Embed Size (px)
Citation preview

MATERNAL PHENYLKETONURIA-CHRONOLOGY OF THE DETRIMENTAL EFFECTS ON EMBRYOGENESIS AND FETAL DEVELOPMENT: Pathological Report, Survey, Clinical Application
Robert 0. Fisch, MD, Barbara Burke, MD, John Bass, MD, T. Bruce Ferrara, MD, and Angeline Mastri, MD 0 Departments of Pediatrics, Laboratory Medicint. and Pathology, and Pediatric Neurology, University of Minnesota Medical School. Minneapolis, Minnesota 55455
11 Maternal phenylki~tonuria (I'KlJ} is likely t o hurw detrimental e f frcts on embryogenesis and fcjtal d(~vc1oprnent. Manifestations in the offspring include spontaneous abortion, various congenital malformations, intrautrrinc growth re tardation, and micrucc~phaly. The t ime at which the metabolic abnormalities induccl pathologic cmbryogenc~sis can be documented by knowing the t ime o f the devclopmr~nt of specifically damaged organ systems. This review reveals that, while thc most recognized congenital malformations occur in the heart, the most c o m m o n abnormality is growth inhibition occurring throughout pregnancy. The organ systrm most commorily aff(,cted by this growth inhibition is the brain, rcsulting in a high incidencc of micrcjncephaly. I t appears that maternal phenyl- kiptonuria interfrrc .~ with appropriate fe tal growth and that this cffcct occurs during the cntirr course of pregnancy and has no tissue specificity. This information can bc bo th informativr t o pathologists and uscJful to clinicians.
K E Y WORDS: maternal phrnylk~tonun'a, datrimrntal i.mhryugrnrsir.
INTRODUCTION
Mothers with phenylkctonuria (PKU), rcgardless of their intclligencc, have previously been observed t o have a high incidence of abnormalities in their offspring. Thcsc previously rcported abnormalities include mental retardation' intrautcrinc and extrauterinc growth retardation with micro- ccphaly,* congenital heart d i s c a ~ c , ~ spon taneous abortion^,^ various addi- tional malformations: and a higher incidence o f PKC' than cxpected.' The incidencc of these aberrrations in maternal PKU progeny appears to be correlated with the maternal concentration o f serum ph~ny la l an ine .~
A recent example o f a malformed infant born to a mother with PKU at the University of Minnesota Hospitals initiated an analysis of prcviously
449
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

450 R . 0. FISCH ET AL.
tlocirmentetl abnormalities in the offspring of PKU mothers. This report cmphdsiles the rrlationship between the effect o f phenylketonuria on different organ s)'stcms during embryogenesis and the development of nidformations.
CASE REPORT
.4 39-\vcek-Kestatioii female infant was admitted to th r Selvborn Intcnsive Care Unit at the University o f Minnesota IIospitals because of c.!.anosis. ' Ihe mothci- \vas ;I 22-year-old primigravatia who was diagnosed ;IS having PKU (serum phenylalanine 22.2 mg/dl) at 6 months o f age, tollo\ving i i n onset o f petit ma1 seizures. The mother was on dietary therap). until 9 years o f age. IIer I Q was 67, and she was graduated from high school with special tutoring. One maternal sibling with PKU was cspilcpric and severely rcstarded. Two additional siblinss bvithout PKU had 1 cii rn ing disc )rde 1-5.
PI-cgnanc), was uncomplicated. 'The mother bvas sccn for routine prcnatal visits, received no dietary restrictions, and gained 20 pounds (lilt-ing pregnant).. Labor and delivery were uncomplicated. Apgar scorcs uerc 5 at both 1 and 5 min. The baby's weight was 2600 2 (25th pcrccntilc), length was 48 cm (25th percentile), and occipital-frontal head ciI-ccimfercncc was 30 cm (more than 2 standard dcviations below the mean). Significant tindings on physical examination included marked c-).anosis and decreased peripheral pulses. An initial arterial blood gas ~-cvc;ilcd 'I Pa02 o f 18 torr. An echocardiogram demonstrated aortic \.al\.cilar atrcsia with a hypoplastic left ventricle. The infant deteriorated d c y i t c medical support , and i t was felt that an at tempt a t surgical palliation o f her Icsion \ \odd be unsuccessful. She siibscquently expired, d t 2 days o f age. Laboratory data obtained prior t o her death included a serum phenylalanine 01' 1 . 1 ing/dl and a serum tyrosinc o f 1.1 mg/dl.
