≥2 ng/mL Fibrinogen ≤ 100 ≥800 mg/dL FSP Pos >5) µg/mL Gentamicin, Peak ≥10 µg/mL Gentamicin, Random ≥10 µg/mL Gentamicin, Trough ≥2 µg/mL Glucose 0 – 31 Days ≤ 30 ≥300 mg/dl Glucose 32 Days + ≤ 40 ≥500 mg/dl Hgb ≤ 6 ≥20 g/dl K ≤ 2.9 ≥6 mmol/L Lithium ≥2 mmol/L Magnesium ≤1 ≥3 mg/dL Na ≤120 ≥160 mmol/L NAPA ≥10 µg/mL Total Bilirubin >18 mg/mL Phenobarbital ≥50 µg/mL Phenytoin ≥30 µg/mL Phosphorous ≤1 Mg/dL Platelet Count ≤ 30 ≥900 K/uL Procainamide ≥16 µg/mL PTT ≥63 Secs Quinidine ≥8 µg/mL Salicylate ≥30 mg/mL Theophylline ≥21 µg/mL Tobramycin, Peak ≥10 µg/mL Tobramycin, Random ≥10 µg/mL Tobramycin, Trough ≥2 µg/mL Troponin-I* (see note) ≥0.6 Ng/mL Valproic Acid ≥175 µg/mL Vancomycin, Peak ≥40 µg/mL Vancomycin, Random ≥40 µg/mL Vancomycin, Trough ≥10 µg/mL WBC ≤ 2 ≥30 K/uL WBC <16Y ≤ 2 ≥20 K/uL INR ≥4 None
WAH PATIENT CARE POLICY MANUAL
CRITICAL TESTS AND CRITICAL RESULTS REPORTING Policy No: 5204 Page: 5 of 5
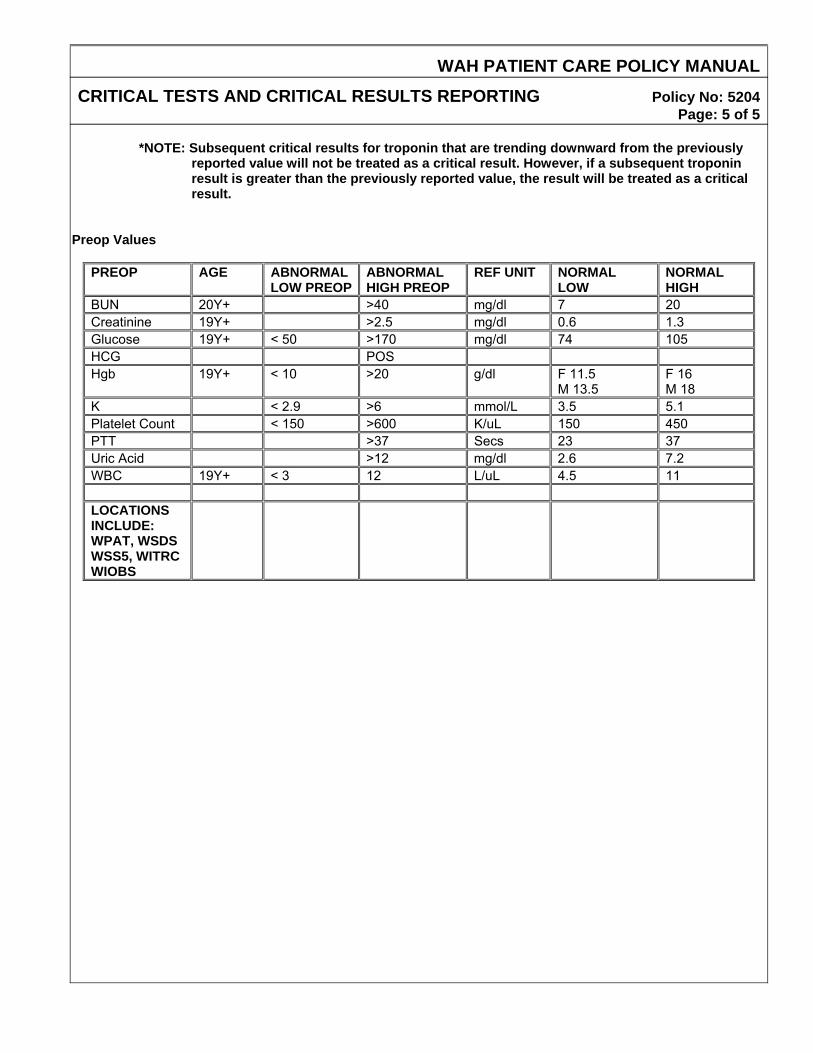
*NOTE: Subsequent critical results for troponin that are trending downward from the previously
reported value will not be treated as a critical result. However, if a subsequent troponin result is greater than the previously reported value, the result will be treated as a critical result.
