Embed Size (px)
Citation preview

Maternal and perinatal outcome in women withthreatened miscarriage in the first trimester:a systematic reviewL Saraswat,a S Bhattacharya,b A Maheshwari,c S Bhattacharyad
a Department of Obstetrics and Gynaecology b Dugald Baird Centre for Research on Women’s Health c University of Aberdeen d School of
Medicine and Dentistry, University of Aberdeen, Aberdeen Maternity Hospital, Aberdeen, UK
Correspondence: Dr L Saraswat, Department of Obstetrics and Gynaecology, Aberdeen Maternity Hospital, Aberdeen AB25 2ZL, UK. Email
Accepted 24 September 2009. Published Online 26 November 2009.
Background Threatened miscarriage is a common complication in
the first trimester of pregnancy and is often associated with
anxiety regarding pregnancy outcome.
Objective We undertook a systematic review to explore the effects
of threatened miscarriage in the first trimester on maternal and
perinatal outcomes.
Search strategy An electronic literature search using MEDLINE
and EMBASE, and bibliographies of retrieved primary articles. No
language restrictions were applied.
Selection criteria All studies analysing outcomes of first-trimester
bleeding where viability was confirmed on ultrasound or the
pregnancy continued beyond viability.
Data collection and analysis Two review authors independently
selected studies and extracted data on study characteristics, quality
and accuracy. Meta-analysis was performed using Review
Manager software
Main outcome measures The outcome was broadly categorised
into maternal and perinatal outcomes. The chief maternal
outcomes included pre-eclampsia/eclampsia or pregnancy-induced
hypertension, antepartum haemorrhage, preterm prelabour
rupture of membranes (PPROM) and mode of delivery. The
perinatal outcomes evaluated were preterm delivery, low
birthweight, intrauterine growth restriction, perinatal mortality,
indicators of perinatal morbidity (Apgar scores and neonatal unit
admission) and presence of congenital anomalies.
Main results Fourteen studies met the inclusion criteria. Women
with threatened miscarriage had a significantly higher incidence of
antepartum haemorrhage due to placenta praevia [odds ratio
(OR) 1.62, 95% CI 1.19, 2.22] or antepartum haemorrhage of
unknown origin (OR 2.47, 95% CI 1.52, 4.02) when compared
with those without first-trimester bleeding. They were more likely
to experience PPROM (OR 1.78, 95% CI 1.28, 2.48), preterm
delivery (OR 2.05, 95% CI 1.76, 2.4) and to have babies with
intrauterine growth restriction (OR 1.54, 95% CI 1.18, 2.00).
First-trimester bleeding was associated with significantly higher
rates of perinatal mortality (OR 2.15, 95% CI 1.41, 3.27) and
low-birthweight babies (OR 1.83, 95% CI 1.48, 2.28).
Authors’ conclusions Threatened miscarriage in the first trimester
is associated with increased incidence of adverse maternal and
perinatal outcome.
Keywords First-trimester bleeding, maternal outcome, perinatal
outcome.
Please cite this paper as: Saraswat L, Bhattacharya S, Maheshwari A, Bhattacharya S. Maternal and perinatal outcome in women with threatened miscarriage
in the first trimester: a systematic review. BJOG 2010;117:245–257.
Introduction
First-trimester bleeding is a common complication which
affects 16–25% of all pregnancies.1 Threatened miscarriage
is diagnosed on the basis of documented fetal cardiac activ-
ity on ultrasound with a history of vaginal bleeding in the
presence of a closed cervix. Bleeding during pregnancy
can cause maternal anxiety and emerging evidence suggests
that it may be associated with poor fetal and maternal
outcomes.2–9
It is hypothesised that first-trimester bleeding may indi-
cate an underlying placental dysfunction, which may mani-
fest later in pregnancy causing adverse outcomes such as
increased risk of pre-eclampsia, preterm delivery, preterm
prelabour rupture of membranes (PPROM), placental
abruption and intrauterine growth restriction (IUGR).8
ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 245
DOI: 10.1111/j.1471-0528.2009.02427.x
www.bjog.orgSystematic review

Knowledge about the outcome of ongoing pregnancies
following first-trimester bleeding is relevant to both women
and their obstetricians in order to plan antenatal care and
consider clinical interventions in pregnancy. Several pri-
mary studies have sought to identify adverse fetal out-
comes, but very few have commented on maternal
complications. A previous meta-analysis summarised the
evidence on adverse perinatal outcome following vaginal
bleeding in the first and second trimesters of pregnancy,10
but language restrictions in its search strategy and the lack
of quality assessment of the studies included potentially
limit the strength of its inferences. Moreover, several new
primary studies have been published since that warrant
inclusion in an updated systematic review. To date, we
know of no systematic review that has looked into both
maternal and perinatal outcomes following first-trimester
bleeding. We therefore undertook a comprehensive system-
atic review on maternal and perinatal outcomes following
first-trimester bleeding.
Methods
A study protocol stating the research question to be
addressed, the population and conditions of interest, the
exposure and outcomes considered, the criteria used for
identifying and selecting or excluding studies, and the
methods used for extracting and analysing data preceded
this systematic review. We followed the guidelines of the
Meta-analysis of Observational Studies in Epidemiology
(MOOSE) group.11
Literature search
Prospective and retrospective observational studies evaluat-
ing the association between threatened miscarriage and
maternal and perinatal outcomes were identified using the
computerised databases MEDLINE (US National Library of
Medicine, Bethesda, MD, USA) and EMBASE (Elsevier,
Amsterdam, the Netherlands). The searches were conducted
for published literature from January 1976 to April 2009,
without language restrictions. The search strategy was writ-
ten in Ovid, then modified and run in each database. Adja-
cency operators and truncation were used. Our search term
combination for electronic databases was MeSH headings
(Medical Subject Headings, US National Library of Medi-
cine), text words, and word variants for threatened miscar-
riage and for maternal and perinatal outcomes.