AUTOPSY FINDINGS
I'crtinent findings a t autopsy included the presence of both growth I ctai-dation and microcephaly as noted clinically. The brain wcighcd 195.4 s pi-ior t o fixation (expected weight =349 ? 36 g). Organ weights other than that o f the brain were within normal limits for the body sizc. I)ccI-c.;ised numbers o f renal lobules were present, b u t thc numbers were n o t in the hypoplastic: range.
'The infant had a hypoplastic left heart syndrome with levocardia, tiorma1 atrial and visceral situs, normal atrial-ventricular and ventricular-atrial 1-clationships, and an intact ventricular septum. Aortic valvular atresia and
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

MATERNAL PHENYLKETONURIA 451
a d1,splastic stenotic mitral valve representing in essence an atretic mitral valve were found together with an intact atrial septum (so-called premature closure o f the foramen ovale6). ‘The left atrium thus ended blindly, having received all of the pulmonary veins as usual. Its lining MW noted t o be pittcd with what was thought t o be the dilated openings of Thcbesian veins representing avenues of egress o f blood from the left a t r i ~ m . ~ ~ ~ A search f o r an o in a1 c) us p u 1 monar y vc n ( )u s connect i o ns , a 1 ev oa t r i oc a r ti i 11 a1 vein, a venous communication between pulmonary and systemic veins, anti coronary s inusdeft atrial window revealed n ~ n e . ~ - ’ ~ A pcrsistent left superior vena cava entered the coronary sinus but had no communication with the pulmonary veins or left atrium. The coronal-). sinus cntcrcd thc right atrium, which was dilated. As anticipated, because o f the pulmonar), venous obstruction, thee were both pulmonary venous and arterial hyper- sensitive changes present in the lung, the latter being manifest by major medial hypertrophy o f pulmonary muscular arteries and b!. premature muscle development in acinar pulmonary arteries. Pulmonary lymphatic channels were niodcrately dilated. The pulmonary trunk was \vide, and a widely patent ductus arteriosus supplied the entire vascular tree. l h e ascending aorta was hypoplastic. There was no endocardia1 fibroclastosis o f the hypoplastic left ventricle.*
The brain shoived no gross abnormalities. On microscopic. cxamination, the cerebral cortex was well developed and normal in architecture and ccll density in both lobes. IIistologic evaluation o f the basal ganglia, thalamus, cerebellum, and brainstem also revealed normal ccll density with no unusual findings. E:xamination o f the spinal cord revealed no gross o r histologic defects. Myelination in all areas o f thc cerebrum, cerebellum, brainstem, and spinal cord corresponded t o published standards for full-term infants.*’
METHODS AND RESULTS
All reports o f fetal congenital malformation related t o maternal PKU, regardless of diet o r phenylalanine concentration during pregnancy, prior t o April 1984 were reviewed. A summary of each rcportcd malformed organ systcm was catalogued along with the time of embryologic develop- ment of each respective system. These data are presented in ‘Table l.22-27
Evaluation o f the data reveals that cardiovascular anomalies are quantitatively more prevalent than others. However, all organ systems show evidence o f some developmental defect. A s cxpected, most o f the
*Jesse E. Edwards, MD, linited-Children’s Hospital, St. Paul, Minnesota, examined thc cardiovascular specimen from this casc in consultation, and he concurs with thc gross and microscopic findings.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

P
VI
N
Aff
ecte
d or
gali
s <
Ihy
s 31
-45
Day
s 46
-56
I)a\
s
9 ~
-10
W
eeks
2-
3 S
lont
hs
4-6
Mon
ths
7 -8
Mon
ths
Unk
nokv
n
Car
diov
ascu
lar
Sit
us in
vcr-
Si
nqle
atr
ium
3 V
entr
icul
ar sc
ptal
.4
nom
aluu
s pu
I-
Pate
nt d
uct
us
(18
40
days
su
s4
aid
pat
cnt
duct
us
mon
ary
vcno
us
vuln
erab
le
Dcx
tro-
Si
ngle
vrn
tri-
ar
tcri
osus
26*2
’ re
turn
4 pe
riod
for
611
card
ia4’
” c:
ulus
’6
Atr
ial
sept
a1
1nc:
ompl
ctc
Tra
nspo
siti
on
of a
rrat
dr
teri
c,sZ
7 ‘t
etra
log)
of
Coa
rcta
tion
s ot
Ric
uspi
dal
I] 3,
2 1.
