Embed Size (px)
Citation preview

Maternal placental vasculopathy and infection: Twodistinct subgroups among patients with preterm labor andpreterm ruptured membranes
Fernando Arias, MD, PhD: Laritza Rodriquez, MD: Susan C. Rayne, MD,b andFrederick T. Kraus, MDb
St. Louis, Missouri
OBJECTIVE: Our aim was to find out whether patients delivered preterm because of preterm labor orpreterm premature rupture of membranes can be categorized according to clinical characteristics andplacental pathologic findings.STUDY DESIGN: We performed a case-control study of 105 patients who were delivered preterm, 42
because of preterm labor and 63 because of premature rupture of membranes, and 105 patients whowere delivered at term after uncomplicated pregnancies.RESULTS: Maternal placental vascular lesions were present in 14 (34.1%) patients with preterm labor, 19
(35.1%) patients with premature rupture of membranes, and 9 (11.8%) control patients (odds ratios 3.8and 4.0. 95% confidence intervals 1.3 to 11.1 and 1.5 to 10.8, P = 0.0065 and 0.0022, respectively).Infection of the products of conception was found in 16 patients (38%) with preterm labor, 23 patients(36.5%) with premature rupture of membranes, and 19 control patients (18%) (odds ratios 2.7 and 2.6,95% confidence intervals 1.1 to 6.6 and 1.2 to 5.6, P = 0.017 and 0.01, respectively). Patients withmaternal placental vasculopathy had significantly different characteristics compared with those of infectedpatients.CONCLUSIONS: It is possible to identify two subgroups of patients among those who are deliveredpreterm because of preterm labor or premature rupture of membranes, one with infection of the productsof conception and another with maternal placental vasculopathy. (AM J OBSTET GYNECOL 1993;168:585-91.)
Key words: Placenta, disorders; decidual vasculopathy; infection; labor, premature; rupturedmembranes; pregnancy complications; pregnancy outcome
There is a considerable amount of information in theliterature indicating a strong association between infection of the amniotic cavity and preterm labor andpremature rupture of membranes.r" Romero et al. 7
demonstrated that in the setting of preterm labor withintact membranes 22% of the patients who were delivered preterm had positive amniotic fluid cultures, and12.5% of those with positive amniotic cultures hadclinical chorioamnionitis. In the setting of prematurerupture of membranes, 55% of patients have infection."The strength of this association is such that manybelieve that a cause-effect relationship is present.
Not all patients with preterm labor or prematurerupture of membranes have infection; therefore conditions other than infection should have an important
From the Departments of Obstetrics and Gynecology" and Pathology/St. John's Mercy Medical Center.Received for publication May 13, 1992; revised July 27, 1992;accepted August 6, 1992.Reprint requests: Fernando Arias, MD, PhD, Department of Obstetrics and Gynecology, 621 S. New Ballas Road, Suite 2009, St. Louis,MO 63141.Copyright © 1993 Mosby-Year Book, Inc.0002-9378/93 $1.00 + .20 6/1/41661
role in producing these problems. In an effort to findexplanations for the occurrence of preterm labor andpremature rupture of membranes, we studied the clinical characteristics and the placental histologic featuresof women who were delivered preterm because of preterm labor or premature rupture of membranes andcompared these findings with those of women who hadan uncomplicated prenatal course and were deliveredat term.
MethodsPatients. The patient population was composed of
210 patients with singleton pregnancies; 63 were delivered preterm after premature rupture of membranes,42 were delivered preterm after preterm labor, and 105were delivered at term after uncomplicated pregnancies. The 105 patients who were delivered pretermcorrespond to 65.6% of the overall number of patients(n = 160) who were delivered preterm because of premature rupture of membranes or preterm labor at ourinstitution during the time of the study (November1988 to November 1989). The other 55 patients (42with premature rupture of membranes and 13 with
585

586 Arias et al. Februarv 1!)~l:{
Am J O bstet C ynccol
,..,
/
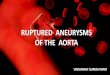
Fig. 1. Severe (grade III ) chorioamnionitis. Polymorphonuclear leukocytes infiltrating amniotic membrane and wholethickness of chorion.
preterm labor) were excluded fro m th e study becauseth e ir placentas were not submitted for pathologic study.Patients in the control group were delivered consecutively during the study period. T he clinical informationwas obta ined by retrospective ch art review and includeddemographic data, gestational age, obstetr ic history,findin gs on admission examination, results of laborato ry exa mina tions, and pregn ancy outcome .