The citation lists were independently reviewed by two
authors (LS and SB). Titles and abstracts were screened and
articles were retrieved if they passed the relevance filter or if
there was uncertainty as to whether or not they were rele-
vant. References from identified studies were also screened
for relevant citations. Retrieved articles were then reviewed
for inclusion/exclusion criteria. Those articles that met the
criteria were then kept for critical appraisal and data collec-
tion using a standard data-capture form. A review of litera-
ture suggested that the use of ultrasound scan in early
pregnancy diagnosis only became popular in the late 1970s
and early 1980s. Therefore, following a general consensus
among the authors, we decided to include only the pub-
lished literature from 1976 to April 2009. As more than one
database was searched, there was some degree of duplication
in the citations identified. Therefore references were man-
aged using ‘RefWorks’ software (RefWorks-COS, Proquest,
Ann Arbor, MI, USA) and duplicates were removed.
Study selection
Inclusion and exclusion criteriaThere were variations in the definitions of ‘threatened mis-
carriage’ and ‘first trimester’ among published studies. We
therefore adopted an inclusive approach and selected all
studies that took into account pregnant women with first-
trimester bleeding where viability was confirmed on ultra-
sound or the pregnancy continued beyond viability. Only
case–control or cohort studies were included in the review.
Case series and studies without controls were excluded.
Outcome measuresWe categorised outcomes broadly into maternal and peri-
natal outcomes. The maternal outcomes included, pre-
eclampsia/eclampsia or pregnancy-induced hypertension
(PIH), antepartum haemorrhage (APH; placenta praevia,
abruption, other APH), PPROM, mode of delivery (instru-
mental and caesarean deliveries), postpartum haemorrhage
(PPH) and retained placenta. The perinatal outcomes eval-
uated were preterm delivery (delivery before 37 completed
weeks), low birthweight (birthweight £2500 g), IUGR, peri-
natal mortality, indicators of perinatal morbidity (Apgar
scores and neonatal unit admission) and presence of con-
genital malformations.
Data synthesis and statistical analysisWe assessed the methodological quality of each study using
the Newcastle–Ottawa scale.12 All studies that met our inclu-
sion criteria were independently evaluated by two reviewers
(LS and SB). We designed a data abstraction form, and the
two reviewers abstracted the data separately. Discrepancies
regarding the inclusion of studies or abstracted data were
resolved by discussion. Where necessary, we contacted
researchers to obtain additional information about study
methods or outcome measures. We entered and analysed the
data using RevMan 4.2 (Cochrane Collaboration, Oxford,
UK). For each outcome, data were only pooled if there were
at least two studies available for a particular outcome mea-
sure. As adjustments for confounding variables varied
Saraswat et al.
246 ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology

among different studies, we used the raw numbers from each
study to calculate the crude odds ratios (OR) and 95% CI
for each outcome before pooling the data. A random effect
model was used (because of statistical heterogeneity in the
outcome data) to calculate combined OR, 95% CI. Tests of
heterogeneity were performed before pooling the data.
Results
Thirty-one publications evaluating the effect of threatened
miscarriage on maternal or perinatal outcome were identi-
fied. A hand search of references of the above papers iden-
tified another seven potentially useful references.
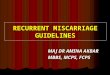
These 38 references were reviewed for inclusion and
exclusion criteria. Figure 1 summarises the process of liter-
ature identification and selection.
Of these references, 16 met the inclusion criteria,
although there was variation in the definition of threatened
miscarriage in terms of gestational age. However, two of
these articles were excluded because of insufficient data.13,14
In both cases, the authors were contacted but no response
was obtained. As a consequence, a total of 145–9,15–23 stud-
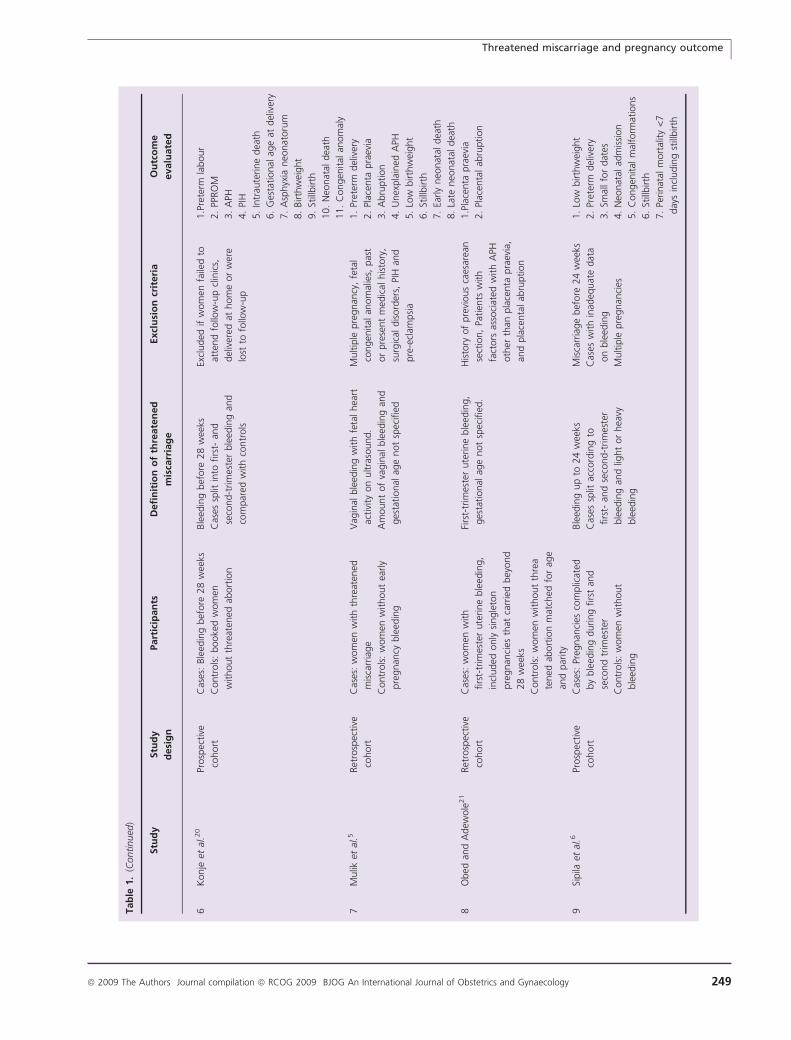
ies were included in the meta-analysis. Thirteen of the 14
studies included in the meta-analysis employed a cohort
design. The report by Hossain et al.17 was a case–control
study. Of the cohort studies, six had a retrospective design
and the other seven used prospective cohorts. The study
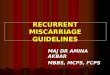
characteristics are described in Table 1.