2Y
aort
a3?3
0+
31
aort
ic v
alve
3
and
vent
ric
u-
righ
t la
r sr
ptal
‘i
nd v
cn t r
icul
ar
sr pt
al d
r fec
t 32
Pate
nt l
uram
cn
oval
c’
Atr
ial
scpt
al
dcfc
ct3’
34
and
patc
nt
I) un d
I c
hran
ch I
)lu<
.h”
Atr
csia
of
duct
us a
rtcr
io-
ascc
ndin
g ~
11s“
’ a”
rt
7 3 1
Ilyp
opla
$tic
ao
rtic
ar
ch ’
Ilyp
opla
stic
: va
vlul
ar
valv
c an
d le
ft
\rnt
ricl
v’
Pulm
onar
y va
lvul
ar
atrc
siaZ
6 Pu
t rno
nir
\alv
ular
\t
cnos
is4
artc
rio-
S,
,SJ.
26r3
1,33
,34.
3s
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

%
> - U
c .-
E
W R m
W L.7 3c C c V
- 3
453
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

' ! I
c c ' ' ?I
..? , 7 - , 3-
c . 2 ; - L' I
454
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

MATERNAL PHENYLKETONURIA 455
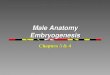
obscrved malformations are those originating in the first trimester, since development of most organ systems is largely completed by the end of the first 12 weeks of gestation. However, the dctrimental effect of hyper- phenylalaninemia is not restricted to any specific time during prc'gnancy but may have a deleterious effect throughout gestation, resulting particularly in growth retardation of the brain (Fig. 1 ) . Somatic growth is also compromised in many of these infants. While the presence of abnormalities is high in PKU offspring, they are not uniformly present, and some infants have been said to have had normal development following birth.
DISCUSS I0 N
There are many gcnetic variations o f hyperphenylalanemia. One of the variations is based on the differences in concentrations of phenylalanine48.4q 'I'hc available data suggest that the higher the concentration of maternal serum phenylalaninc during pregnancy, the higher the incidence of abnor- malities in the o f f s p r i ~ i g . ~ ~ ~ ~ ~ ~ ~ ~ ~ For example, the most commonly reported abnormality in the offspring of PKU mothers is microcephaly. The incidence of microcephaly is 2.7% in the normal p o p ~ l a t i o n . ~ ' Infants born to PKU
AFFECTED ORGANS
- BrainGrowth
-- Sornati Growth ---- Cardiovascular
Spleen
Chert Cavity
LunO
I 9
.._ ............ _ _ _ _ -.-.- - Gastrointestinal Tract
bw Urimary Tract - Ear
Eye =---
-..- Oral Cavity
000 Extremitas
o--o Neural Tube and Spine
FIGURE 1 . Thc organ systems of the fetus that arc dctrimentally affcctcd by maternal PKU prcscnted in chronological ordcr suggest that ( 1 ) thc rffcct has no organ sprcificity and (2) the anomalies occur during the rntirc course of thc prcgnancy. Numbers indicate monthyl duration of the pregnancy.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

456 R . 0. FlSCH ET AL.
mothers with blood phenylalaninc levels >20 mg/dl have a 73% incidence of microccphal).. This incidence of microcephaly decreases to 34% with levels between 16 and 19 mg/dl and t o 33% with levels between 11 and 13 mg/dl, but is reported to be 44% with levels between 3 and 10 mg/dl.' As o u r case indicates, thc affected infants exhibit n o gross malformations o r histologic abnormalitirs o f brain development b u t have brains that are disproportionatcl), small c.omparcti t o agc-matched normals, indicating that inpaired brain growth has occurred. Similarly, the incidence o f malformation o f the ciirdiovascular system in this setting is reported t o be 14% if thc concentration o f maternal blood phenylalaninc is over 20 mg/dl, 17% i f i t is between 16 m d 19 mg/dl, 13% i f i t is between 11 anti 13 mg/dl, and none i f i t is tintier IO ing/tII.'-'O
Although incrcascd conccntration of maternal serum phen),lalaninc and coiiconiitarit metabolitcs o r the deficiency o f tyrosine" have been proposed a 4 rcspc)nsiblc f o r the microcephaly and decreased birth size found in the offspring o f mothers \vith PKU, there is n o consensus on the exact mcchanism 1)). which the inability t o oxidize phrnylalanine t o tyrosine disrupts normal embr)fogenesis and fetal growth. T h e conccntration o f phcn).lalanine in the amniotic fluid from mothers with PKU has been found t o bc 3 5 times greater i hicii bu t this is no t reflected proportionately in thc fctal blood.