Collection of placentas. Del ivered placentas wereplaced in clean plastic bags, tak en to th e laboratory, andsto red at 0° C until processed for cu ltures and histologicstud ies. T hese stud ies were always performed within 24hours o f delivery .
Histologic examination of placenta. Each placentawas placed on a clean su rface, the membranes werestr ip ped, and a membrane role was made by rolling a 2to 3 ern strip of the chorioam n ion with the site ofrupture in the center. Portion s of th e umbilical cordand tissue blocks of the placenta were di ssected fromthe maternal side; it was always a ttem p ted to include inthese blo cks fragments of decidual tissue attached toth e placental surface to demonstrate spiral arteries .Microscopic sections were made of all these differentparts of the placenta and were reviewed by two of theau thors .
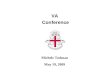
Fig. 2. Decidual vasculopathy. Spiral artery architecture iswell preserved, without adaptive changes, and contains old.partially organized thrombus.
Histologic chorioamnionitis was characte rized by thepresence of polymorphonuclear leukocytes, with orwithout necrosis, in the fet al m embranes and the subcho rionic fibrin plate. The d egree of severity wasgraded independently and subjectively by two of theauthors as slight (grade I), moderate (grate II), orsevere (grade III) on the basis of th e number and extentof infiltrating neutrophils." Fig. I is an example ofsevere histologic chorioamnionitis.
Mat ernal placental vasculopathy was diagnosed whensegments of spiral arteries a ttache d to the maternalsu rface of the placenta fail ed to show the presence ofadap tive changes and remained as small, muscularvessels with well-defined walls, co n tainin g recent or oldorg anized thrombi, mural or oc clusive (Fig. 2). Additional histologic criteria were th e presence of unevenaccelerated maturation of the chorio n ic villi (Fig. 3),large numbers of multinucleated syncy tial knots, andmultiple placental infarcts.
A mix ed lesion was diagnoscd wh en features of infection and maternal placental vascu lopa thy were presentin th c same specimen.
Ch ro nic villitis was di agnosed when areas of chronicinfl ammation with mononuclear cell infiltrates and area s of fibrinoid necrosis affect ed clusters of villi.

Vnlume 16H. Number ~
Am J Obstct (;""t'<'01
Abruptio placentae was diagnosed when a retroplacental clot leaving a definite impression on the maternal surface of the placenta was found in the histologicexamination of the placenta.
Microbiologic study of placenta. Subchorionic cultures of the placenta were obtained by scaring theamniotic surface, incising through this area with asterile scalpel blade, and inserting a swab through theopening to sample the subchorionic layers. III Culturalmethods involved aerobic and anaerobic techniques inall cases.
Definitions. Patients were considered to have infection if one or more of the following could bedemonstrated: (I) positive amniotic fluid Gram stain orcultures; (2) positive subchorionic placental cultures; (3)positive central cultures (blood, spinal fluid, trachealaspirate) of the neonate, obtained shortly after birth; (4)severe (grade HI) histologic chorioamnionitis.
Patients were considered to have maternal placentalvasculopathy if they had characteristic vascular lesionsin the decidual spiral arteries and uneven acceleratedvilli maturation, multiple syncytial knots, and placentalinfarcts or the placental weight was < 10th percentilefor gestational age. II A newborn was classified as growthretarded if the birth weight was < 10th percentile forgestational agel" and the nursery stay was consistentwith the clinical impression of intrauterine malnutrition.
A patient was considered to have chronic villitis if theplacenta exhibited the characteristic histologic findingswith mononuclear cell infiltration and there was noclinical, histologic or laboratory evidence of acute infection.