Women with first-trimester bleeding had an elevated risk
of adverse maternal and perinatal outcome.
Maternal outcomes
Pregnancy-induced hypertension, pre-eclampsiaand eclampsiaSix of the 14 studies reported on PIH, pre-eclampsia and
eclampsia. The incidence of PIH, pre-eclampsia or eclamp-
sia was not significantly altered by bleeding in first tri-
mester; OR (95% CI) of 0.99 (0.84, 1.17). These results
could be attributed to the influence of two large studies by
Weiss et al.8 and Wijesiriwardana et al.9 There was no sig-
nificant heterogeneity (P = 0.19) in results across the dif-
ferent studies (Figure 2A).
Antepartum haemorrhageWomen with first-trimester bleeding were prone to subse-
quent APH in pregnancy. The meta-analysis included all
those studies that analysed outcomes following first-trimes-
ter bleeding where the pregnancy continued beyond
viability. In this context we have defined APH as bleeding
beyond viability (‡24 weeks). These women were more
likely to have placenta praevia (OR 1.62, 95% CI 1.19, 2.22)
as well as placental abruption (OR 1.46, 95% CI 1.00, 2.14).
Antepartum haemorrhage of unknown origin was twice as
likely in those with threatened miscarriage (OR 2.47, 95%
CI 1.52, 4.02) as in women without first-trimester bleeding.
Except for placental abruption (P = 0.03) there was no sig-
nificant statistical heterogeneity (placenta praevia P = 0.46,
APH of unknown origin P = 0.07) when results were
pooled across the different studies (Figure 2B).
Preterm prelabour rupture of membranesThe incidence of PPROM was significantly higher in
women whose pregnancy was complicated by first-trimester
bleeding (OR 1.78, 95% CI 1.28, 2.48). The test of hetero-
geneity for PPROM was significant (P = 0.01) (Figure 2C).
Mode of deliveryFirst-trimester bleeding did not appear to influence the mode
of delivery. The risk of instrumental delivery (OR 1.01, 95%
CI 0.96, 1.07) or caesarean section (OR 0.92, 95% CI 0.73,
1.16) was not significantly altered. There was evidence of
significant statistical heterogeneity (P = 0.00001) in results
relating to the risk of caesarean section (Figure 2D).
Other maternal outcomesThe only study in the meta-analysis that evaluated PPH
and retained placenta as an outcome is by Wijesiriwardana
Total citations identified from initial search (n = 6043)
Citations excluded after removing duplicates and screening titles
and/or abstracts (n = 6012)
Potential references reviewed for detailed evaluation (n = 38) From electronic search (n = 31) From reference list (n = 7)
Studies included in the review (n = 14)
Excluded studies (n = 24) Reason for exclusion Review =1 No control group = 3 Bleeding in assisted reproductive technique pregnancies = 2 Bleeding beyond first trimester = 14 Threatened miscarriage with intrauterine haematoma = 2 Insufficient data =2
Figure 1. Study selection process.
Threatened miscarriage and pregnancy outcome
ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 247

Tab
le1.
Char
acte
rist
ics
of
the
studie
sin
cluded
Stu
dy
Stu
dy
desi
gn
Part
icip
an
tsD
efi
nit
ion
of
thre
ate
ned
mis
carr
iag
e
Excl
usi
on
crit
eri
aO
utc
om
e
evalu
ate
d
1A
rafa
etal
.15
Ret
rosp
ective
cohort
study
Cas
es:
wom
enw
ith
firs
t-an
d
seco
nd-t
rim
este
rble
edin
g
Contr
ols
:w
om
enw
ithout
ble
edin
g
Wom
enw
ith
firs
t-an
d
seco
nd-t
rim
este
rble
edin
g,
incl
uded
both
light
and
hea
vy
ble
edin
g
Outc
om
eas
sess
edse
par
atel
yfo
r
firs
t-an
dse
cond-t
rim
este
r
ble
edin
g
Excl
uded
multip
lebirth
s,
ble
edin
gin
third
trim
este
ronly
,
wher
eth
ere
was
confu
sion
regar
din
gsp
ott
ing
and
mis
sed
abort
ion
1.
Low
birth
wei
ght
2.
Prem
aturity
3.G
row
thre
strict
ion
4.
Congen
ital
anom
aly
5.
Perinat
aldea
th
2D
avar
i-Ta
nha
etal
.16
Prosp
ective
cohort
study
Cas
es:
wom
enw
ith
firs
t-tr
imes
ter
ble
edin
g
Contr
ols
:w
om
enw
ithout
ble
edin
g
Wom
enw
ith
ble
edin
gin
firs
t
trim
este
r
Not
defi
ned
1.
Pre-
ecla
mpsi
a
2.
Plac
enta
pra
evia
3.
Plac
enta
lab
ruption
4.
PPRO
M
5.
Cae
sare
andel
iver
y
6.
Pret
erm
del
iver
y
7.
IUG
R
8.
Low
birth
wei
ght
9.