Preop Values
PREOP AGE ABNORMAL LOW PREOP
ABNORMAL HIGH PREOP
REF UNIT NORMAL LOW
NORMAL HIGH
BUN 20Y+ >40 mg/dl 7 20 Creatinine 19Y+ >2.5 mg/dl 0.6 1.3 Glucose 19Y+ < 50 >170 mg/dl 74 105 HCG POS Hgb 19Y+ < 10 >20 g/dl F 11.5
M 13.5 F 16 M 18
K < 2.9 >6 mmol/L 3.5 5.1 Platelet Count < 150 >600 K/uL 150 450 PTT >37 Secs 23 37 Uric Acid >12 mg/dl 2.6 7.2 WBC 19Y+ < 3 12 L/uL 4.5 11 LOCATIONS INCLUDE: WPAT, WSDS WSS5, WITRC WIOBS
WASHINGTON ADVENTIST HOSPITAL HOSPITAL POLICY MANUAL COMPETENCY ASSESSMENT & DEVELOPMENT Effective Date: 6/95 Policy No: WAH.2184 Cross Referenced: Origin: ADM/PERS Reviewed: BL Authority: LS Revised: 1/98, 7/99, 6/01, 3/02, 8/02, 12/02, 12/31/02, 1/7/03, 6/04, 09/06, 02/09, 6/09, 9/09, 12/09, 1/11, 3/13.
Page: 1 of 6 SCOPE The Competencies portion of this policy applies to all employees, volunteers, contract personnel, students and clinical Instructors working at WAH. The Performance Dialogue Process (PDP) portion of this policy applies only to employees. PURPOSE To define the process and plan for competency assessment and skills development. DEFINITIONS
1. Competency – “Competency is an integration of the knowledge, attitudes, and skills necessary to function in a specific role and work setting.” (From Staff Nurse to Preceptor, 2nd Edition, page 2). Competency also means the ability to perform skills in a safe manner to prevent patient harm, qualifications, and licensure /certification requirements. This includes a self assessment at the time of orientation, and continues post hire.
2. Orientation – Orientation is the means by which new staff is introduced to the philosophy, goals, policies,
procedures, position expectations, physical facilities, and services of a particular work setting.” (From Staff Nurse to Preceptor, 2nd Edition, page 2).
3. Preceptor – A preceptor is an experienced and competent staff who has received formal training to
function in this capacity and who serves as a role model and a resource person to new staff. 4. Preceptee – A Preceptee is a newly hired staff who participates in a preceptorship program for orientation
to an assigned unit
5. Preceptorship – Preceptorship is an organized instructional program in which preceptors facilitate the
integration of newly hired employed nursing staff into their role responsibilities in the work setting.
6. Performance Dialogue - The performance dialogue process provides an opportunity for an ongoing exchange of views between a supervisor and the support staff regarding job results and performance planning. This process is designed to offer communication between supervisors and staff, improve job understanding and performance, and staff development, and provide a basis for salary improvement decisions.