Patients were considered to have negative findingswhen a complete evaluation including amniotic fluidcultures, placental cultures, placental histologic results,and neonatal evaluation failed to reveal findings associated with preterm labor or premature rupture ofmembranes.
Statistical analysis. The significance of the differences observed between the control group and thepremature rupture of membranes and preterm laborgroups were determined with the Student t, Fisher'sexact probability, and the X" tests, calculated by meansof the True Epistat program from Epistat Services,Richardson, Texas. A two-tailed jJ value of ~ 0.05 wasconsidered to indicate a significant difference.
Results
The descriptive variables for patients \11 the threegroups (preterm labor, premature rupture of membranes, control) are shown in Table I. As expected,there were significant differences between the controland study groups (preterm labor and premature rupture of membranes) with respect to gestational age atthe time of delivery and birth weight. The difference in
Arias et al. 587
Fig. 3. Acceleruted maturation of chorionic villi. Abnormallysmall, fibrotic villi with abnormally thin syncytiotrophoblast.
the incidence of primigravid patients \11 the threegroups (34 in the control group, 20 in the preteI'mlabor group, and 21 in the premature rupture of membranes group) was not statistically significant.
Table II shows the classification of patients intodifferent groups: intortion, maternal placental vasculopathy, mixed lesions, chronic villi tis, abruptio placentae, and normal findings, according to the definitionsdescribed. The prevalence of infection and maternalplacental vasculopathy was significantly higher in patients with preterm labor (odds ratio 2.7 and 3.8, 95%confidence intervals 1.1 to 6.6 and 1.3 to 11.1, P = 0.0 Iand 0.0065, respectively) and premature rupture ofmembranes (odds ratio 2.6 and 4.0, 95% confidenceinterval 1.2 to 5.6 and 1.5 to 10.8, jJ = 0.0 I and 0.0022,respectively) than in control women who were deliveredat term. Abruptio placentae occurred significantly morefrequently (p = 0.006) in patients with preteI'm laborthan in controls. The number of patients with normalfindings was significantly larger in the control groupthan in the prcterm labor group (odds ratio 0.06, 957cconfidence interval 0.0 I to 0.20, jJ < 0.00000 I) or thepremature rupture of membranes group (odds ratio0.07, 95% confidence interval 0.02 to 0.18, jJ <0.(00001).
All patients with preteI'm labor classified as having

588 Arias at al.
Table I. Characteristics of patients
February 1993Am J Obstet Gynecol
Premature rupturePreterm labor Control of membranes
(n = 42) (n = 105) (n = 63)Characteristic (mean ± SE) Significance (mean ± SE) Significance (mean ± SE)
Age (yr)GravidityParityGestational age (wk)Cesarean deliveries (No.)Birth weight (gm)
NS, Not significant.
25.6 ± 6.02.0 ± 1.20.6 ± 0.9
3\.4 ± 3.316 (32.6%)
1759 ± 510
NSNSNS
P= 0.001NS
P= 0.001
26.0 ± 5.32.3 ± 1.50.9 ± 1.1
39.0 ± 1.224 (30.0%)
3362 ± 476
NSNSNS
P = 0.001NS
P = 0.001
27.9 ± 4.92.3 ± 1.30.9 ± 1.0
31.8 ± 3.031 (44%)
1829 ± 494
Table II. Classification of patients according to clinical and laboratory findings
Premature rupturePreterm labor Control of membranes
Finding (n = 42) Significance (n = 105) Significance (n = 63)
Infection 16 (38.0%) P = 0.01 19 (18.0%) P = 0.01Maternal placental vascu- 14 (34.1%) P = 0.001 9 (11.8%) P = 0.001
lar lesionsMixed infection and vas- 3 (7.1%) NS 3 (2.8%) NS
cular lesionsChronic villitis 1 (2.3%) NS 7 (6.6%) NSAbruptio placentae 4 (9.5%) P = 0.001 0(0%) NSNegative findings 4(9.5%) p = 0.001 66 (63.8%) P = 0.001
NS, Not significant.