'I'hcre is considcrat)lc evidcncc that an cxc(:ss o f either 21 single amino ;i<.id o r o f several amino acids produces a variety o f detrimental metabolic conscqucnccs, bu t thcsc arc usually direct toxic effects. An amino acid irnbal;incc produced hy c.xcessivcly large amounts o f methionine, cystinc, o r glycinc. may have inhibitory effects on growth similar t o amino acid dct'icicnc). in rats, but phenylalaninc has relatively little ~ f f e c t . " ~ ~ ' I)cc-r.cased levels o f other amino acids ma)- play a role in abnormal cmbq.ogcnesis and in growth inhibition in the Ictus. Phenylalanine t lcpr iut ion o f rat dams leads t o severel). damaged fetuses with only a slight (20%) drop in fetal plienylalanine b u t an 80% d r o p in fctal tyrosine lcvels.s6 Kt:duced in tc,slinal absorptioin of t r y p t o p h a ~ i , ' ~ valinc," a r g i n i n ~ , ~ ~ Ieucinc, ar id tryosine60 and a relatively gcncra l ixd hypoamino acidemia6' have been ot)sct-vcd in untreated PKl.'s. Tyrosine deficiency experimentally produced in pregnant rats causes a severe inhibition o f tubulin s).nthesis in brain.62 ' I ' \ i I ) i r I i i i is thc major struc.tura1 protein in the brain cell.
T h e high incidenc c o f microcephaly and the absence of specific brain malformations in cil'fspring of mothcrs with I'KU indicates that the inhibitory effect o n brain drvelopment is no t related t o an insult a t a spccific timc during gestation but occiirs secondary t o a general developmental fai lui . t r that is present throughout pregnancy.
T h c neural plate is clearly demarcated at 16 days' gestation, and a faint
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

MATERNAL PHENVLKETONURIA 457
neural groove with early neural folds is evident by 18 days. This complex development continues throughout gestation. At approximately 6 months’ gestation, the primary fissures and sulci begin to appear. Secondary sulci develop a t approximately 8 months’ gestational age, and tertiary sulci are present a t approximately 9 months. ‘The brain weight increases from about 70 g a t approximately 24 weeks’ gestation to 250 g a t 32 weeks’ and approximately 380 g a t 40 weeks’ gestation.63964 When the brain growth spurt begins in the middle of gestation, the adult number of neurons has already been largely a c h i e v ~ d . ~ ’ At birth, only a small fraction of the total myelin is p r ~ s e n t . ~ ’ * ~ ~ As our case report indicates, the lack of malformation, the normal myclination, and normal histologic appearance indicate that the development of the central nervous system progresses normally in PKU offspring but that overall brain growth is impaired. Micrencephaly may be a reflection o f the deficit in the total number of cells, a feature that is not detectable in routine brain examination, even though cell density appears normal in all areas o f brain examined. Although the mechanism involved in brain growth inhibition is unknown, previous experimental work in rats has shown a reduction in total DNA, RNA, and protein in fetal brains subscqucnt to the administration of excessive phenylalanine and alpha- mcthylphenylalanine, which is an inhibitor o f phenylalanine h y d r o ~ y l a s e . ~ ~ It is again not a ccrtainty whether the defects were caused by phenylalanine excess, tyrosine deficirncy, or some effects of alpha-methylphenylalanine itself.
The incidence o f different malformations and the inhibitory impact on both brain and somatic growth suggests that the metabolic abnormality caused by maternal PKU phenylketonuria docs not have organ specificity. Because microccphaly and growth retardation are more common than various other malformations, one can conclude that the common pathologic effect of maternal PKU is also not time-specific during pregnancy. This may have a considerablc clinical importance, for if there is not a specific time during pregnancy that the fetus can be protected, whatever factor causes these problems, it is probably not an increased phenylalanine o r any of its metabolites, for dietary restriction at any particular time during pre<gnancy has only limited, i f any, value. Large numbers o f physically and mentally
preconccptual dietary treatment has been utilized in these mothers, even then abnormalities occurred among their ~ f f s p r i n g . ~ ’ , ~ ~ The withholding of phenylalanine as therapy is relatively ineffective, but it is reported that tryosinc added to the maternal diet during pregnancy” docs prevent abnormalities, lending credence ot the tyrosine deficiency theory of phcnylketonuria.