WAH HOSPITAL POLICY MANUAL
COMPETENCY ASSESSMENT Policy No: WAH.2184 Page: 2 of 6 POLICY Competency Assessment at Washington Adventist Hospital will be in accordance with the process and plan delineated in the Adventist Healthcare HR Competency Assessment Policy (#2.25). Additional guidelines, as provided in this policy, address that which is unique to the Hospital. The Corporate policy is to be used in conjunction with the Hospital policy. The Clinical Education Advisory Committee at Washington Adventist Hospital provides oversight to competency activities at the Hospital. Committee members participate in competency development and planning at the corporate level. 1. Calendar Year:
WAH Calendar Year - January 1 through December 31. 2. Age Specific Categories: The hospital has designated criteria for age specific patient population as
identified in the Plan for Delivery of Care. 3. Introductory Period: 90 days following the date of hire for full-time employees, and 120 days for part-time and limited part-time employees. A. Orientation
1. All employees, volunteers, school clinical Instructor, students and contractual personnel are required to complete required orientation. Orientation for all new staff, volunteers, travelers (contractual clinical personnel), non-group students and new school clinical Instructor include General Hospital Orientation or equivalent orientation with documentation. Clinical Instructors are responsible for orientation of their students. Nursing clinical Instructors are required to attend nursing orientation unless they have been an instructor at WAH in the past six months.
2. Any practicum Student completing practicum hours with an assigned and approved preceptor who is an employee of this hospital is required to complete the required hospital orientation unless they have had a clinical rotation at WAH in the past six months.
3. The director/manager is responsible for arranging the provision of unit based competency orientation for
each position. a. Unit based – orientation checklist will be completed by an assigned preceptor. Unit or department
director/manager will review the checklist and file in employee’s file.
4. The director/manager and/or designee determine which competencies require validation of performance and appropriate learning activities in collaboration with clinical specialist for the unit and the Education Department.
5. Orientation includes completion of the Learning Suite Computer-Based Training assigned modules within
the first thirty (30) days of employment, annually, and as needed thereafter.
6. In the event that an employee’s role changes or an employee transfers to a new position, it is required that the employee completes all required orientations and unit based training for the new position as specified. The new director/manager is responsible for arranging the provision of unit based competency orientation for the transferred employee.
WAH HOSPITAL POLICY MANUAL
COMPETENCY ASSESSMENT Policy No: WAH.2184 Page: 3 of 6
7. The Education Department is responsible for providing RN (including interns and nurse-in-training), PCT USC, and Monitor Tech orientations prior to assuming the role on the Nursing unit or in Department. Participants must complete each job specific orientation in its entirety before starting patient care.
8. Care Excellence training is required for clinical areas. Days of training are determined by responsibilities
and clinical area. 9. Learning Suite module assignment is position-specific and determined by the Education Council. 10. Performance is appraised during and/or at completion of the introductory period.
B. Hospital Based In-services and Education
1. Employees are required to attend all mandatory in-services and education for department or unit in meeting the educational requirements for their role. 2. An employee who misses a mandatory inservice or education on the unit or in department will be required to follow up with the departmental director/manager and or designee for completion of the required education.
C. Competency Development
1. Hospital based competencies can be developed at the unit/department level, must be evidence-based and referenced. Competencies will be reviewed by the Clinical Education Advisory Committee (CEAC) in conjunction with the Professional Development Council and or departmental leadership.
2. For Unit based competencies, depending on the type and scope of the competency, development and
approval may occur at the department level or may be broader based with approval from the Professional Development Council.
3. The standard for a particular competency is recognized as residing in the department(s) in which the
activity exists as well as in the Education Department. D. Competency Plans
1. Organizational leadership in conjunction with the Clinical Education Advisory Committee (CEAC), Professional Development Council and the AHC Education Council Team develop the competency plan on an annual basis and maintain it current throughout the year, revising the plan as necessary to reflect organizational, professional, or regulatory changes.