Table III. Severity of histologic amnionitis
23 (36.5%)19 (35.1%)
5 (7.9%)
7(11.1%)2 (3.1%)7 (11.1%)
Premature rupturePreterm labor Control of membranes
Grade (n = 16) Significance (n = 19) Significance (n = 23)
IIIIII
NS, Not significant.
2 (12.5%)3 (18.7%)
11 (68.7%)
p = 0.004NS
P < 0.0001
12 (63.1%)7 (36.8%)0(0%)
p < '0.0001NS
P < 0.0001
1 (4.4%)6 (26.0%)
16 (69.5%)
infection had positive histologic findings in the placentaand positive amniotic fluid, placental, or neonatal cultures. Of the 23 patients with premature rupture ofmembranes classified as having infection 7 had gradeIII chorioamnionitis, 9 had grade III chorioamnionitisand positive amniotic fluid, placental, or neonatal cultures, and 7 had focal acute chorioamnionitis andpositive amniotic fluid, placental, or neonatal cultures.Severe histologic amnionitis (grade III) was significantlymore frequent in patients with premature rupture ofmembranes (two-tailed p = 0.000002, odds ratio notcalculable) and preterm labor (two-tailed p = 0.00001,odds ratio not calculable) than in patients in the controlgroup (Table III). The bacteria isolated by subchorionicplacental cultures and their association with the presence of clinical amnionitis, the severity of histologicamnionitis, and the results of amniotic fluid Gram stainare shown in Table IV.
The criteria used to classify patients with pretermlabor into the maternal placental vasculopathy groupwere placental histologic findings plus newborn andplacental weights < 10th percentile (8 patients), placental histologic findings plus fetal growth retardation (2patients), and placental histologic findings only (4 patients). The criteria used to classify patients with premature rupture of membranes in the maternal placental vasculopathy group were placental histologic findings and placental weight < l Oth percentile (14patients), placental histologic findings and fetal growthretardation (2 patients), and placental histologic findings only (3 patients). Decidual spiral arteries wereidentified in 93 (88.5%) of the patients who were delivered preterm and in 76 (73.3%) of the control patientswho were delivered at term. The incidence of decidualvasculopathy in patients with preterm labor or premature rupture of membranes and control patients (Table

Volume 168, Number 2Am J Obstet Gynecol
Arias et al. 589
Table IV. Microbiologic characteristics of placental cultures and their relation to amniotic fluid Gram stain,severity of histologic amnionitis, and presence of clinical chorioamnionitis
Severity of AmnioticCase Clinical histologic amnionitis fluidNo. Organism amnionitis (grade) Gram stain
Patients with preterm labor1 Fusobacterium nucleatum2 Neisseria sicca3 Propionibacterium sp.4 Escherichia coli
Anaerobic gram-negative rods5 Fusobacterium nucleatum6 Gardnerella vaginalis
Anaerobic gram-positive cocciAnaerobic gram-negative rods
7 Fusobacterium nucleatum8 Listeria monocytogenes9 Gardnerella vaginalis
Patients with premature rupture of membranes1 Bacteroides vulgatum2 Staphylococcus aureus3 a-Hemolytic streptococci4 Bacteroides distasonis5 Haemophilus influenzae6 Staphylococcus aureus7 Streptococci group B8 Anaerobic gram-negative rods
Anaerobic gram-positive rods9 Streptococci group D (not en-
terococci)10 Streptococci group D (not en-
terococci)
ND, Not done.*Focal necrotic deciduitis.
+ 1Il+ 1Il+ 1Il
1Il
+ 1Il+ 1Il
1Il+ 1Il
1Il
+ 1Il+ 1Il+ 1Il+ 1Il+ 1Il+ 1Il+ 1Il
1*
1Il
1Il
++
ND
+
++
ND
NDND+
ND+
NDND
+
ND
Table V. Comparison between patients with preterm labor and those with premature rupture ofmembranes who had infection or placental vascular lesions
Birth weight (gm)Gestational age (wk)Stay in neonatal intensive care
unit (days)Deaths (No.)
NS, Not significant.