The presence in an infant o f the constellation of fetal and neonatal
handicapped children have been born to treated m o t h c r ~ . ~ ~ ~ ” ~ ~ ~ ’ ~ ~ Alth ough
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

458 R . 0. FlSCH ET AL.
;~ l ) i~u rma l i tics notcd i n 1 his stud). should alcrt clinicians and pathologists t o t111, possil)ilit) o f rn;itcrnal I'Kt;. Gro\\.th retardation, micwct.ph;il>-, and c 1 ) I I gcn i t al c;ir di ovasc iiI;i1- an r ) ma1 ics rep rcsen t t h c com mon c s t ;i bc r r;i t i ( )ns Ioiind in m,ircrn,il PKL.. '['his suggcsts that the lack o f t).rosinr cniiscd b\. the I.iiliii-c 01 thc mothcr norinally t o oxidizc phenylalanine t o tyrosine Ind) lead [ ( I J dcficicnc). o f t ) I osiric huppl). to the fetus. This is consistent with thc gc.nc. 1x1 t h (*( 1 I T t ical ap p i-;i( w h t c) PI( I: 'O and M' i th th c Icp ( ) r tcd con f i 1-m ;I t i o n o t that appro,[ch the successful prcvcntion o f fetal damage b y fccding t!.i.osinc t o thc mothcr throiighoiit prcgniincy. O u r s t u d y suggcsts that cvcn / H . ~ ~ c * I - siicccss might I) ( , obtained \vith tyrosine supplcmcnt t o thc P K L mc )tIici. prioi- t o concept ion.
REFERENCES
I .
_.
3.
4 .
>.
I .
h .
(1.
I t l .
11.
17.
I I . 1 5 .
I f ) .
S lab!) CC. Dcriniston I( : . S r l w i i TI., C h o w DS: Maternal phrnvlkctonuria . N FhgI J Mcd 269: 1404--1108, 1963. I isch KO. h'alkcr h ' A . ;\ridc.rcori J.4: Prcnatal and postnatal dcLelolirncntal (onsc..lucncrs of inaterndl phcnylkctoriurid. Pc diatrics 37:979 -986. 1966. S t < w i w m RE. Iluntlt L (:C: Coiigcriital maltormations i l l offspring of phrnl, lkr tonurir inorhrrs. Pediatrics 40:'37 43, 1967. t isc h KO. Docdcri D. I.alisk) LL. Anderson JA: Materndl pliciiylkctonuria: k t r i m c r i t a l cICcct, (11) rnit)rbogcncsis a ~ l d I c f d development. A m .I Dis Child 118:847--858. 1969. I.t.iikc RK, I.cv\. Il l . : hlatt.rrial phrnylkr tor iur ia dnd hyperphenylaldnincmia. An iiitcrndtiorial \urw\ t > f thc ou rcomr of un t r r a t rd and rerratcd prrgnancies. 3 k.ngI J \ l e d 303: 1202 -1208. 1980. 1 . 1 . ~ hl. , \rcilla K, Himoldi I I . J . 2 . Licdta RII. Gasul RM: Prcm.sturr ri.irrowinp o r closure vl tlir I o r d i r i c i i ovdlc . Am Heart J 65 :638-647 . 1963. l3<.( kiridn (:B, Mollrr . I [ { , k.dndrds J t:: Altcrnatr pa thwa j s to pulmonary vcnous floh in It.it.sidcd otistructivt. aniikin.tlirs. Circulation 5 2 : 5 0 9 4 1 6 . 1975. ! I \ inan .MA: Atiscncc 0 1 t h e . !eft cardiac vcntriclc, with aplasid of t h e aortic vrif:ce am! h \ popldsia of rhc aorta. Arch Yathol 4 2 : 5 9 0 4 9 3 , 1946. I I('( do in Khl: IIypoli last i t . Iclt heart svndrornc. In: Moss' Heart [)iscase in Infants, Childrcn. arid :\dolc\cciits, c d i t ( d b \ F. 11. Adams and (;. C:. k.rnmanouilidcs. Sd cd.. p. 41 I . Baltimore: I\ illiams dnd Wilkins. 1983. I.uc.i\ KV Jr. hiidcrsoii K(:. Ampldtc K , Addms P J r , Edwards JE: (hi igcii i tal C ~ U C S 01 puIrnciii.ir\ V ~ I I O U S obstructic,rl. Pidiatr C l i r i North A m 10:781 - 8 3 6 , 1963. H u n t (Xi, Kau S, hlollcr ,111, Eelwards Jk.: Anomalous pulmondr) vein scrvinx a \ collatrral ch.iiiiic.1 ii i Aortic stcrio,is \\ irh h \ popldstic Irfl vrritriclr arid ciidoi drdial IibruclastoTis. ( h e s t
S; l ld i . ir J , Martinex t , \ ' a k r u MI, (:asddo dc Frias E: Polysplcnia with l r f t vrntricular t1! popla& a n d partidl mt)ii ialous piilrntm.ar\ vri ious connect ion. h c t a Cardiol 31 ~ 4 8 3 4 9 0 , 1976. I.ucds KV J r , Lester R(;. 1-illrhei CM'. Edwards JE: Mitrdl dtrra5ia H irh Icvoatrit)cardindl vein. A dforrn of corigc.iiital p u I m ~ ~ i i a r \ YCIIIJUS obstruction. Am J Cardiol 9 :607-613 , 1962. k;ci\rdrds JE, DuSharie JN': -I hciracic venous ancimalirs. Arch Pathol 44:517 537. 1950. K C W .4G, Bcrkman CB. Edwards JE: Communicat ion bctwcen cororidry Tinu3 aiid lclt atrium. H r I l rar t J 36: 182-185, 1971. S d t h I'll. 1)cIanc) UJ, %tillikufc,r C. Ben-Sachar C;, Castaneda-Zuruga W, Formarick A. Arnplatx K: Corondrb s i n u s 4 r f t . i tr id window. Rddiolog). 135:319322, 1980.