Intr
aute
rine
dea
th
3H
oss
ain
etal
.17
Cas
e–co
ntr
ol
Cas
es:
wom
enw
ith
pre
term
del
iver
y
Contr
ols
:w
om
enw
ithout
pre
term
del
iver
y
Wom
enw
ith
ble
edin
gin
firs
tor
seco
nd
trim
este
r.O
utc
om
e
asse
ssed
separ
atel
yfo
rfirs
t-
and
seco
nd-t
rim
este
rble
edin
g
Multip
lepre
gnan
cies
,fe
tal
dem
ise
prior
to28
wee
ks,
wom
enlo
stto
follo
w-u
p
1.
Pret
erm
del
iver
y
2.
PPRO
M
4Jo
hns
etal
.18
Ret
rosp
ective
cohort
Cas
es:
pre
gnan
tw
om
enw
ith
ble
edin
gor
abdom
inal
pai
nat
<12
wee
ks
Contr
ols
:as
ympto
mat
icw
om
en
atte
ndin
gdat
ing
scan
at
11–1
4w
eeks
mat
ched
for
age
and
par
ity
Vag
inal
ble
edin
gor
abdom
inal
pai
nat
<12
com
ple
ted
wee
ks
Multip
lepre
gnan
cies
Wom
enw
ho
opte
dfo
r
term
inat
ion
1.
PIH
2.
Feta
lgro
wth
rest
rict
ion
3.
Plac
enta
lab
ruption
(and
intr
aute
rine
dea
th)
4.
PPRO
M
5.
Pret
erm
labour
5Jo
hns
and
Jaunia
ux1
9
Prosp
ective
cohort
Cas
es:
wom
enw
ith
vagin
alble
edin
g
at<
14
com
ple
ted
wee
ks
Contr
ols
:ag
e-m
atch
edw
om
enw
ho
booke
dfo
ran
tenat
alca
rein
the
hosp
ital
during
the
sam
etim
e
per
iod
Vag
inal
ble
edin
gin
anongoin
g
pre
gnan
cyof
<14
wee
ks,
only
wom
enw
ith
fres
hre
dble
edin
g
wer
eel
igib
le
Excl
uded
wom
enw
ith
‘spott
ing’
only
.
Twin
s,co
ngen
ital
ute
rine
anom
aly,
larg
ele
iom
yom
ata
dis
tort
ing
the
ute
rine
cavi
ty,
know
nth
rom
bophili
a
1.
Pret
erm
labour
2.
Late
mis
carr
iage
(14
to
22
+6
wee
ks)
3.
PPRO
M
4.
Pre-
ecla
mpsi
a
5.
Abru
ption
6.
Plac
enta
pra
evia
7.
Congen
ital
anom
alie
s
Saraswat et al.
248 ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology
Tab
le1.
(Continued
)
Stu
dy
Stu
dy
desi
gn
Part
icip
an
tsD
efi
nit
ion
of
thre
ate
ned
mis
carr
iag
e
Excl
usi
on
crit
eri
aO
utc
om
e
evalu
ate
d
6K
onje
etal
.20
Prosp
ective
cohort
Cas
es:
Ble
edin
gbef
ore
28
wee
ks
Contr
ols
:booke
dw
om
en
without
thre
aten
edab
ort
ion
Ble
edin
gbef
ore
28
wee
ks
Cas
essp
litin
tofirs
t-an
d
seco
nd-t
rim
este
rble
edin
gan
d
com
par
edw
ith
contr
ols
Excl
uded
ifw
om
enfa
iled
to
atte
nd
follo
w-u
pcl
inic
s,
del
iver
edat
hom
eor
wer
e
lost
tofo
llow
-up
1.P
rete
rmla
bour
2.
PPRO
M
3.
APH
4.
PIH
5.
Intr
aute
rine
dea
th
6.
Ges
tational
age
atdel
iver
y
7.
Asp
hyx
ianeo
nat
oru
m
8.
Birth
wei
ght
9.
Still
birth
10.
Neo
nat
aldea
th
11.
Congen
ital
anom
aly
7M
ulik
etal
.5Ret
rosp
ective
cohort
Cas
es:
wom
enw
ith
thre
aten
ed
mis
carr
iage
Contr
ols
:w
om
enw
ithout
early
pre
gnan
cyble
edin
g
Vag
inal
ble
edin
gw
ith
feta
lhea
rt
activi
tyon
ultra
sound.
Am
ount
of
vagin
alble
edin
gan
d
ges
tational
age
not
spec
ified
Multip
lepre
gnan
cy,
feta
l
congen
ital
anom
alie
s,pas
t
or
pre
sent
med
ical
his
tory
,
surg
ical
dis
ord
ers,
PIH
and
pre
-ecl
ampsi
a
1.
Pret
erm
del
iver
y
2.
Plac
enta
pra
evia
3.
Abru
ption
4.
Unex
pla
ined
APH
5.
Low
birth
wei
ght
6.
Still
birth
7.
Early
neo
nat
aldea
th
8.
Late
neo
nat
aldea
th
8O
bed
and
Adew
ole
21
Ret
rosp
ective
cohort
Cas
es:
wom
enw
ith
firs
t-tr
imes
ter
ute
rine
ble
edin
g,
incl
uded
only
single
ton
pre
gnan
cies
that
carr
ied
bey
ond
28
wee
ks
Contr
ols
:w
om
enw
ithout
thre
a
tened
abort
ion
mat
ched
for
age
and
par
ity
Firs
t-tr
imes
ter
ute
rine
ble
edin
g,
ges
tational
age
not
spec
ified
.
His
tory
of
pre
vious
caes
area
n
sect
ion,
Patien
tsw
ith
fact
ors
asso
ciat
edw
ith
APH
oth
erth
anpla
centa
pra
evia
,
and
pla
centa
lab
ruption
1.P
lace
nta
pra
evia
2.