2. The competency plan delineates expected competencies for each position.
E. Ongoing Annual Required Training
1. Learning Suite assigned modules are to be completed no later than the end of the calendar year, or
earlier if specified by organizational leadership in conjunction with the Education Department. Volunteers are not required to complete learning suite assignments.
WAH HOSPITAL POLICY MANUAL
COMPETENCY ASSESSMENT Policy No: WAH.2184 Page: 4 of 6
2. Requirements for BLS/CPR, ACLS, NRP, PALS, PEAT and other life support training requirements are determined by job position. Requirements for BLS/CPR, ACLS, NRP, PALS or other certification must be completed as defined in the job description.
3. There will be no grace period for Life Support certification requirements; employees and contract staff must have a current card at all times. Life Support Certification Card expires at the end of the month that is written on the card. Any employee or contract staff with an expired card will be suspended without pay (cannot use PTO) during this period until a new card has been obtained within 5 days maximum. Human Resources must be notified upon the implementation of suspension status. If non-compliance continues after 5-days of suspension, the employee will be terminated.
4. Life Support Classes are offered through AHC Life Support Training Center and classes are free of
charge to AHC employees per position requirement. If employee fails to cancel an enrolled course within 48 hours or shows up to class late and/or unprepared and sent home, he/she will be required to pay out of pocket for the next course.
5. The requirement for ACLS and other Life Support Training courses will be determined by job position.
Life Support Classes are offered through AHC Life Support Training Center and classes are free of charge to AHC employees per position requirement. If employee fails to cancel an enrolled course within 48 hours or shows up to class late and/or unprepared and sent home, he/she will be required to pay out of pocket for the next course.
All direct patient care and appropriate non-direct patient care staff will be required to complete Skills Day annually on the calendar year. Required skills are identified and approved by the unit manager/director and facilitated with the assistance of the Education Department. Note the following:
a. Newly hired employees will be required to complete Skills Day in the calendar year following their hire year and annually thereafter.
b. Graduate Nurse Interns will be required to complete Skills Day during the calendar year following their internship program and annually thereafter.
F. Competency Records
1. Registration and rosters of attendance will be maintained in Learning Suite and available on the staff’s transcript.
2. Staff may submit documentation of External Educational Activities to the Education Department for
inclusion on their Learning Suite Transcript. G. Performance Dialogue Process
1. Annual Electronic Performance Dialogue Plans (ePDPs) must be completed on an annual basis as
determined by Human Resources Leadership. 2. Introductory ePDPs must be completed by the end of the month in which the employee completes either
the 90 or 120 day introductory period. Where that date falls in the last week of a month, the due date will be extended to the end of the following month.
3. Introductory PDPs will still be required upon transferring to a different job title or when the transfer, with the same job title, represents a significant change in job duties.
WAH HOSPITAL POLICY MANUAL
COMPETENCY ASSESSMENT Policy No: WAH.2184 Page: 5 of 6 H. Failure to Complete Mandatory Organizational Competencies:
1. For Online Learning Suite Modules: failure to complete by the established communicated deadline may result in loss of eligibility for annual merit increase, suspension, and eventually termination.
2. For Assigned Skills Day: failure to complete assigned Skills Day stations in Learning Suite by the last
scheduled Skills Day for the department or hospital wide for that year will result in termination with the exception of pre-approval absence by departmental director or manager.
3. Required Department competencies and mandatory In-services and education: failure to complete by
end of calendar year or date defined by leadership will result in suspension up to 5-days during which time the competency must be satisfied to maintain employment. Human Resources must be notified upon the implementation of suspension status. If non-compliance continues after 5-days of suspension, the employee will be terminated.
I. Contract Personnel
1. All agencies / companies are screened, through an interview process, for their ability to provide personnel that are competent in the role they are expected to fill, and satisfy any regulatory and accreditation requirements.
2. Staff will be required, prior to working, to submit / provide evidence of any required licensure or
certification(s), skills assessment, and competencies specific to the position that have not already been received.