Infection(n = 39)
1566 ± 51730.1 ± 3.239.7 ± 35.7
4
Significance
p = 0.01P = 0.005P = 0.03
NS
Maternal placentalvascular lesions
(n = 33)
1859 ± 39732.3 ± 2.623.8 ± 21.9
o
II) was calculated with only those cases in which decidual vessels were seen on histologic examination used asdenominator.
Table V compares several clinical features of patientswith preterm labor and premature rupture of membranes who were considered to have infection and whohad placental vascular lesions. It is apparent that patients with placental vascular lesions had better perinatal outcomes, including delivery at more advancedgestational ages (p = 0.005), greater birth weights(p = 0.0 I), and less time in the neonatal intensive careunit (p = 0.03) than infected patients.
There were four neonatal deaths, all of them in
patients with infection. The first occurred in the infantof a 32-year-old, white woman, gravida 2, para I, with ahistory of neonatal death caused by Enterobacter meningitis after premature rupture of membranes. She hadrecurrent premature rupture of membranes at 29 weeksand was admitted with clinical chorioamnionitis. Birthweight was 1753 gm. The baby died of sepsis. Bacteroides fragilis grew in placental and neonatal blood cultures. The second death occurred in the infant of a26-year-old, white woman, gravida 3, para 2, admittedwith premature rupture of membranes and clinicalchorioamnionitis at 28 weeks. The baby died in septicshock caused by disseminated herpes simplex virus type

590 Arias at al.
II infection. All maternal cultures, except the cervicalculture, were negative. The third death occurred in theinfant of a 25-year-old, white woman, gravida I, para 0,admitted at 28 weeks with preterm labor, 3 days aftergenetic amniocentesis for evaluation of a fetal omphalocele. Amniocentesis revealed multiple gram-positivecocci, and amniotic fluid and placental cultures grewNeisseria sicca. The baby weighed 1000 gm and died inseptic shock. The fourth death occurred in the infant ofa 25-year-old, white woman, gravida I, para 0, admittedwith premature rupture of membranes at 23 weeks.Two days later clinical chorioamnionitis developed. Shewas delivered of a 541 gm fetus who died shortly afterbirth. Placental culture grew group D Streptococcus (notenterococci).
Comment
Our data suggest the presence of two well-definedsubgroups among patients with preterm labor andpremature rupture of membranes. One of them ischaracterized by the presence of bacterial infection ofthe products of conception and the other by the presence of placental vascular abnormalities consisting oflack of adaptive changes in the decidual portion of thespiral arterioles and presence of uneven acceleratedmaturation of villi, multiple syncytial knots, and placental infarcts.
The finding of an association between chorioamnioticinfection and preterm labor and premature rupture ofmembranes is not surprising and has been clearly substantiated by other investigators. 2, 8 This association isfound so frequently that the possibility of a cause-effectrelationship between infection and preterm labor andpremature rupture of membranes is widely acceptedamong experts in this field. I, 3, 5
Less popular, in spite of its intrinsic teleologic appeal,is the idea of an association between maternal placentalvasculopathy and preterm labor and premature ruptureof membranes. The changes in the maternal vascularcompartment of the placenta in patients with pretermlabor and premature rupture of membranes are similarto those found in patients with preeclampsia, 13, 14 inthose with fetal growth retardation, 15, 16 and in some
patients with repetitive second-trimester fetal death. I7
Naeye'" originally described the association betweenthese placental changes and spontaneous preterm delivery in patients without hypertension during pregnancy. Westgren et al.;'" Weiner et al.," Gianopoulosand Defierto," and Tamura et al. 2 2 have reported thatfetal growth retardation is a common finding in patients who are delivered preterm. Other investigators'?25 have found alterations in maternal and fetal arteryflow velocity waveforms in patients in preterm labor,and there is evidence'"?" indicating that those changesreflect vascular alterations of the placenta. Also, recent
February 1993Am J Obstet Gynecol
work by Salafia et al. 29 looking exclusively at placentalhistologic findings demonstrated that decidual vasculopathy occurs more frequently than chorioamnionitisin patients delivered preterm in all gestational agegroups.