Plac
enta
lab
ruption
9Si
pila
etal
.6Pr
osp
ective
cohort
Cas
es:
Preg
nan
cies
com
plic
ated
by
ble
edin
gduring
firs
tan
d
seco
nd
trim
este
r
Contr
ols
:w
om
enw
ithout
ble
edin
g
Ble
edin
gup
to24
wee
ks
Cas
essp
litac
cord
ing
to
firs
t-an
dse
cond-t
rim
este
r
ble
edin
gan
dlig
ht
or
hea
vy
ble
edin
g
Mis
carr
iage
bef
ore
24
wee
ks
Cas
esw
ith
inad
equat
edat
a
on
ble
edin
g
Multip
lepre
gnan
cies
1.
Low
birth
wei
ght
2.
Pret
erm
del
iver
y
3.
Smal
lfo
rdat
es
4.
Neo
nat
alad
mis
sion
5.
Congen
ital
mal
form
atio
ns
6.
Still
birth
7.
Perinat
alm
ort
ality
<7
day
sin
cludin
gst
illbirth
Threatened miscarriage and pregnancy outcome
ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 249

Tab
le1.
(Continued
)
Stu
dy
Stu
dy
desi
gn
Part
icip
an
tsD
efi
nit
ion
of
thre
ate
ned
mis
carr
iag
e
Excl
usi
on
crit
eri
aO
utc
om
e
evalu
ate
d
10
Stro
bin
oan
dPa
nte
l7Pr
osp
ective
cohort
Cas
es:
wom
enw
ith
vagin
al
ble
edin
gin
pre
gnan
cy
Contr
ols
:Pr
enat
alw
om
en
regis
tere
dbef
ore
22
wee
ks
Firs
t-tr
imes
ter
ble
edin
g.
Ble
edin
gsp
litin
tolig
ht
and
hea
vyble
edin
g
Multip
lebirth
s,lo
stto
follo
w-u
p,
unkn
ow
n
ble
edin
ghis
tories
1.
Low
birth
wei
ght
2.
Pret
erm
del
iver
y
3.
Smal
lfo
rges
tational
age
4.
Plac
ebta
lab
ruption
and
pla
centa
pra
evia
5.
Chro
moso
mal
anom
aly
6.
Mal
form
atio
n
11
Tongso
ng
etal
.22
Prosp
ective
cohort
Cas
es:
wom
enw
ith
firs
t-tr
imes
ter
ble
edin
g
Contr
ols
:w
om
enw
ithout
firs
t-tr
imes
ter
ble
edin
g
Firs
t-tr
imes
ter
ble
edin
g
with
single
viab
le
intr
aute
rine
pre
gnan
cy
on
ultra
sound
Multip
lebirth
s,Lo
stto
follo
w-u
p
1.
Sponta
neo
us
abort
ion
(bef
ore
20
com
ple
ted
wee
ks)
2.
Pret
erm
del
iver
y
3.
Prem
ature
ruptu
reof
mem
bra
nes
4.
APH
5.
PIH
6.C
horioam
nio
nitis
7.
Congen
ital
anom
alie
s
8.
Feta
lgro
wth
rest
rict
ion
9.
Still
birth
10.
Low
birth
wei
ght
11.
Cae
sare
anse
ctio
n
12.
Apgar
score
at5
min
<7
13.
Mea
nbirth
wei
ght
12
Wei
sset
al.
8Pr
osp
ective
cohort
Cas
es:
wom
enw
ith
ble
edin
g
up
to14
wee
ks
Contr
ols
:W
om
enw
ithout
firs
t-tr
imes
ter
ble
edin
g
Vag
inal
ble
edin
gin
firs
t
trim
este
r.C
ases
split
acco
rdin
gto
light
and
hea
vyble
edin
g
Not
defi
ned
.
Adju
stm
ents
mad
ein
stat
istica
lm
odel
for
pote
ntial
confo
undin
g
fact
ors
1.
IUG
R
2.
Ges
tational
hyp
erte
nsi
on
3.
Pre-
ecla
mpsi
a
4.
Pret
erm
del
iver
y
5.
PPRO
M
6.
Plac
enta
lab
ruption
7.
Plac
enta
pra
evia
8.
Cae
sare
andel
iver
y
Saraswat et al.
250 ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology

Tab
le1.
(Continued
)
Stu
dy
Stu
dy
desi
gn
Part
icip
an
tsD
efi
nit
ion
of
thre
ate
ned
mis
carr
iag
e
Excl
usi
on
crit
eri
aO
utc
om
e
evalu
ate
d
13
Wije
siriw
ardan
a
etal
.9
Ret
rosp
ective
cohort
Cas
es:
wom
enw
ith
vagin
alble
edin
gbef
ore
12
wee
ksw
her
e
pre
gnan
cyco
ntinued
to
am
inim
um
of
24
wee
ks
Contr
ols
:W
om
en
del
iver
ing
afte
r
24
wee
ksw
ithin
the
sam
etim
eper
iod,
but
without
firs
t-tr
imes
ter
ble
edin
g
Wom
enw
ith
vagin
al
ble
edin
gbef
ore
12
wee
ksw
her
e
pre
gnan
cyco
ntinued
to
am
inim
um
of
24
wee
ks
Wom
enw
ith
com
ple
te,
inco
mple
te,
or
mis
sed
mis
carr
iage.
Wom
enopting
for
term
inat
ion
Multip
lepre
gnan
cies
Preg
nan
cies
with
feta
l
mal
form
atio
n
Hyd
atid
iform
mole
s
Seco
nd-t
rim
este
r
mis
carr
iages
1.
Pre-
ecla
mpsi
a
2.
Ecla
mpsi
a
3.
Plac
enta
lab
ruption
4.
Plac
enta
pra
evia
5.O
ther
APH
6.
PPRO
M
7.
Induce
dla
bour
8.
Inst
rum
enta
ldel
iver
y
9.
Elec
tive
caes
area
n
10.
Emer
gen
cyca
esar
ean
11.
Post
par
tum
hae
morr
hag
e
12.
Man
ual
rem
ova
lof
pla
centa
13.
Pret
erm
del
iver
y
14.
Mal
pre
senta
tion
15.
Still
birth
16.
Neo
nat
aldea
th
17.