5:: i w - i w . i g i n .
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

MATERNAL PHENYLKETONURIA 459
17. Freedom RM, Culham JAG, Rowe RI): Left atrial t o coronary sinus fencstration (partially unroofed coronary sinus). Morphological and angiocardiographic observations. Br Heart J 4 6 : 6 3 4 8 , 1981.
18. Grant CA, Robertson B: Microangiography of the pulmonary arterial system in “hypoplastic left heart syndrome.” Circulation 45:382-:388, 1972.
19. liaworth SG, Reid L: Quantitative structural study o f pulmonary circulation in thc ncwborn with aortic atrcsia, stcnosis, o r coarctation. Thorax 32: 121-128, 1977.
20. Neumann MP, Ileidelhergcr KP, Macdonald D 11, Rosenthal A: Pulmonary vascular changes associatcd with hypoplastic left vcntriclc syndromc. Pcdiatr Cardiol 1 : 3 0 1 3 0 6 , 1980.
21. Rorkc LB, Riggs HE: Myelination of the Brain in thc. Newborn. Philadelphia: J. B. Lippincott, 1969.
22. Illy L, Shcpard TII, Jakabovits A, Lemire RJ, Kcrncr P: l h c rate of growth in young human embryos of Strceter’s horkons XI11 t o XXIII. Acta Anat 66: 178-1 86, 1967.
23. Nora JJ: Updatr in the ctiology o f congcnital heart discasc and gcnctic counseling. In: Etiology and Morphogrncsis of Congcnital Ilcart Discasc. cditcd by R. van Praagh and A. Takao, pp. 21-39, Mount Kisco, SY: kutura, 1980.
24. Smith DW, Joncs KL (editors): Recognizablc Patterns o f Human Malformation: Grnrtic, Embriologic and Clinical Aspects, vol. 111: Major Prohlcms in Clinical Pediatrics, 3d cd. Philadelphia: W. B. Saundcrs, 1982.
25. Brown ES, Waisman IIA: Mcntal rctardatiori in f o u r offspring o f a hyperphcnylalanincmic mother. Pcdiatrics 4 8 : 4 0 1 4 1 0 , 1971.
26. Bovicr-Lapierrc M, Saint-Dizier C, Freycon E‘, David M, Dorche C, Jeunc M: Two infants horn o f a mothcr with phrnylkctonuria. Failure o f a low phenylalaninc dir t during second pregnancy. Pcdiatric 29:51-72, 1974.
27. Murphy D, Troy EM: Maternal phcnylketonuria. Ir J Med Sci 148:310--313, 1979. 28. Williams R: Matcrnal phrnylkctonuria. Mcd J h u s t 68:216-219, 1968. 29. Anacli E, Dcnman AR, Harris KF, Kirman BIi, Stern J: Maternal phenylketonuria: A
family with seven mentally retarded siblings. Dev Mcd Child Scurol 1 6 : 8 0 0 4 0 7 , 1974. 30. Zalcski I A , Cascy RE, Zalcski W: Maternal phrnylketonuria: Dietary trcatmcnt during
prrgnancy. Can Mrd Assoc J 121:1591-1594, 1979. 31. Smith I, Erdohazi M, Macartncy FJ, Pincott J R , W o l f OH, Brcnton DP, Biddle SA,
Fairweathcr DV, Dohbing J: Fetal damagc drspitc low-phenylalaninc dict aftcr conccption in a phcylkctonuric woman. Lancct i: 17-19, 1979.