All the evidence accumulated in the literature pointsto the possibility that a deficiency in the ability of thetrophoblastic cells to produce adaptive changes in thespiral arterioles leads to inadequate and unevenuteroplacental blood flow with production of accelerated maturation, increased syncytial knots, thinning ofthe syncytiotrophoblast, fibrotic villi, and infarcts inthose areas of the placenta affected by low flow. What isunknown at the present time is the nature of the linkbetween the failure to establish adequate hemochorialplacentation and its clinical expression. This enigma isof singular importance because it may explain whypreeclampsia develops in some of these patients andsome others have fetal growth retardation without hypertension, preterm labor, or preterm rupture of membranes. Another possibility, unsupported by evidence, isthat the changes observed in the placenta are unrelatedto the clinical picture shown in these patients.
In addition to the obvious differences in laboratoryfindings patients with chorioamniotic infection and patients with maternal placental vasculopathy and eitherpreterm labor or premature rupture of membranesseem to have a different clinical course and a differentprognosis. We found that patients with preterm labor orpremature rupture of membranes who have infectionare delivered earlier, have smaller babies, have moresevere morbidity, and have greater mortality than patients with preterm labor or premature rupture ofmembranes who do not have infection and have maternal placental vascular abnormalities.
Our results should be interpreted with caution. As
shown in Table IV, in the setting of infection thecorrelation between placental histologic type, placentalcultures, amniotic fluid Gram stain, amniotic fluid cultures, and clinical findings is not perfect. A similarimperfect correlation exists between decidual vasculopathy and clinical findings. However, it is tempting tospeculate that in 60% to 70% of patients preterm laborand premature rupture of membranes are the result ofinfection and maternal placentalvasculopathy. If this istrue, strenuous efforts to inhibit preterm uterine activityand prolong pregnancy may be inappropriate, not onlybecause of their lack of effectiveness'" but also becauseprolongation of pregnancy will keep the fetus in ahostile environment and potentially may cause moreharm than good.
REFERENCES1. Romero R, Mazor M. Infection and preterm labor. Clin
Obstet Gynecol 1988;31 :553-84.

Volume 168, Number 2Am J Obstet Gynecol
2. Hillier SL, Martius], Krohn M, et al. A case-control studyof chorioamniotic infection and histologic chorioamnionitis in prematurity. N Engl] Med 1988;319:972-8.
3. Gravett MG, Hummel D, Eschenbach DA, et al. Pretermlabor associated with subclinical amniotic fluid infectionand with bacterial vaginosis. Obstet Gynecol 1986;67:22937.
4. Hameed C, Tejani N, Verma UL, Archbald F. Silentchorioamnionitis as a cause of preterm labor refractory totocolytic therapy. AM] OBSTET GVNECOL 1984;149:726-30.
5. Minkoff H. Prematurity: infection as an etiologic factor.Obstet Gynecol 1983;62: 137-44.
6. Guzick OS, Winn K. The association of chorioamnionitiswith preterm delivery. Obstet Gynecol 1985;65: 11-6.
7. Romero R, Sirtori M, Oyarzun E, et al. Infection and labor.V. Prevalence, microbiology, and clinical significance ofintraamniotic infection in women with preterm labor andintact membranes. AM] OBSTET GVNECOL 1989; 161 :817-24.
8. Romero R, Quintero R, Oyarzun E, et al. Intraamnioticinfection and the onset of labor in preterm prematurerupture of the membranes. AM ] OBSTET GVNECOL 1988;159:661-6.
9. Zhang], Kraus FT, Aquino Tl. Chorioamnionitis: a comparative histologic, bacteriologic, and clinical study. Int JGynecol Pathol 1985;4: 1-10.
10. Aquino TI, Zhang], Kraus F'F, et al. Improved techniquefor bacteriologic study of the placenta. Am J Clin Pathol1984;81 :482-6.
II. Naeye RL. Disorders of the placenta and decidua. In:Naeye RL, ed. Disorders of the placenta, fetus, and neonate. Diagnosis and clinical significance. St. Louis: MosbyYear Book, 1992:125.
12. Brenner WE, Edelman DA, Hendricks CH. A standard offetal growth for the United States of America. AM] OBSTETGVi'iECOL 1976; 126:555-64.