Birth
wei
ght
<2500
g
18.
Apgar
at5
min
<7
19.
Adm
issi
on
toneo
nat
alunit
14
Will
iam
set
al.2
3Ret
rosp
ective
cohort
Cas
es:
wom
enw
ith
firs
t-
trim
este
rble
edin
gw
ho
del
iver
edaf
ter
20
wee
ks
Contr
ols
:w
om
enw
ith
no
vagin
alble
edin
g
Vag
inal
ble
edin
gor
spott
ing
limited
tofirs
t
trim
este
r
Preg
nan
cies
com
plic
ated
with
dia
bet
es,
pla
centa
pra
evia
,pla
centa
l
abru
ption,
or
idio
pat
hic
ble
edin
gbeg
innin
gin
trim
este
rsoth
erth
an
the
firs
t
1.
Low
birth
wei
ght
2.
Pret
erm
birth
3.
Term
low
birth
wei
ght
4.
Still
birth
5.
Neo
nat
aldea
th
APH
,an
tepar
tum
hae
morr
hag
e;IU
GR,
intr
aute
rine
gro
wth
rest
rict
ion;
PIH
,pre
gnan
cy-induce
dhyp
erte
nsi
on;
PPRO
M,
pre
term
pre
labour
ruptu
reof
mem
bra
nes
.
Threatened miscarriage and pregnancy outcome
ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 251

et al.9 They reported increased incidence of PPH (OR 1.13,
95% CI 1.04, 1.23) and manual removal of retained pla-
centa (OR 1.45, 95% CI 1.26, 1.68). However, in the origi-
nal study, after adjusting for potential confounders the
increase in PPH was no longer significant.
Perinatal outcome
First-trimester bleeding was a predictor of poor perinatal
outcome.
Preterm deliveryThe reported risk of preterm delivery in women with threa-
tened miscarriage varied between 1.5 and 4.5 across the dif-
ferent studies. The overall adjusted risk of preterm delivery
was 2.05 (95% CI 1.76, 2.4) in women who experienced
first-trimester bleeding. There was evidence of significant
statistical heterogeneity in reported results (P < 0.0001)
(Figure 3A).
Intrauterine growth restrictionA significant association existed between first-trimester
bleeding and IUGR. The risk of having a baby with IUGR
was 1.54 (95% CI 1.18, 2.0) times in women with first-tri-
mester threatened miscarriage. Once again there was evi-
dence of significant statistical heterogeneity (P = 0.0002) in
the reported results (Figure 3B).
Low birthweightThe overall risk of having a low-birthweight baby was
higher in women who bled in the first trimester (OR 1.83,
95% CI 1.48, 2.28) than in women who did not. The risk
varied from 1.1 to 3.7 across the different studies. The test
for heterogeneity was highly significant (P < 0.0001) (Fig-
ure 3C).
Perinatal mortalityPerinatal deaths were observed to be nearly twice as fre-
quent in women who experienced threatened miscarriage
when pooled across different studies (OR 2.15, 95% CI
1.41, 3.27). The results displayed evidence of significant sta-
tistical heterogeneity (P = 0.001) (Figure 3D).
Perinatal morbidityThe women with history of early pregnancy bleeding were
more likely to deliver babies with Apgar score <7 at 5 min-
utes after birth (OR 1.2, 95% CI 1.03, 1.4) and babies that
were admitted to the neonatal unit (OR1.13, 95% CI 1.03,
1.23) (Figure 3E).
Congenital malformationsFour studies reported the incidence of congenital anomalies
in babies born to mothers with early pregnancy bleeding.
The odds of having a baby with a congenital anomaly was
1.26 (95% CI 0.89, 1.79) (Figure 3F).
Discussion
In this comprehensive review we evaluated 12 different
maternal and perinatal outcomes and found a consistent
association between first-trimester bleeding and adverse
fetal and maternal outcomes.
To our knowledge this is the first report to systematically
review and pool data on both maternal and perinatal out-
comes associated with first-trimester bleeding. It was rigor-
ously carried out without language restrictions and met the
criteria laid down in the MOOSE statement.11 We paid
careful attention to quality assessment of studies and col-
lected information important for evaluation of the validity
of the observed associations, potential for bias, and causal-
ity.
Our literature search identified one previous meta-analy-
sis by Ananth and Savitz,10 which evaluated the effect of
vaginal bleeding up to 28 weeks and focused on perinatal
outcomes only. This systematic review included 28 studies
published between 1950 and 1992 and found that vaginal
bleeding was associated with increased risk of low birth-
weight, preterm birth, stillbirth, perinatal death and con-
genital malformations in infants. However, with changes in
practice and advances in medical technology, the limit of
viability is now 20 weeks (World Health Organization) or
24 weeks (UK) and therefore the 28-week cutoff used by
Ananth and Savitz10 is no longer compatible with the cur-
rent practice as there would be overlap between exposure
and outcome with this approach. Moreover, the objective
of our meta-analysis was to evaluate the association of
bleeding primarily in the first trimester with both maternal
as well as perinatal outcome. Only those studies that have
used first-trimester bleeding as inclusion criteria for the
women or have performed an independent analysis for
first-trimester or any subsequent bleeding were included in
the review. Among the included studies, five studies evalu-
ated outcome following first-trimester and second-trimester
bleeding and performed separate analysis for each trimes-
ter. For the purpose of the review, we have only used data
relating to first-trimester bleeding. As a consequence, this
meta-analysis aims to provide information regarding preg-
nancy outcomes for women who had threatened miscar-
riage in the first trimester.
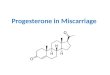
Figure 2. Maternal outcome: (A) pregnancy-induced hypertension, pre-eclampsia, eclampsia; (B) antepartum haemorrhage – placental praevia,
placental abruption and antepartum haemorrhage of unknown origin; (C) preterm prelabour rupture of membranes; (D) mode of delivery –
instrumental delivery and caesarean section.
Saraswat et al.