32. IIuntley CC, Stcvenson RE: Maternal phcnylketonuria. Coursc of two prcgnancirs. Ohstct Gynccol 34:694-700, 1969.
33. Buist NR, Lis EW, Tucrck JM, Murphey W I 1 : Maternal pheyrdkctonuria. ( Ix t te r ) Lancct i i :5849, 1979.
34. Bush RT, Dukes PC: Progcny, prcgnancy and phenylketonuria. SZ .MedJ 82:226-229, 1975. 35. Michcls VV, Justice CI.: Treatment of phenylketonuria during prrgnancy. Clin ( k n c t
36. Farquhar JW: Baby of phcnylkrtonuric mother. Inferences drawn from a single case. Arch Dis Child 49:205-208, 1974.
37. Kasvistik B: Childcn of phcnylkctonuric mothers. Prenatal p h m ) lalaninc poisoning. Monatsschr Kinderheilkd 120: 189-192, 1972.
38. Lipson A, Buehler B, Bartlcy J , Walsh D, Yu J , O’lialloran M, Wehstcr W: Maternal hyprrphenylalaninemia effects. J Pcdiatr 104: 21 6-220, 1984.
39. Koch R, Balskovics M: Four cases of hyprrphenylalaninemia: Studies during pregnancy and of the offspring produced. J Inheritrd Metab Dis 5:11-15, 1982.
40. Kromrowcr GM, Sardharwalla IB, Coutts JM, Ingham D: Management of maternal phcnylketonuria: An emerging clinical problem. Br Mrd J 1:1383-1387, 1979.
41. Frankenburg Wk. Duncan BR, Cotfelt RW, Koch R, Coldwell JG, Son CD: Maternal phenylkctonuria: Implication for growth and developmcnt. J Pcdiatr 7 3 : 5 6 0 4 7 0 . 1968.
42. Blomquist HK, Gustavson KIi , Holmgrcn G: Sevcrc mental rctartiation i r i live siblings due to maternal phenylkt-tonuria. Neuropacdiatric 11:256-261, 1980.
2 1 : 1 4 1-1 44, 1982.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

460 R. 0. FlSCH ET AL.
43.
44.
45.
46. 47. 48.
49.
50.
5 1 .
52.
5 3.
54.
55.
56.
57.
.i8.
59.
60.
61.
b2.
63.
64. 65.
66.
67.
68.
69.
Levy IIL, Waisbrrq SE: Etfccts o f untrcalrd mattrrnal p h m ) Iketonurid aiid hypr i ~ ihc r iy l a l an in~~mia on thc frtus. N Eiig1.J .Mrd 309:1269--1274, 1983. Scot t lM, k y f r WM, Hart DM: Matcrnal phrnylkctonuria: i\hlic>rmdl baby dcspitr luw phcnylalaninv d i r t during prrgnancy. Arch Dis Child 5 5 : 6 3 4 4 3 7 , 1980. (;iovannini M, Riva F., Magnoni D. Calcagni I., Brsana K: Maternal hyp~~rri)hrriylalariinl-mia ar a causr o f rmbryo- l r t a l dislwc,. Minrrva Pcdiatr 31:615424, 1979. Fisch KO: Lnrr1ior t t~d cabt.. Pollak S, Vardy PA, Brazilai A: Matc.rnal phcnylketonuria syndromr. Harcfuah 100:78-80, 198 1. Scrivcr CR, Clow CI.: Phenylkr tonuria: Epi tomlc of human hiochrmical gcnctics (first 0 1 two parts). N Engl J Mcd 303: 1336 -1 342, 1980. Scrivcr CR, Clc~w CI: Phc nylkctunuria: Ep i tomr 01 human hiochrmical Krnctics (si.coild 01 t w o parts). N Engl J M r d 303:1394--1400, 1980. In-vy HL, Lrnkr RR, Crockvr AC: Matcriial PKU Procrcdings o f a Conft .rrncr, PHIIS Publication Nt). (HSA) 81-5299. Washington, D.C.: US. Dcpar tmrn t of Hcalth and Human S c n i c r s , p. 7. Nclson KB, F.llrnht.rg JH: N(.oriatal signs as predictors of cerebral palsy. Prdiatrics 64:225-232, 1979. Rrssman SP: Grnc t i c failurr 0 1 f m l amino acid “justification”: A c o m m o n basis for many forms o l nirtabolis. nutri t ional and "non-specific" mental