13. Brosens I, Robertson WB, Dixon HG. The role of thespiral arteries in the pathogenesis of preeclampsia. In:Wynn RM, ed. Obstetrics and gynecology annual. NewYork: Appleton-Century-Crofts, 1972: 177.
14. Robertson WB, Brosens I, Dixon HG. The pathologicalresponse of the vessels of the placental bed to hypertensive pregnancy.] Pathol Bacteriol 1967;93:581-92.
15. Van del' Veen F, Fox H. The human placenta in idiopathicintrauterine growth retardation: a light and electron microscopy study. Placenta 1983;4:65-77.
16. Sheppard BL, Bonnar ]. An ultrastructural study ofuteroplacental spiral arteries in hypertensive and normotensive pregnancy and fetal growth retardation. Br JObstet Gynaecol 1981 ;88:695-705.
17. Khong TY, Liddell HS, Robertson WB. Defective hemo-
Arias at al. 591
chorial placentation as a cause of miscarriage: a preliminary study. Br.J Obstet Gynaecol 1987;94:649-55.
18. Naeye RL. Pregnancy hypertension, placental evidences oflow uteroplacental blood flow, and spontaneous pretermdelivery. Hum Pathol 1989;20:441-4.
19. Westgren MD, Beall M, Divon M, et al. Fetal femurlength/abdominal circumference ratio in preterrn laborpatients with and without successful tocolytic therapy.J Ultrasound Med 1986;5:243-5.
20. Weiner CP, Sabbagha RE, Vasirub N, et al. A hypotheticalmodel suggesting suboptimal intrauterine growth in infants delivered preterrn. Obstet Gynecol 1985;65:323-6.
21. Gianopoulos JG, DeSerto T. Premature labor: its association with asymmetrical intrauterine growth [Abstract 387].In: Proceedings of the ninth annual meeting of the Societyof Perinatal Obstetricians, New Orleans, Louisiana, February 2-4, 1989. New Orleans: Society of Perinatal Obstetricians, 1989.
22. Tamura RK, Sabbagha RE, Depp R, et al. Diminishedgrowth in fetuses born pretcrm after spontaneous labor orrupture of membranes. AM J OBSTF:I GVNECOL 1984; 148:1I05-10.
23. Brar HS, Medearis AL, DeVore GR, et al. Maternal andfetal blood velocity waveforms in patients with pretermlabor: prediction of successful tocolysis. AM] OBSTf.T GvNECOL 1988; 159:947-50.
24. Brar HS, Medearis AL, DeVore GR, et al. Maternal andfetal blood flow velocity waveforms in patients with preterm labor: relationship to outcome. AM J OBSIEI GVNECOL1989; 161 :1519-22.
25. Trudinger B], Giles WB. Clinical and pathologic correlations of umbilical and uterine artery waveforms. ClinObstet Gynecol 1989;32:669-78.
26. Giles WB, Trudinger BJ, Baird P. Fetal umbilical arteryflow velocity waveforms and placental resistance: pathological correlation. Br J Obstet Gynaecol 1985;92:31-8.
27. McCowan LM, Mullen BM, Ritchie K. Umbilical arteryflow velocity waveforms and the placental vascular bed. AMJ OBSTET GVNECOL 1987;157:900-2.
28. Fok RY, Pavlova Z, Benirschke K, et al. The correlation ofarterial lesions with umbilical artery Doppler velocimetryin the placentas of small-for-dates pregnancies. ObstetGynecol 1990;75:578-83.
29. Salafia CM, Vogel CA, Vinzileos AM, et al. Placentalpathologic findings in preteI'm birth. AM J OBSTET GVNECOI.1991;165:934-8.
30. Leveno K], Little BB, Cunningham FG. The nationalimpact of ritodrine hydrochloride for inhibition of preterm labor. Obstet Gynecol 1990;76: 12-5.




















![Diabetes is a vasculopathy [autosaved]](https://img.pdfslide.us/doc/110x75/58ed40fc1a28ab99298b45f1/diabetes-is-a-vasculopathy-autosaved.jpg)