252 ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology

A
B
C
D
Threatened miscarriage and pregnancy outcome
ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 253

A
B
C
D
E
F
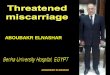
Figure 3. Perinatal outcome: (A) preterm delivery; (B) intrauterine growth restriction; (C) low birthweight; (D) perinatal mortality; (E) perinatal
morbidity – Apgar score and neonatal unit admission; (F) congenital anomalies.
Saraswat et al.
254 ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology

Women with threatened miscarriage have a higher likeli-
hood of miscarrying. Some of the studies included in the
review reported miscarriage rates whereas others only
included women where pregnancy continued beyond viabil-
ity. Five out of the 14 studies reported miscarriage rates.
Davari-Tanha et al.16 quoted a figure as high as 42.7%
spontaneous pregnancy loss in first trimester whereas other
studies reported miscarriage incidence of 7.8% by
14 weeks,18 9.3% in first trimester,19 5.5% by 20 weeks22
and Weiss et al.8 reported a rate of 1% for light bleeding
and 2% for heavy bleeding by 24 weeks. However, none of
these studies excluded these women from the denominator
when reporting results.
One of the challenges of performing this systematic
review was the fact that the definition of threatened miscar-
riage is rarely stated in explicit terms. Some studies have
defined first trimester up to 12 weeks,5,9 some up to
14 weeks8,19 whereas others have just mentioned first tri-
mester without defining gestational age in terms of
weeks.6,16,22,23 Moreover, it is possible that the risk of
adverse outcome may be different in women who experi-
ence ‘light’ versus ‘heavy’ bleeding. While some studies
have attempted to distinguish between light and heavy
bleeding,6–8 others have failed to do so. However, in this
context it is important to realise that subjective assessment
of blood loss is often erroneous in such situations and
objective assessment is often impractical.
Limitations and potential bias
Meta-analyses are limited by biases introduced through
individual studies as well as through the processes of sys-
tematic review and quantitative summary. Although we rig-
orously carried out an extensive literature search, we were
unable to search the grey literature and unpublished data.
Hence publication bias may have an impact on our results.
Moreover, in meta-analyses of observational data secondary
researchers are unable to adjust for potential confounders;
however, the present topic does not lend itself to experi-
mental studies including randomised trials. Despite this,
the consistent associations seen in large primary studies
included in our review would suggest that the direction of
association would remain even if we had missed smaller
studies with equivocal or negative associations.
Other concerns relate to the use of non-standard defini-
tions with questionable validity or reliability to discrimi-
nate between the exposure and the outcome. Often studies
were lacking in one or another quality feature. For these
reasons, associations that are not strong and consistent
should be viewed as no more than hypothesis generating.
Also, confidence in some of the findings may be con-
strained as certain outcomes have been evaluated only by
one or two studies. The study by Wijesiriwardana et al.9
was the only one that looked at outcomes like PPH, and
retained placenta.
Diverse factors are associated with poor pregnancy out-
come such as maternal age, social class, ethnicity and previ-
ous obstetric history so it is difficult to compare directly
the results of individual outcomes across all studies because
of varying degrees of control for potential confounders.
For certain outcomes like placental abruption, PPROM,
preterm delivery, IUGR and low birthweight the assump-
tion of homogeneity was violated when the overall risks
were adjusted for different studies and designs. The way
around this would be to perform a meta-regression, but
the number of studies looking at each individual outcome
was too small.
Inter-related risk factors
It is important to disentangle the relative importance of
key outcomes that may be inter-related. For instance,
women with PPROM are more likely to have preterm
babies who may in turn be of low birthweight. We could
not perform multivariate analysis in our meta-analyses to
explore such interactions between factors. Pooling of raw
data from relevant studies in meta-analysis from individual
women might help to clarify the causality of some observed
associations. Moreover, for certain outcomes like preterm
labour/delivery, most studies have given the overall risk of
preterm labour/delivery and not made an attempt to distin-
guish between spontaneous labour or iatrogenic preterm
delivery and therefore the association should be interpreted
with caution.
Meaning of findings
Reasons for the association between first-trimester bleeding
and adverse pregnancy outcomes are poorly understood.
Bleeding in the first trimester may be associated with a
chronic inflammatory reaction in the decidua. It is known
that in about two-thirds of early pregnancy failures, there
is evidence of defective placentation, characterised by thin-
ner and fragmented trophoblast shell and reduced cyto-
trophoblast invasion of the spiral arterioles. Later
pregnancy complications such as pre-eclampsia, preterm
labour and PPROM have been shown to be associated with
impaired placentation and failure of physiological invasion
of the spiral arterioles. Problems with placental develop-
ment may therefore explain why women with threatened
miscarriage are more likely to have placenta praevia, pla-
cental abruption and APH of unknown origin.
Our data highlight the fact that first-trimester bleeding
increases the risk of prematurity, growth restriction and
perinatal deaths. While some of the incidences of prematu-
rity can be linked to maternal complications such as APH,
Threatened miscarriage and pregnancy outcome
ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 255

growth restriction suggests a degree of placental compro-
mise.
Overall, our results suggest that pregnancies with first-
trimester bleeding are at a higher risk for poor fetal and
maternal outcome compared with women without bleed-
ing. However owing to the risk of adverse outcomes being
relatively modest (OR £2) and the lack of availability of
any specific interventions to prevent these adverse events, it
would be premature to suggest a policy of increased fetal
and maternal surveillance.
Further research
Our review consists of six retrospective cohort studies and
seven studies with a prospective cohort design as well as
one case–control study. Prospective cohort studies are a
more reliable way of establishing a causal association
because retrospective designs are subject to recall bias.
However, bearing in mind the significant cost (both
financial and manpower) implications of implementing a
programme of increased surveillance and the limitations
of the studies included in the meta-analysis, perhaps what
is needed are more prospective studies on women with
and without vaginal bleeding in early pregnancy that are
large enough to allow subgroup analyses based on gesta-
tion, severity and duration of bleeding to be performed
with a degree of confidence. Another possibility is to
aggregate raw data from existing studies to perform indi-
vidual women data meta-analysis, which will permit
adjustment for confounders and meaningful subgroup
analyses.