rctardation. J Pcdiatr 81:834 842, 1972. Thomas GH, Parrncrlcy TH. Strvcnson RE, Ilowcll RR: Dcvclopmrntal changcs in amino acid concrntrat ions in human amniot ic fluic: Abnormal findings in matcrnal phrnylkctonuria . Arn .J Obs t r t Gynccol 11 1 : 3 8 4 2 , 1971. I larprr AE. Lcunx P, Yoshida A, Rugrr DR: Somr new thoughts o n aniino acid imhal;iiicc. E‘rd Proc 23:1087-1092, 1964. Salmon WD: T h r significanct. i ) I amino acid imhalaiicr in nutri t ion. Am,J Clin Nu t r 6:487 494, 1958. Brssman SP, Wapnir RA, ‘I’i)wc.ll ME: Dcwrlopmrnt of livrr phcnylalaniiic hydroxylasr and hrain aromatic hydroxylases in Iiumaii Irtusrs. Biochcm Mcd 17: 1-7, 1977. Yarho MT, Anderson J A : I .- trvptr)phanr metabolism in phcnylketonuria. J Pvdiatr 68:895-903, 1966. Krisvr S, Christianstm PA: Intr \ t inal absorpt ion 01 valinr as aflrctrtl h) o the r amino acids. .I Lab Cliii Mrd 60:1009-1010, 1962. Linncwch F, Ehrlich M, (;ra\l EH, Hundrshagcri 11: U b r r drii Amiii[)saurrn-TransI,urt bri i,hcnylkrtonririscher Oligoplirciiic. Kliri Wochrnschr 41 :253 255, 1963. I.in F X X , Wilson l l i : Transport (11 L-tyrosinc by the small intrs t inr in vitro. A m J Ph)siol 199:1?7-130, 1960. I h n r w r h I , I.;hrlich M: Zur I’athogrrirsc dcs Schwachsinns h r i Phcriylkrtonuria. Klin Wochcnsc-hr 40:225-226, 1962. Hrssman SP. Choi 21, Toni.ism\vski 1.: T h e justif ication throry: T h r rlfrct of tyrosinr dcficirnc) on tubulin synthrsis in t h r brain. In: Protr ins in thc Ncrvous Systrm: Structurr arid Funct ion, cd i t rd by B. Hahcr, pp. 187-192, iqcw York: Alan R. I k , 1982. O’Kahilly R, (;ardnrr E: . l h r t iming and s rqucnc r of rv rn t s in t h r drvclopmcnt o f t h r human i i rnous s j s t r i n during t h r r rnbrvonic prrioti proprr . Z Anat Entwickl Gcsch 134: 1-12, 197 1. I. ricdr RL: Dcvclopmrntal Xruropathology, pp. 1- 19. N r w York: Springrr-Vcrlag. 1975. Dobhing J , Sands J: Quant i ta t ivr Krowth and d rvc lopmrn t ot huniari brain. Arch Dis Child 48: i57-767, 1973. (:has? HP, Dahirrr CS, Wrlch NN, O’Brirn D: Intrautcr inr undrrnutr i t ion and brain dcvrlopmrnt . Prdiatrics 47:491-500, 1971. Spr ro D A , Yu MC: Effrc t s 0 1 matrrnal hy~irrphri iylalai icmia 011 frtal brain drvrlopmrnt: A biochrmical s tudy. Exp Ncurol 79:641654, 1983. I . rvy IIL, Kaplan GN, Eric kson AM: Comparison o f t r r a t rd and ur i t r ra t rd prrgnancirs in ino th r r n i t h phrnylkctonuria . J Prdiatr 100:876-880, 1982. Lorijn RHW, Scngcrs RCA. Trijbrls JMF: Matcrnal phrnylkctonuria: Thc o u t c o m r 01 prcsiiancy. Eur , J Ohstct Gynarcol Rcprocl Biol 12:281 -285, 1981.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.

MATERNAL PHENYLKETONURIA 461
70. Kornrowcr GM,Sardharwalla IB, Coutts JMJ, Ingham D: Managcmrnt o f matcrnal phcnylkctonuria: An rmrrgin): clinical problrm. Br Mrd.1 1:1383-1387, 1979.
Rcceivsd Dgccmber 7 , 1984 Hmisc,d uer.rion accepted March 1, 1986
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Q
UT
Que
ensl
and
Uni
vers
ity o
f T
ech
on 1
0/31
/14
For
pers
onal
use
onl
y.