3. The Education Department will work with the contracting department and HR to determine orientation
needs related to job role.
4. Contract personnel will complete Learning Suite modules prior to the start of their assignment.
5. Contract personnel will be provided an orientation appropriate to the position they have been contracted to fill.
6. Orientation may include: Hospital philosophy General safety information Emergency Codes Policies and procedures deemed essential Unit specific information and procedures Confidentiality and Medical Records Rights and Responsibilities of Patients Reporting Patient Abuse Interdisciplinary Patient Care Planning (clinical staff only) Philosophy of Department
7. The contracting department will maintain current any continuing requirements for the personnel contracted.
J. Leadership Competencies
1. Leadership competencies are determined by Senior Management. These may include continuing education activities that are undertaken to meet the performance expectations of the position or to develop a more expansive knowledge or specific expertise.
WAH HOSPITAL POLICY MANUAL
COMPETENCY ASSESSMENT Policy No: WAH.2184 Page: 6 of 6
K. Affiliation School Instructor
1. Affiliating Institution Clinical Instructor will be required to submit / provide evidence of any required licensure or certification(s), skills assessment, and competencies specific to the role to the Education Department prior to supervising students.
2. Nursing Clinical Instructor from the colleges/schools must attend General, Nursing Orientation and Unit
Orientation if they have not had a clinical rotation at WAH within the last six months. Additionally, nursing instructors must attend Care Excellence training to utilize the electronic medical record. Days of training will vary with clinical location. Schools are to contact the Education Department for specific guidelines and orientation materials.
3. Non Nursing Clinical Instructor from the colleges/schools must attend General and Unit Orientation if they
have not had a clinical rotation at WAH within the last six months. Additionally, clinical Instructor must attend Care Excellence training to utilize the electronic medical record. Days of training will vary with clinical location. Schools are to contact the Education Department for specific guidelines and orientation materials.
4. The Education Department will maintain current any continuing requirements for the School
Instructor.
5. The School’s Instructor will be responsible for orienting the students to the assigned unit with each clinical rotation.
6. Students will complete all required role Learning Suite Assignments before clinical rotation.
7. The Students will practice under the supervision of their School Instructor or assigned licensed preceptor.
8. The School Instructor will also be held to the policies and procedures outlined in Contracts and
Affiliations Educational Policy # WAH. 2014 and the Adventist Healthcare Affiliation Agreement.
EVIDENCE BASED LABOR AND DELIVERY PRACTICES
WEDNESDAYFebruary 27, 20136:00 p.m.
Washington Adventist Hospital Continuing Medical Education (CME) Program presents
A Multidisciplinary Approach to
Obstetrical Emergencies
Friday, September 21, 2012 12 Noon – 1:00 p.m.
Conference Rooms A & B, LL2
Pre ne,
senter: Donna M. Neale, MD, The Johns Hopkins University School of MediciDirector of the Center for Maternal and Fetal Medicine and Obstetrics, HCGH
LUNCH WILL BE PROVIDED Washington Adventist Hospital (WAH) is accredited by MedChi, the Maryland State Medical Society to provide continuing medical education for physicians. WAH designates this educational activity for a maximum of 1 AMA PRA ategory 1 Credit (s)™. Physicians should only claim credit commensurate with the extent of their participation in the Cactivity. In accordance with the Accreditation Council for Continuing Medical Education requirements on disclosure, nformation about relationships of presenters with commercial interests and any off‐label product discussions will be ncluded in materials which will be distributed at the time of the conference. ii For more information, please contact: Donna M. Davidson, MPH, CME Program Coordinator, 301‐891‐5384
Educational Objectives
At the e : nd of this session, participants should be able to
1. Recognize the types of obstetrical emergencies.
2. Devise a multidisciplinary team (rapid response) approach for identifying and resolving an obstetric emergency.
3. Explain how to develop, train, and utilize a rapid response team to support obstetric patients in crises.
GRAND ROUNDS