Embed Size (px)
Citation preview

Maternal and Child Health Block Grant
NC Division of Public Health Women’s and Children’s Health Section
Kelly Kimple, MD, MPH, FAAP September 26, 2017

Title V - Maternal and Child Health Block Grant Program • Nation’s oldest federal-state partnership
• Aims to improve health and well-being of all mothers and children by − investing in the health of mothers, children & families − improving accountability of performance and impact − demonstrating returns on investment while
maintaining state flexibility

Title V Goals – MCHB/ HRSA • Access to quality care, especially for people with low-incomes
or limited availability of care • Assistance in reduction of infant mortality • Access to comprehensive prenatal and postnatal care for
women, especially low-income and at-risk pregnant women • An increase in health assessments and follow-up diagnostic
and treatment services • Access to preventive and child care services as well as
rehabilitative services for certain children • Family-centered, community-based systems of coordinated
care for children with special health care needs • Toll-free hotlines and assistance in applying for services to
pregnant women with infants and children who are eligible for Title XIX (Medicaid)

Maternal and Child Health Block Grant • First award in 1980
• Annually awarded for the federal fiscal year (October 1 – September 30)
• 2 years to spend the award
• Funds awarded by formula–on the basis of the number of children in poverty in a state in relation to the total number of such children nationally

MCHBG Requirements • Requirements for use of federal MCHBG funds:
• ≥30% preventive and primary care services for children • ≥30% services for children with special health care
needs • ≤10 percent may be used for administering funds
• States must provide a three dollar match for every four Federal dollars allocated
• Maintenance of effort requirement • State will maintain level of funds being provided for
MCH programs at least equal to the level provided in FY 1989

Federal funding for MCHBG
• Decreased by $92 million since FY 2003
Association of Maternal and Child Health Programs, February 2016

Overall buying power has decreased
The image cannot be displayed. Your computer may not have enough memory to open the image, or the image may have been corrupted. Restart your computer, and then open the file again. If the red x still appears, you may have to delete the image and then insert it again.
6000000
8000000
10000000
12000000
14000000
16000000
18000000
20000000
Impact of Inflation on MCHBG for North Carolina* *difference between data points for each year is the actual award less the CPI
rate adjusted award using the 1981 award as the standard
Annual Award Inflation Adjusted Award

MCHBG – State Side
• Block Grant Plans approved on a state fiscal year (July 1 – June 30) basis through the Budget Act
• An annual plan is proposed by DHHS and certified with legislative approval
• Funding must adhere to federal requirements
• General Assembly may designate funding for particular activities and/or organizations

MCHBG – State Side
• Designated set-aside amounts must come from available funds in category assigned − Therefore, existing allocations in those categories must be reduced − Designated allocations mostly are in the local services categories

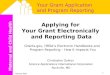
MCHBG – State Side • Since 2011, # of programs and amount of money set
aside by the NC General Assembly has increased to 39% of entire MCHBG in 2017
7.65% 6.73%
11.70%
15.72%
23.06% 22.26%
38.73%
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0.45
FY 11-12 FY 12-13 FY 13-14 FY 14-15 FY 15-16 FY 16-17 FY 17-18
Per
cent
of t
otal
pla
n
Legislated set-asides in the Maternal and Child Health Block Grant state plan

MCHBG – Local Public Health • As a result, “Healthy Mothers, Healthy Children” funding to local health departments has declined
$12,000,000
$12,500,000
$13,000,000
$13,500,000
$14,000,000
$14,500,000
$15,000,000
$15,500,000
$16,000,000
$16,500,000
$17,000,000
SFY 10-11 SFY 11-12 SFY 12-13 SFY 13-14 SFY 14-15 SFY 15-16 SFY 16-17 SFY 17-18**
Healthy Mothers Healthy Children Funding Trends

MCHBG – Local Public Health • Money to fund MCHBG legislated set-asides mostly comes
from local health department (LHD) funding (i.e., no new resources provided) − This in part has been to maintain compliance with Title V statute
• Even with the attempt to minimize impact, LHDs absorb largest share of reductions
• LHDs are critical, especially in rural areas with limited resources and health care access issues
• LHDs have experienced cumulative reductions, now concern for damaging infrastructure to provide safety net services and programs for pregnant women, infants/children and women
• Impacts LHDs ability to offer medical services as a safety net provider and evidence-based programs for maternal and child health

MCHBG Local Public Health • LHDs may receive: − State and Federal funding − County appropriations − Local revenues (i.e. grants) − Medicaid revenues
• Some counties are dependent on state and federal funding for maternal and/or child health services − 22.5% of LHD expenditures (SFY 15-16) overall came from
state/federal funding, but significant range by county − Some counties receive up to 92% of all maternal health
funding from state/federal sources and up to 100% of all child health funding from state/federal funding sources

MCHBG Local Program Expenditures
• Child Health preventive/clinical services
• Maternal Health/ Prenatal services • Reproductive Life Planning • Coordinated Care for Children (CC4C) • Innovative Approaches for Children
with Special Health Care Needs • Strengthening Families/Triple P • Local Child Fatality Prevention Teams • Medical genetics • Newborn metabolic testing/ follow up • Speech and Hearing • Pregnancy Care Management • Healthy Beginnings projects • Oral Health • Preconception Care
• Nurse Family Partnership* • Safe Sleep* • Teen Pregnancy Prevention* • March of Dimes* • 17 P* • Carolina Pregnancy Care Fellowship* • Prevent Blindness* • Sickle Cell Centers* • Perinatal Quality Collaborative • Perinatal & Neonatal Outreach
Coordinator Contracts* • Evidence-Based Programs in Counties
with Highest Infant Mortality Rates* • Every Week Counts Demonstration
Project*
Programs reduced to support designated funding Legislated designated funding (*currently designated)

Questions