In conclusion, the current meta-analysis reports that
women with first-trimester threatened miscarriage are at
increased risk of adverse maternal and perinatal outcome,
although in the majority of women the risks are low
(OR £2). As a consequence, in the interim, it would be
rational to use the findings of our review to reassure
women with first-trimester bleeding and at the same
time alert clinicians for the signs of the possible compli-
cations.
Disclosure of interestsNone of the authors report any conflict of interest or
financial interest.
Contribution to authorshipL.S. prepared the protocol, collected data, assessed eligibil-
ity and methodological quality of studies and wrote the
review. S.B. conceived the idea, conducted searches,
assessed eligibility and quality of studies, and provided
comments on the manuscript. A.M. performed the statisti-
cal analysis and S.B. conceived the idea, provided com-
ments on the manuscript and supervised the review.
Details of ethics approvalApproval was not required.
FundingNot required. j
References
1 Farrell T, Owen P. The significance of extrachorionic membrane sep-
aration in threatened miscarriage. Br J Obstet Gynaecol
1996;103:926–8.
2 Batzofin JH, Fielding WL, Friedman EA. Effect of vaginal bleeding in
early pregnancy on outcome. Obstet Gynecol 1984;63:515–8.
3 Funderburk SJ, Guthrie D, Meldrum D. Outcome of pregnancies
complicated by early vaginal bleeding. Br J Obstet Gynaecol
1980;87:100–5.
4 Hertz JB, Heisterberg L. The outcome of pregnancy after threatened
abortion. Acta Obstet Gynecol Scand 1985;64:151–6.
5 Mulik V, Bethel J, Bhal K. A retrospective population-based study of
primigravid women on the potential effect of threatened miscarriage
on obstetric outcome. J Obstet Gynaecol 2004;24:249–53.
6 Sipila P, Hartikainen Sorri AL, Oja H, Von WL. Perinatal outcome of
pregnancies complicated by vaginal bleeding. Br J Obstet Gynaecol
1992;99:959–63.
7 Strobino B, Pantel SJ. Gestational vaginal bleeding and pregnancy
outcome. Am J Epidemiol 1989;129:806–15.
8 Weiss JL, Malone FD, Vidaver J, Ball RH, Nyberg DA, Comstock CH,
et al. Threatened abortion: a risk factor for poor pregnancy out-
come, a population-based screening study. Am J Obstet Gynecol
2004;190:745–50.
9 Wijesiriwardana A, Bhattacharya S, Shetty A, Smith N, Bhattacharya
S. Obstetric outcome in women with threatened miscarriage in the
first trimester. Obstet Gynecol 2006;107:557–62.
10 Ananth CV, Savitz DA. Vaginal bleeding and adverse reproductive
outcomes: a meta-analysis. Pediatr Perinat Epidemiol 1994;8:62–78.
11 Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D,
et al. Meta-analysis of observational studies in epidemiology: a pro-
posal for reporting. Meta-analysis Of Observational Studies in Epide-
miology (MOOSE) group. JAMA 2000;283:2008–12.
12 Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al.
The Newcastle-Ottawa scale (NOS) for assessing the quality of
nonrandomised studies in meta-analyses [www.ohri.ca/programs/
clinical_epidemiology/oxford.htm]. Accessed 28 April 2009.
13 Karim SA, Bakhtawar I, Butta AT, Jalil M. Effects of first and second
trimester vaginal bleeding on pregnancy outcome. J Pak Med Assoc
1998;48:40–2.
14 Yang J, Hartmann KE, Savitz DA, Herring AH, Dole N, Olshan AF,
et al. Vaginal bleeding during pregnancy and preterm birth. Am J
Epidemiol 2004;160:118–25.
15 Arafa M, AbdelFataah M, Abou Seid H, ElKhouly A. Outcomes of
pregnancies complicated by early vaginal bleeding. East Med Health
J 2000;6:457–64.
16 Davari-Tanha F, Shariat M, Kaveh M, Ebrahimi M, Jalalvand S. Threa-
tened abortion: a risk factor for poor pregnancy outcome. Acta Med
Iran 2008;46:314–20.
17 Hossain R, Harris T, Lohsoonthorn V, Williams MA. Risk of preterm
delivery in relation to vaginal bleeding in early pregnancy. Eur J
Obstet Gynecol Reprod Biol 2007;135:158–63.
18 Johns J, Hyett J, Jauniaux E. Obstetric outcome after threatened mis-
carriage with and without a hematoma on ultrasound. Obstet Gyne-
col 2003;102:483–7.
Saraswat et al.
256 ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology

19 Johns J, Jauniaux E. Threatened miscarriage as a predictor of obstet-
ric outcome. Obstet Gynecol 2006;107:845–50.
20 Konje JC, Ewings PD, Adewunmi OA, Adelusi B, Ladipo OA. The
outcome of pregnancies complicated by threatened abortion.
J Obstet Gynaecol 1992;12:150–5.
21 Obed JY, Adewole IF. Antepartum haemorrhage: the influence of
first trimester uterine bleeding. West Afr J Med 1997;16:24–6.
22 Tongsong T, Srisomboon J, Wanapirak C, Sirichotiyakul S, Pongsatha
S, Polsrisuthikul T. Pregnancy outcome of threatened abortion with
demonstrable fetal cardiac activity: a cohort study. J Obstet Gynae-
col 1995;21:331–5.
23 Williams MA, Mittendorf R, Lieberman E, Monson RR. Adverse infant
outcomes associated with first-trimester vaginal bleeding. Obstet
Gynecol 1991;78:14–8.
Threatened miscarriage and pregnancy outcome
ª 2009 The Authors Journal compilation ª RCOG 2009 BJOG An International Journal of Obstetrics and Gynaecology 257